Retrospective Exposure Assessment Methods Used in Occupational Human Health Risk Assessment: A Systematic Review

 ,
,  , ,
, ,  , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
1.1. Background
1.2. Problem Statement
1.3. Aim of the Study
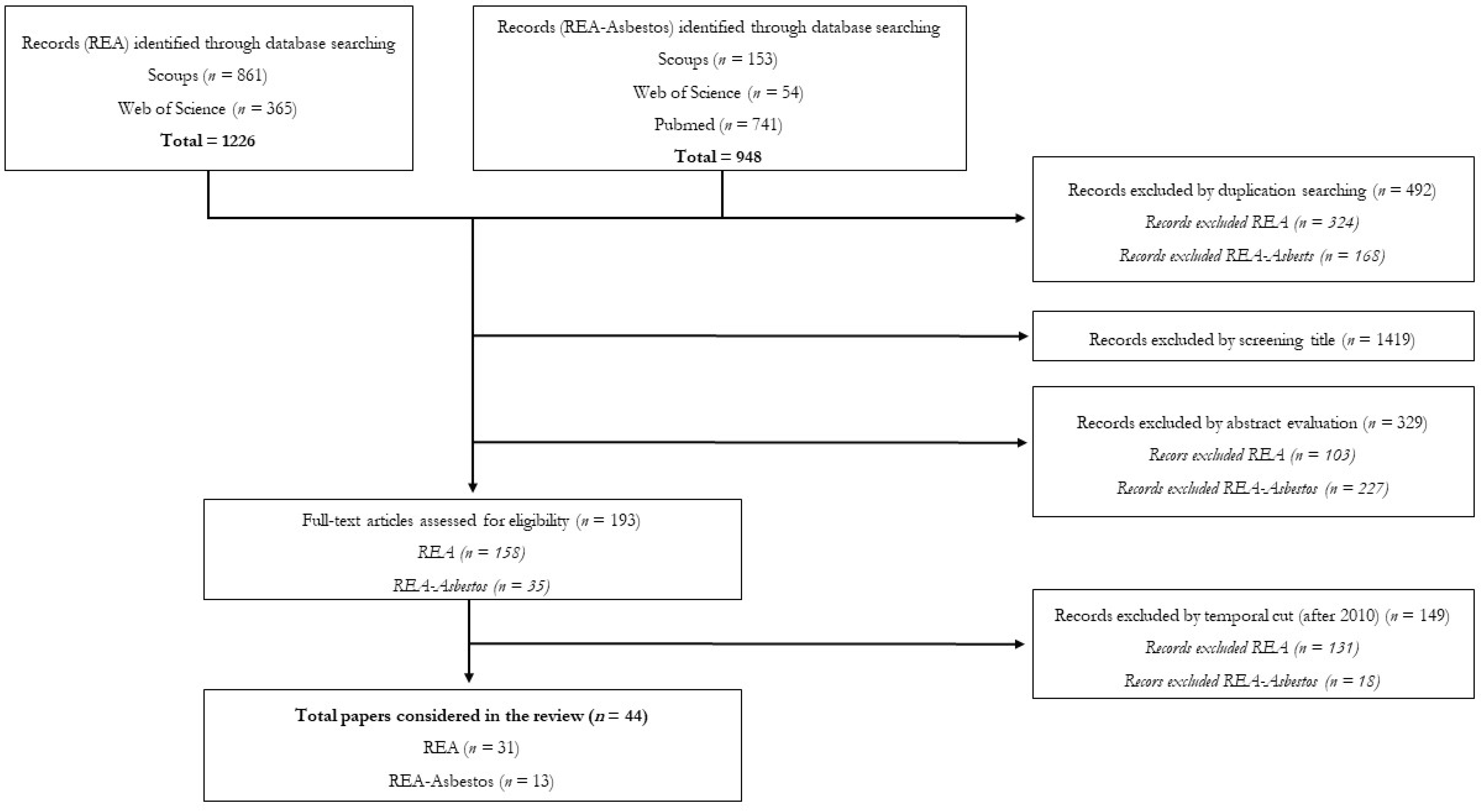
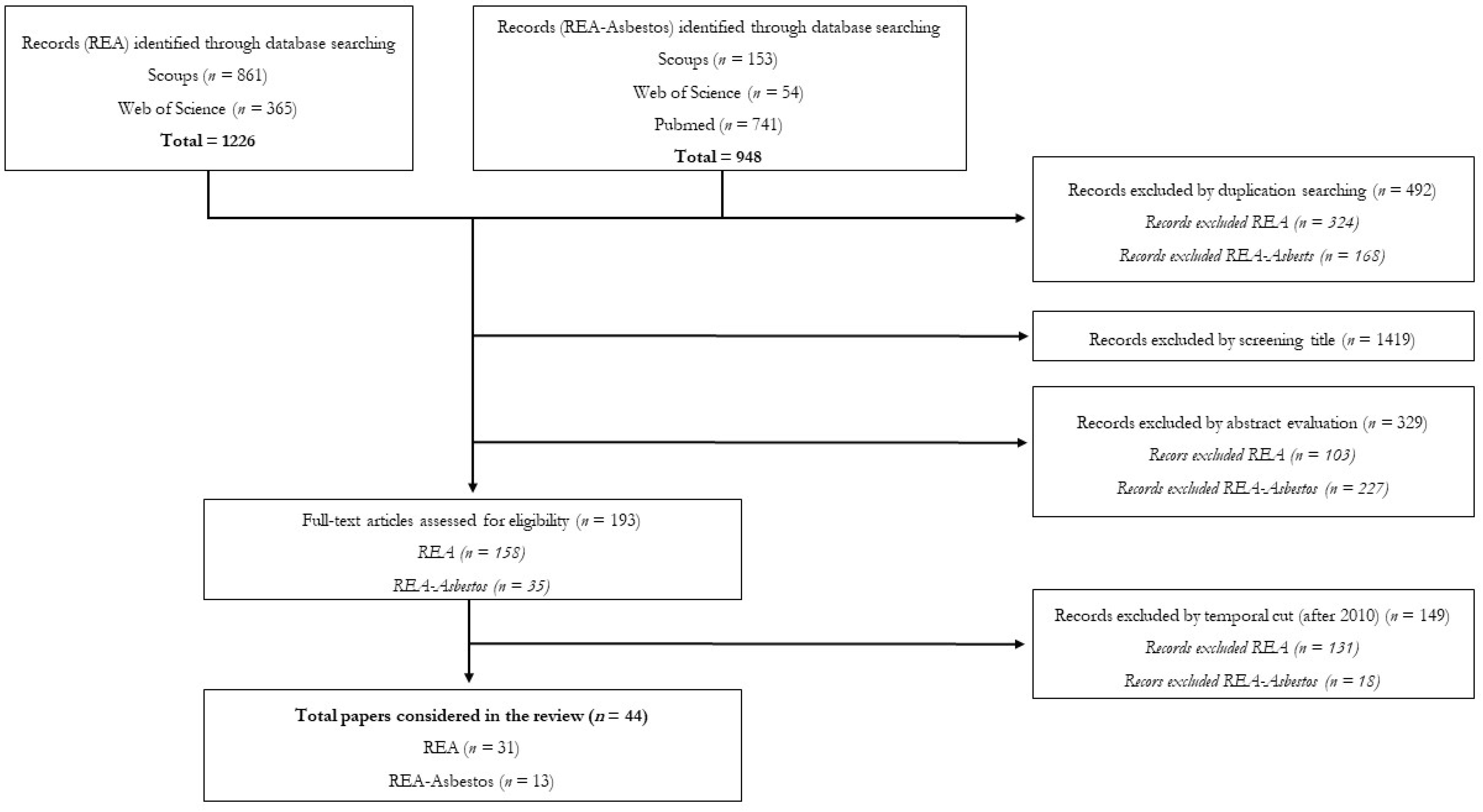
2. Materials and Methods
3. Results and Discussions
3.1. REA
3.1.1. Applications for Occupational Exposure to Chemical Risk Agents
3.1.2. Methods Used in the Past Exposure Reconstruction
3.1.3. Parameters to Be Considered
3.1.4. Statistical Methods
3.1.5. JEMs Used
3.1.6. Principal Results
3.1.7. Problems and Solutions
3.2. REA–Asbestos
3.2.1. Applications for Occupational Exposure Assessment to Asbestos
3.2.2. Methods Used in the Past Exposure Reconstruction
3.2.3. Parameters to Be Considered
3.2.4. Statistical Methods
3.2.5. JEMs Used
3.2.6. Principal Results
3.2.7. Problems and Solutions
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sahmel, J.; Devlin, K.; Paustenbach, D.; Hollins, D.; Gaffney, S. The role of exposure reconstruction in occupational human health risk assessment: Current methods and a recommended framework. Crit. Rev. Toxicol. 2010, 40, 799–843. [Google Scholar] [CrossRef]
- Corradi, M. What is new in the air? Monaldi Arch. Chest Dis. Pulm. Ser. 2020, 57, 227–228. [Google Scholar]
- Miller, G.; Sciences, D.J. The nature of nurture: Refining the definition of the exposome. Toxicological 2014, 134, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daiber, A.; Münzel, T. Explaining the impact of environmental risk factors on cardiovascular health by the “exposome” concept. FASEB J. 2020, 34, 1. [Google Scholar] [CrossRef]
- Grandjean, P.; Budtz-Jøorgensen, E.; Keiding, N.; Weihe, P. Underestimation of Risk due to Exposure Misclassification. Int. J. Occup. Med. Environ. Health 2004, 17, 131–136. [Google Scholar] [CrossRef]
- Blair, A.; Stewart, P.; Lubin, J.H.; Forastiere, F. Methodological issues regarding confounding and exposure misclassification in epidemiological studies of occupational exposures. Am. J. Ind. Med. 2007, 50, 199–207. [Google Scholar] [CrossRef]
- Esmen, N.A. Analysis of strategies for reconstructing exposures. Appl. Occup. Environ. Hyg. 1991, 6, 488–494. [Google Scholar] [CrossRef]
- Stewart, P. Challenges to retrospective exposure assessment. Scand. J. Work. Environ. Health 1999, 25, 505–510. [Google Scholar] [CrossRef] [Green Version]
- Viet, S.M.; Stenzel, M.; Rennix, C.; Armstrong, T.; Couch, J. Guideline on Occupational Exposure Reconstruction; American Industrial Hygiene Association Press: Fairfax, VA, USA, 2008. [Google Scholar]
