A Comparison Study of Posture and Fatigue of Neck According to Monitor Types (Moving and Fixed Monitor) by Using Flexion Relaxation Phenomenon (FRP) and Craniovertebral Angle (CVA)

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
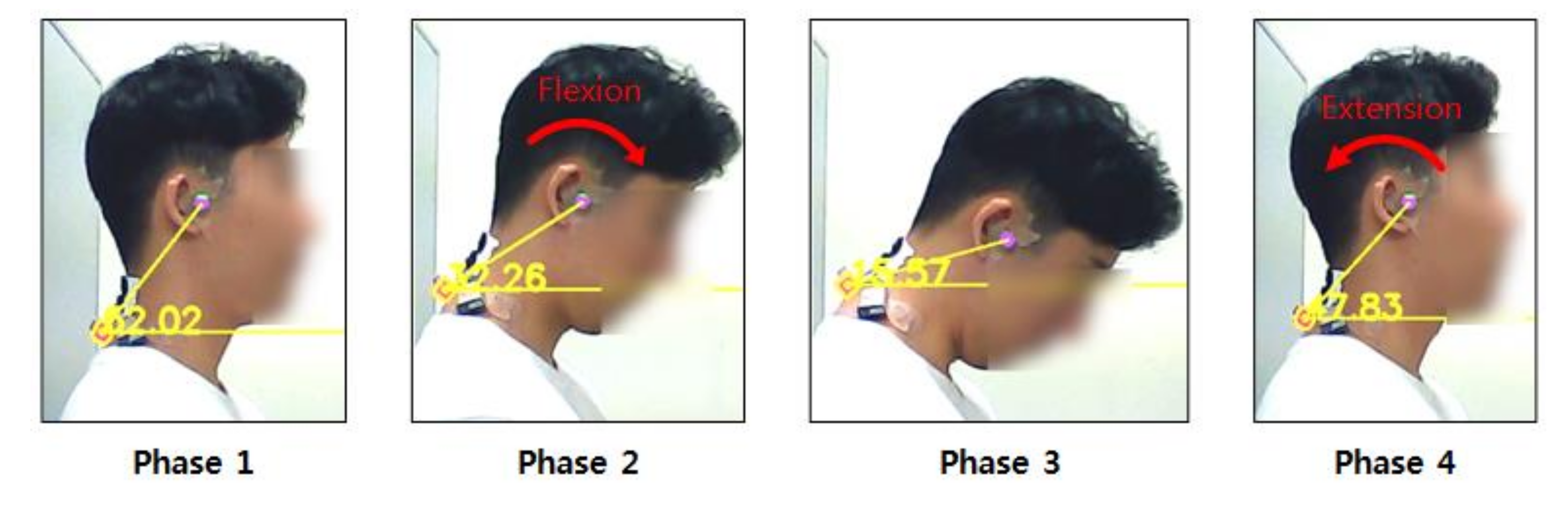
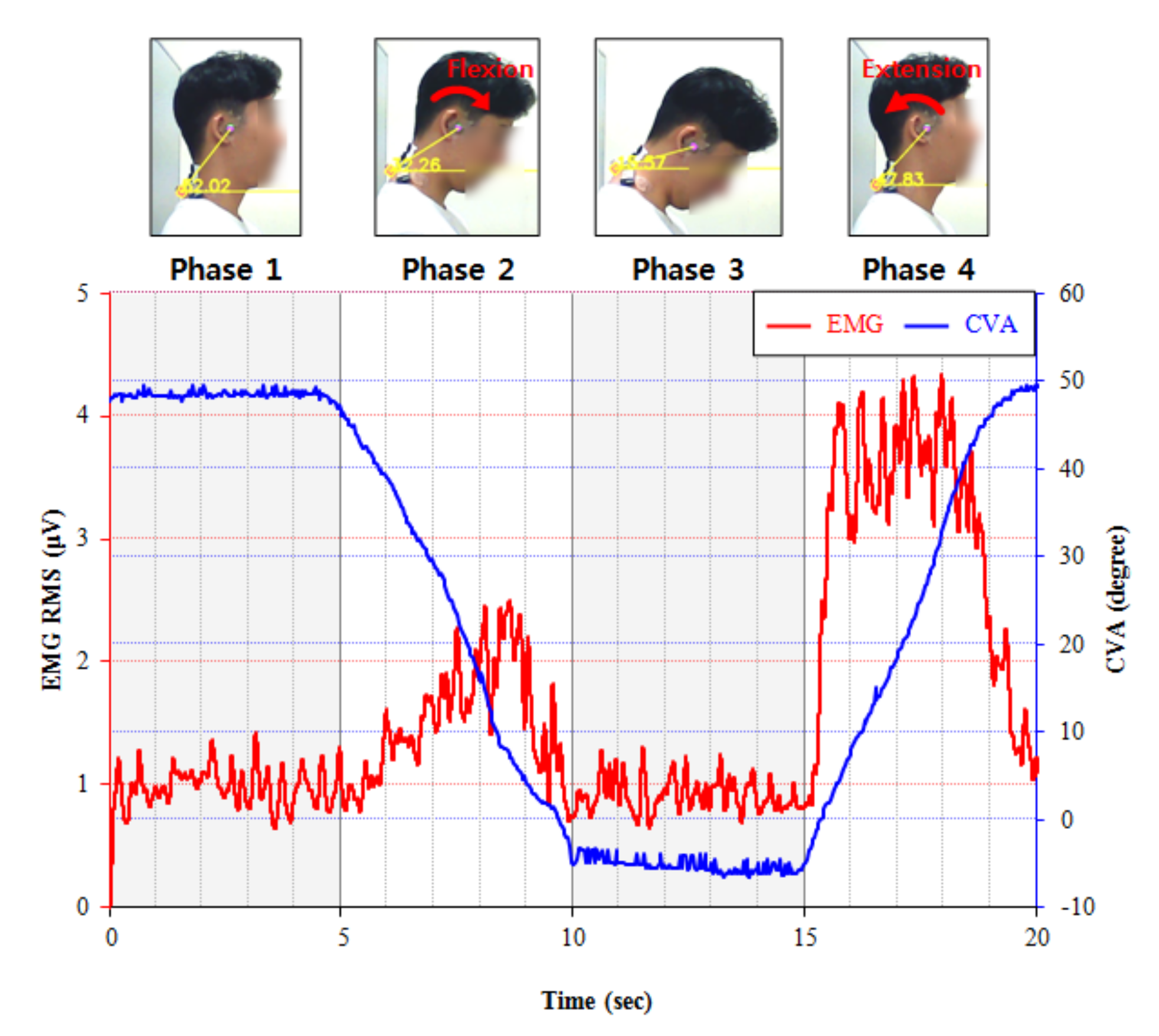
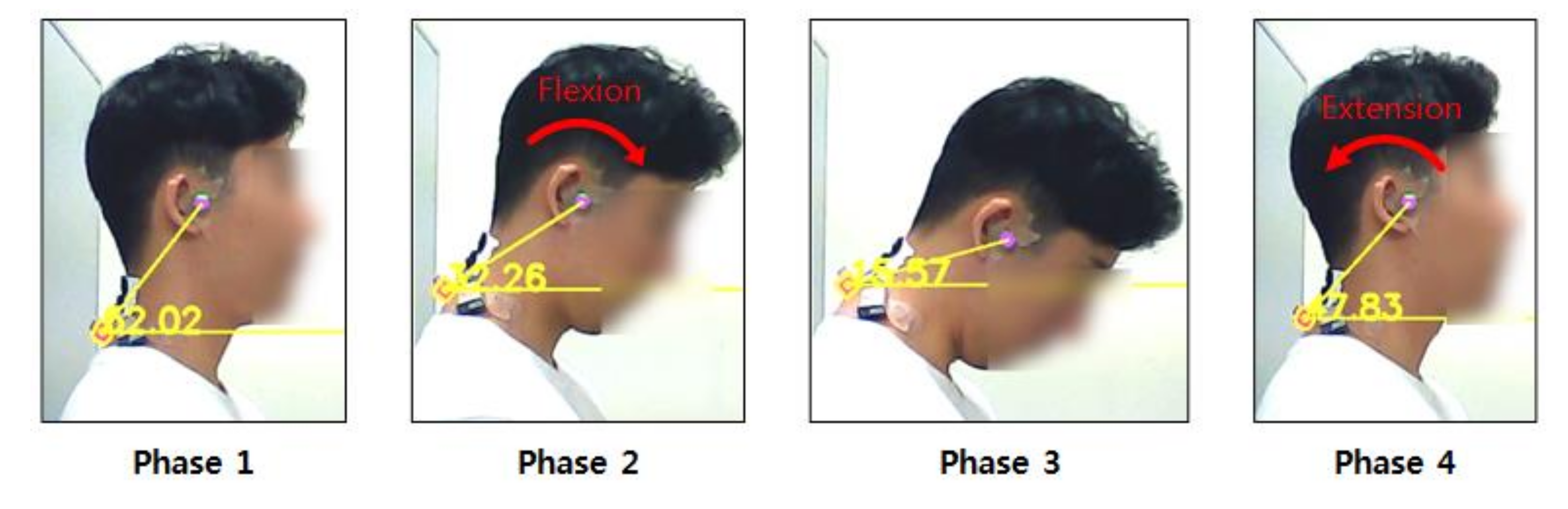
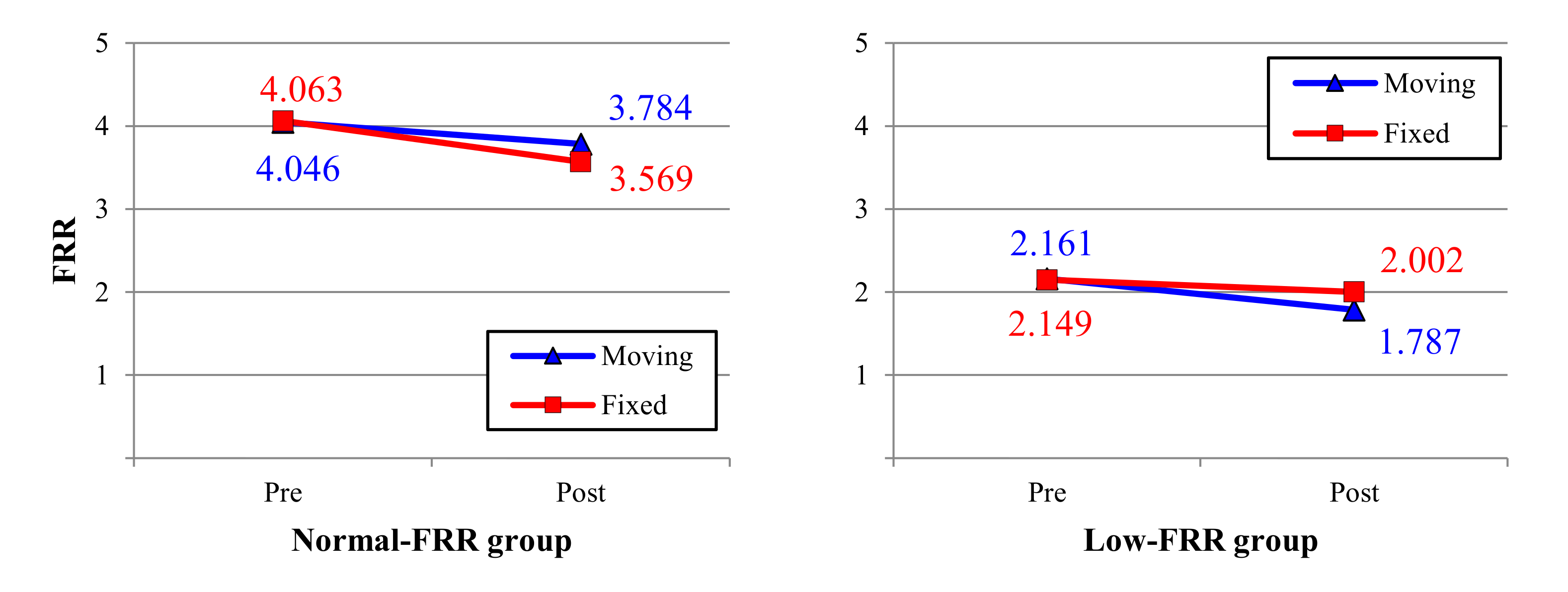
