Perspectives and Impact of a Parent-Child Intervention on Dietary Intake and Physical Activity Behaviours, Parental Motivation, and Parental Body Composition: A Randomized Controlled Trial

 , ,
, ,
Abstract
1. Introduction
Study Purpose
2. Materials and Methods
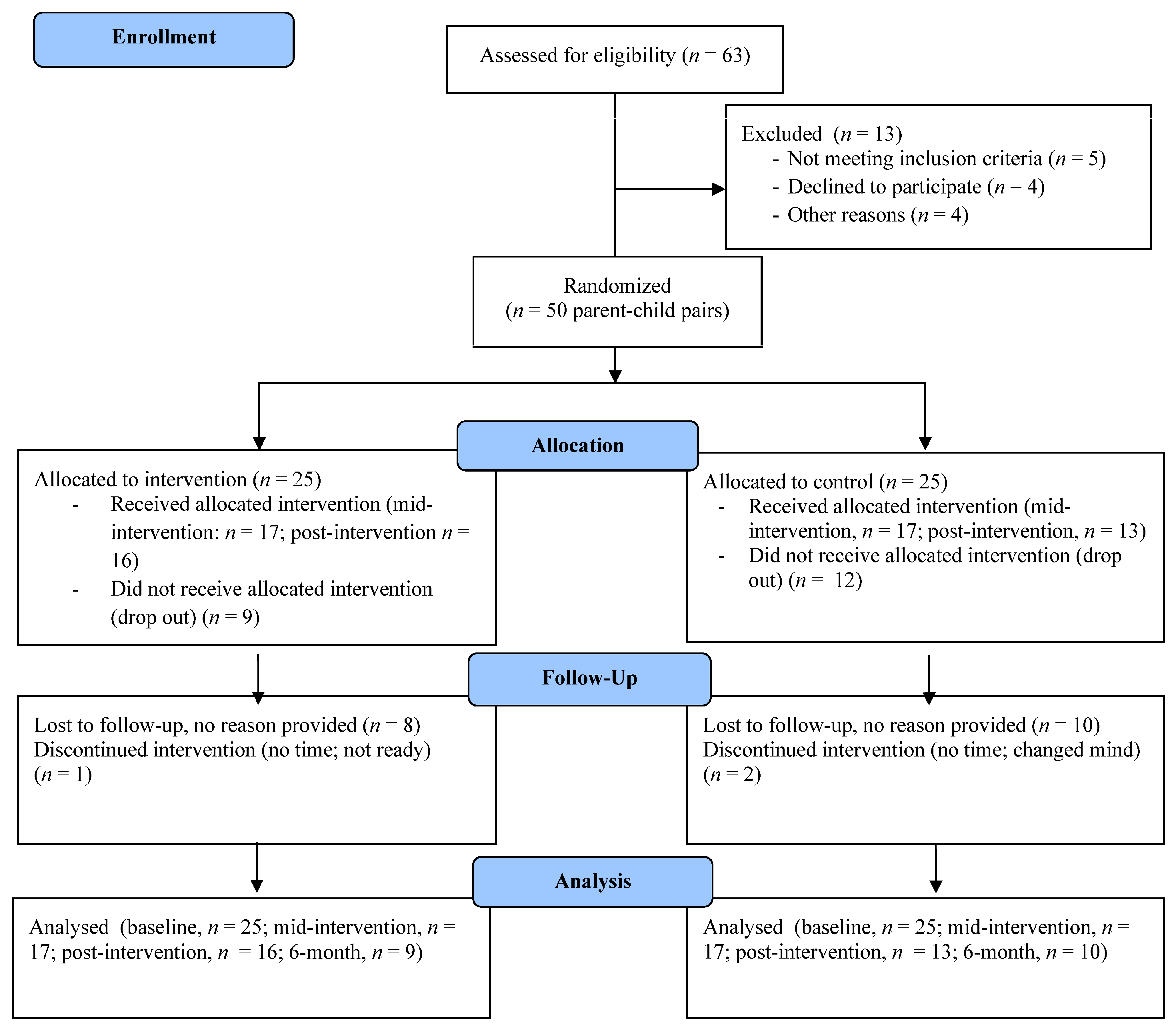
2.1. Design
2.1.1. Participants and Recruitment
2.1.2. Health Education Modules (Webinars)
2.1.3. CALC Plus Health Education Intervention
2.1.4. Certified Professional Co-Active Coaches
2.2. Data Collection
2.3. Measures
2.3.1. Pedometer and 24-h Food Recall (Parent and Child)
2.3.2. Height, Weight, and Waist Circumference (Parent)
2.3.3. Standardized and Validated Questionnaires (Parent)
2.3.4. In-Person Interviews (Parent)
2.4. Analysis
3. Results
3.1. Quantitative Results
3.1.1. Child PA and Dietary Intake
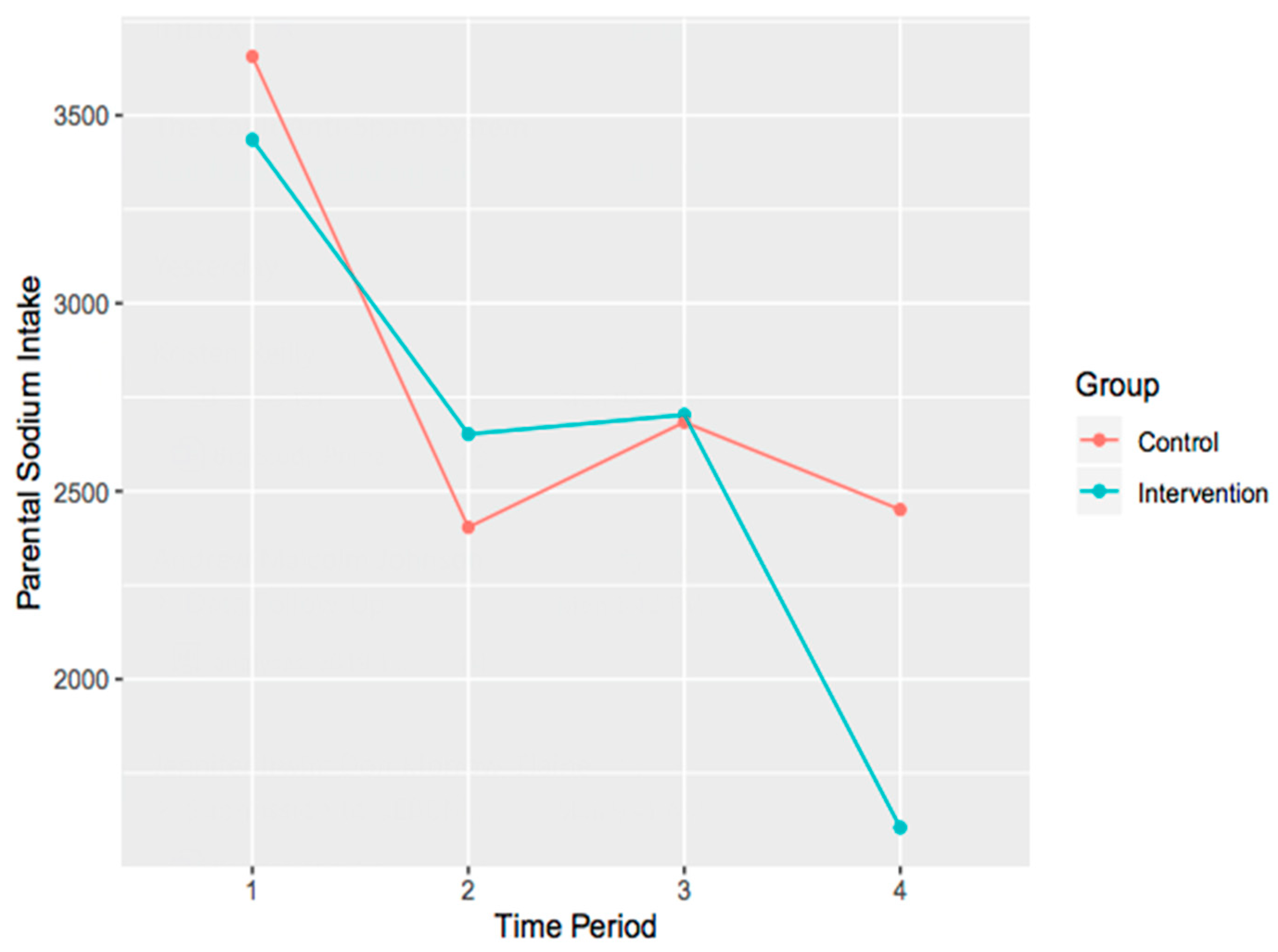
3.1.2. Parent PA, Dietary Intake, and Anthropometric Variables
3.1.3. Parental Motivation
3.2. Qualitative Findings
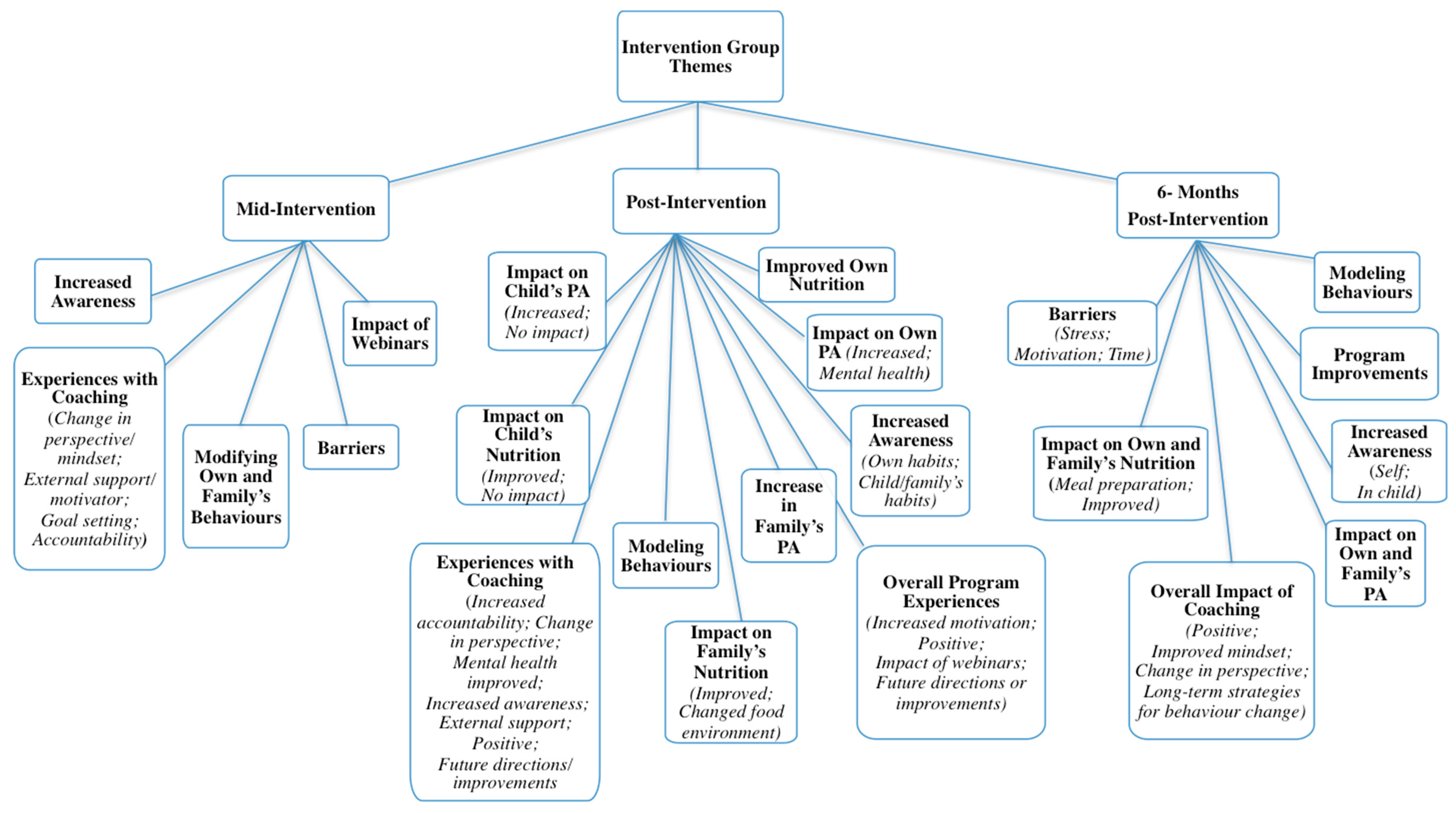
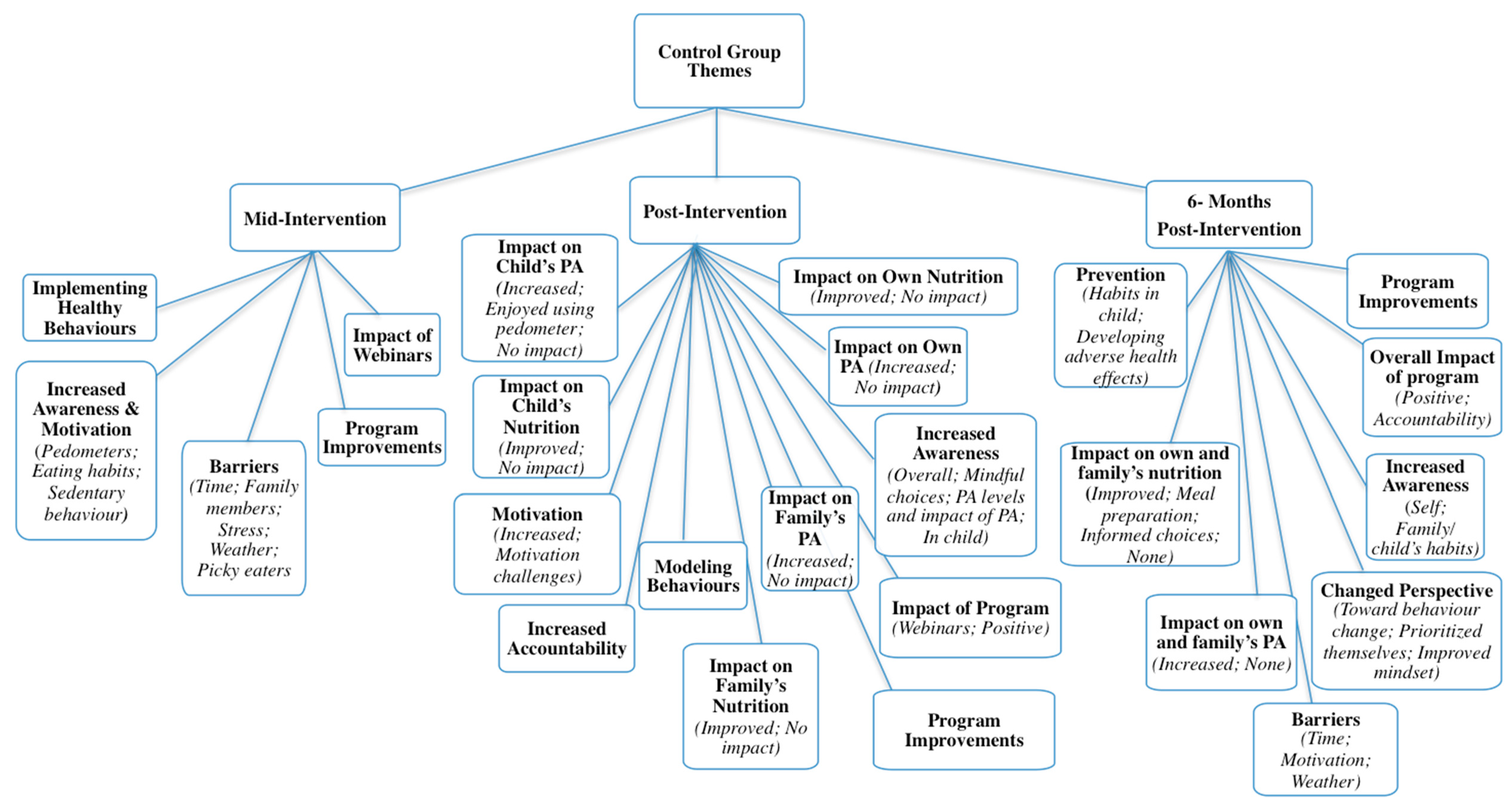
3.2.1. Mid-Intervention Themes
3.2.2. Post-Intervention Follow-Up Themes
3.2.3. Six-Month Follow-Up Themes
4. Discussion
4.1. Strengths
4.2. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO|Childhood Overweight and Obesity. Available online: http://www.who.int/dietphysicalactivity/childhood/en/ (accessed on 16 August 2018).
- Lioret, S.; Campbell, K.J.; Crawford, D.; Spence, A.C.; Hesketh, K.; Mcnaughton, S.A. A parent focused child obesity prevention intervention improves some mother obesity risk behaviors: The Melbourne infant program. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 1. [Google Scholar] [CrossRef] [PubMed]
- Wolfenden, L.; Bell, C.; Wiggers, J.; Butler, M.; James, E.; Chipperfield, K. Engaging parents in child obesity prevention: Support preferences of parents. J. Paediatr. Child Health 2012, 48, 2010–2012. [Google Scholar] [CrossRef] [PubMed]