- Armstrong, T.; Boelter, F.; Rasmuson, J. Exposure reconstruction. In Mathematical Models for Estimating Occupational Exposure to Chemicals; Keil, C.B., Simmons, C.E., Anthony, T.R., Eds.; American Industrial Hygiene Association Press: Fairfax, VA, USA, 2009. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Andersson, L.; Burdorf, A.; Bryngelsson, I.L.; Westberg, H. Estimating trends in quartz exposure in swedish iron foundries-Predicting past and present exposures. Ann. Occup. Hyg. 2012, 56, 362–372. [Google Scholar]
- Armstrong, T.W.; Liang, Y.; Hetherington, Y.; Bowes, S.M.; Wong, O.; Fu, H.; Chen, M.; Schnatter, A.R. Retrospective occupational exposure assessment for case-control and case-series epidemiology studies based in Shanghai China. J. Occup. Environ. Hyg. 2011, 8, 561–572. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Ramachandran, G.; Vadali, M.; Sahmel, J. Bayesian Hierarchical framework for occupational hygiene decision making. Ann. Occup. Hyg. 2014, 58, 1079–1093. [Google Scholar] [PubMed] [Green Version]
- Bello, A.; Woskie, S.R.; Gore, R.; Sandler, D.P.; Schmidt, S.; Kamel, F. Retrospective assessment of occupational exposures for the GENEVA study of ALS among military veterans. Ann. Work Expo. Health 2017, 61, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Boelter, F.W.; Persky, J.D.; Podraza, D.M.; Bullock, W.H. Characterizing and Communicating Risk with Exposure Reconstruction and Bayesian Analysis: Historical Locomotive Maintenance/Repair Associated with Asbestos Woven Tape Pipe Lagging. Risk Anal. 2016, 36, 228–243. [Google Scholar] [CrossRef]
- Boelter, F.W.; Xia, Y.; Persky, J.D. A Bayesian Model and Stochastic Exposure (Dose) Estimation for Relative Exposure Risk Comparison Involving Asbestos-Containing Dropped Ceiling Panel Installation and Maintenance Tasks. Risk Anal. 2017, 37, 1729–1741. [Google Scholar] [CrossRef]
- Chen, Y.C.; Ramachandran, G.; Alexander, B.H.; Mandel, J.H. Retrospective exposure assessment in a chemical research and development facility. Environ. Int. 2012, 39, 111–121. [Google Scholar] [CrossRef]
- Cherrie, J.W.; McElvenny, D.; Blyth, K.G. Estimating past inhalation exposure to asbestos: A tool for risk attribution and disease screening. Int. J. Hyg. Environ. Health 2018, 221, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.; Kang, D.; Park, D.; Lee, H.; Choi, B. Developing Asbestos Job Exposure Matrix Using Occupation and Industry Specific Exposure Data (1984–2008) in Republic of Korea. Saf. Health Work 2017, 8, 105–115. [Google Scholar] [CrossRef] [Green Version]