- FRR: The FRR has been widely used to quantify the relaxation ability of the extensor muscles of the neck. The FRR, as calculated by using Equation (1), is defined as the ratio of the maximum EMG value in the extension phase (phase 4) to the average EMG value in the full flexion phase (phase 3), as shown in Figure 2 [15].
- 2.
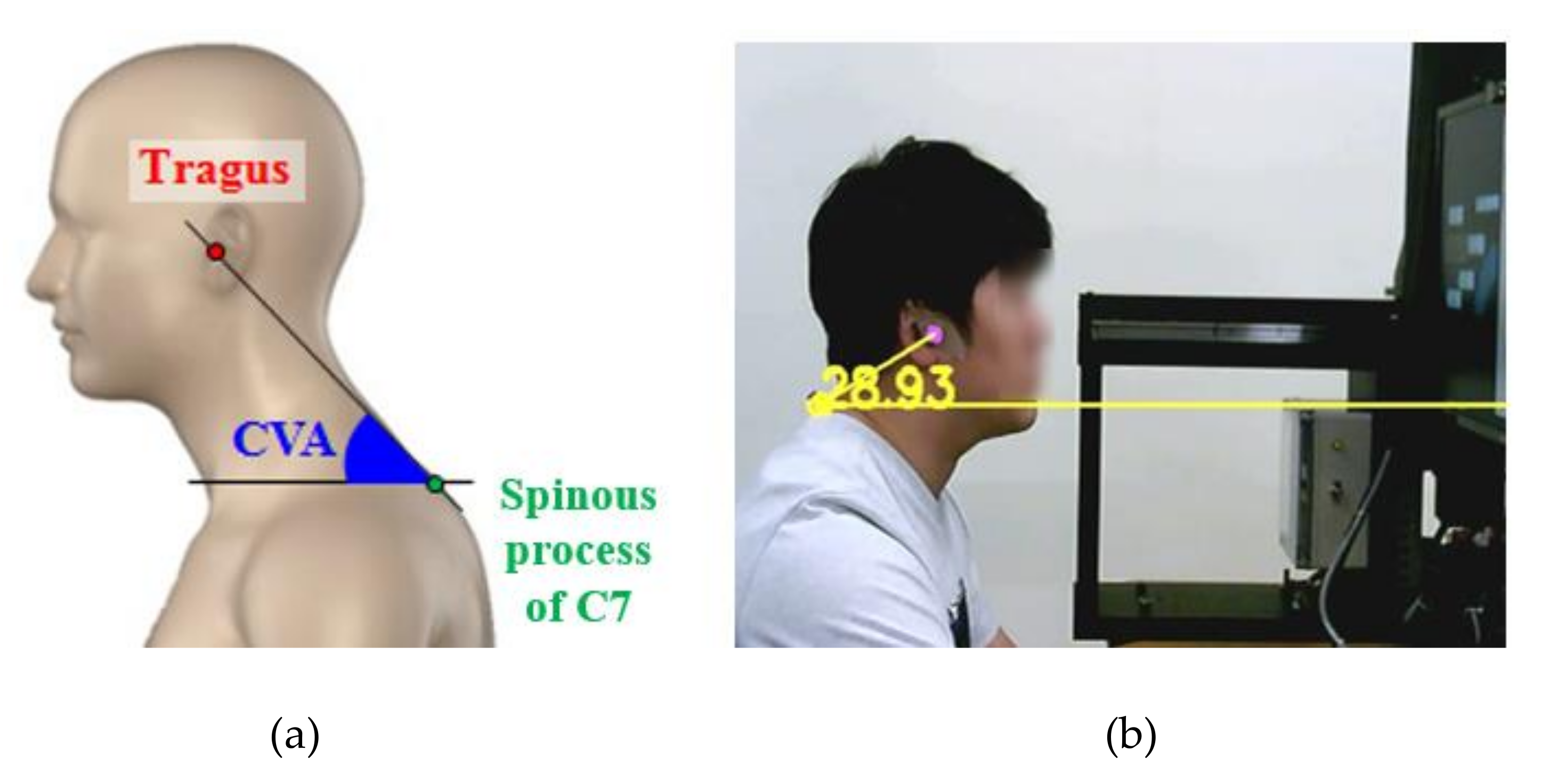
- CVA (degree): The CVA is the angle between a horizontal line