- Golan, M.; Crow, S. Parents Are Key Players in the Prevention and Treatment of Weight-related Problems. Nutr. Rev. 2004, 62, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Ash, T.; Agaronov, A.; Young, T.; Aftosmes-Tobio, A.; Davison, K.K. Family-based childhood obesity prevention interventions: A systematic review and quantitative content analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Canadian Society of Exercise Physiology. Canadian 24-Hour Movement Guidelines for the Early Years (0-4 years): An Integration of Physical Activity, Sedentary Behaviour and Sleep. Available online: https://csepguidelines.ca/early-years-0-4/ (accessed on 15 September 2020).
- Canadian Society of Exercise Physiology. Canadian Physical Activity Guidelines for Adults (18–64 Years); Canadian Society of Exercise Physiology: Ottawa, ON, Canada, 2011. [Google Scholar]
- ParticipACTION. The Brain + Body Equation: Canadian Kids Need Active Bodies to Build Their Best Brains. The 2018 ParticipACTION Report Card on Physical Activity for Children and Youth; ParticipACTION: Toronto, ON, Canada, 2018. [Google Scholar]
- Tremblay, M.S.; Colley, R.C.; Saunders, T.J.; Healy, G.N.; Owen, N. Physiological and health implications of a sedentary lifestyle. Appl. Physiol. Nutr. Metab. 2010, 35, 725–740. [Google Scholar] [CrossRef] [PubMed]
- Chaddock, L.; Erickson, K.I.; Prakash, R.S.; Voss, M.W.; VanPatter, M.; Pontifex, M.B.; Hillman, C.H.; Kramer, A.F. A functional MRI investigation of the association between childhood aerobic fitness and neurocognitive control. Biol. Psychol. 2012, 89, 260–268. [Google Scholar] [CrossRef]
- Reddon, H.; Meyre, D.; Cairney, J. Physical Activity and Global Self-worth in a Longitudinal Study of Children. Med. Sci. Sport. Exerc. 2017, 49, 1606–1613. [Google Scholar] [CrossRef]
- Schaeffer, D.J.; Krafft, C.E.; Schwarz, N.F.; Lingxi, C.; Rodrigue, A.L.; Pierce, J.E.; Allison, J.D.; Yanasak, N.E.; Liu, T.; Davis, C.L.; et al. An 8-month Exercise Intervention Alters Fronto-temporal White Matter Integrity in Overweight Children. Psychophysiology 2014, 51, 728–733. [Google Scholar] [CrossRef]
- Statistics Canada. Sport Participation 2010; Statistics Canada: Ottawa, ON, Canada, 2012.