- Couch, J.R.; Petersen, M.; Rice, C.; Schubauer-Berigan, M.K. Development of retrospective quantitative and qualitative job-exposure matrices for exposures at a beryllium processing facility. Occup. Environ. Med. 2011, 68, 361–365. [Google Scholar] [CrossRef]
- Chung, D.A.; Yang, R.; Verma, D.K.; Luo, J. Retrospective Exposure Assessment for Occupational Disease of an Individual Worker Using an Exposure Database and Trend Analysis. J. Occup. Environ. Hyg. 2015, 12, 855–865. [Google Scholar] [CrossRef]
- Dopart, P.J.; Friesen, M.C. New Opportunities in Exposure Assessment of Occupational Epidemiology: Use of Measurements to Aid Exposure Reconstruction in Population-Based Studies. Curr. Environ. Health Rep. 2017, 4, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.E.; Hart, J.E.; Laden, F.; Garshick, E.; Smith, T.J. A retrospective assessment of occupational exposure to elemental carbon in the U.S. Trucking Industry. Environ. Health Perspect 2011, 119, 997–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fayerweather, W.E.; Trumbore, D.C.; Johnson, K.A.; Niebo, R.W.; Maxim, L.D. Quantitative exposure matrix for asphalt fume, total particulate matter, and respirable crystalline silica among roofing and asphalt manufacturing workers. Inhal. Toxicol. 2011, 23, 668–679. [Google Scholar] [CrossRef] [PubMed]
- Felten, M.K.; Knoll, L.; Eisenhawer, C.; Ackermann, D.; Khatab, K.; Hüdepohl, J.; Zschiesche, W.; Kraus, T. Retrospective exposure assessment to airborne asbestos among power industry workers. J. Occup. Med. Toxicol. 2010, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Févotte, J.; Dananché, B.; Delabre, L.; Ducamp, S.; Garras, L.; Houot, M.; Luce, D.; Orlowski, E.; Pilorget, C.; Lacourt, A.; et al. Matgéné: A program to develop job-exposure matrices in the general population in France. Ann. Occup. Hyg. 2011, 55, 865–878. [Google Scholar] [CrossRef] [Green Version]
- Fleming, D.A.; Woskie, S.R.; Jones, J.H.; Silver, S.R.; Luo, L.; Bertke, S.J. Retrospective assessment of exposure to chemicals for a microelectronics and business machine manufacturing facility. J. Occup. Environ. Hyg. 2014, 11, 292–305. [Google Scholar] [CrossRef] [Green Version]
- Føreland, S.; Bugge, M.D.; Bakke, B.; Bye, E.; Eduard, W. A novel strategy for retrospective exposure assessment in the norwegian silicon carbide industry. J. Occup. Environ. Hyg. 2012, 9, 230–241. [Google Scholar] [CrossRef]
- Friesen, M.C.; Coble, J.B.; Lu, W.; Shu, X.O.; Ji, B.T.; Xue, S.; Portengen, L.; Chow, W.H.; Gao, Y.T.; Yang, G.; et al. Combining a job-exposure matrix with exposure measurements to assess occupational exposure to benzene in a population cohort in Shanghai, China. Ann. Occup. Hyg. 2012, 56, 80–91. [Google Scholar]