passing through the spinous process of C7, and a line extending from the tragus of the ear to C7 (Figure 4a) was also observed to assess the angles of the neck postures in this study. A webcam (HD WebCam C270, Logitech, Seoul, Korea) was installed on the right side of the participants to measure the CVA. The CVA detection program was developed based on the OpenCV-Python; it could detect two markers attached to the participant’s Tragus and C7 and calculate the CVA in real-time (Figure 4b).
- 3.
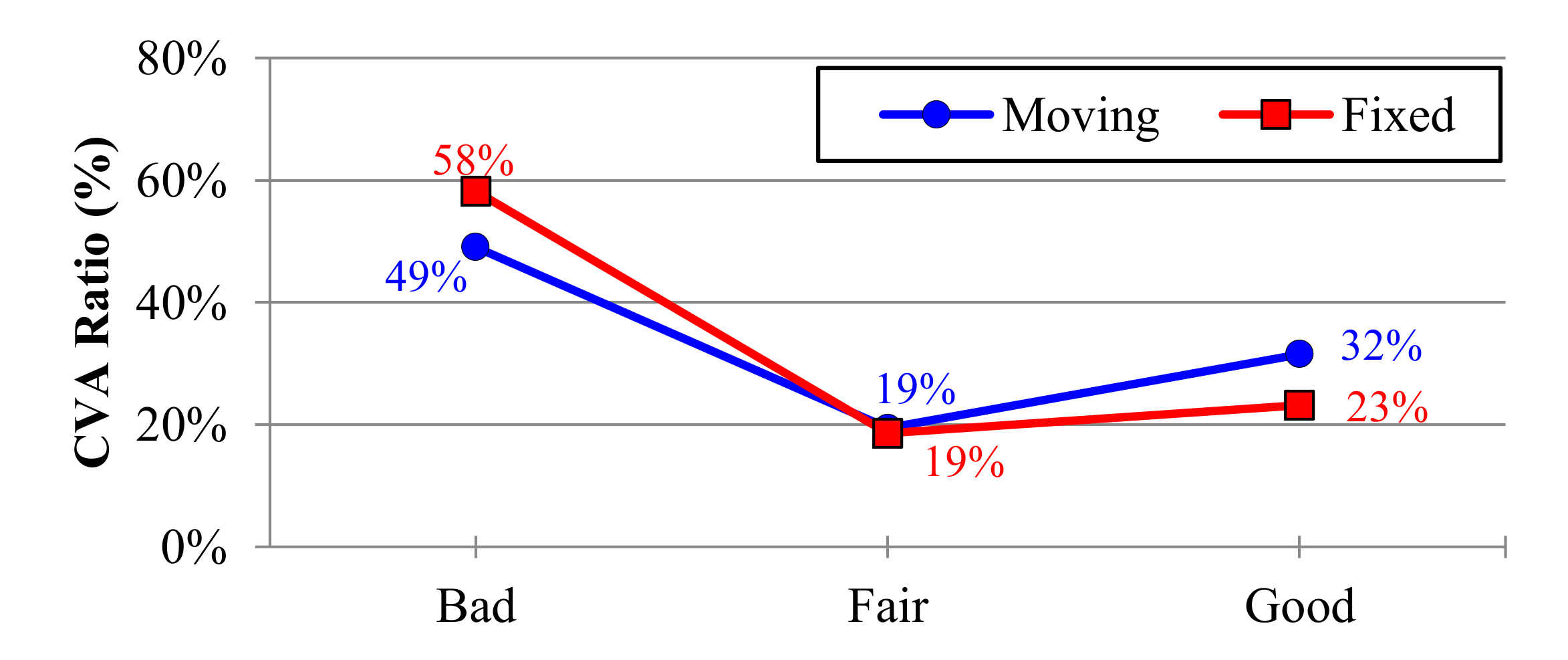
- The ratio of the CVA: Based on the FHP, the CVA ratio was considered as reflecting good, fair, and bad posture. If the CVA was higher than 48.7°, it was defined as a “good” posture. A CVA range of 43.8–48.7° and a value lower than 43.8° were defined as “fair” and “bad” postures, respectively [6].
