Life Expectancy in Chinese Cities: Spatially Varied Role of Socioeconomic Development, Population Structure, and Natural Conditions



Abstract
1. Introduction
2. Literature Review
3. Study Area, Data, and Methods
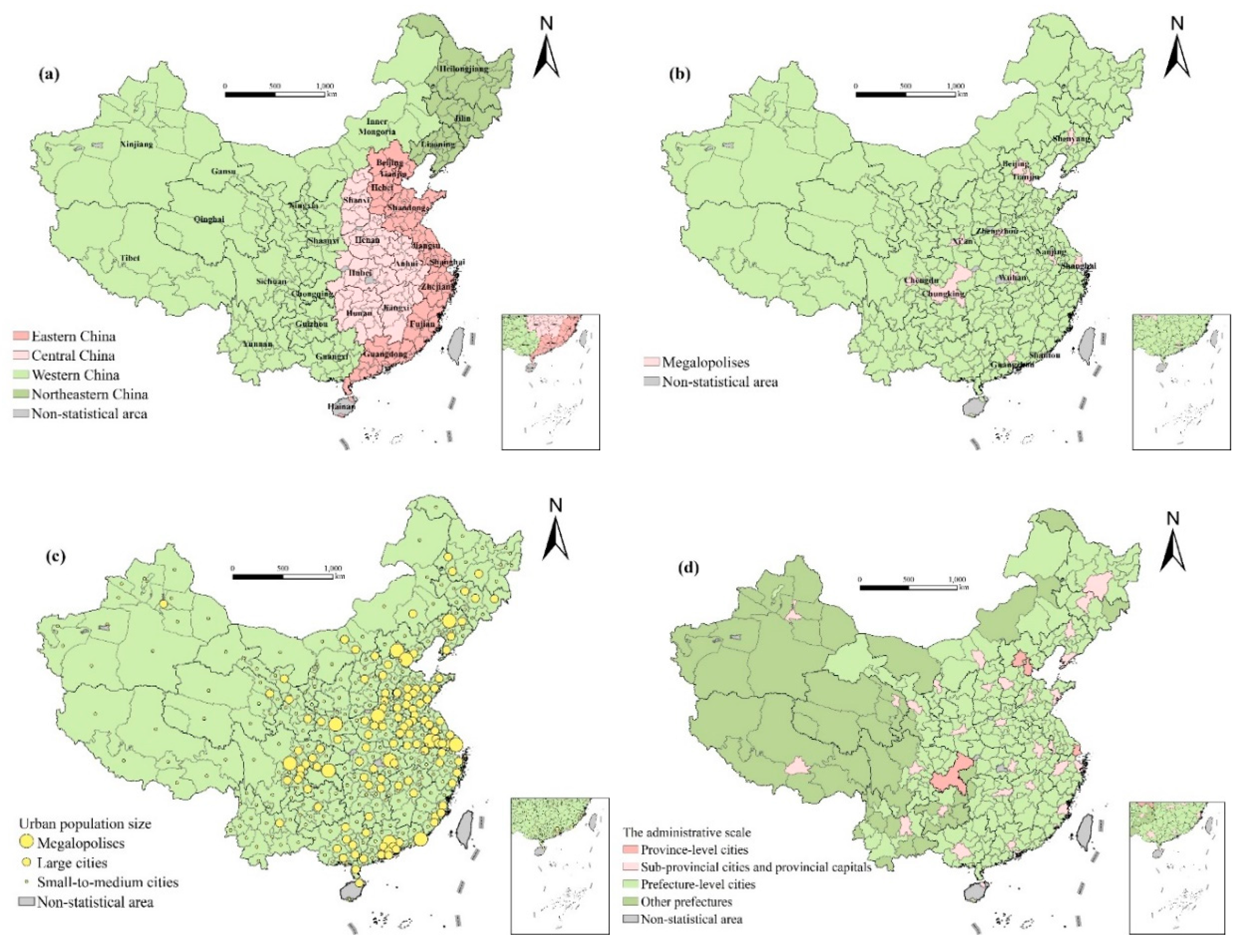
3.1. Study Area
3.2. Data
3.3. Calculation of Life Expectancy
- (1)
- Calculating age-specific mortality rate nmx:nmx = DX/PX
- (2)
- Calculating age-specific probability of death nqx:nqx = 1 − , is the empirical value, according to Reed–Merrell, = 0.008.
- (3)
- Calculating age-specific number of survivors lx and deaths 5dx, assuming l0 = 100,000. 5dx = lx × 5qx, lx+5 = lx−5 dx
- (4)
- Calculating total person-years of survival TxThe values of each group aged 10 years and above were calculated from the higher age group by the following formula: Tx = −0.20833lx−5 + 2.5lx + 0.20833lx+5 + 5
- (5)
- Calculating person-years of survival 5 Lx:L0 = 0.276l0 + 0.724l1L1 = 0.410l0 + 0.590l25 L5 = −0.003l0 + 2.242l5 + 2.761l105 Lx = Tx − Tx+5