- Hanley, K.W.; Viet, S.M.; Hein, M.J.; Carreón, T.; Ruder, A.M. Exposure to o-Toluidine, Aniline, and nitrobenzene in a rubber chemical manufacturing plant: A retrospective exposure assessment update. J. Occup. Environ. Hyg. 2012, 9, 478–490. [Google Scholar] [CrossRef]
- Hidajat, M.; McElvenny, D.M.; Mueller, W.; Ritchie, P.; Cherrie, J.W.; Darnton, A.; Agius, R.M.; Kromhout, H.; De Vocht, F. Job-exposure matrix for historical exposures to rubber dust, rubber fumes and n-Nitrosamines in the British rubber industry. Occup. Environ. Med. 2019, 76, 259–267. [Google Scholar] [CrossRef]
- Canu, I.G.; Jacob, S.; Cardis, E.; Wild, P.; Caër-Lorho, S.; Auriol, B.; Laurier, D.; Tirmarche, M. Reprocessed uranium exposure and lung cancer risk. Health Phys. 2010, 99, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.Y.; Rocheleau, C.M.; Hein, M.J.; Waters, M.A.; Stewart, P.A.; Lawson, C.C.; Reefhuis, J. Agreement between twomethods for retrospective assessment of occupational exposure intensity to six chlorinated solvents: Data fromthe national birth defects prevention study. J. Occup. Environ. Hyg. 2017, 14, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.M.; Dell, L.; Torres, C.; Simmons, C.E.; Poole, J.; Boelter, F.W.; Harper, P. Exposure reconstruction and risk analysis for six semiconductor workers with lymphohematopoietic cancers. J. Occup. Environ. Med. 2015, 57, 649–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koeman, T.; Offermans, N.S.M.; Christopher-De Vries, Y.; Slottje, P.; Van Den Brandt, P.A.; Goldbohm, R.A.; Kromhout, H.; Vermeulen, R. JEMs and incompatible occupational coding systems: Effect of manual and automatic recoding of job codes on exposure assignment. Ann. Occup. Hyg. 2013, 57, 107–114. [Google Scholar]
- Lavoué, J.; Pintos, J.; Van Tongeren, M.; Kincl, L.; Richardson, L.; Kauppinen, T.; Cardis, E.; Siemiatycki, J. Comparison of exposure estimates in the Finnish job-exposure matrix FINJEM with a JEM derived from expert assessments performed in Montreal. Occup. Environ. Med. 2012, 69, 465–471. [Google Scholar] [CrossRef] [Green Version]
- MacFarlane, E.; Benke, G.; Sim, M.R.; Fritschi, L. OccIDEAS: An innovative tool to assess past asbestos exposure in the Australian mesothelioma registry. Saf. Health Work 2012, 3, 71–76. [Google Scholar] [CrossRef] [Green Version]
