A Comparative Analysis of Health Impact Assessment Implementation Models in the Regions of Montérégie (Québec, Canada) and Nouvelle-Aquitaine (France)

 ,
, 
Abstract
1. Introduction
1.1. Health Impact Assessment in the Province of Québec and in France
1.1.1. A Gradual Emergence in Québec
1.1.2. A Growing Practice in France
1.2. Main Theme and Study Goal
2. Materials and Methods
3. Results
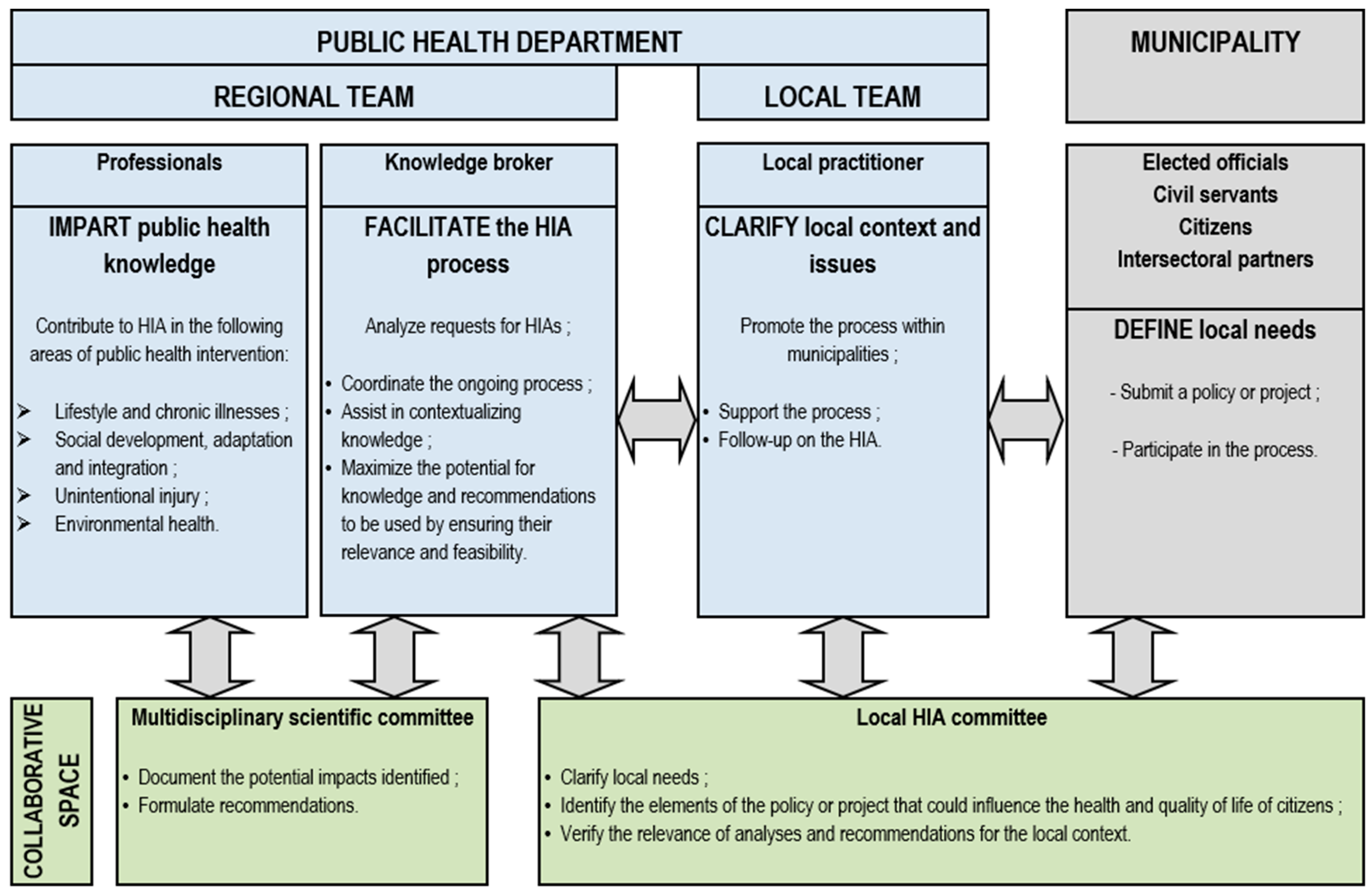
3.1. HIA Implementation Model in Montérégie
3.2. HIA Implementation Model in Nouvelle-Aquitaine
3.3. Cross-Comparison Analysis of the Two Implementation Models
4. Discussion
4.1. Influence of Governance Modes on Approach to HIA Implementation
4.1.1. Leadership and Sharing of Roles and Responsibilities
4.1.2. Degree of Stakeholder Incentivization and Buy-in
4.1.3. Resource Allocation and Capacity Building
4.1.4. Diversity of HIA Practitioners’ Profiles and Potential for Innovation
4.2. Two Implementation Schemes Inserted in Distinctive Contexts
4.2.1. Pre-Existing Structural Context
4.2.2. HIA Approaches and Underlying Representations
4.2.3. The Stance of the Regional Health Structures
4.3. Linkages with International Contexts
4.3.1. The Driving Role of the Health Sector
4.3.2. A Plurality of Organizations Fulfilling Several Functions
4.3.3. Effective and Clear Governance
4.4. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lerer, L.B. Health Impact Assessment. Health Policy Plan. 1999, 14, 198–203. [Google Scholar] [CrossRef]
- Dannenberg, A.L. Effectiveness of Health Impact Assessments: A Synthesis of Data from Five Impact Evaluation Reports. Prev. Chronic Dis. 2016, 13, 13. [Google Scholar] [CrossRef]
- Vanclay, F. Changes in the impact assessment family 2003–2014: Implications for considering achievements, gaps and future directions. J. Environ. Assess. Policy Manag. 2015, 17, 1550003. [Google Scholar] [CrossRef]