2.3. Experimental Procedure
2.4. Data Analysis
3. Results
3.1. Craniovertebral Angle (CVA)
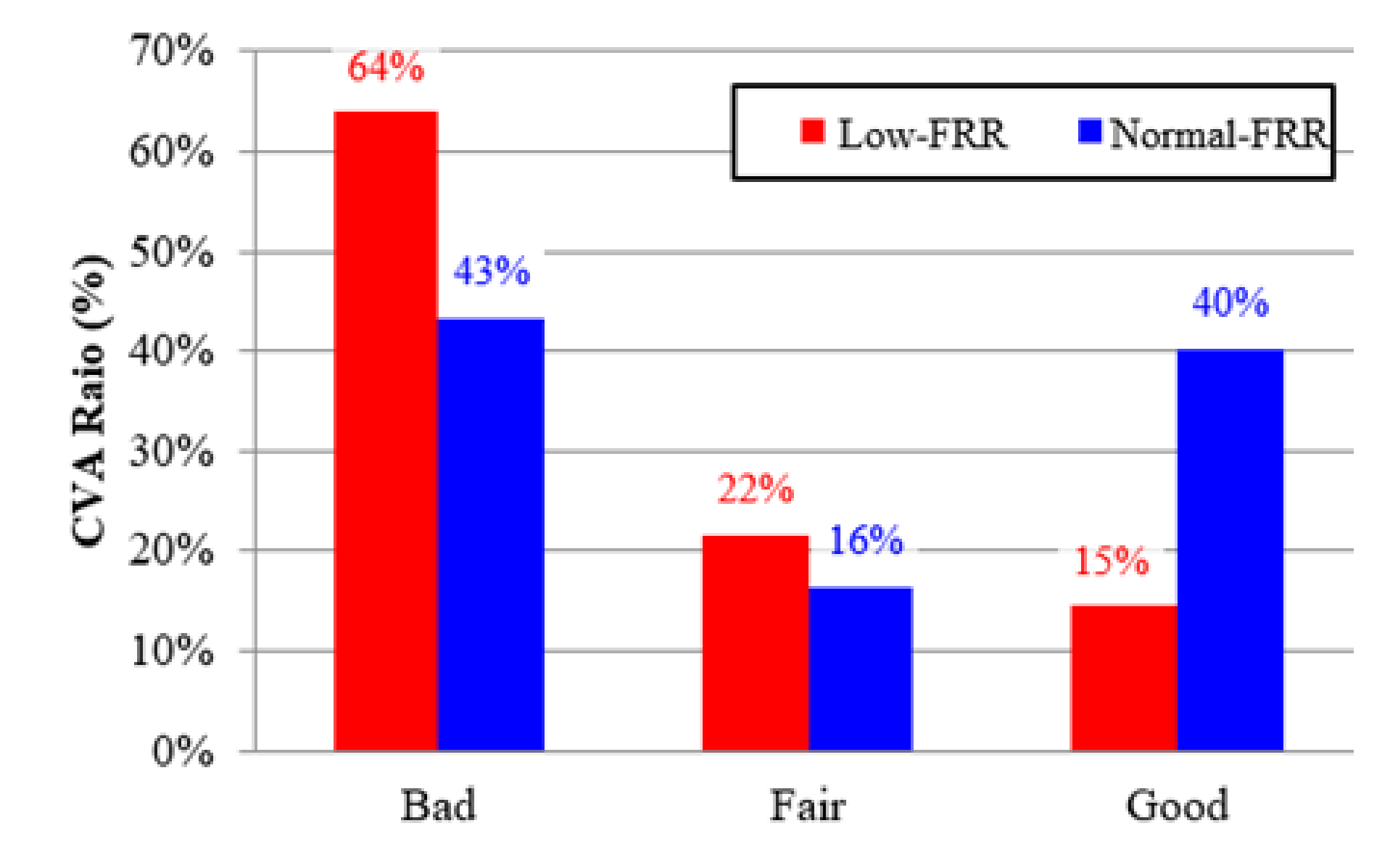
3.2. The Ratio of Craniovertebral Angle (CVA)
3.3. Flexion Relaxation Ratio (FRR)
4. Discussion
4.1. Craniovertebral Angle (CVA)
4.2. Flexion Relaxation Ratio (FRR)
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lee, I.S.; Kim, S.Y. Correlation among the cervical kyphotic angle, pain, and disability level in patients with temporomandibular disorders. Phys. Ther. Korea 2020, 27, 102–110. [Google Scholar] [CrossRef]
- Yoo, W.G.; Yi, C.H.; Kim, M.H. Effects of a proximity-sensing feedback chair on head, shoulder, and trunk postures when working at a visual display terminal. J. Occup. Rehabil. 2006, 16, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Sauter, S.L.; Schleifer, L.M.; Knutson, S.J. Work posture, workstation design, and musculoskeletal discomfort in a VDT data entry task. Hum. Factors 1991, 33, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Mekhora, K.; Liston, C.B.; Nanthavanij, S.; Cole, J.H. The effect of ergonomic intervention on discomfort in computer users with tension neck syndrome. Int. J. Ind. Ergon. 2000, 26, 367–379. [Google Scholar] [CrossRef]
- Grace, E.G.; Sarlani, E.; Read, B. The use of an oral exercise device in the treatment of muscular TMD. Cranio 2002, 20, 204–208. [Google Scholar] [CrossRef]
- Kim, E.J. Effects of Turtle Neck Syndrome on Respiratory Volume According to Posture. Ph.D. Thesis, Daegu Catholic University, Daegu, Korea, 2018. [Google Scholar]
- Kim, S.W.; Kim, S.J.; Son, S.K.; Dong, S.O.; Lee, J.C.; Shin, D.J. Correlation between the head forward posture and the site of herniation of single level cervical intervertebral disc. J. Korea CHUNA Man. Med. Spine Nerves 2013, 8, 31–38. [Google Scholar]
- Kim, S.Y.; Kim, N.S.; Jung, J.H.; Jo, M.R. Effect of Forward Head Posture on Respiratory Function in Young Adults. J. Korean Phys. Ther. 2013, 25, 311–315. [Google Scholar]
- Cho, J.; Lee, E.; Lee, S. Upper thoracic spine mobilization and mobility exercise versus upper cervical spine mobilization and stabilization exercise in individuals with forward head posture: A randomized clinical trial. BMC Musculoskelet. Disord. 2017, 18, 525. [Google Scholar] [CrossRef]
- Yip, C.H.T.; Chiu, T.T.W.; Poon, A.T.K. The relationship between head posture and severity and disability of patients with neck pain. Man. Therap. 2008, 13, 148–154. [Google Scholar] [CrossRef]
- Quek, J.; Pua, Y.H.; Clark, R.A.; Bryant, A.L. Effects of thoracic kyphosis and forward head posture on cervical range of motion in older adults. Man. Therap. 2013, 18, 65–71. [Google Scholar] [CrossRef]
- Floyd, W.F.; Silver, P.H.S. Function of erectores spinae in flexion of the trunk. Lancet 1951, 257, 133–134. [Google Scholar] [CrossRef]
- Panjabi, M.M. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J. Spinal Disord. Tech. 1992, 5, 383. [Google Scholar] [CrossRef] [PubMed]