- Colley, R.C.; Garriguet, D.; Janssen, I.; Craig, C.L.; Clarke, J.; Tremblay, M.S. Physical activity of Canadian children and youth: Accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Stat. Can. Health Rep. 2011, 22, 1–10. [Google Scholar]
- Garriguet, D.; Colley, R.; Bushnik, T. Parent-Child association in physical activity and sedentary behaviour. Stat. Can. Health Rep. 2017, 28, 3–11. [Google Scholar]
- Canadian Fitness and Lifestyle Research Institute. Bulletin 07: Parental Involvement in Children’s Physical Activity; Canadian Fitness and Lifestyle Research Institute: Ottawa, ON, Canada, 2011. [Google Scholar]
- Health Canada. Do Canadian Children Meet Their Nutrient Requirements Through Food Intake Alone? Health Canada: Ottawa, ON, Canada, 2012. [Google Scholar]
- Garriguet, D. Diet Quality in Canada. Stat. Can. Health Rep. 2009, 20, 1–12. [Google Scholar]
- Rao, T.S.S.; Asha, M.R.; Ramesh, B.N.; Rao, K.S.J. Understanding nutrition, depression and mental illnesses. Indian J. Psychiatry 2008, 50, 77–82. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; Food and Agriculture Organization of the United Nations. Fruit and Vegetables for Health: Report of a Joint FAO/WHO Workshop, 1–3 September 2004, Kobe, Japan; World Health Organization (WHO): Kobe, Japan, 2004. [Google Scholar]
- Health Canada. Do Canadian Adults Meet Their Nutrient Requirements Through Food Intake Alone? Health Canada: Ottawa, ON, Canada, 2012.
- Government of Canada. Canada’s Dietary Guidelines: Foods and Beverages that Undermine Healthy Eating; Government of Canada: Ottawa, ON, Canada, 2019.
- Birch, L.; Savage, J.S.; Ventura, A. Influences on the Development of Children’s Eating Behaviours: From Infancy to Adolescence. Can. J. Diet. Pract. Res. 2007, 68, S1–S56. [Google Scholar] [PubMed]
- Young, E.M.; Fors, S.W.; Hayes, D.M. Associations between Perceived Parent Behaviors and Middle School Student Fruit and Vegetable Consumption. J. Nutr. Educ. Behav. 2004, 36, 2–12. [Google Scholar] [CrossRef]
- Vaughn, A.E.; Ward, D.S.; Fisher, J.O.; Faith, M.S.; Hughes, S.O.; Kremers, S.P.J.; Musher-Eizenman, D.R.; O’Connor, T.M.; Patrick, H.; Power, T.G. Fundamental constructs in food parenting practices: A content map to guide future research. Nutr. Rev. 2016, 74, 98–117. [Google Scholar] [CrossRef]
- Rollnick, S.; Mason, P.; Butler, C. Health Behavior Change: A Guide for Practitioners; Elsevier Health Sciences: London, UK, 1999. [Google Scholar]
- Miller, W.R.; Rollnick, S. Motivational Interviewing: Preparing People to Change Addictive Behavior; Guilford Press: New York, NY, USA, 1991. [Google Scholar]
- Gunnarsdottir, T.; Njardvik, U.; Olafsdottir, A.S.; Craighead, L.W.; Bjarnason, R. The role of parental motivation in family-based treatment for childhood obesity. Obesity 2011, 19, 1654–1662. [Google Scholar] [CrossRef]
- Van Allen, J.; Kuhl, E.S.; Filigno, S.S.; Clifford, L.M.; Connor, J.M.; Stark, L.J. Changes in parent motivation predicts changes in body mass index z-score (zBMI) and dietary intake among preschoolers enrolled in a family-based obesity intervention. J. Pediatr. Psychol. 2014, 39, 1028–1037. [Google Scholar] [CrossRef]
- Jansen, E.; Mulkens, S.; Jansen, A. Tackling childhood overweight: Treating parents exclusively is effective. Int. J. Obes. 2011, 35, 501–509. [Google Scholar] [CrossRef][Green Version]
- O’Neil, M.E.; Shewokis, P.A.; Falkenstein, K.K.; DeLago, C.W.; Smith, S.A.; Vaughn, N.A.; Costigan, T.E. Psychosocial factors and health perceptions in parents and children who are overweight or obese. Obesity 2010, 18, 1558–1565. [Google Scholar] [CrossRef]
- Braet, C.; Jeannin, R.; Mels, S.; Moens, E.; Van Wincke, M. Ending Prematurely a Weight Loss Programme: The Impact of Child and Family Characteristics. Clin. Psychol. Psychother. 2010, 17, 406–417. [Google Scholar] [CrossRef]
- Brown, H.E.; Atkin, A.J.; Panter, J.; Wong, G.; Chinapaw, M.J.M.; Van Sluijs, E.M.F. Family-based interventions to increase physical activity in children: A systematic review, meta-analysis and realist synthesis. Obes. Rev. 2016, 17, 345–360. [Google Scholar] [CrossRef] [PubMed]
- Sung-Chan, P.; Sung, Y.W.; Zhao, X.; Brownson, R.C. Family-based models for childhood-obesity intervention: A systematic review of randomized controlled trials. Obes. Rev. 2013, 14, 265–278. [Google Scholar] [CrossRef] [PubMed]
- Fried, R.R.; Irwin, J.D. Calmly coping: A Motivational Interviewing Via Co-Active Life Coaching (MI-VIA-CALC) pilot intervention for university students with perceived levels of high stress. Int. J. Evid. Based Coach. Mentor. 2016, 14, 16–33. [Google Scholar]
- Mantler, T.; Irwin, J.D.; Morrow, D.; Hall, C.; Mandich, A. Assessing motivational interviewing via co-active life coaching on selected smoking cessation outcomes. Addict. Res. Theory 2015, 23, 131–142. [Google Scholar] [CrossRef]
- Newnham-Kanas, C.; Irwin, J.D.; Morrow, D. Co-Active Life Coaching as a Treatment for Adults with Obesity. Int. J. Evid. Based Coach. Mentor. 2008, 6, 1–12. [Google Scholar]
- Pearson, E.S.; Irwin, J.D.; Morrow, D.; Hall, C.R. The CHANGE Program: Comparing an interactive versus prescriptive obesity intervention on university students’ self-esteem and quality of life. Appl. Psychol. Health Well-Being 2012, 4, 369–389. [Google Scholar] [CrossRef]
- Kimsey-House, H.; Kimsey-House, K.; Sandahl, P.; Whitworth, L. Co-Active Coaching: The Proven Framework for Transformative Conversations at Work and in Life, 4th ed.; Nicholas Brealey Publishing: Boston, MA, USA, 2018. [Google Scholar]
- Shannon-Baker, P. Making paradigms meaningful in mixed methods research. Mix. Methods Res. 2016, 10, 319–334. [Google Scholar] [CrossRef]
- Karmali, S.; Ng, V.; Battram, D.; Burke, S.; Morrow, D.; Pearson, E.S.; Tucker, P.; Mantler, T.; Cramp, A.; Petrella, R.; et al. Coaching and/or education intervention for parents with overweight/obesity and their children: Study protocol of a single-centre randomized controlled trial. BMC Public Health 2019, 19, 1–12. [Google Scholar] [CrossRef]
- Canadian Institutes of Health Research; Natural Sciences and Engineering Research Council of Canada; Social Sciences and Humanities Research Council. Tri-Council Policy Statement Ethical Conduct for Research Involving Humans; Government of Canada: Ottawa, ON, Canada, 2018.
- Chen, J.; Weiss, S.; Heyman, M.B.; Lustig, R.H. Efficacy of a child-centered and family-based program in promoting healthy weight and healthy beahviors in Chinese American children: A randomized controlled study. J. Public Health 2009, 32, 219–229. [Google Scholar] [CrossRef]
- Beech, B.; Klesges, R. Child-and parent-targeted interventions: The Memphis GEMS pilot study. Ethn. Dis. 2003, 13, S40–S53. [Google Scholar]
- World Health Organization. Health Promotion: What Is Health Promotion? World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Health Canada. Food and Nutrition; Health Canada: Ottawa, ON, Canada, 2017.
- Amisola, R.V.B.; Jacobson, M.S. Physical activity, exercise, and sedentary activity: Relationship to the causes and treatment of obesity. Adolesc. Med. 2003, 14, 23. [Google Scholar] [PubMed]
- Co-Active Training Institute. Professional Coach Certification. Available online: https://coactive.com/training/professional-coach-certification/ (accessed on 17 September 2020).
- Heart and Stroke Foundation of Canada Health Seekers: Healthy Weight and Waist. Available online: https://www.heartandstroke.ca/get-healthy/healthy-weight/healthy-weight-and-waist (accessed on 10 August 2016).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Connell, J.P. Perceived locus of causality and internalization: Examining reasons for acting in two domains. J. Pers. Soc. Psychol. 1989, 57, 749–761. [Google Scholar] [CrossRef] [PubMed]
- Levesque, C.S.; Williams, G.C.; Elliot, D.; Pickering, M.A.; Bodenhamer, B.; Finley, P.J. Validating the theoretical structure of the Treatment Self-Regulation Questionnaire (TSRQ) across three different health behaviors. Health Educ. Res. 2006, 22, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Pearson, E.S.; Irwin, J.D.; Burke, S.M.; Shapiro, S. Parental perspectives of a 4-week family-based lifestyle intervention for children with obesity. Glob. J. Health Sci. 2013, 5, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Newnham-Kanas, C.; Morrow, D.; Irwin, J.D. Participants’ perceived utility of motivational interviewing using Co-Active Life Coaching skills on their struggle with obesity. Coach. Int. J. Theory Res. Pract. 2011, 4, 104–122. [Google Scholar] [CrossRef]
- Jennrich, R.I.; Schluchter, M.D. Unbalanced repeated-measures models with structured covariance matrices. Biometrics 1986, 42, 805–820. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2019; Available online: https://www.r-project.org/ (accessed on 18 September 2020).