- Mester, B.; Schmeißer, N.; Lünzmann, H.; Pohlabeln, H.; Langner, I.; Behrens, T.; Ahrens, W. Development and evaluation of a tool for retrospective exposure assessment of selected endocrine disrupting chemicals and EMF in the car manufacturing industry. Ann. Occup. Hyg. 2011, 55, 736–751. [Google Scholar]
- Miller, J.B.; Machado, R.J. Prospective and retrospective exposure assessment. Environ. Claims J. 2010, 22, 221–229. [Google Scholar] [CrossRef]
- Nano, G.; Derudi, M.; Rota, R. Risk assessment of past exposure in forensic engineering. Chem. Eng. Trans. 2012, 26, 603–608. [Google Scholar]
- Offermans, N.S.M.; Vermeulen, R.; Burdorf, A.; Peters, S.; Goldbohm, R.A.; Koeman, T.; Van Tongeren, M.; Kauppinen, T.; Kant, I.; Kromhout, H.; et al. Comparison of expert and job-exposure matrix-based retrospective exposure assessment of occupational carcinogens in the Netherlands Cohort Study. Occup. Environ. Med. 2012, 69, 745–751. [Google Scholar] [CrossRef]
- Peters, S.; Vermeulen, R.; Olsson, A.; Van Gelder, R.; Kendzia, B.; Vincent, R.; Savary, B.; Williams, N.; Woldbæk, T.; Lavoué, J.; et al. Development of an exposure measurement database on five lung carcinogens (ExpoSYN) for quantitative retrospective occupational exposure assessment. Ann. Occup. Hyg. 2012, 56, 70–79. [Google Scholar] [PubMed]
- Peters, S.; Vermeulen, R.; Portengen, L.; Olsson, A.; Kendzia, B.; Vincent, R.; Savary, B.; LavouCrossed Sign, J.D.S.; Cavallo, D.; Cattaneo, A.; et al. SYN-JEM: A Quantitative Job-Exposure Matrix for Five Lung Carcinogens. Ann. Occup. Hyg. 2016, 60, 795–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portengen, L.; Linet, M.S.; Li, G.L.; Lan, Q.; Dores, G.M.; Ji, B.T.; Hayes, R.B.; Yin, S.N.; Rothman, N.; Vermeulen, R. Retrospective benzene exposure assessment for a multi-center case-cohort study of benzene-exposed workers in China. J. Expo. Sci. Environ. Epidemiol. 2016, 26, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Lin, Q.H.; Jiang, C.Q.; Lam, T.H.; Xu, L.; Jin, Y.L.; Cheng, K.K. Past occupational dust exposure, depressive symptoms and anxiety in retired Chinese factory workers: The Guangzhou biobank cohort study. J. Occup. Health 2014, 56, 444–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rando, R.J.; Vacek, P.M.; Glenn, R.E.; Kwon, C.W.; Parker, J.E. Retrospective Assessment of Respirable Quartz Exposure for a Silicosis Study of the Industrial Sand Industry. Ann. Work Expo. Heal. 2018, 62, 1021–1032. [Google Scholar] [CrossRef] [PubMed]