- Colloca, C.J.; Hinrichs, R.N. The biomechanical and clinical significance of the lumbar erector spinae flexion-relaxation phenomenon: A review of literature. J. Manip. Physiol. Ther. 2005, 28, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Nimbarte, A.D.; Zreiqat, M.M.; Chowdhury, S.K. Cervical flexion-relaxation response to neck muscle fatigue in males and females. J. Electromyogr. Kinesiol. 2014, 24, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.J.; Berk, R.J.; Anderson, A.V. Recruitment patterns in the cervical paraspinal muscles during cervical forward flexion: Evidence of cervical flexion-relaxation. Electromyogr. Clin. Neurophysiol. 1993, 33, 217–223. [Google Scholar]
- Hashemirad, F.; Talebian, S.; Hatef, B.; Kahlaee, A.H. The relationship between flexibility and EMG activity pattern of the erector spinae muscles during trunk flexion-extension. J. Electromyogr. Kinesiol. 2009, 19, 746–753. [Google Scholar] [CrossRef]
- Murphy, B.A.; Marshall, P.W.; Taylor, H.H. The cervical flexion-relaxation ratio: Reproducibility and comparison between chronic neck pain patients and controls. Spine 2010, 35, 2103–2108. [Google Scholar] [CrossRef]
- Maroufi, N.; Ahmadi, A.; Khatir, S.R.M. A comparative investigation of flexion relaxation phenomenon in healthy and chronic neck pain subjects. Eur. Spine J. 2013, 22, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Nimbarte, A.D.; Zreiqat, M.; Ning, X. Impact of shoulder position and fatigue on the flexion-relaxation response in cervical spine. Clin. Biomech. 2014, 29, 277–282. [Google Scholar] [CrossRef]
- Zabihhosseinian, M.; Holmes, M.W.; Ferguson, B.; Murphy, B. Neck muscle fatigue alters the cervical flexion relaxation ratio in sub-clinical neck pain patients. Clin. Biomech. 2015, 30, 397–404. [Google Scholar] [CrossRef]
- Lindstrom, L.H.; Magnusson, R.I. Interpretation of Myoelectric Power Spectra: A Model and Its Applications. In Proceedings of the IEEE, Dayton, OH, USA, 17–19 May 1977; pp. 653–662. [Google Scholar] [CrossRef]
- Murata, A.; Uetake, A.; Matsumoto, S.; Takasawa, Y. Evaluation of shoulder muscular fatigue induced during VDT tasks. Int. J. Hum. Comput. Interact. 2003, 15, 407–417. [Google Scholar] [CrossRef]
- Niu, H.; Li, R.; Liu, G.; Pu, F.; Li, D.; Fan, Y. Using EMG to Evaluate Muscular Fatigue Induced during Video Display Terminal Keyboard Use Task. In Proceedings of the 7th Asian-Pacific Conference on Medical and Biological Engineering, Beijing, China, 22–25 April 2008; pp. 329–332. [Google Scholar] [CrossRef]
- Chea, Y.W. The measurement of forward head posture and pressure pain threshold in neck muscle. J. Korean Phys. Ther. 2002, 14, 117–124. [Google Scholar]
- Kang, J.H.; Park, R.Y.; Lee, S.J.; Kim, J.Y.; Yoon, S.R.; Jung, K.I. The effect of the forward head posture on postural balance in long time computer based worker. Ann. Rehabil. Med. 2012, 36, 98–104. [Google Scholar] [CrossRef] [Green Version]