- Bates, D.; Maechler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. lmerTest Package: Tests in Linear Mixed Effects Models. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar] [CrossRef]
- Lenth, R. Emmeans: Estimated Marginal Means, aka Least-Squares Means. 2019. Available online: https://cran.r-project.org/web/packages/emmeans/index.html (accessed on 18 September 2020).
- Patton, M.Q. Qualitative Research & Evaluation Methods, 4th ed.; Sage Publications: London, UK, 2015. [Google Scholar]
- Karmali, S.; Battram, D.S.; Burke, S.M.; Cramp, A.; Mantler, T.; Morrow, D.; Ng, V.; Pearson, E.S.; Petrella, R.; Tucker, P.; et al. Clients’ and coaches’ perspectives of a life coaching intervention for parents with overweight/obesity. Int. J. Evid. Based Coach. Mentor. 2020, 18, 115–132. [Google Scholar]
- Hammersley, M.; Okely, A.D.; Batterham, M.J.; Jones, R.A. An Internet-Based Childhood Obesity Prevention Program (Time2bHealthy) for Parents of Preschool-Aged Children: Randomized Controlled Trial. J. Med. Internet Res. 2019, 21, 1–44. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.-H.; Feng, H.; Xu, T.-T.; Zhang, H.-R.; Zhao, Z.-Y.; Lai, J.-B.; Xu, D.-R.; Xu, Y. Altered microstructure of brain white matter in females with anorexia nervosa: A diffusion tensor imaging study. Neuropsychiatr. Dis. Treat. 2017, 13, 2829–2836. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Health Canada. Sodium in Canada; Health Canada: Ottawa, ON, Canada, 2017.
- Health Canada. Sodium Reduction in Processed Foods in Canada: An Evaluation of Progress toward Voluntary Targets from 2012 to 2016; Health Canada: Ottawa, ON, Canada, 2018.
- Goddard, A.M.; Morrow, D. Assessing the impact of Motivational-Interviewing via Co-active Life Coaching on engagement in physical activity. Int. J. Evid. Based Coach. Mentor. 2015, 13, 101–122. [Google Scholar]
- Van Zandvoort, M.; Irwin, J.D.; Morrow, D. The impact of co-active life coaching on female university students with obesity. Int. J. Evid. Based Coach. Mentor. 2009, 7, 104–118. [Google Scholar]
- Newnham-Kanas, C.; Irwin, J.D.; Morrow, D.; Battram, D. The quantitative assessment of Motivational Interviewing using Co-active Life Coaching Skills as an intervention for adults struggling with obesity. Int. Coach. Psychol. Rev. 2011, 6, 211–228. [Google Scholar]
- Montesi, L.; El Ghoch, M.; Brodosi, L.; Calugi, S.; Marchesini, G.; Dalle Grave, R. Long-term weight loss maintenance for obesity: A multidisciplinary approach. Diabetes Metab. Syndr. Obes. Targets Ther. 2016, 9, 37–46. [Google Scholar] [CrossRef]
- Pearson, E.S.; Irwin, J.D.; Morrow, D.; Battram, D.S.; Melling, C.W.J. The CHANGE program: Comparing an interactive vs. prescriptive approach to self-management among university students with obesity. Can. J. Diabetes 2013, 37, 4–11. [Google Scholar] [CrossRef]
- Ostbye, T.; Krause, K.M.; Stroo, M.; Lovelady, C.A.; Evenson, K.R.; Peterson, B.L.; Bastian, L.A.; Swamy, G.K.; West, D.G.; Brouwer, R.J.N.; et al. Parent-focused change to prevent obesity in preschoolers: Results from the KAN-DO study. Prev. Med. 2012, 55, 188–195. [Google Scholar] [CrossRef]
- Webber, K.H.; Tate, D.F.; Ward, D.S.; Bowling, J.M. Motivation and Its Relationship to Adherence to Self-monitoring and Weight Loss in a 16-week Internet Behavioral Weight Loss Intervention. J. Nutr. Educ. Behav. 2010, 42, 161–168. [Google Scholar] [CrossRef]
- Dwyer, L.A.; Bolger, N.; Laurenceau, J.; Patrick, H.; Oh, A.; Nebeling, L.C.; Hennessy, E. Autonomous Motivation and Fruit/Vegetable Intake in Parent–Adolescent Dyads. Am. J. Prev. Med. 2017, 52, 863–871. [Google Scholar] [CrossRef]
- Fisher, A.; Hammersley, M.L.; Jones, R.A.; Morgan, P.J.; Collins, C.E.; Okely, A. Goal setting for weight-related behavior change in children: An exploratory study. Nutr. Health 2018, 24, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Burgess, E.; Hassmen, P.; Pumpa, K.L. Determinants of adherence to lifestyle intervention in adults with obesity: A systematic review. Clin. Obes. 2017, 7, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Patton, M.Q. Enhancing the Quality and Credibility for Qualitative Analysis. Health Serv. Res. 1992, 34, 1189. [Google Scholar]
- Sobo, E.J.; Seid, M.; Gelherd, L.R. Parent-Identified Barriers to Pediatric Health Care: A Process-Oriented Model. Health Serv. Res. 2005, 41, 148–172. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Young, M.D.; Lloyd, A.B.; Wang, M.L.; Eather, N.; Miller, A.; Murtagh, E.M.; Barnes, A.T.; Pagoto, S.L. Involvement of Fathers in Pediatric Obesity Treatment and Prevention Trials: A Systematic Review. Pediatrics 2017, 139, e20162635. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Kitos, N.; Aftosmes-Tobio, A.; Ash, T.; Agaronov, A.; Sepulveda, M.; Haines, J. The forgotten parent: Fathers’ representation in family interventions to prevent childhood obesity. Prev. Med. 2018, 114, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Loth, K.A.; MacLehose, R.F.; Fulkerson, J.A.; Crow, S.; Neumark-Sztainer, D. Food-Related Parenting Practices and Adolescent Weight Status: A Population-Based Study. Pediatrics 2013, 131, e1443–e1450. [Google Scholar] [CrossRef]
- Wong, M.S.; Jones-Smith, J.C.; Colantuoni, E.; Thorpe, R.J.; Bleich, S.N.; Chan, K.S. The Longitudinal Association Between Early Childhood Obesity and Fathers’ Involvement in Caregiving and Decision-Making. Obesity 2017, 25, 1754–1761. [Google Scholar] [CrossRef]
- Cui, Z.; Seburg, E.M.; Sherwood, N.E.; Faith, M.S.; Ward, D.S. Recruitment and retention in obesity prevention and treatment trials targeting minority or low-income children: A review of the clinical trials registration database. BMC Trials 2015, 16, 1–15. [Google Scholar] [CrossRef]
- Hattori, A.; Sturm, R. The obesity epidemic and changes in self-report biases in BMI. Obesity 2013, 21, 856–860. [Google Scholar] [CrossRef]
- Fisher, R.J. Social desirability bias and the validity of indirect questioning. J. Consum. Res. 1993, 20, 303–315. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| - Please give us feedback on this program, positive or negative, about your experiences so far |
| ○ Please elaborate on what has assisted with behaviour change and what has not |
| - What did you like best about the program? |
| ○ What parts of the program did you find most helpful, and why? |
| - What did you not like about the program? |
| - Thinking back to before you started the program compared to now: |
| ○ What impact do you think the program has had on the physical activity behaviours of your child (the one who is registered in the study)? |
| ○ What impact do you think the program has had on your physical activity behaviours? |
| ○ What impact do you think the program has had on the physical activity behaviours of your family, as a whole? |
| ○ What impact do you think the program has had on the dietary intake/nutrition of your child (the one who is registered in the study)? |
| ○ What impact do you think the program has had on your dietary intake/nutrition behaviours? |
| ○ What impact do you think the program has had on the dietary intake/nutrition behaviours of your family, as a whole? |
| ○ What would you say is the most important thing you learned from being in the program? |
| ○ If we were to provide this program again, what recommendations would you have for any changes we should make? |
| ○ What else do you want us to know about your experience with the program and how it has influenced you, your child, and your family? |
| Participant Characteristic (Baseline) | N | % | Mean | SD |
|---|---|---|---|---|
| Parent Sex | ||||
| Male | 3 | 6 | ||
| Female | 47 | 94 | ||
| Parent Ethnicity | ||||
| Caucasian | 43 | 86 | ||
| African Canadian | 2 | 4 | ||
| Latin-American | 2 | 4 | ||
| Asian | 1 | 2 | ||
| Other | 2 | 4 | ||
| Parent BMI (kg/m2) | 36.1 | 7.3 | ||
| Parent Waist Circumference (inches) | 44.0 | 5.6 | ||
| Parent Education (Highest level completed) | ||||
| Secondary/High School | 6 | 12 | ||
| College | 20 | 40 | ||
| University | 17 | 34 | ||
| Graduate School | 7 | 14 | ||
| Family Situation | ||||
| Single-parent | 8 | 16 | ||
| Double-parent | 42 | 84 | ||
| Number of people in household | ||||
| 2 | 0 | 0 | ||
| 3 | 12 | 24 | ||
| 4 | 26 | 52 | ||
| 5 | 6 | 12 | ||
| 6 | 5 | 10 | ||
| 7 or more | 1 | 2 | ||
| Annual Household Income | ||||
| Less than $20,000 | 1 | 2 | ||
| $20,000–$39,999 | 7 | 14 | ||
| $40,000–$59,999 | 5 | 10 | ||
| $60,000–$79,999 | 10 | 20 | ||
| $80,000–$99,999 | 4 | 8 | ||
| $100,000–$119,999 | 3 | 6 | ||
| $120,000–$149,999 | 10 | 20 | ||
| >$150,000 | 5 | 10 | ||
| Prefer not to answer | 5 | 10 | ||
| Child Sex | ||||
| Male | 18 | 36 | ||
| Female | 32 | 64 | ||
| Child Age | 6.8 | 2.8 | ||
| Child Ethnicity | ||||
| Caucasian | 39 | 78 | ||
| African Canadian | 4 | 8 | ||
| Native/Aboriginal | 1 | 2 | ||
| Latin-American | 2 | 4 | ||
| Asian | 1 | 2 | ||
| Other | 2 | 4 |
| Intervention Group Baseline | Intervention Group 6-Week | Intervention Group Post | Intervention Group 6-Month | Control Group Baseline | Control Group 6-Week | Control Group Post | Control Group 6-Month | |
|---|---|---|---|---|---|---|---|---|
| Mean steps (SD) | 6830 (1782.55) | 10,371 (6884) | 11,179 (4323) | 9259 (2072) | 11,671 (4264) | 10,741 (3520) | 11,016 (4700) | 10,537 (4981) |
| Protein, g (SD) | 59.5 (17.3) | 64.1 (25.1) | 75.3 (24.2) | 50.2 (10.8) | 75.9 (23.5) | 67.8 (23.4) | 69.7 (20.9) | 71.8 (14.8) |
| Fibre, g (SD) | 17.7 (13.1) | 15.9 (6.5) | 15.6 (3.8) | 15.2 (8.1) | 17.9 (9.2) | 15.9 (7.8) | 17.7 (7.8) | 18.9 (6.1) |
| Saturated Fat, g (SD) | 17.9 (5.5) | 25.7 (14.5) | 17.2 (8.0) | 23.9 (26.0) | 21.4 (8.8) | 16.7 (10.9) | 20.7 (16.6) | 26.5 (16.1) |
| Sodium, mg (SD) | 2204.1 (806.3) | 2467.0 (1498.3) | 2119.9 (608.9) | 2848.1 (1874.7) | 2551.9 (1016.26) | 2306.7 (2113.08) | 2904.1 (2275.6) | 2698.2 (1343.7) |
| Intervention Group Baseline | Intervention Group 6-Week | Intervention Group Post | Intervention Group 6-Month | Control Group Baseline | Control Group 6-Week | Control Group Post | Control Group 6-Month | |
|---|---|---|---|---|---|---|---|---|
| Mean steps (SD) | 6381 (1731.8) | 7396 (2531) | 8700 (6053) | 5871(1341) | 6550 (2726) | 6805 (2270) | 7677 (1896) | 10,331 (5021) |
| Mean BMI (SD) | 36.7 (7.6) | 37.3 (8.4) | 36.7 (8.4) | 34.8 (7.8) | 35.8 (7.3) | 36.5 (8.5) | 35.9 (9.6) | 36.8 (8.9) |