- Rasmuson, J.O.; Roggli, V.L.; Boelter, F.W.; Rasmuson, E.J.; Redinger, C.F. Cumulative Retrospective Exposure Assessment (REA) as a predictor of amphibole asbestos lung burden: Validation procedures and results for industrial hygiene and pathology estimates. Inhal. Toxicol. 2014, 26, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, E.G.; Stewart, J.; Herrick, R.; Palacios, H.; Laden, F.; Clark, W.; Delzell, E. Retrospective Exposure Assessment for Semiconductor and Storage Device Manufacturing Facilities. J. Occup. Environ. Med. 2019, 61, E132–E138. [Google Scholar] [CrossRef]
- Sauvé, J.F.; Lavoué, J.; Nadon, L.; Lakhani, R.; Senhaji Rhazi, M.; Bourbonnais, R.; Richard, H.; Parent, M.É. A hybrid expert approach for retrospective assessment of occupational exposures in a population-based case-control study of cancer. Environ. Health A Glob. Access Sci. Source 2019, 18, 1–12. [Google Scholar] [CrossRef]
- Sauvé, J.F.; Davies, H.W.; Parent, M.É.; Peters, C.E.; Sylvestre, M.P.; Lavoué, J. Development of Quantitative Estimates of Wood Dust Exposure in a Canadian General Population Job-Exposure Matrix Based on Past Expert Assessments. Ann. Work Expo. Health 2019, 63, 22–33. [Google Scholar] [CrossRef]
- Sauvé, J.F.; Siemiatycki, J.; Labrèche, F.; Richardson, L.; Pintos, J.; Sylvestre, M.P.; Gérin, M.; Bégin, D.; Lacourt, A.; Kirkham, T.L.; et al. Development of and Selected Performance Characteristics of CANJEM, a General Population Job-Exposure Matrix Based on Past Expert Assessments of Exposure. Ann. Work Expo. Health 2018, 62, 783–795. [Google Scholar]
- Shao, Y.; Hwang, J.; Alexander, B.H.; Mandel, J.H.; MacLehose, R.F.; Ramachandran, G. Reconstructing historical exposures to elongate mineral particles (EMPs) in the taconite mining industry for 1955–2010. J. Occup. Environ. Hyg. 2019, 16, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Sivulka, D.J.; Seilkop, S.K.; Lascelles, K.; Conard, B.R.; Jones, S.F.; Collinson, E.C. Reconstruction of historical exposures at a Welsh nickel refinery (1953–2000). Ann. Occup. Hyg. 2014, 58, 739–760. [Google Scholar] [PubMed]
- Vermeulen, R.; Coble, J.B.; Lubin, J.H.; Portengen, L.; Blair, A.; Attfield, M.D.; Silverman, D.T.; Stewart, P.A. The diesel exhaust in miners’ study: IV. Estimating historical exposures to diesel exhaust in underground non-metal mining facilities. Ann. Occup. Hyg. 2010, 54, 774–788. [Google Scholar] [PubMed] [Green Version]

{kind=link}
| General Retrospective Assessment | ||
|---|---|---|
| Database | Search Query | n |
| Scopus | (TITLE-ABS-KEY(“exposure assessment” OR “occupational exposure” OR “risk assessment” OR “exposure estimation”) AND TITLE-ABS-KEY(“exposure reconstruction” OR “past exposure” OR “historical exposure” OR “retrospective exposure assessment”)) | 857 |