- Pialasse, J.P.; Dubois, J.D.; Choquette, M.H.P.; Lafond, D.; Descarreaux, M. Kinematic and electromyographic parameters of the cervical flexion–relaxation phenomenon: The effect of trunk positioning. Ann. Phys. Rehabil. Med. 2009, 52, 49–58. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.J.; Han, H.Y.; Cheon, S.H.; Park, S.H.; Yong, M.S. The effect of forward head posture on muscle activity during neck protraction and retraction. J. Phys. Ther. Sci. 2015, 27, 977–979. [Google Scholar] [CrossRef] [Green Version]
- Harman, K.; Hubley-Kozey, C.L.; Butler, H. Effectiveness of an exercise program to improve forward head posture in normal adults: A randomized, controlled 10-week trial. J. Man. Manip. Ther. 2005, 13, 163–176. [Google Scholar] [CrossRef]
- Im, B.; Kim, Y.; Chung, Y.; Hwang, S. Effects of scapular stabilization exercise on neck posture and muscle activation in individuals with neck pain and forward head posture. J Phys. Ther. Sci. 2016, 28, 951–955. [Google Scholar] [CrossRef] [Green Version]
- Gurudut, P.; Welling, A.; Chodankar, A. Effect of self-care exercises in forward head posture on craniovertebral angle and craniocervical flexion endurance: A pilot study. Indian J. Phys. Ther. Res. 2020, 2, 25–30. [Google Scholar] [CrossRef]
- Watson, D.H.; Trott, P.H. Cervical headache: An investigation of natural head posture and upper cervical flexor muscle performance. Cephalalgia 1993, 13, 272–284. [Google Scholar] [CrossRef]
- Salahzadeh, Z.; Maroufi, N.; Ahmadi, A.; Behtash, H.; Razmjoo, A.; Gohari, M.; Parnianpour, M. Assessment of forward head posture in females: Observational and photogrammetry methods. J. Back. Musculoskelet. Rehabil. 2014, 27, 131–139. [Google Scholar] [CrossRef]
- Shin, S.J.; An, D.H.; Oh, J.S.; Yoo, W.G. Changes in pressure pain in the upper trapezius muscle, cervical range of motion, and the cervical flexion-relaxation ratio after overhead work. Ind. Health 2012, 50, 509–515. [Google Scholar] [CrossRef] [Green Version]
- DeVocht, J.W.; Gudavalli, K.; Gudavalli, M.; Xia, T. Novel electromyographic protocols using axial rotation and cervical flexion-relaxation for the assessment of subjects with neck pain: A feasibility study. J. Chiropr. Med. 2016, 15, 102–111. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.J.; Yoo, W.G. Changes in cervical range of motion, flexion-relaxation ratio and pain with visual display terminal work. Work 2014, 47, 261–265. [Google Scholar] [CrossRef]
- Yoo, W.G.; Park, S.Y.; Lee, M.R. Relationship between active cervical range of motion and flexion–relaxation ratio in asymptomatic computer workers. J. Physiol. Anthropol. 2011, 30, 203–207. [Google Scholar] [CrossRef] [Green Version]
- Allen, D.G. Skeletal muscle function: Role of ionic changes in fatigue, damage and disease. Clin. Exp. Pharmacol. Physiol. 2004, 31, 485–493. [Google Scholar] [CrossRef]
- Vukova, T.; Vydevska-Chichova, M.; Radicheva, N. Fatigue-induced changes in muscle fiber action potentials estimated by wavelet analysis. J. Electromyogr. Kinesiol. 2008, 18, 397–409. [Google Scholar] [CrossRef]