| Mean Waist Circumference, inches (SD) | 44.1 (6.2) | 43.5 (6.4) | 43.8 (7.2) | 42.6 (6.9) | 43.7 (5.6) | 43.5 (6.2) | 42.9 (7.1) | 43.9 (6.6) |
| IPAQ MET Mins Per Week (SD) | 1113.6 (1009.6) | 1894.8 (1600.0) | 1603.8 (773.3) | 1436.4 (347.1) | 1948.4 (1451.1) | 2920.2 (2084.5) | 2044.5 (1095.2) | 2394.0 (1497.1) |
| IPAQ Sitting Mins Per Day (SD) | 261.8 (181.3) | 580.0 (1340.8) | 240.0 (144.7) | 285.0 (79.9) | 354.6 (247.8) | 328.9 (210.8) | 326.4 (108.8) | 222.0 (176.8) |
| Intervention Group Baseline | Intervention Group 6-Week | Intervention Group Post | Intervention Group 6-Month | Control Group Baseline | Control Group 6-Week | Control Group Post | Control Group 6-Month | |
|---|---|---|---|---|---|---|---|---|
| Calories (SD), kcal | 2026.5 (753.3) | 1833.9 (1741.7) | 2012.8 (622.3) | 1810.5 (730.3) | 2256.8 (557.9) | 1884.3 (561.2) | 1741.7 (438.4) | 1660.2 (381.4) |
| Protein (SD), grams | 82.1 (34.8) | 86.6 (34.8) | 107.1 (37.9) | 70.7 (31.9) | 98.1 (37.3) | 94.7 (31.3) | 88.4 (22.9) | 98.9 (33.9) |
| Fibre (SD), grams | 24.1 (18.2) | 24.7 (17.5) | 20.8 (5.7) | 19.5 (7.8) | 22.6 (10.4) | 23.6 (11.1) | 18.6 (9.7) | 17.1 (7.5) |
| Saturated Fat (SD), grams | 24.8 (12.4) | 27.6 (23.2) | 27.4 (14.9) | 30.7 (25.7) | 34.0 (17.1) | 21.9 (12.1) | 33.4 (26.7) | 28.5 (17.7) |
| Sodium (SD), milligrams | 3380.8 (1790.3) | 2670.5 (2000.8) | 2617.9 (1332.0) | 1942.9 (1450.6) | 3659.4 (1713.3) | 2450.2 (1657.7) | 2766.4 (1571.7) | 2468.9 (1737.0) |
| Intervention Group Baseline | Intervention Group 6-Week | Intervention Group Post | Intervention Group 6-Month | Control Group Baseline | Control Group 6-Week | Control Group Post | Control Group 6-Month | |
|---|---|---|---|---|---|---|---|---|
| TSRQ Diet, Autonomous Motivation (SD) | 5.9 (1.0) | 5.9 (1.1) | 5.6 (1.2) | 5.6 (1.2) | 6.0 (0.8) | 5.9 (0.8) | 5.7 (0.9) | 6.2 (1.0) |
| TSRQ Diet, Controlled Motivation (SD) | 3.8 (1.3) | 3.9 (1.3) | 4.0 (0.9) | 3.5 (1.6) | 3.7 (1.1) | 4.6 (1.2) | 3.8 (1.1) | 3.6 (1.5) |
| TSRQ Diet, Amotivation (SD) | 2.2 (1.0) | 2.1 (1.2) | 2.5 (1.0) | 2.5 (1.4) | 2.4 (1.1) | 2.5 (1.4) | 2.3 (1.2) | 2.0 (0.9) |
| TSRQ Exercise, Autonomous Motivation (SD) | 5.9 (1.3) | 5.8 (1.5) | 5.8 (0.9) | 6.0 (1.0) | 6.0 (1.0) | 5.6 (1.0) | 5.6 (1.1) | 6.0 (1.3) |
| TSRQ Exercise, Controlled Motivation (SD) | 3.5 (1.2) | 3.8 (1.1) | 3.9 (1.3) | 3.6 (1.2) | 3.6 (1.5) | 4.2 (1.2) | 3.8 (1.4) | 3.6 (1.5) |
| TSRQ Exercise, Amotivation (SD) | 2.1 (1.3) | 2.2 (1.2) | 2.6 (1.6) | 2.9 (1.3) | 2.1 (1.2) | 2.6 (1.4) | 2.4 (1.9) | 1.7 (1.0) |
| Theme: Increased Awareness |
| Quote: “…The coaching aspect has definitely [made] a big difference for me. Because I can read the module, and then for a day I really think about it, or the days where, you know, I have to check the steps, I’m much more conscious of it, of, ‘Okay, I’ve got to do this.’ I want [my children] to be active, you know, I want to be on it. Or when I had to write down my food, I thought about it a lot more.” |
| Theme: Modifying Own and Family Behaviours |
| Quote: “I think that my nutrition’s changing … in the options that I’m picking, ‘cause I have to eat certain amounts of carbs, but it’s trying to make those healthier options of what type of carbohydrates I’m eating. Like, having a piece of bread or vegetable or fruit instead. … Is a much better option than having a bowl of cheezies. … I have to have a snack every night I’ll have a peanut butter sandwich instead of a bowl of chips.” |
| Theme: Impact of Webinars |
| Quote: “The biggest [learning] … that was impactful for me was going into the grocery store and reading the ingredients a little bit more. … You see things like 20 percent or 5 percent, and it didn’t mean anything to me [before completing the webinars].” |
| “I really like some of the tips for handling the issues…with children and eating… The idea of not giving them food when they’re upset… was interesting to me and the way it was described [I] was like, ‘Yeah that makes sense.’ If you feed them when they’re upset then they learn that food just makes them feel good… I can see how that would lead to emotional eating.” |
| Theme: Barriers |
| Quote: “I think over the winter … some of [webinar] ideas will be good, because we’re kind of stuck inside now. … That’s where we kind of get … lazier. So I think just doing different activities inside and stuff will be really good.” |
| “[If] I went to the YMCA that’s closest to me now I’m gone for over an hour to go to a class that’s 30 min. … It’s just a lot to take out of your day when you have two young kids at home.” |
| “So, if you are buying a lot [of healthy food], that adds up. Same with every single fruit. … even the ones that are not organic [are] expensive. The meat went through the roof, certain spices [are] way … too expensive.” |
| Increased Awareness & Motivation |
|---|
| ● Pedometers |
| “This [pedometer] is addictive. … I’m surprised how many more steps [my daughter] does in a day. … She was at … 16,000 where I was still at [9000].” |
| “My daughter… is talking about [the program] a lot, and was very excited about the step counters, and was …Very excited to be like, ‘Hey, look at how many steps I’ve achieved.’” |
| ● Eating Habits |
| “I have noticed … my daughter… is a lot more active than I am currently, but I have noticed…what we’re eating is starting to affect her. … my bad choices are now affecting the entire family, not just me … [A]ll of the [webinar] videos that were related to the child part of it … she watched with me. … She enjoyed that. But I think for me too, it’s realizing that the choices I’m making are affecting more than just me.” |
| “I have a job … driving around the city all day… [leading to] bad habits of going through drive-thrus… so I am now making more conscious decisions to stop at the grocery store, if I don’t have a lunch … I can just get a salad or something a little more healthier. … [The program has] made me more conscious that way. |
| ● Sedentary Behaviour |
| “[My child] loves YouTube. … So, we’ve always limited …screen time. But it’s interesting, when [the webinar is] saying… one or two hours a day of screen time. You think about how that adds up so fast. … She’s eating her breakfast, she comes home, she watches a little bit. It can easily be an hour, two hours without thinking about it. … So that’s definitely something that… I pay attention to.” |
| Implementing Healthy Behaviours |
| “[My child] can be a little bit of a picky eater, so [prior to joining the program] we would end up just caving into him and giving him whatever he wanted. … So, we cut back on that.” |
| “My husband and I have … got rid of all treats in the house, so when it’s a snack … the only option available is fruit.” |
| “… [I am] parking further away and walking and just trying to get as many steps in as possible.” |
| Impact of Webinars |
| “The program itself has been good information. The videos are good …it wasn’t a lot of things that I didn’t already know. … But, it’s good to … have the reiteration of things that I should know, but don’t follow.” |
| “I read [daily value percentages] now every time I go to a grocery store, I always check the values, I check the fat, I check everything that is not healthy, I try to stay away from that. … [Before] I wouldn’t care about that much.” |
| Barriers |
| ● Time |
| “[L]ife is busy, so… I kind of forgot about the [webinars] and so I have to remind myself to do that.” |
| ● Family members |
| “I find it frustrating sometimes … because my husband doesn’t eat vegetables. … And so, I’ll try to prepare … carrots and make them a bit sweet, or try and … entice [my family] with it. … And my husband will be making a face ‘cause he doesn’t like it and I’m like, ‘Can we not? Just like, don’t influence [the children], right? Or don’t say you don’t like it, can you not just eat one carrot and smile?’” |
| ● Stress |
| “I did start [eating healthy] for quite a while [during the program]. I was doing really well, and then some things changed, and there was a little bit too much stress…then I took a week off, and I realized how easy it is to fall back into bad habits.” |
| ● Weather |
| “But when it is that hot [outside], most people are staying in and kind of hibernating, because it’s too hot to be out, and so we have been trying to get outside every single day, but even if it’s just the backyard, but again, walking from my bedroom to the back door isn’t really a lot of exercise…” |
| ● Picky eaters |
| “I also feel like incorporating [healthy foods] in a way that [kids] don’t know isn’t really teaching them why it’s important [to eat healthy]. … And I also wish they would just give it a chance. Cause like, I make turnips, and I use a little bit of brown sugar, and I know that the oldest would like it, it’s just there’s no chance [my younger child will] even try it.” |
| Program Improvements |
| “I would forget about the online [webinars], just cause it’s online or whatever, maybe … a reminder… every week … Just kind of like touch base and remind you that the videos are on there.” |
| “… I think that extra accountability piece would have made a difference. Whereas, now this is the second time we’re meeting, it’s a couple months in, and… I know I’m accountable but not to the extent … if I was also getting that [coaching] phone call. I would have been, like, ‘Oh my gosh, they’re gonna know even more.’ … Not that I’m hiding anything, but… just having the extra little bit of accountability… would have been better in my situation.” |
| Impact on Child’s Nutrition |
|---|
| ● Improved |
| “[The program has] had a huge impact on [my child]. [W]e were always … a free feed family …the fridge is open, the cupboards are open, take what you want, when you want. [My son is] nine so what he wanted was cookies, and sugars, and sweets, and starches all the time. [W]e do so much more meal planning now than we ever did. We sit … and figure out the whole week…. [On] ‘eat whatever you want Friday’ … he won’t eat a whole bag of cookies… which makes me happy…. [He says] ‘I ate my sub I’m going to eat an apple first and then I’ll have my cookie.’ … Whereas before he would’ve been like ‘can I have two? … three?’ Both [of] my… children, but definitely my son [program participant], has been [making] significantly better choices.” |