- Kemm, J.R. Health Impact Assessment Past Achievement, Current Understanding, and Future Progress; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Sohn, E.K.; Stein, L.J.; Wolpoff, A.; Lindberg, R.; Baum, A.; Simoncelli, A.M.-I.; Pollack, K.M. Avenues of Influence: The Relationship between Health Impact Assessment and Determinants of Health and Health Equity. J. Hered. 2018, 95, 754–764. [Google Scholar] [CrossRef]
- World Health Organization (Regional Office for Europe). Health and Safety Component of Environmental Impact Assessment; World Health Organization: Geneva, Switzerland, 1987. [Google Scholar]
- Lee, J.H.; Röbbel, N.; Dora, C. Analyse Transnationale Sur l’institutionnalisation de l’évaluation d’impact Sur La Santé. Genève. Available online: https://apps.who.int/iris/bitstream/handle/10665/128046/9789242505436_fre.pdf (accessed on 25 August 2020).
- Harris, P.; Harris, E. Differing forms, differing purposes: A typology of health impact assessment. Environ. Impact Assess. Rev. 2011, 31, 396–403. [Google Scholar] [CrossRef]
- Fakhri, A.; Maleki, M.; Gohari, M.; Harris, P. Investigating underlying principles to guide health impact assessment. Int. J. Health Policy Manag. 2014, 3, 17–22. [Google Scholar] [CrossRef]
- Brown, H.; Katscherian, D.; Spickett, J.; Maycock, B.; Hendrie, D. Health Impact Assessment Guidelines. Available online: https://www.google.com.hk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwjc2M34u9jrAhXQ-GEKHT9wBkcQFjAAegQIBRAB&url=http%3A%2F%2F152.91.79.30%2Finternet%2Fmain%2Fpublishing.nsf%2FContent%2FA12B57E41EC9F326CA257BF0001F9E7D%2F%24File%2FwHealth-Impact-Assessment-Guidelines.docx&usg=AOvVaw0WWlVG1rAC9jwO6dOeHlEw (accessed on 25 August 2020).
- Smits, P.; Préval, J.; Denis, J.-L. Prendre en compte la santé dans les politiques publiques. Étude d’un régime de gouvernementalité au Québec. Sci. Soc. Et St. Eacute 2016, 34, 45–70. [Google Scholar] [CrossRef]
- St-Pierre, L.; Mendell, A. L’implantation de l’ÉIS Au Canada: Le Projet Pilote ÉIS En Montérégie, Québec; Centre de collaboration nationale sur les politiques publiques et la santé. Available online: https://www.ccnpps.ca/100/Publications.ccnpps?id_article=665 (accessed on 25 August 2020).