- Yoo, W.G.; Yoo, I.G. Changes in the cervical FRR, shoulder muscle pain and position after continuous detailed assembly work. Work 2014, 49, 735–739. [Google Scholar] [CrossRef]
- Cagnie, B.; Danneels, L.; van Tiggelen, D.; de Loose, V.; Cambier, D. Individual and work related risk factors for neck pain among office workers: A cross sectional study. Eur. Spine. J. 2007, 16, 679–686. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, R.D.C.P.; Carvalho, F.M.; Assunção, A.Á. Prevalence of musculoskeletal disorders among plastics industry workers. Cad. Saude Publica 2011, 27, 78–86. [Google Scholar] [CrossRef]
- Skov, T.; Borg, V.; Orhede, E. Psychosocial and physical risk factors for musculoskeletal disorders of the neck, shoulders, and lower back in salespeople. Occup. Environ. Med. 1996, 53, 351–356. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Neck Condition | FRR | Age (Year) | Weight (kg) | Height (cm) | Sitting Height (cm) |
|---|---|---|---|---|---|
| Normal-FRR group | 3.9 ± 1.4 | 26.4 ± 2.5 | 74.6 ± 7.7 | 174.2 ± 3.8 | 92.0 ± 3.4 |
| Low-FRR group | 2.0 ± 0.5 | 27.6 ± 3.1 | 81.4 ± 14.3 | 172.9 ± 2.9 | 90.0 ± 2.9 |
| FRR Group | Fixed Monitor | Moving Monitor | ||||
|---|---|---|---|---|---|---|
| Good | Fair | Bad | Good | Fair | Bad | |
| Normal-FRR | 38.4% | 16.4% | 45.2% | 42.0% | 16.5% | 41.5% |
| Low-FRR | 8.0% | 20.9% | 71.2% | 21.0% | 22.4% | 56.6% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, K.-H.; Cho, M.-U.; Park, C.-W.; Kim, S.-Y.; Kim, M.-J.; Hong, B.; Kong, Y.-K. A Comparison Study of Posture and Fatigue of Neck According to Monitor Types (Moving and Fixed Monitor) by Using Flexion Relaxation Phenomenon (FRP) and Craniovertebral Angle (CVA). Int. J. Environ. Res. Public Health 2020, 17, 6345. https://doi.org/10.3390/ijerph17176345
Choi K-H, Cho M-U, Park C-W, Kim S-Y, Kim M-J, Hong B, Kong Y-K. A Comparison Study of Posture and Fatigue of Neck According to Monitor Types (Moving and Fixed Monitor) by Using Flexion Relaxation Phenomenon (FRP) and Craniovertebral Angle (CVA). International Journal of Environmental Research and Public Health. 2020; 17(17):6345. https://doi.org/10.3390/ijerph17176345
Chicago/Turabian StyleChoi, Kyeong-Hee, Min-Uk Cho, Chae-Won Park, Seoung-Yeon Kim, Min-Jung Kim, Boram Hong, and Yong-Ku Kong. 2020. "A Comparison Study of Posture and Fatigue of Neck According to Monitor Types (Moving and Fixed Monitor) by Using Flexion Relaxation Phenomenon (FRP) and Craniovertebral Angle (CVA)" International Journal of Environmental Research and Public Health 17, no. 17: 6345. https://doi.org/10.3390/ijerph17176345
APA StyleChoi, K.-H., Cho, M.-U., Park, C.-W., Kim, S.-Y., Kim, M.-J., Hong, B., & Kong, Y.-K. (2020). A Comparison Study of Posture and Fatigue of Neck According to Monitor Types (Moving and Fixed Monitor) by Using Flexion Relaxation Phenomenon (FRP) and Craniovertebral Angle (CVA). International Journal of Environmental Research and Public Health, 17(17), 6345. https://doi.org/10.3390/ijerph17176345