- (6)
- Calculating life expectancy Tx/lx
3.4. Spatial Autocorrelation
3.4.1. Global Moran’s I index
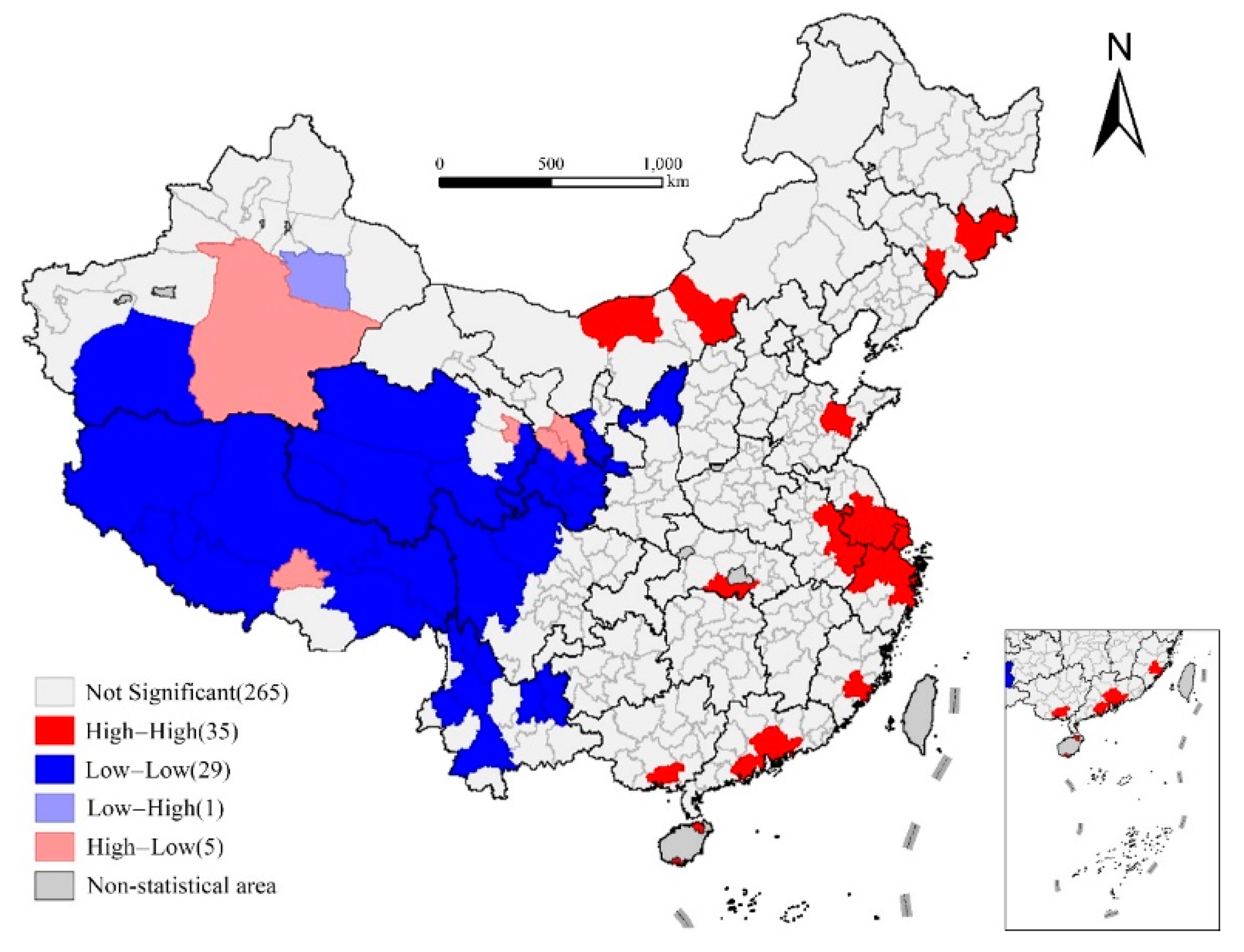
3.4.2. Local Moran’s I index
3.5. Empirical Model
3.5.1. Influencing Factors and Variable Selection
3.5.2. Geographically Weighted Regression Model
4. Results
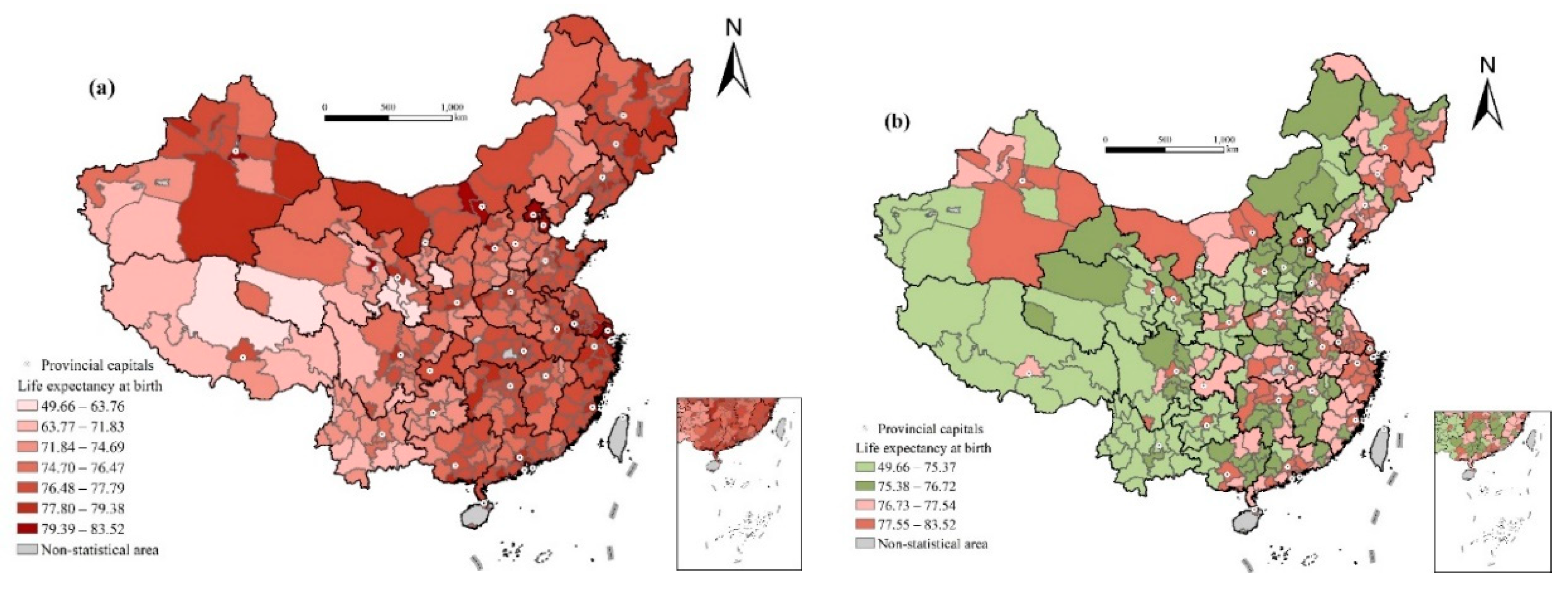
4.1. Spatial Distribution Characteristics of Life Expectancy in Prefecture-Level Cities
4.2. Analysis of Factors Influencing Life Expectancy
4.2.1. Influence of Economic Development Level
4.2.2. Influence of Medical Conditions
4.2.3. Influence of Demographic Structure
4.2.4. Influence of Natural Environment
4.2.5. Influence of City Attributes
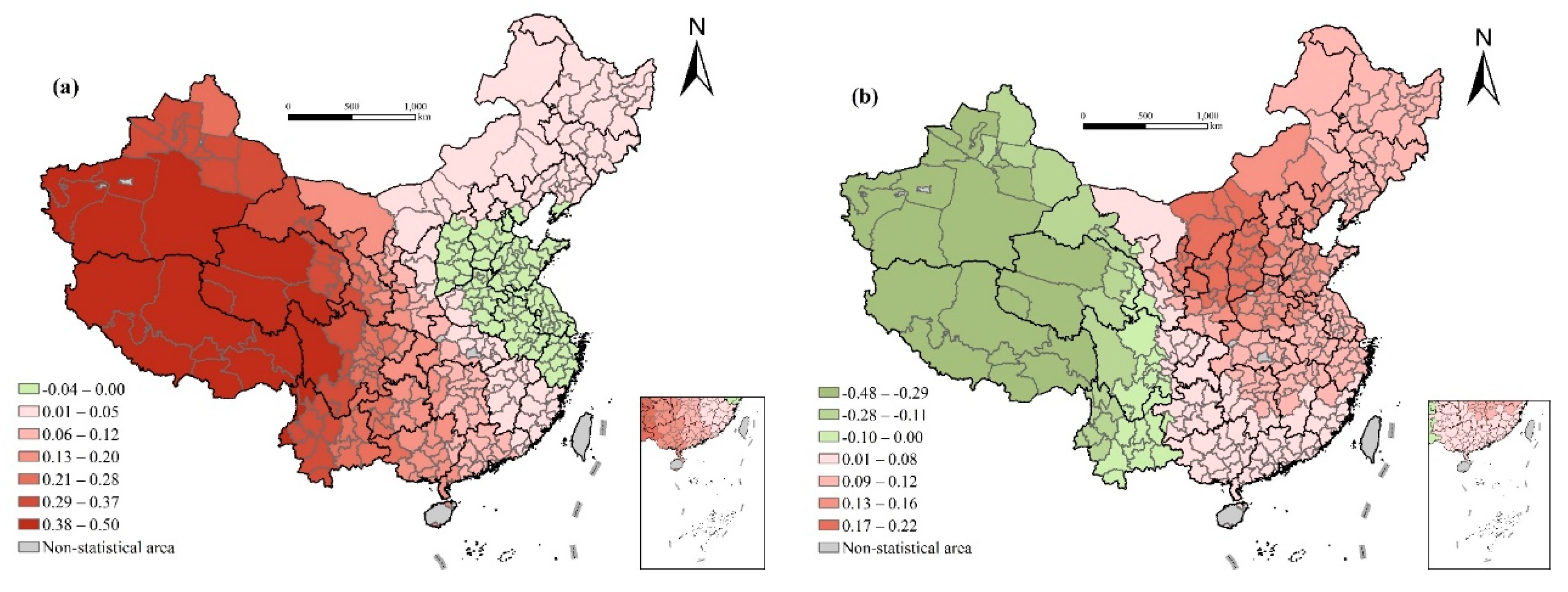
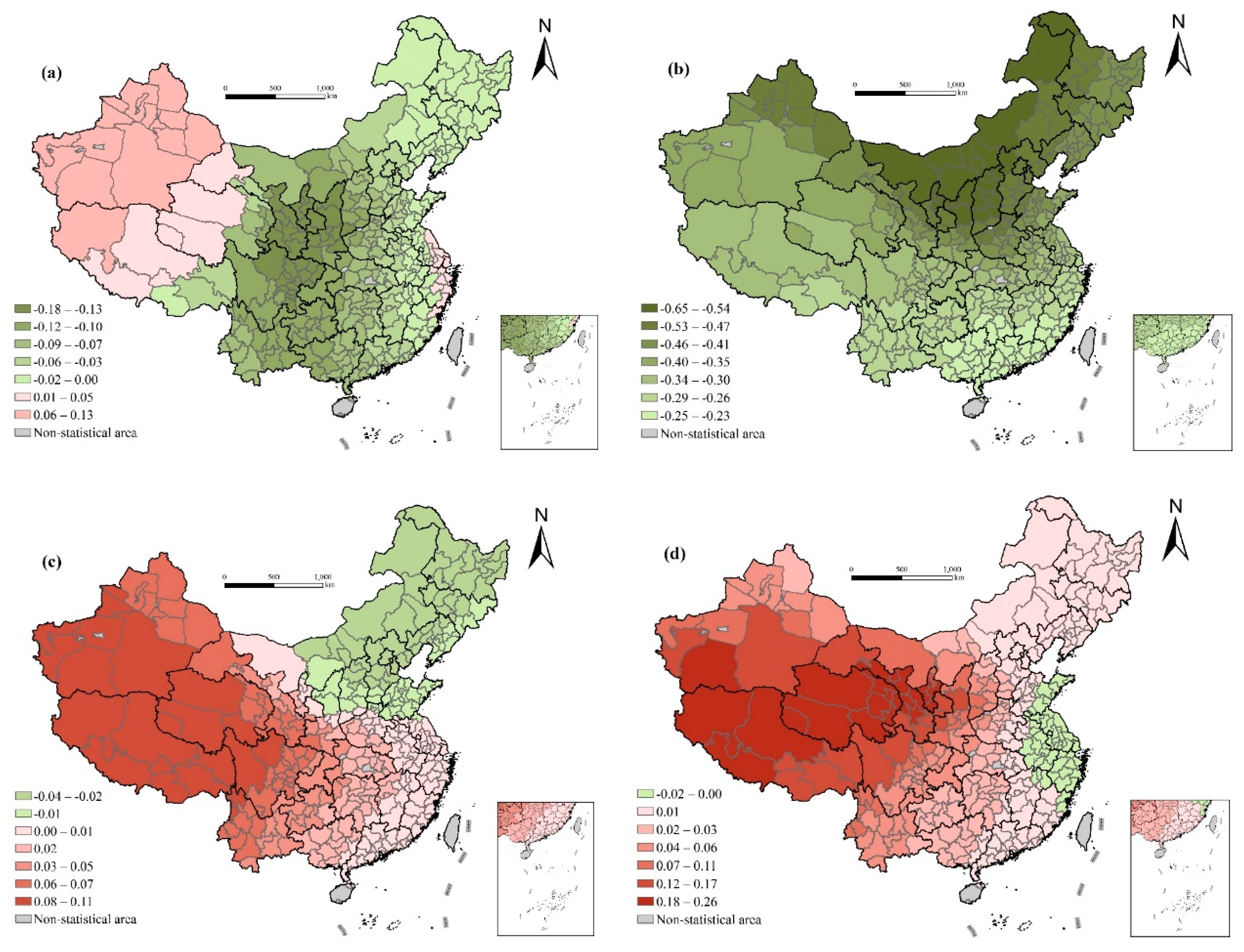
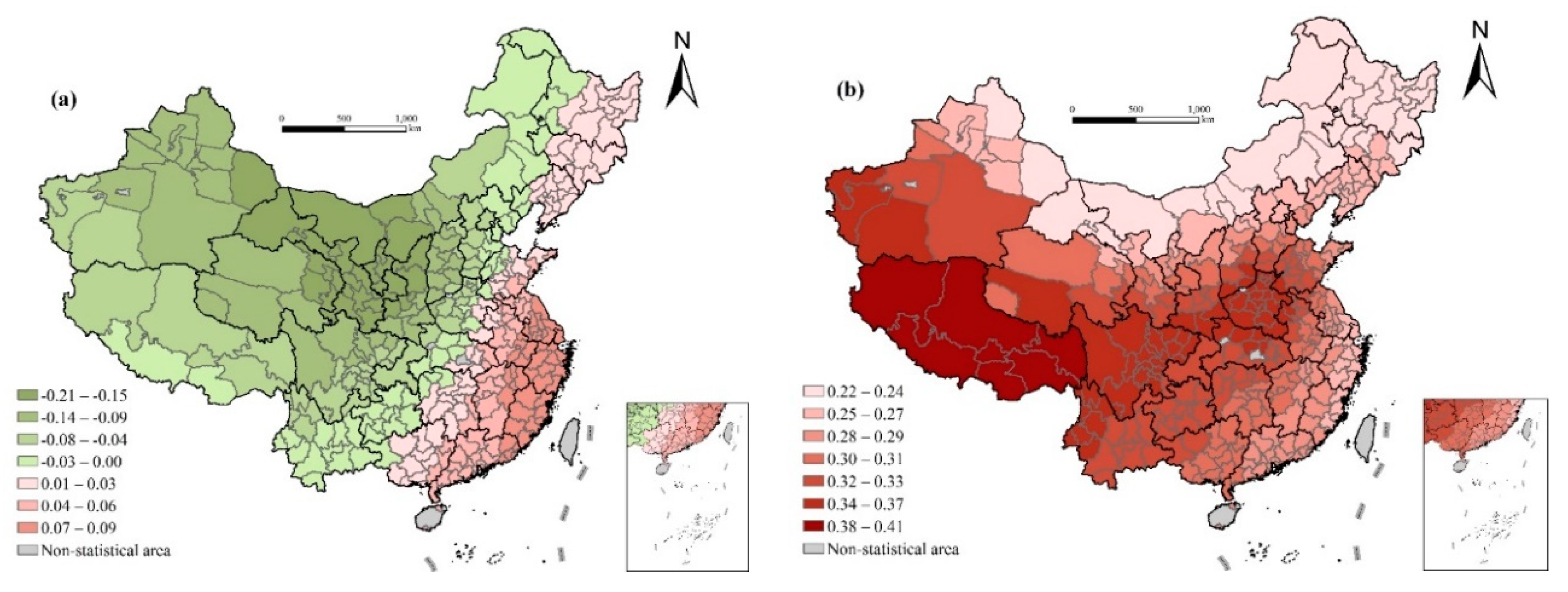
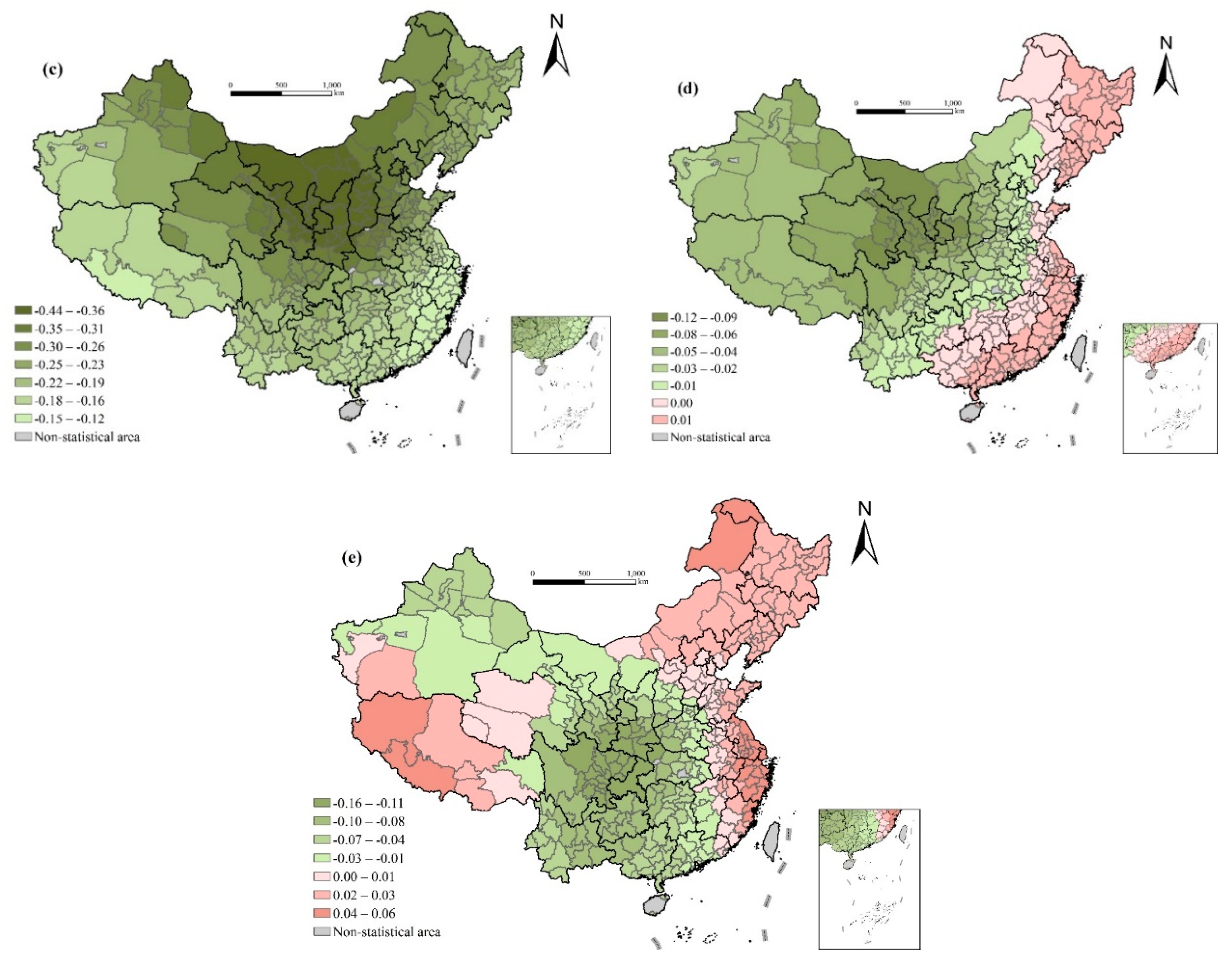
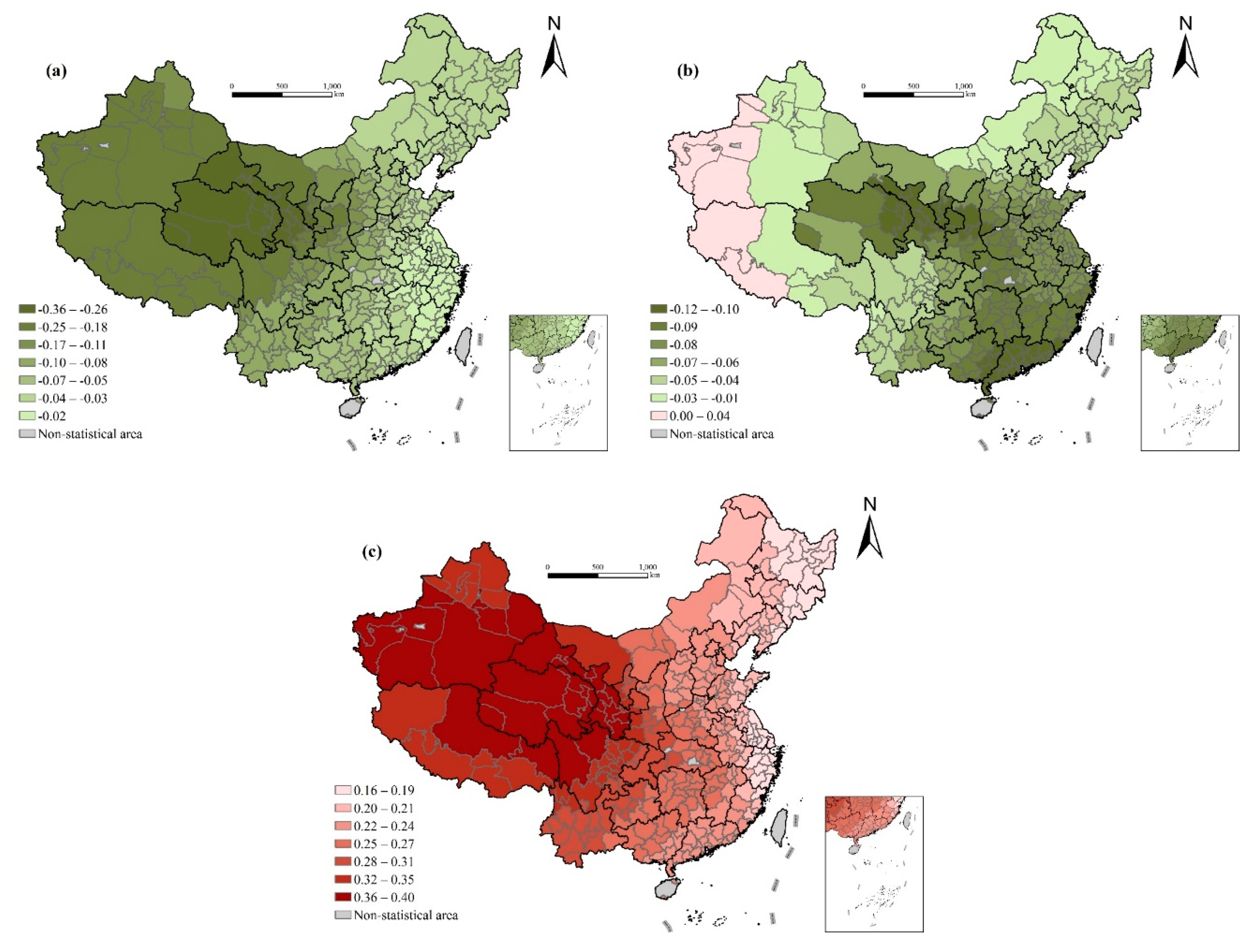
4.3. Spatial Variation of Dominant Factors
5. Conclusions and Policy Implications
Author Contributions