- Diallo, T.; Freeman, S. Health impact assessment—Insights from the experience of Québec. Environ. Health Rev. 2020, 63, 6–13. [Google Scholar] [CrossRef]
- Le Gall, A.R.; Jabot, F. Health impact assessment on urban development projects in France: Finding pathways to fit practice to context. Glob. Health Promot. 2017, 24, 25–34. [Google Scholar] [CrossRef]
- Haut conseil de la santé publique. Pour Une Meilleure Intégration de La Santé Dans Les Documents de Planification Territoriale. Available online: https://www.hcsp.fr/explore.Cgi/avisrapportsdomaine?clefr=640 (accessed on 25 August 2020).
- Bhatia, R.; Farhang, L.; Heller, J.; Lee, M.; Orenstein, M.; Richerdson, M.; Wernham, A. Minimum Elements and Practice Standards for Health Impact Assessment, Version 3 (September 2014). Available online: https://pdfs.semanticscholar.org/040d/8ff2749f8ef2ec8b8233b7bffae9f7a38a12.pdf (accessed on 25 August 2020).
- Diallo, T.; Bize, R. Guide d’introduction à l’Évaluation d’Impact Sur La Santé En Suisse. Available online: https://serval.unil.ch/en/notice/serval:BIB_016D388FAC60 (accessed on 25 August 2020).
- Harris, P.J.; Harris-Roxas, B.F.; Kemp, L. Health impact assessment in urban settings. New South Wales Public Health Bull. 2007, 18, 149–150. [Google Scholar] [CrossRef]
- Linzalone, N.; Ballarini, A.; Piccinelli, C.; Viliani, F.; Bianchi, F. Institutionalizing Health Impact Assessment: A consultation with experts on the barriers and facilitators to implementing HIA in Italy. J. Environ. Manag. 2018, 218, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Davenport, C.; Mathers, J.; Parry, J. Use of health impact assessment in incorporating health considerations in decision making. J. Epidemiol. Community Health 2006, 60, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Haigh, F.; Harris, E.; Harris, P.; Baum, F.; Dannenberg, A.L.; Harris, M.F.; Kelehera, H.; Kemp, L.; Morgan, R.; Chok, H.N.; et al. What makes health impact assessments successful? Factors contributing to effectiveness in Australia and New Zealand. BMC Public Health 2015, 15, 1009. [Google Scholar] [CrossRef] [PubMed]
- O’Mullane, M.; Quinlivan, A. Health Impact Assessment (HIA) in Ireland and the role of local government. Environ. Impact Assess. Rev. 2012, 32, 181–186. [Google Scholar] [CrossRef]
- O’Mullane, M. Integrating Health Impact Assessment with the Policy Process: Lessons and Experiences from Around the World; OUP Oxford: Oxford, UK, 2013. [Google Scholar]
- Ahmad, B.; Chappel, D.; Pless-Mulloli, T.; White, M. Enabling factors and barriers for the use of health impact assessment in decision-making processes. Public Health 2008, 122, 452–457. [Google Scholar] [CrossRef]
- Kearns, N.; Pursell, L. Time for a paradigm change? Tracing the institutionalisation of health impact assessment in the Republic of Ireland across health and environmental sectors. Health Policy 2011, 99, 91–96. [Google Scholar] [CrossRef]
- Iglesias-Merchan, C.; Domínguez-Ares, E. Challenges to integrate health impact assessment into environmental assessment procedures: The pending debate. Impact Assess. Proj. Apprais. 2020, 38, 299–307. [Google Scholar] [CrossRef]
- Harris, P.; Haigh, F. Including health in environmental impact assessments: Is an institutional approach useful for practice? Impact Assess. Proj. Apprais. 2015, 33, 135–141. [Google Scholar] [CrossRef]
- McCallum, L.C.; Ollson, C.A.; Stefanovic, I.L. An adaptable Health Impact Assessment (HIA) framework for assessing health within Environmental Assessment (EA): Canadian context, international application. Impact Assess. Proj. Apprais. 2017, 36, 5–15. [Google Scholar] [CrossRef]
- Nowacki, J.; Viliani, F.; Martuzzi, M.; Fehr, R. Health in Impact Assessments—Opportunities not to be missed: Rainer Fehr. Eur. J. Public Health 2014, 24, 242. [Google Scholar] [CrossRef]