| “[T]wo weeks ago, we went to McDonald’s and [my child] made a comment going ‘Mommy I don’t really like McDonald’s anymore.’ … But he used to want McDonald’s all the time.” |
| “[My child’s nutrition has] changed a lot. She’s looking more at what’s healthy for her, compared to ‘I’m just hungry and bored and wanna eat.’” |
| ● No Impact |
| “We try to eat… a lot of vegetables, and a lot of fruit, and…we’re already trying to do a lot of substitutions with a lot of vegetables, you know, tofu, beans, etc. … We’ve been doing that all along, so nothing’s changed for her.” |
| “I made it a goal even before the program… [to] feed [my child] better than I feed myself. … I made it a goal when she started eating sold food … to make sure that she was introduced to tons of vegetables and fruit, because it wasn’t the same for me growing up.” |
| Impact on Child’s PA |
| ● Increased |
| “[My child’s behaviours] completely [changed since starting the program]. [H]e’s probably watching half as much TV now as he did three months ago… and … [he’s] wanting to go outside, wanting to play games, wanting to explore … anything [to be] outside more… And he was never that kid before.” |
| [My child] sees me moving more. And she wants to participate, so … I did a 100 squat challenge every day for 30 days… and she would join in with me. … it’s acceptable behaviour to her now, to move more and to exercise. [S]he’ll come to me… and [say] ‘it’s time for exercise.’” |
| “[Before the program my child] was signed up for nothing, and now she’s signed up for 3 things. … So she’s doing karate, yoga, and skating.” |
| ● No Impact |
| “[My child] was super active before we started [the program] and she’s still really active today. … I think the only thing that I’ve changed is that.… I’m going to be enrolling her in some more programs for exercise and things like that.” |
| Improved Own Nutrition |
| “I’ve been… more purposeful to make extras for dinner because that’s one of the healthier meals that we eat [because] we eat as a family. … So I’ll make sure I’ll have enough leftovers for… myself for lunch, versus eating a small bowl of chips.” |
| “Grocery shopping has just changed. [I stick] to the outside perimeter of the grocery store versus going deep into the aisles. … [And when I’m] making muffins… I’ll just throw the carrots in. … I’m sure it’s not even a lot, but again, it’s changing the flavour, texture, getting the taste buds more used to having the sweetness of the carrot and the pineapple in the muffin instead of the sweetness of chocolate.” |
| “The program has definitely [had] a positive impact [on my dietary intake]. … I still struggle with stuff like eating enough fruits and vegetables. … My major goal when I was working with the coach was my sugar intake, that’s what we ended up focusing on. … I realized the other day that my coffee was too sweet and I reduced how much sugar was in it by one teaspoon and then it tasted so much better. I’m losing my taste for sugar for a little bit.” |
| Impact on Own PA |
| ● Increased |
| “I think [what] the program did for me was [help me] understand how important my routine was and how much of an impact it was having on my life. So…the last four weeks I’m up early and working out, I’m making breakfast for my family before I get to work instead of rolling out and [saying] ‘we’re grabbing [fast food] today.’ [Before] I would be like ‘here’s a donut, here’s a cupcake. … And I think if I hadn’t gone through the program, I think I’d still be that way.” |
| “I’m doing more practical activity … like raking and shoveling and playing, skating, skipping, that kind of stuff. It’s not that I’m going to the gym, ‘cause I’ll never be a gym person, is what I have learned over the years. … But [the program] has just spurred me to try and be more active so, it’s … in the back of my mind all the time.” |
| “[Because my job involves a lot of sitting] I can’t incorporate a lot of walking, but I did start… parking further, in parking lots. …[When] sit[ting] in client meetings all day …started standing up, even between the meetings, and I started stretching a little bit more instead of just sitting at the desk and waiting for the next client to come.” |
| ● Mental health |
| “[My coach and I] were talking about how when I’m feeling stuck, like literally just getting up and moving your body, can snap you out of a funk.” |
| Impact on Family’s Nutrition |
| ● Improved |
| “We’re eating healthier because we are following our meal plan, we’re pre-planning our meals so we know what we have in the house and that we make sure we have enough for the rest of the week because I don’t want to go to the grocery store four-five times a week, now it might be twice.” |
| “I’ll just buy one of those vegetable trays from the grocery store and just put it out and [my children] eat it!” |
| “All the kids [love salads now]. One night… was a huge success, half [my son’s] plate was just salad, just naked veggies. … And before [the program], I don’t think that they would have been.” |
| ● Changed food environment |
| “I think [my family] feel[s] like they’re getting a little bit more of a choice [of foods] now. Like if I call home and say we’re having this and this and this, [my children will] say like ‘oh can we have the green beans instead of that?’… [I say] ‘sure, we can switch those.’ …. [I]f I come home and I… need to then cook and then we eat, its 6:30–7:00. Whereas if [my family members] help, I get home, we eat, and then we can spend time together.” |
| “I now go through two bags of apples a week… and two bundles of bananas. … [Before], my bananas would just kind of rot, and then I’d make banana bread.” |
| “[We have been looking for] different [food] options. Like, the kids are even saying, ‘well, that’s not a good option, Mom. Let’s do this one.’ … So, having them buy into it is much easier. … And it’s just more of a conversation we have [about healthy eating], versus mom just plops stuff in front of them.” |
| Increase in Family’s PA |
| “We’ve been skating, we do skipping, and we were out raking yesterday. So [the program] pushes me…to try and do something everyday. Whereas before there were days where… I would come home and just be too tired and we wouldn’t do much at all.” |
| “[Physical activity is] easier because now …on days when I don’t feel like doing [physical activity], [my husband will] say … ‘okay, are we going to go on a walk with the dog tonight’ or ‘we’re going to take kids to the park, and on days where he doesn’t feel like doing it, then I’m the one pushing him. Whereas before it was both of us …watch[ing] TV.’” |
| “Friday nights [used to be] pizza and a movie nights. … And chips. …[V]ersus [now it is family] gym night. … Like, that’s a big change.” |
| Modeling Behaviours |
| “[The program is a] reminder that everything I do in my life, my children are watching me. So whatever I’m doing that I am a model for them. So if I’m modeling very lazy lethargic behaviour, watching TV all the time, not keeping active in my lifestyle, that’s what my kids are going to… think is okay and it’s going to trickle down because that’s what my parents were like. …[A]nd it trickled down into my life and I want to stop that now. I want my children to see what a healthy [life]style looks like.” |
| “I’m being accountable for what [my children are] putting in their bodies. … I knew what I was buying wasn’t the healthiest for them, but it was something that they like. So, I was [starting] to realize ‘okay, well just because it was something they like it doesn’t mean that they need to indulge in that.’” |
| Overall Program Experiences |
| ● Increased motivation |
| “[The program] helped me to get the first step to being motivated to doing something … literally just moving.” |
| ● Positive |
| “I loved the fact that you guys come to the house [for follow-ups]. [Because] … I’ve got a kid, so … getting out of the house is a whole production.” |
| “[The program] was just nice and… an overall reminder just to focus, slow down, look at what it is that we’re doing, and in my case, it was good to reinforce that … we’re doing the right things. …[Y]ou get so stuck in your routine … that you don’t slow down to actually look at what it is that you’re doing, and why, and is it working. So it was kind of nice to have a little bit of a review.” |
| ● Future directions or improvements |
| “I thought it was a really great program… I guess maybe if I was to say anything it would be to like give two different options to people [for the education sessions]… of being flexible, versus having … deadlines and check points. My personality is that I will either try and … rush through it at the start or … do it at the very end, but if there’s deadlines I’m always committed to meeting my deadlines.” |
| “I think there are so many more people [who] could benefit from the program …. [T]he program is so impactful for me that I think… it should be offered to every kid in school. [I]f their parents don’t take it, they don’t take it, but this sort of stuff needs to be taught more in our school at a younger age.” |
| “The only recommendation was to do the webinars… an audio version of them.” |
| Increased Awareness |
|---|
| “[My child and I] talked about healthy [eating], like she always knew what a healthy versus unhealthy food was, but like when [she’s] five and there’s a bag of chips and apple I mean obviously she is going to choose that. So I find now that she is more likely to go and choose one of her healthy snacks without me having to remind her.” |
| Impact on Child’s Nutrition |
| ● Improved |
| “We are hard on fast food now. …instead of just eating fries or cheese pizza [at the mall] she would go and get white rice, broccoli, or like shrimp. …[E]ven though some of that stuff’s not…made the best, at least I know … that stuff is going to fill her up [better] than the other stuff.” |
| “Even getting [my child] things like a protein bar right, because at least that’s better than eating a chocolate bar. … So, we would buy something that was a little… healthier on the go, because he’s usually running out the door in the mornings. … And, [I am] buying the … cut fruits and vegetables so that it is already ready for him to grab….” |
| “[My child has] always been a pretty good fruit eater. But we tried to introduce new foods, expand the repertoire… some vegetables, some protein. … [He is] eating carrots now, celery… we tried some beans, black beans and kidney beans. … Scrambled eggs.” |