Funding
Conflicts of Interest
References
- Wu, Y.; Hu, K.; Han, Y.; Sheng, Q.; Fang, Y. Spatial Characteristics of Life Expectancy and Geographical Detection of Its Influencing Factors in China. Int. J. Environ. Res. Public Health 2020, 17, 906. [Google Scholar] [CrossRef] [PubMed]
- UN. United Nations Sustainable Development Goals. 2015. Available online: https://www.un.org/sustainabledevelopment/zh/ (accessed on 9 September 2020).
- Woods, L.M.; Rachet, B.; Riga, M.; Stone, N.; Shah, A.; Coleman, M.P. Geographical variation in life expectancy at birth in England and Wales is largely explained by deprivation. J. Epidemiol. Community Health 2005, 59, 115–120. [Google Scholar] [CrossRef]
- Okamoto, K. Life expectancy at the age of 65 years and environmental factors: An ecological study in Japan. Arch. Gerontol. Geriatr. 2006, 43, 85–91. [Google Scholar] [CrossRef] [PubMed]
- HCAPC. Health China Action Promotion Committee: Healthy China Initiative 2019–2030. Available online: http://www.gov.cn/xinwen/2019-07/15/content_5409694.htm (accessed on 9 September 2020).
- Cockerham, W.C. The social determinants of the decline of life expectancy in Russia and Eastern Europe: A lifestyle explanation. J. Health Soc. Behav. 1997, 38, 117–130. [Google Scholar] [CrossRef]
- Lin, C.C.; Rogot, E.; Johnson, N.J.; Sorlie, P.D.; Arias, E. A further study of life expectancy by socioeconomic factors in the National Longitudinal Mortality Study. Ethn. Dis. 2003, 13, 240–247. [Google Scholar]
- Perenboom, R.J.M.; van Herten, L.M.; Boshuizen, H.C.; van den Bos, G.A.M. Life expectancy without chronic morbidity: Trends in gender and socioeconomic disparities. Public Health Rep. 2005, 120, 46–54. [Google Scholar] [CrossRef]
- Meara, E.R.; Richards, S.; Cutler, D.M. The gap gets bigger: Changes on mortality and life expectancy, by education, 1981–2000. Health Aff. 2008, 27, 350–360. [Google Scholar] [CrossRef]
- Leon, D.A. Trends in European life expectancy: A salutary view. Int. J. Epidemiol. 2011, 40, 271–277. [Google Scholar] [CrossRef]
- Pickett, K.E.; Wilkinson, R.G. Income inequality and health: A causal review. Soc. Sci. Med. 2015, 128, 316–326. [Google Scholar] [CrossRef]
- Kim, J.I.; Kim, G. Country-Level Socioeconomic Indicators Associated with Healthy Life Expectancy: Income, Urbanization, Schooling, and Internet Users: 2000–2012. Soc. Indic. Res. 2016, 129, 391–402. [Google Scholar] [CrossRef]
- Li, R.; Tan, J.; Wang, W.; He, Y. The yearly change and regional difference of population life-span in China. Hum. Geogr. 2000, 15, 1–6. [Google Scholar]
- Guo, Y. Analysis of spatio-temporal changes in life expectancy and its influencing factors in China. Chin. J. Health Policy 2018, 11, 44–49. [Google Scholar]
- SCPRC. The State Council of the People’s Republic of China: The 13th Five-Year Plan on Hygiene and Health. 2016. Available online: http://www.gov.cn/zhengce/content/2017-01/10/content_5158488.htm (accessed on 9 September 2020).