| Web of Science | TS = (“exposure assessment” OR “occupational exposure” OR “risk assessment” OR “exposure estimation”) AND TS = (“exposure reconstruction” OR “past exposure” OR “historical exposure” OR “retrospective exposure assessment”) | 361 |
| Pubmed * | (((((exposure assessment) OR occupational exposure) OR risk assessment) OR exposure estimation)) AND ((((exposure reconstruction) OR past exposure) OR historical exposure) OR retrospective exposure assessment) | 11,800 |
| Retrospective Assessment of Asbestos | ||
|---|---|---|
| Database | Search Query | n |
| Scopus | (TITLE-ABS-KEY(“exposure assessment” OR “occupational exposure” OR “risk assessment” OR “exposure estimation”) AND TITLE-ABS-KEY(“exposure reconstruction” OR “past exposure” OR “historical exposure” OR “retrospective exposure assessment”)) AND TITLE-ABS-KEY (asbestos) | 152 |
| Web of Science | TS = (“exposure assessment” OR “occupational exposure” OR “risk assessment” OR “exposure estimation”) AND TS = (“exposure reconstruction” OR “past exposure” OR “historical exposure” OR “retrospective exposure assessment”) AND TS = (asbestos) | 51 |
| Pubmed | (((((exposure assessment) OR occupational exposure) OR risk assessment) OR exposure estimation)) AND ((((exposure reconstruction) OR past exposure) OR historical exposure) OR retrospective exposure assessment) AND (asbestos) | 730 |
| Reference | Author | Year of Publication | Contents |
|---|---|---|---|
| [12] | Andersson et al. | 2012 | ** |
| [13] | Armstrong et al. | 2011 | * |
| [14] | Banerjee et al. | 2014 | * |
| [15] | Bello et al. | 2017 | * |
| [16] | Boelter et al. | 2016 | ** |
| [17] | Boelter et al. | 2017 | ** |
| [18] | Chen et al. | 2012 | * |
| [19] | Cherrie et al. | 2018 | ** |
| [20] | Choi et al. | 2017 | ** |
| [21] | Couch et al. | 2011 | * |
| [22] | Chung et al. | 2015 | ** |
| [23] | Dopart et al. | 2017 | * |
| [24] | Davis et al. | 2011 | * |
| [25] | Fayerweather et al. | 2011 | * |
| [26] | Felten et al. | 2010 | ** |
| [27] | Févotte et al. | 2011 | * |
| [28] | Fleming et al. | 2014 | * |
| [29] | Føreland et al. | 2012 | ** |
| [30] | Friesen et al. | 2012 | * |
| [31] | Hanley et al. | 2012 | * |
| [32] | Hidajat et al. | 2019 | * |
| [33] | Canu et al. | 2010 | * |
| [34] | Johnson et al. | 2017 | * |
| [35] | Jones et al. | 2015 | * |
| [36] | Koeman et al. | 2013 | * |
| [37] | Lavoué et al. | 2020 | ** |
| [38] | MacFarlane et al. | 2012 | ** |
| [39] | Mester et al. | 2011 | * |
| [40] | Miller and Machado | 2010 | * |
| [41] | Nano et al. | 2012 | * |
| [42] | Offermans et al. | 2012 | ** |
| [43] | Peters et al. | 2012 | ** |