| ● No Impact |
| “I don’t think [nutrition] necessarily changed for [my child]. It wasn’t necessarily the dietary stuff, for her. … There’s never been a lack of healthy options in the home.” |
| Impact on Child’s PA |
| ● Increased |
| “[Before the program my children would] come home… get a freezie or … a pack of gummies, and they would just sit. … Most of the time my oldest would always fall asleep then she would complain of headaches, so this summer… she wasn’t the one steady participating [in this program] per se but she picked up off of the younger one [who was participating]. [T]he younger one … now …[has] a routine, it’s normal for her. So now if she’s watching TV too long, she gets fidgety. … It’s almost like her body’s telling her like you need to get up and do something … She’s like ‘okay, I’m going to go play’ … [the older child is] getting better, too.” |
| “We definitely are more active now. … Like [my child] snowboards now, he plays hockey, so I volunteer on their hockey team. …. Before [the program] I’d put him in maybe one sport, but now I’m … trying to get him to do more. … So I’ll be taking him more often because it’s really important… it’s fun and we can be active and spend time together.” |
| ● Enjoyed using pedometer |
| “I do think [my child] tried to get more steps in with that pedometer. She’d be sitting still and then stand up and walk around and then look at the pedometer and stand up and look at the [step count]. And I would remind her, ‘It’s supposed to be honest, so when you’re walking… you don’t need to do extra steps.’ But, I suppose it is nice that she did get excited by it, and I couldn’t squash that, it was great.” |
| “[My child] was very conscious of [step counting], and of course he liked [it] because he got more steps the days he played soccer… he was into it.” |
| ● No impact |
| “I don’t think [my child’s PA was] really impacted that much. I think… out of the two of us, [my child is] far healthier than I am. Probably because I realize how unhealthy I can be, and want to make sure I’m not instilling those bad habits into her. So I think for her, it was … repetitive information. … She listened to what I had to say, she watched a few videos with me, whenever it was directed towards the child portion, and then just went on her way. I don’t think it really made a significant difference… she’s always active.” |
| Impact on Own Nutrition |
| ● Improved |
| “[Now] I [have] been like ‘nope, I don’t need to get those chips.’” |
| “When I have one carrot, or two, you know, just leftover vegetables… I just puree them…freeze it, and then I use it in my pasta sauce.” |
| “[I]ts not that I don’t like vegetables, it’s that… I find them like boring, and so … I try to make [healthy food] fun for me, too. But… [also trying to stay] away from … bad fats and everything like that.” |
| “[The program helped with me] knowing if I do want a snack, I don’t need the whole bag… [of] chips …. [N]ow, I put some in … a little kid bowl. … [I]f I eat a bag of chips with 1100 calories, that’s more than half of what I should be eating in a day… and I’m still hungry,’ so that was like a big ‘what did you just put in your body’ [realization].” |
| ● No Impact |
| “I wouldn’t say that my eating habits improved all that much but definitely I’m more aware of it.” |
| Impact on Own PA |
| ● Increased |
| “I play baseball during the summer, …I signed up for yoga, which I’ve always been intimidated by. … [I also have been] going to [the gym at work] after work, and now… I park further away so I walk 15 min to work, and 15 min from work.” |
| “I started a new job in the Fall. … And I’ve got my office on the sixth floor and I have stuff to do on the ninth floor and first floor and second floor; so I’m taking the stairs as much as I can.” |
| “Because my son is more active, I’m more active, I don’t just sit around all day. I’m …going out and doing sports with him …before I would probably never. I mean I would have but like it’s a drag. … I still find it exhausting, but I much rather go out and do things with him if it makes him happy.” |
| ● No impact |
| “When I did the first surveys and read the modules, I had a plan, well not exactly a plan, a thought that I would increase my walking, kind of throughout my work day, like take regular walk breaks. … But it just, it hasn’t happened.” |
| “I can’t seem to find time in the days … the days are just so busy, it’s hard to kind of find a time. I mentioned it to a colleague also, who said she would be interested in going walking… but we have never found a time that we’re both free to do that…which is depressing.” |
| Impact on Family’s PA |
| ● Increased |
| “I think [we have] increased physical activity… heading down to the park after school or going for a walk, [because] … it’s really easy sometimes when you’ve had a really long day…to say ‘No we’re just going to stay in.’ But if [my child is] asking to go on a walk, nine out of ten times we’re going to say yes. … We’ll take her to the park, or go for a rollerblade, or whatever it is she wants to do. … So just being more active as a family… more frequently.” |
| “Before [the program] we [would] go for walks but it was like just around the corner and then come back with the dogs and that’s it. But right now, we spend more time together, because we don’t go anymore to the corner, we… go for example to [the park] and we walk the whole [trail]. … We walk, and walk, and walk, and we play together, and we run, we go to parks so, it’s keeping up [PA] together, and my family is helping a lot.” |
| ● No impact |
| “To be fairly honest, I don’t think [the program has] impacted us at all. Probably because I went through it… at the beginning. We were all reading through it, and paying attention to it, and being cognizant of it, and then we just kind of got busy and fell off the track, right? So, [my child]… was excited to watch the videos with me, and we discussed it, and once that piece was over, it was kind of just over. There was nothing, there was nothing more to kind of, pull through.” |
| “I would say [the program had no impact on my family’s PA]… my two sons are very active, my daughter doesn’t really do extra-curriculars yet because she’s small, but she’s kind of active throughout her day.” |
| Impact on Family’s Nutrition |
| ● Improved |
| “We’ve been eating less canned food, too. … [Because] there’s a lot of salt in there.” |
| “Before going back to school, I would hit Costco and just buy boxes of things … and there’s … a drawer [in our home] so they put their hand in and grab whatever they want for a snack… but it’s all packages. … gummies, granola bars … Jello …juice boxes. And now they they get water bottles, so they have nice water bottles… One’s got a Caesar wrap in her lunch for tomorrow and the other one has a cheese quesadilla on …whole wheat naan … instead of … before it’d be morning of, I’d just be grabbing handfuls and throwing it in lunch… grabbing a packet of ‘garbage.’” |
| ● No impact |
| “Once I was through all the videos and stuff I kind of fell off [the program]. So, overall the impact was more just me, and being cognizant of my, I guess bad behaviours, is essentially what it is, my bad eating behaviours. But overall, as a family, it hasn’t changed.” |
| “My husband [went to Costco]… and he said, ‘well, I’ll just buy some food for us,’ [because] I was out, and so they brought a whole… prepared lasagne. [Because] it was only 13 dollars, and it was really good, you know? … So, I’m asking, you know, ‘Where’s the box, [what was the nutritional content] in it?’ … They don’t care. … [If they could, they would eat] that lasagne thing everyday, and the apple pie.” |
| Modeling Behaviours |
| “My husband… is now down 43 pounds. … He doesn’t drink sugar anymore… the fridge mostly [has] water… he’s coaching… football… and out he’s out in the heat right now, where[as] before he would come home, get on his laptop, watch TV, and then have his phone. … So, now three nights a week he’s out coaching football. … It blows my mind because he doesn’t feel sluggish anymore. … sugar… was … the biggest thing for our family. [O]nce we went through that massive first two weeks of … shock to your system, where everyone felt horrible… then we started feeling better….’” |
| “[My child] joined track this year, she’s joined the volleyball team so I think [me changing my habits] helped to motivate even her to be… more active as well. …. [S]he sees me being more active instead of… coming home and just slumping on the couch, which isn’t good. …. I was coming home so exhausted… so she just noticed… that I’m not looking and feeling so exhausted.” |
| “Obviously I don’t wanna see my husband eating a hamburger, and I would be eating vegetables. … So, I wouldn’t like that. … My husband doesn’t like vegetables, but he’s eating them… because he wants to help me and help my son too, because obviously my son would say ‘okay why [is] daddy not eating that and why I am eating this?’ … So, all of them are changing.” |
| Overall Impact of Coaching |
|---|
| ● Positive |
| “It was an interesting experience having a life coach, as it made you realize how much all the aspects of your life are correlated. So that made a big difference.” |
| “I loved the start of [the program] I don’t think I would’ve done as well if I hadn’t had someone to talk to. Personally I probably would have loved [coaching] to go on a lot longer. But I think that’s why people who join programs are successful, it’s because they have someone they are accountable to for a longer period of time. … I felt like I could talk to somebody about what my struggles were, who was going to not just listen but help me overcome some of them.” |
| ● Improved mindset |
| “I think [coaching] was probably the best part [of the program]. I think just working on that mental stuff really helps translate into everyday life. … Like, after the sessions, you feel better. And so then you’re more inclined to … eat something healthy and go for a walk as opposed to come home and sit and eat chips on the couch, you know? … More motivated.” |