- NBS. National Bureau of Statistics: Notice of the Sixth National Census. 2011. Available online: http://www.stats.gov.cn/ztjc/zdtjgz/zgrkpc/dlcrkpc/dlcrkpczl/index_1.html (accessed on 9 September 2020).
- Ma, L.J.C. Urban administrative restructuring, changing scale relations and local economic development in China. Political Geogr. 2005, 24, 477–497. [Google Scholar] [CrossRef]
- Wei, H. Administrative Hierarchy and Growth of City Scale in China. Urban Environ. Stud. Chin. 2014, 1, 4–17. [Google Scholar]
- Li, H.; Wei, Y.D.; Liao, F.H.; Huang, Z. Administrative hierarchy and urban land expansion in transitional China. Appl. Geogr. 2015, 56, 177–186. [Google Scholar] [CrossRef]
- Shkolnikov, V.M.; Andreev, E.M.; Jasilionis, D.; Leinsalu, M.; Antonova, O.I.; McKee, M. The changing relation between education and life expectancy in central and eastern Europe in the 1990s. J. Epidemiol. Community Health 2006, 60, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.-T.; Chen, Y.-M.; Chien, L.-C.; Chan, C.-C. Political and social determinants of life expectancy in less developed countries: A longitudinal study. BMC Public Health 2012, 12, 85. [Google Scholar] [CrossRef]
- Renton, A.; Wall, M.; Lintott, J. Economic growth and decline in mortality in developing countries: An analysis of the World Bank development datasets. Public Health 2012, 126, 1–10. [Google Scholar] [CrossRef]
- Singh, G.K.; Siahpush, M. Widening Rural-Urban Disparities in Life Expectancy, US, 1969–2009. Am. J. Prev. Med. 2014, 46, E19–E29. [Google Scholar] [CrossRef]
- Gilligan, A.M.; Skrepnek, G.H. Determinants of life expectancy in the Eastern Mediterranean Region. Health Policy Plan. 2015, 30, 624–637. [Google Scholar] [CrossRef]
- Manuel, D.G.; Perez, R.; Sanmartin, C.; Taljaard, M.; Hennessy, D.; Wilson, K.; Tanuseputro, P.; Manson, H.; Bennett, C.; Tuna, M.; et al. Measuring Burden of Unhealthy Behaviours Using a Multivariable Predictive Approach: Life Expectancy Lost in Canada Attributable to Smoking, Alcohol, Physical Inactivity, and Diet. PLoS Med. 2016, 13, e1002082. [Google Scholar] [CrossRef] [PubMed]
- Duque, A.M.; Peixoto, M.V.; Lima, S.V.M.A.; Goes, M.A.O.; Santos, A.D.; Gomes Machado Araujo, K.C.; Nunes, M.A.P. Analysis of the relationship between life expectancy and social determinants in a north-eastern region of Brazil, 2010–2017. Geospat. Health 2018, 13, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Luo, L.; Xu, P.; Wang, P. How does social development influence life expectancy? A geographically weighted regression analysis in China. Public Health 2018, 163, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, R.G. Unhealthy Societies: The Afflictions of Inequality; Routledge: London, UK, 1996. [Google Scholar]
- Inglebart, R.; Welzel, C. How development leads to democracy what we know about modernization. Foreign Aff. 2009, 88, 33. [Google Scholar]
- Gong, S.; Chen, Y.; Zhang, T.; Zhang, Z. The correlation between life expectancy and per capita GDP in China from 1990 to 2010 and its changing characteristics. Econ. Geogr. 2020, 40, 23–30, 51. [Google Scholar]
- Anand, S.; Ravallion, M. Human Development in Poor Countries: On the Role of Private Incomes and Public Services. J. Econ. Perspect. 1993, 7, 133–150. [Google Scholar] [CrossRef]
- Elo, I.T.; Beltran-Sanchez, H.; Macinko, J. The Contribution of Health Care and Other Interventions to Black-White Disparities in Life Expectancy, 1980–2007. Popul. Res. Policy Rev. 2014, 33, 97–126. [Google Scholar] [CrossRef]
- Lu, X.; Chen, X. Factors on mean lifespan of each province in china. Yunnan Geogr. Environ. Res. 2007, 2, 72–79. [Google Scholar]
- Feng, Z.; Tang, Y.; Yang, Y.; Zhang, D. The Relief Degree of Land Surface in China and Its Correlation with Population Distribution. Acta Geogr. Sin. 2007, 62, 1073–1082. [Google Scholar]
- Song, W.; Li, Y.; Hao, Z.; Li, H.; Wang, W. Public health in China: An environmental and socio-economic perspective. Atmos. Environ. 2016, 129, 9–17. [Google Scholar] [CrossRef]
- Qin, J.; Yu, G.; Xia, T.; Li, Y.; Liang, X.; Wei, P.; Long, B.; Lei, M.; Wei, X.; Tang, X.; et al. Spatio-Temporal Variation of Longevity Clusters and the Influence of Social Development Level on Lifespan in a Chinese Longevous Area (1982–2010). Int. J. Environ. Res. Public Health 2017, 14, 812. [Google Scholar] [CrossRef]
- Zha, X.; Tian, Y.; Gao, X.; Wang, W.; Yu, C. Quantitatively evaluate the environmental impact factors of the life expectancy in Tibet, China. Environ. Geochem. Health 2019, 41, 1507–1520. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, Y.; Li, H.; Holdaway, J.; Hao, Z.; Wang, W.; Krafft, T. Regional aging and longevity characteristics in China. Arch. Gerontol. Geriatr. 2016, 67, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Yang, D. A Study on Ambient Air Quality’s Effects on Public Health in China:Based on Comparative Analysis with G20. Popul. Econ. 2018, 15, 1471. [Google Scholar]
- Zhou, R.; Zhuang, R.; Huang, C. Pattern evolution and formative mechanism of aging in China. Acta Geogr. Sin. 2019, 74, 2163–2177. [Google Scholar]
- Wang, S. Life Expectancy Decomposition and it’s Influencing Factors Analysis:Based on Provincial Panel Data. Northwest Popul. J. 2014, 35, 37–42. [Google Scholar]
- Ming, Y.; Dong, Z. Life expectancy of China’s population analysis of the impact of factors. Theory Res. 2010, 4, 47–50. [Google Scholar]