- Yin, R.K. Case Study Research: Design and Methods, 2nd ed.; Applied Social Research Methods Series; Sage Publications: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Bourcier, E.; Charbonneau, D.; Cahill, C.; Dannenberg, A.L. An Evaluation of Health Impact Assessments in the United States, 2011–2014. Prev. Chronic Dis. 2015, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- Wismar, M.; Blau, J.; Ernst, K.; Figueras, J. The Effectiveness of Health Impact Assessment: Scope and Limitations of Supporting Decision-Making in Europe; WHO: Copenhagen, Denmark, 2007. [Google Scholar]
- Winkler, M.S.; Furu, P.; Viliani, F.; Cave, B.; Divall, M.; Ramesh, G.; Harris, P.; Winkler, M.S. Current Global Health Impact Assessment Practice. Int. J. Environ. Res. Public Health 2020, 17, 2988. [Google Scholar] [CrossRef] [PubMed]
- Lacouture, A.; Breton, E.; Guichard, A.; Ridde, V. The concept of mechanism from a realist approach: A scoping review to facilitate its operationalization in public health program evaluation. Implement. Sci. 2015, 10, 153. [Google Scholar] [CrossRef] [PubMed]
- Meuleman, L. Owl meets beehive: How impact assessment and governance relate. Impact Assess. Proj. Apprais. 2014, 33, 4–15. [Google Scholar] [CrossRef]
- Tremblay, É.; St-Pierre, L.; Viens, C. L’évaluation d’impact sur la santé en Montérégie: Un processus appuyé sur le courtage de connaissances. Glob. Health Promot. 2017, 24, 66–74. [Google Scholar] [CrossRef]
- Cambon, L.; Alla, F. Transfert et partage de connaissances en santé publique: Réflexions sur les composantes d’un dispositif national en France. St. Publique 2013, 25, 757. [Google Scholar] [CrossRef]
- King, J.A.; Alkin, M.C. The Centrality of Use: Theories of Evaluation Use and Influence and Thoughts on the First 50 Years of Use Research. Am. J. Eval. 2018, 40, 431–458. [Google Scholar] [CrossRef]
- Volkov, B.B. Beyond being an evaluator: The multiplicity of roles of the internal evaluator. New Dir. Eval. 2011, 2011, 25–42. [Google Scholar] [CrossRef]
- Fehr, R.; Alexanderson, K.; Favaretti, C.; De Jong, J.; La Torre, G.; Lim, T.-A.; Martin-Olmedo, P.; Mekel, O.C.L.; Michelsen, K.; Rosenkötter, N.; et al. Health assessments for health governance—Concepts and methodologies. Eur. J. Public Health 2017, 27, 609–616. [Google Scholar] [CrossRef][Green Version]
- Honta, M.; Haschar-Noé, N.; Salaméro, E. L’État à l’épreuve de la régulation territoriale. La mise en négociations des contrats locaux de santé. Négociations 2018, 29, 143–155. [Google Scholar] [CrossRef]
- Thondoo, M.; Rueda, D.R.; Gupta, J.; De Vries, D.H.; Nieuwenhuijsen, M. Systematic Literature Review of Health Impact Assessments in Low and Middle-Income Countries. Int. J. Environ. Res. Public Health 2019, 16, 2018. [Google Scholar] [CrossRef] [PubMed]
- Fakhri, A.; Harris, P.; Maleki, M. Proposing a framework for Health Impact Assessment in Iran. BMC Public Health 2015, 15, 335. [Google Scholar] [CrossRef] [PubMed]
- Berensson, K.; Tillgren, P. Health impact assessment (HIA) of political proposals at the local level: Successful introduction, but what has happened 15 years later? Glob. Health Promot. 2017, 24, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Green, L. Health Impact Assessment (HIA) in Wales: From voluntary to statutory. Eur. J. Public Heal. 2017, 27 (Suppl. 3), 27. [Google Scholar] [CrossRef]
- Simos, J.; Spanswick, L.; Palmer, N.; Christie, D.P.T.H. The role of health impact assessment in Phase V of the Healthy Cities European Network. Health Promot. Int. 2015, 30, i71–i85. [Google Scholar] [CrossRef]
- Nour, K.; Dutilly-Simard, S.; Brousselle, A.; Smits, P.; Buregeya, J.-M.; Loslier, J.; Denis, J.-L. Evaluation of the effects of health impact assessment practice at the local level in Monteregie. Health Res. Policy Syst. 2016, 14, 7. [Google Scholar] [CrossRef]
- Rivadeneyra, A. Évaluation de l’EIS Du Projet d’aménagement de La ZAC.; Bordeaux Métropole: Bordeaux. 2018. Available online: file:///C:/Users/MDPI/AppData/Local/Temp/RAPPORTFINAL_15octobre%202018_BMetroCom%20COMPLET.pdf (accessed on 25 August 2020).