| [44] | Peters et al. | 2016 | ** |
| [45] | Portengen et al. | 2016 | * |
| [46] | Lin et al. | 2014 | ** |
| [47] | Rando et al. | 2018 | * |
| [48] | Rasmuson et al. | 2014 | ** |
| [49] | Rodrigues et al. | 2019 | * |
| [50] | Sauvé et al. | 2019 | * |
| [51] | Sauvé et al. | 2019 | * |
| [52] | Sauvé et al. | 2018 | * |
| [53] | Shao et al. | 2019 | * |
| [54] | Sivulka et al. | 2014 | * |
| [55] | Vermuele et al. | 2010 | * |
| Reference | Chemicals |
|---|---|
| [53] | Elongate mineral particle (EMP) |
| [25,47] | Respirable quartz |
| [55] | Respirable Elemental Carbon (REC) and carbon monoxide (CO) |
| [15] | “Group A” agents (lead, formaldehyde, hydrocarbon solvents, and chlorinated solvents) and “Group B” agents (mercury, selenium, arsenic, polychlorinated biphenyls, electromagnetic field, pesticides, and viral agents) |
| [39] | Endocrine Disruptors Chemicals (EDC) |
| [41] | Polycyclic Aromatic Hydrocarbons (PAH) |
| [13,30,45] | Benzene |
| [21] | Beryllium |
| [54] | Nickel |
| [50] | Wood dust |
| [25] | Asphalt fumes and total particulate matter |
| [32] | Rubber dust, rubber fumes and n-Nitrosamines |
| [18,36,37,45,52] | Other chemicals |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borghi, F.; Mazzucchelli, L.A.; Campagnolo, D.; Rovelli, S.; Fanti, G.; Keller, M.; Cattaneo, A.; Spinazzè, A.; Cavallo, D.M. Retrospective Exposure Assessment Methods Used in Occupational Human Health Risk Assessment: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 6190. https://doi.org/10.3390/ijerph17176190
Borghi F, Mazzucchelli LA, Campagnolo D, Rovelli S, Fanti G, Keller M, Cattaneo A, Spinazzè A, Cavallo DM. Retrospective Exposure Assessment Methods Used in Occupational Human Health Risk Assessment: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(17):6190. https://doi.org/10.3390/ijerph17176190
Chicago/Turabian StyleBorghi, Francesca, Libero Andrea Mazzucchelli, Davide Campagnolo, Sabrina Rovelli, Giacomo Fanti, Marta Keller, Andrea Cattaneo, Andrea Spinazzè, and Domenico Maria Cavallo. 2020. "Retrospective Exposure Assessment Methods Used in Occupational Human Health Risk Assessment: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 17: 6190. https://doi.org/10.3390/ijerph17176190
APA StyleBorghi, F., Mazzucchelli, L. A., Campagnolo, D., Rovelli, S., Fanti, G., Keller, M., Cattaneo, A., Spinazzè, A., & Cavallo, D. M. (2020). Retrospective Exposure Assessment Methods Used in Occupational Human Health Risk Assessment: A Systematic Review. International Journal of Environmental Research and Public Health, 17(17), 6190. https://doi.org/10.3390/ijerph17176190