- Reed, L.J.; Merrell, M. A short method for constructing an abridged life table. Am. J. Hyg. 1939, 30, 32–62. [Google Scholar]
- Ni, J. Research on the Life expectancy of Chinese population. Chin. J. Health Stat. 1985, 1, 6–9. [Google Scholar]
- Le Gallo, J.; Ertur, C. Exploratory spatial data analysis of the distribution of regional per capita GDP in Europe, 1980–1995. Pap. Reg. Sci. 2003, 82, 175–201. [Google Scholar] [CrossRef]
- Anselin, L. Local indicators of spatial association—LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Fotheringham, A.; Brunsdon, C.; Charlton, M. Geographically Weighted Regression: The Analysis of Spatially Varying Relationships; Wiley: Hoboken, NJ, USA, 2003. [Google Scholar]
- Ma, L.; Yu, Z. Analysis of influencing factors of average life expectancy in China. Econ. Res. Guide 2009, 9, 161–162. [Google Scholar]
- Zheng, C. Analysis of regional differences and economic and social influencing factors of life expectancy. China Collect. Econ. 2010, 19, 81–83. [Google Scholar]
- Moore, M.; Gould, P.; Keary, B.S. Global urbanization and impact on health. Int. J. Hyg. Environ. Health 2003, 206, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Liu, H.; Wang, X. Spatio-temporal variations of population health distribution in China and its influencing factors. World Reg. Stud. 2017, 26, 161–168. [Google Scholar]
- Ming, Y. Trends and regional differences of infant mortality in China. Popul. Res. 2009, 33, 77–87. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Variables | Mean | Std. Dev. | Min | Max |
|---|---|---|---|---|---|
| Dependent Variables | |||||
| Life expectancy | 76 | 3.45 | 49.66 | 83.52 | |
| Independent Variables | |||||
| Economic development | Per capita GDP (ln) | 10.16 | 0.64 | 8.55 | 11.84 |
| Urbanization rate | 46.51% | 17.13% | 12.69% | 100.00% | |
| Medical conditions | Health care | 4.33 | 1.38 | 1.3 | 9.61 |
| Infant mortality rate | 0.51% | 0.60% | 0.02% | 6.75% | |
| Per capita health expenditure (ln) | 5.78 | 0.37 | 4.17 | 7.27 | |
| Road density | 90.99 | 81.11 | 0.43 | 1156.65 | |
| Demographic structure | Aging rate | 8.63% | 1.93% | 1.79% | 16.50% |
| Average years of education | 8.75 | 1.11 | 3.47 | 11.71 | |
| Average household size | 3.18 | 0.46 | 2.11 | 5.55 | |
| Sex ratio | 105.49 | 4.22 | 89.65 | 132.58 | |
| The proportion of migrants | 4.74% | 8.13% | 0.11% | 64.87% | |
| Natural environment | Average annual PM2.5 concentration | 33.89 | 18.13 | 2.09 | 74.79 |
| Average altitude (ln) | 5.77 | 1.59 | 0.26 | 8.53 | |
| Perennial mean temperature | 12.96 | 6.56 | −3.52 | 25.54 | |
| City attributes | Urban population size (ln) | 4.3 | 0.98 | 0.78 | 7.34 |
| The city located in Central China | CC = 1 (frequency: 82), else = 0 | ||||
| The city located in Northeastern China | NC = 1 (36), else = 0 | ||||
| The city located in Eastern China | EC = 1 (87), else = 0 | ||||
| Prefecture-level cities | PREC = 1 (250), else = 0 | ||||
| Sub-provincial cities and provincial capitals | SUB_PRO/PRO = 1 (32), else = 0 | ||||
| Province-level cities | PROC = 1 (4), else = 0 | ||||
| Variables | Moran’s I | Z(I) | P |
|---|---|---|---|
| Life expectancy | 0.424 | 12.535 | 0.001 |
| Per capita GDP | 0.396 | 11.961 | 0.001 |
| Urbanization rate | 0.402 | 12.107 | 0.001 |
| Health care | 0.292 | 8.627 | 0.001 |
| Infant mortality rate | 0.434 | 13.48 | 0.001 |
| Per capita health expenditure | 0.402 | 11.942 | 0.001 |
| Road density | 0.245 | 8.962 | 0.001 |
| Aging rate | 0.644 | 19.003 | 0.001 |
| Average years of education | 0.533 | 15.784 | 0.001 |
| Average household size | 0.572 | 16.677 | 0.001 |
| Sex ratio | 0.425 | 12.233 | 0.001 |
| The proportion of migrants | 0.572 | 17.165 | 0.001 |
| Average annual PM2.5 concentration | 0.894 | 26.035 | 0.001 |
| Average altitude | 0.905 | 27.102 | 0.001 |
| Perennial mean temperature | 0.933 | 26.908 | 0.001 |
| Urban population size | 0.086 | 2.742 | 0.013 |
| Prefecture-level cities | 0.276 | 8.136 | 0.001 |
| Sub-provincial cities and provincial capitals | −0.081 | −2.218 | 0.007 |
| Province-level cities | 0.087 | 2.814 | 0.032 |
| Variables | Standardized Coefficient | ||
|---|---|---|---|
| Model 1 | Model 2 | Model 3 | |
| Per capita GDP (ln) | 0.111 * | 0.162 ** | |
| (0.341) | (0.382) | ||
| Urbanization rate | 0.002 | −0.026 | |
| (0.014) | (0.015) | ||
| Health care | 0.012 | −0.004 | |
| (0.155) | (0.164) | ||
| Infant mortality rate | −0.335 *** | −0.336 *** | |
| (0.253) | (0.263) | ||
| Per capita health expenditure (ln) | 0.007 | 0.007 | |
| (0.443) | (0.499) | ||
| Road density | −0.004 | 0.001 | |
| (0.002) | (0.002) | ||
| Aging rate | 0.013 | 0.029 | |
| (0.106) | (0.112) | ||
| Average years of education | 0.290 *** | 0.272 *** | |
| (0.219) | (0.224) | ||
| Average household size | −0.204 *** | −0.196 *** | |
| (0.473) | (0.488) | ||
| Sex ratio | −0.004 | −0.014 | |
| (0.038) | (0.040) | ||
| The proportion of migrants | −0.027 | 0.010 | |
| (0.024) | (0.027) | ||
| Average annual PM2.5 concentration | −0.095 | −0.117 | |
| (0.013) | (0.014) | ||
| Average altitude (ln) | −0.081 | −0.073 | |
| (0.137) | (0.156) | ||
| Perennial mean temperature | 0.208 *** | 0.234 *** | |
| (0.026) | (0.033) | ||
| Urban population size (ln) | 0.014 | 0.039 | |
| (0.197) | (0.238) | ||