{kind=link}
{kind=link}
| Analytical Dimensions | Montérégie | Nouvelle-Aquitaine |
|---|---|---|
| A. Contextual factors triggering HIA | ||
| Political support and commitment | Commitment to healthy public policy | Commitment to healthy public policy |
| HIA pilot project in 2007–2008 | 3 HIA pilot projects launched in 2015 | |
| Policy or administrative framework | HIA included in the regional PH action plan in 2009 | HIA included in the REHP 2017–2021 |
| HUP frameworks | ||
| Legal mandate | Not mandatory, conducted voluntarily, notwithstanding section 54 at the national level | Not mandatory, conducted voluntarily |
| B. Implementation scheme | ||
| Stewardship (lead agency providing framework, support and supervision) | PHD | Environmental Health Department at the RHA |
| Knowledge broker | RAHPE | |
| Roles and responsibilities | Regional public health teams: scoping, analysis, recommendations | RHA and RAHPE territorial agents, Municipalities: selection and establishment of ToR |
| Local public health teams and Municipalities: screening, recommendations | Regional Health Observatory (RHO), private firms, consultants: analysis, recommendations | |
| Technical support and expertise | Scientific committee (professionals from the PHD) | Technical committee (RHA, RAHPE, HIA experts) |
| HIA model | Broad model of health Stand-alone | Broad model of healthStand-alone |
| Decision-support HIAs | Decision-support HIAs | |
| C. HIA delivery | ||
| Proponents | Municipalities | Municipalities |
| Practitioners’ profile and capacities | Public health professionals | RHO, private firms and consultants. Mainly trained on the job (basic training + learning by doing approach) |
| Resource persons | ||
| Learning by doing approach | ||
| Type of HIA | Intermediate | Mostly intermediate HIAs |
| Decision level | Municipal projects | Municipal projects |
| Sector | Urban planning and social policy | Mainly housing and urban planning |
| Funding | Sustained budget within the general budget of the Public | Dedicated funds within the 2017–2021 REHP (allocated to RAHPE and municipalities commissioning HIAs) |
| Health Department (1 position, working hours of scientific committee members) | ||
| Capacity building | Ongoing training of new professionals joining the regional HIA team | 1-day training targeting all stakeholders at the scoping stage |
| Resource generation (practice framework, methods, tools, evidence) | Tools developed by the regional HIA team | HIA website (ToR, screening and advocacy tools, HIA reports) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jabot, F.; Tremblay, E.; Rivadeneyra, A.; Diallo, T.A.; Lapointe, G. A Comparative Analysis of Health Impact Assessment Implementation Models in the Regions of Montérégie (Québec, Canada) and Nouvelle-Aquitaine (France). Int. J. Environ. Res. Public Health 2020, 17, 6558. https://doi.org/10.3390/ijerph17186558
Jabot F, Tremblay E, Rivadeneyra A, Diallo TA, Lapointe G. A Comparative Analysis of Health Impact Assessment Implementation Models in the Regions of Montérégie (Québec, Canada) and Nouvelle-Aquitaine (France). International Journal of Environmental Research and Public Health. 2020; 17(18):6558. https://doi.org/10.3390/ijerph17186558
Chicago/Turabian StyleJabot, Françoise, Emile Tremblay, Ana Rivadeneyra, Thierno Amadou Diallo, and Geneviève Lapointe. 2020. "A Comparative Analysis of Health Impact Assessment Implementation Models in the Regions of Montérégie (Québec, Canada) and Nouvelle-Aquitaine (France)" International Journal of Environmental Research and Public Health 17, no. 18: 6558. https://doi.org/10.3390/ijerph17186558
APA StyleJabot, F., Tremblay, E., Rivadeneyra, A., Diallo, T. A., & Lapointe, G. (2020). A Comparative Analysis of Health Impact Assessment Implementation Models in the Regions of Montérégie (Québec, Canada) and Nouvelle-Aquitaine (France). International Journal of Environmental Research and Public Health, 17(18), 6558. https://doi.org/10.3390/ijerph17186558