| “[My coach] had me actually walk away from a fitness company that wasn’t serving me… the relationships I had built with this fitness company were harming my mental health more than helping my physical health. So, she had me walk away from that, which, for mental health was really good … [I began] at-home workouts …which, with my busy schedule, worked really well for being able to fit that in at home.” |
| “My friends can see the struggle of ‘I don’t want to eat that’ or ‘I want to lose weight,’ but [my coach] was able to take me to a deeper level of why I was so enamoured with food … and you know … the other things I needed to deal with and heal to stop replacing them with food. … So, [coaching] was probably the best part of that entire thing.” |
| ● Change in perspective |
| “[My coach and I] talked a lot about happiness and what does that weight really mean and the end of it… [I realized] ‘you know what, I’m just as happy whether I’m 5 pounds up or whether I’m 10 pounds down.’ … I don’t stress [about weight] nearly as much as about it as I did before.” |
| “It’s hard to keep [behaviour change] going and that was something that my life coach sort of helped drill into me, that just because you’re not doing it exactly the way you want to do it now doesn’t mean you should stop, right? So, I think that’s something that I keep in my head, you know, just because you haven’t gone to the gym in 2 weeks doesn’t mean that now you can never go again. … you can start again.” |
| “[My coach] allowed me to see that I can get healthier, but still love who I am. It doesn’t mean I don’t love myself or the size I’m at, or the person I am, currently.” |
| ● Long-term strategies for behaviour change |
| “I still will sometimes force myself to go back and look at things the way [my coach] would have made me look at it. … I’ve gone back and read my notes about things that we’ve talked about… she has changed my thinking on so many important things [which] has really helped …going forward. And then that does change things like the physical aspect and the nutrition, because I’m looking at it from a different lens.” |
| “The main thing that the life coach kind of instilled on me [was] that you have to kind of put yourself first because if you don’t then everyone else kind of suffers too, so it’s the biggest thing that I took away from it.” |
| “[My coach] encouraged me to do some journaling… and I’ve continued to do that. And then she just gave me some just tips on how to, how to get that motivation going again so when it starts to get to a low period, what to do to kind of kick start that.” |
| Impact on Own and Family’s Nutrition |
| ● Meal preparation |
| “[Meal preparation] saved me a lot of time and energy just making things simpler, knowing my family’s eating better. I’m not running to the grocery store every other day trying to grab stuff to eat. So, [the program] just improved our life in a lot of ways.” |
| “We go grocery shopping on Saturday and buy everything we need for the week, so there’s no stress that way. … And it is something that I’ll just continue, because it works well for our family. … We know exactly what’s there, and some of the things I will prep on the weekends, and so it’s easier to then cook on the weekday.” |
| “We were a big granola bar family or cookies or chips, the things that are really super high in carbohydrates, and quick to grab. But if we do meal prep, then we’re a lot faster to grab like a salad or some vegetables that are already cut, or fruit.” |
| Barriers |
| ● Stress |
| “Probably more than 6 months ago I was going to the gym more often, and making a better effort with my diet, and making sure my daughter was getting more activity as well. And now it just, because of time constraints, and probably a bit of stress, and probably a bit of anxiety, it’s sort of slid back a bit. … Eating has been a challenge and we’ve definitely been relying a little more on restaurants than we want to.” |
| “I still notice when I’m stressed, I do eat a lot and then it doesn’t help and then when I get sick … I use that as an excuse to like not do anything. … It’s … that habit-forming thing, you have to do it for um at least 21 days before it sticks. And so, I have to just get back in to that and stick with it.” |
| ● Motivation |
| “As I’m watching the leaves start to change I can feel … excuses starting, like, ‘Oh, well I could put something in my lunch time so I don’t have to go for that walk.’ …[T]hose excuses … won’t better myself, but it’s a pattern I’ve always done and it’s very normal for myself. But I’m trying to go against those and work against what my natural inclination to continue those walks.” |
| ● Time |
| “One of the biggest challenges is now [my children] have something every single evening, and we are literally flying from where I pick them up at their after-school program, home, eat dinner, and then out to something for them. They continue to stay active. … But that forces me to go and be sedentary most of the time, at their things, watching them be part of those fun activities.” |
| Prevention |
|---|
| ● Habits in child |
| “[I am] trying to develop health habits long-term so that when [my child is] a teenager, [and] he has more access to food, that he makes good choices.” |
| “I think [I am] realizing that my decisions, and [the] behaviour [I] model for [my child] could… become a struggle, and I don’t want that for her. … Now [I’m] realizing that my decisions aren’t only decisions for me. And I think that’s been probably the biggest part [that helped with behaviour change], is realizing I don’t want her to ever [struggle with health].” |
| ● Developing adverse health effects |
| “Some of the questions [in the questionnaires] about your like physical things like ‘has this stopped you from doing this?’ I never thought at my age [that I would] answer yes to those things but like I was literally [having] a hard time getting off the floor.” |
| “I am getting older and my health may deteriorate outside of my control, so the things I can control I feel like I should control like keep my weight down, keep my heart active.” |
| Changed Perspective |
| ● Toward behaviour change |
| “I don’t have any resounding health issues. So, I feel like that’s almost been an excuse. ‘Well, it’s not that bad. I don’t have high cholesterol, I don’t have diabetes, I don’t have thyroid issues.’ And I think I needed to get past that mind frame of thinking it’s not that bad, and being like, ‘You know what? I’m not happy with what I see in the mirror, and I need to change that. And the only person that can change that is me.’” |
| “I do have to give myself a little bit of credit. I am doing a much better job [of being healthier] than I have previously. … This year my goal [was] living a healthier lifestyle. So I didn’t choose the, ‘I’m gonna join a gym and lose weight,’ I chose the overall healthier lifestyle.” |
| ● Prioritized themselves |
| “I try to make sure I carve out ‘me time’ in the day [now], so if they choose to join, that’s awesome.” |
| “Cardio helps me a lot, because I make that my time. … I’ll listen to a podcast, or I’ll watch YouTube. … Zone everyone else out. … [Which helps with my mental health]… It helps me sleep better, too, which is great.” |
| ● Improved mindset |
| “I think that it [was] maybe not necessarily the nutritional information and stuff I was watching, but kind of the subliminal messages of, ‘You don’t need to be afraid of [changing behaviours].’ And, people aren’t viewing you and judging you the way you are judging yourself. So I think that has kind of been my biggest takeaway from the whole process.” |
| “Exercise makes me relax. … Before I [was] always fighting with everybody and I was so stressed. … And now, I started going to the gym and whenever I’m stressed I just go and run … and I come [home] like new. So I think that’s what helps me [continue with behaviour change].” |
| Barriers |
| ● Motivation |
| “Before I had like more time to focus on [health behaviours], and that was my focus and like being somebody that has grown up with weight issues it always has to be a focus. … Like I’m not going to wake up one day and… be like I really feel like a kale salad right now. … So it has to really be a conscious decision for me… to eat in a healthy mindful way. … And I just haven’t been in that mind set right now.” |
| “[It has been] just like super busy time at [work] right now. Like I didn’t even stop today for lunch. … It [has] just been crazy. … [But] hard it’s that like cognitive dissonance like I know I should be [eating better and being physically active] and then I’m not doing it, and then I feel guilty because I know I should be doing it, and I’m not doing it.” |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karmali, S.; Battram, D.S.; Burke, S.M.; Cramp, A.; Johnson, A.M.; Mantler, T.; Morrow, D.; Ng, V.; Pearson, E.S.; Petrella, R.J.; et al. Perspectives and Impact of a Parent-Child Intervention on Dietary Intake and Physical Activity Behaviours, Parental Motivation, and Parental Body Composition: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 6822. https://doi.org/10.3390/ijerph17186822
Karmali S, Battram DS, Burke SM, Cramp A, Johnson AM, Mantler T, Morrow D, Ng V, Pearson ES, Petrella RJ, et al. Perspectives and Impact of a Parent-Child Intervention on Dietary Intake and Physical Activity Behaviours, Parental Motivation, and Parental Body Composition: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(18):6822. https://doi.org/10.3390/ijerph17186822
Chicago/Turabian StyleKarmali, Shazya, Danielle S. Battram, Shauna M. Burke, Anita Cramp, Andrew M. Johnson, Tara Mantler, Don Morrow, Victor Ng, Erin S. Pearson, Robert J. Petrella, and et al. 2020. "Perspectives and Impact of a Parent-Child Intervention on Dietary Intake and Physical Activity Behaviours, Parental Motivation, and Parental Body Composition: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 18: 6822. https://doi.org/10.3390/ijerph17186822
APA StyleKarmali, S., Battram, D. S., Burke, S. M., Cramp, A., Johnson, A. M., Mantler, T., Morrow, D., Ng, V., Pearson, E. S., Petrella, R. J., Tucker, P., & Irwin, J. D. (2020). Perspectives and Impact of a Parent-Child Intervention on Dietary Intake and Physical Activity Behaviours, Parental Motivation, and Parental Body Composition: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 17(18), 6822. https://doi.org/10.3390/ijerph17186822