| The city located in Central China | 0.195 *** | 0.062 | |
| (0.440) | (0.396) | ||
| The city located in Northeastern China | 0.173 *** | 0.045 | |
| (0.564) | (0.626) | ||
| The city located in Eastern China | 0.260 *** | −0.035 | |
| (0.438) | (0.460) | ||
| Prefecture-level cities | 0.384 *** | −0.044 | |
| (0.503) | (0.487) | ||
| Sub-provincial cities and provincial capitals | 0.452 *** | −0.028 | |
| (0.688) | (0.75) | ||
| Province-level cities | 0.177 *** | −0.020 | |
| (1.534) | (1.458) | ||
| Constant | 72.053 *** | 67.514 *** | 65.54 *** |
| (0.410) | (6.120) | (6.597) | |
| Adj-R-squared | 0.298 | 0.631 | 0.630 |
| F | 24.755 | 39.173 | 28.123 |
| Variables | Standardized Coefficient | |||
|---|---|---|---|---|
| Eastern | Central | Western | Northeastern | |
| Per capita GDP (ln) | 0.057 | 0.269 | 0.330 ** | 0.272 |
| (−0.324) | (−0.427) | (−1.038) | (−0.667) | |
| Urbanization rate | −0.026 | 0.103 | −0.182 | 0.558 |
| (−0.009) | (−0.026) | (−0.042) | (−0.038) | |
| Health care | 0.183 | 0.236 | 0.021 | −0.368 |
| (−0.132) | (−0.185) | (−0.322) | (−0.415) | |
| Infant mortality rate | −0.260 *** | −0.106 | −0.305 *** | −0.001 |
| (−0.844) | (−0.480) | (−0.454) | (−2.467) | |
| Per capita health expenditure (ln) | −0.116 | −0.004 | 0.016 | 0.535 * |
| (−0.330) | (−0.542) | (−1.120) | (−1.509) | |
| Road density | 0.062 | −0.325 ** | 0.035 | −0.904 * |
| (−0.002) | (−0.004) | (−0.003) | (−0.02) | |
| Aging rate | 0.177 | 0.605 *** | −0.091 | 0.572 * |
| (−0.084) | (−0.117) | (−0.285) | (−0.227) | |
| Average years of education | 0.230 ** | 0.179 *** | 0.350 *** | 0.259 *** |
| (−0.198) | (−0.290) | (−0.462) | (−0.773) | |
| Average household size | −0.323 *** | 0.228 *** | −0.142 * | 0.749 |
| (−0.357) | (−0.638) | (−1.163) | (−2.058) | |
| Sex ratio | 0.046 | 0.079 | −0.094 | 0.027 |
| (−0.029) | (−0.036) | (−0.086) | (−0.16) | |
| The proportion of migrants | 0.302 ** | 0.123 | 0.023 | −0.065 |
| (−0.016) | (−0.170) | (−0.109) | (−0.131) | |
| Average annual PM2.5 concentration | −0.282 ** | 0.605 ** | −0.045 | 0.23 |
| (−0.009) | (−0.023) | (−0.047) | (−0.048) | |
| Average altitude (ln) | −0.194 * * | 0.095 | 0.041 | −0.296 |
| (−0.097) | (−0.266) | (−0.557) | (−0.272) | |
| Perennial mean temperature | 0.172 * | −0.009 *** | 0.302 *** | 0.249 *** |
| (−0.032) | (−0.05) | (−0.079) | (−0.149) | |
| Constant | 75.061 *** | 55.288 *** | 55.324 *** | 35.268 |
| (−5.950) | (−7.603) | (−16.988) | (−22.891) | |
| Adj-R-squared | 0.749 | 0.49 | 0.569 | 0.182 |
| F | 19.326 | 6.555 | 13.246 | 1.555 |
| Variables | Min | Lower Quartile | Median | Upper Quartile | Max | Average |
|---|---|---|---|---|---|---|
| Per capita GDP (ln) | −0.040 | −0.003 | 0.039 | 0.185 | 0.503 | 0.102 |
| Urbanization rate | −0.479 | 0.049 | 0.095 | 0.122 | 0.218 | 0.052 |
| Health care | −0.182 | −0.102 | −0.058 | −0.017 | 0.134 | −0.058 |
| Infant mortality rate | −0.648 | −0.460 | −0.354 | −0.280 | −0.232 | −0.375 |
| Per capita health expenditure (ln) | −0.038 | −0.012 | 0.005 | 0.030 | 0.112 | 0.013 |
| Road density | −0.018 | −0.001 | 0.009 | 0.046 | 0.256 | 0.035 |
| Aging rate | −0.207 | −0.067 | −0.005 | 0.034 | 0.088 | −0.023 |
| Average years of education | 0.215 | 0.267 | 0.299 | 0.330 | 0.414 | 0.298 |
| Average household size | −0.436 | −0.294 | −0.236 | −0.181 | −0.116 | −0.246 |
| Sex ratio | −0.117 | −0.041 | −0.010 | 0.003 | 0.011 | −0.023 |
| The proportion of migrants | −0.160 | −0.066 | −0.023 | 0.019 | 0.062 | −0.029 |
| Average annual PM2.5 concentration | −0.361 | −0.104 | −0.059 | −0.041 | −0.017 | −0.090 |
| Average altitude (ln) | −0.124 | −0.094 | −0.081 | −0.053 | 0.040 | −0.074 |
| Perennial mean temperature | 0.163 | 0.213 | 0.237 | 0.288 | 0.397 | 0.254 |
| Urban population size (ln) | 0.014 | 0.040 | 0.059 | 0.080 | 0.130 | 0.063 |
| Prefecture-level cities | −0.160 | −0.059 | −0.029 | 0.003 | 0.056 | −0.032 |
| Sub-provincial cities and provincial capitals | −0.173 | −0.078 | −0.040 | −0.023 | 0.166 | −0.042 |
| Province-level cities | −0.087 | −0.053 | −0.038 | −0.031 | −0.016 | −0.043 |
| Intercept | −0.087 | −0.063 | −0.047 | −0.038 | 0.033 | −0.046 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, D.; Yang, S.; Liu, T. Life Expectancy in Chinese Cities: Spatially Varied Role of Socioeconomic Development, Population Structure, and Natural Conditions. Int. J. Environ. Res. Public Health 2020, 17, 6597. https://doi.org/10.3390/ijerph17186597
Huang D, Yang S, Liu T. Life Expectancy in Chinese Cities: Spatially Varied Role of Socioeconomic Development, Population Structure, and Natural Conditions. International Journal of Environmental Research and Public Health. 2020; 17(18):6597. https://doi.org/10.3390/ijerph17186597
Chicago/Turabian StyleHuang, Daquan, Shuimiao Yang, and Tao Liu. 2020. "Life Expectancy in Chinese Cities: Spatially Varied Role of Socioeconomic Development, Population Structure, and Natural Conditions" International Journal of Environmental Research and Public Health 17, no. 18: 6597. https://doi.org/10.3390/ijerph17186597
APA StyleHuang, D., Yang, S., & Liu, T. (2020). Life Expectancy in Chinese Cities: Spatially Varied Role of Socioeconomic Development, Population Structure, and Natural Conditions. International Journal of Environmental Research and Public Health, 17(18), 6597. https://doi.org/10.3390/ijerph17186597