1. Introduction
Resistance training is largely used in sports to increase muscle strength and promoting hypertrophic response [
1] and in rehabilitation to reinforce muscles after injury [
2]. Several exercises have been developed to target the agonist muscles through a series of mechanical stimuli; hence, a definition of the agonist muscle activation during each exercise may help to select the exercises appropriately [
3,
4]. Among the possible targets, the muscles surrounding the shoulders are involved in a series of multiplanar movements in many sports and daily life activities [
5], so that several exercises are performed to reinforce these muscles. Particularly,
deltoid muscle (which can be divided into
anterior,
medial, and
posterior deltoid),
trapezius (especially its upper portion), the clavicular head of
pectoralis major, and
triceps brachii are among the muscles targeted when performing shoulder exercises [
5,
6,
7].
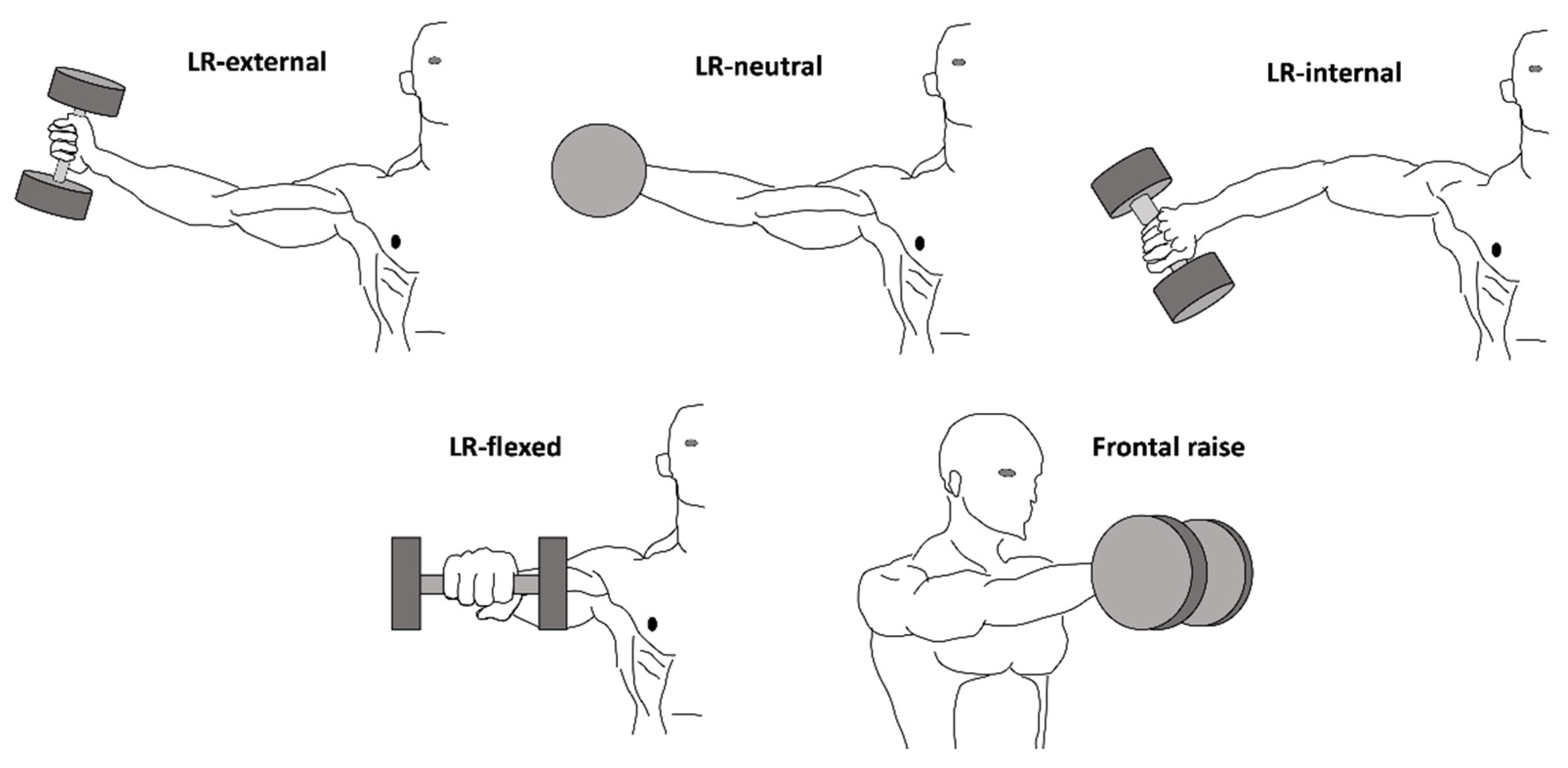
Lateral raise (LR) and frontal raise consist of arm abduction and flexion on the frontal or sagittal plane, respectively, and are largely used to stimulate the shoulders muscles [
5,
8,
9,
10]. LR can be performed with a range of variations, including an exercise where the humerus is rotated externally (LR-external), neutrally (LR-neutral), or internally (LR-internal) [
5,
10]. Comparing LR-external vs. LR-internal, a previous study reported that the latter elicited
medial and
posterior deltoid more than the former, while no data were observed for LR-neutral and
anterior deltoid [
10]. Another study also showed that the
upper trapezius activation increased by rotating abducting the humerus on the sagittal vs. frontal plane [
11]. Additionally, frontal raise is expected to mainly elicit
anterior deltoid and the clavicular head of
pectoralis major—two strong humerus flexors [
5,
11]. Interestingly, in practice, LR can be performed with a flexed elbow (LR-flexed). It is expected that LR-flexed might elicit less activation in
deltoid muscles because of the shorter lever in frontal abduction; however, no study has compared these exercises so far. Lastly,
triceps brachii is a strong stabilizer of the elbow during all LR variations and frontal raise. However, no study has examined its activation during these exercises. A comprehensive examination of the activation of the muscles surrounding the shoulders during LR variations and frontal raise may help to properly plan resistance training sessions to increase strength and possibly promote hypertrophy [
12]. As such, each exercise could be selected depending on the muscle activation we want to focus on.
The previous studies investigating muscle activation in LR variations and frontal raise mainly recruited subjects with no-specified experience in strength training [
6,
8,
10,
11]. It has been shown that muscle activation for a given exercise is correlated with training experience [
13] and possibly lead to different results. In contrast, competitive bodybuilders have a greater capacity to activate the agonist muscles while practicing strength exercises [
3] and have shown already unique muscle pattern in bench press variations [
14]. Consequently, investigating the differences in muscle activation across a range of similar exercises in subjects with greater training experience may elicit greater between-exercise differences in muscle recruitment comparing LR variations and frontal raise. Remarkably, resistance exercises usually consist of performing both the concentric and eccentric phases. Interestingly, performing repetitive eccentric phases incur into specific short-term [
15,
16] and long-term training-induced effects [
1,
17,
18] compared to concentric-based training. Hence, examining the muscle activation in LR variations and frontal raise during both the concentric and the eccentric phase could further differentiate the training stimuli through an accentuation of the concentric or eccentric phase. To date, only one study investigated the muscle recruitment during the eccentric phase of isokinetic shoulder abduction, highlighting that overall muscle activation was influenced by velocity and torque exerted, but no comparison was done with the concentric phase [
9]. Therefore, the present study aimed to examine the muscle activation of
deltoid,
upper trapezius, the clavicular head of
pectoralis major, and
triceps brachii in a range of LR variations (LR-external, LR-neutral, LR-internal, LR-flexed) and frontal raise during both the concentric and eccentric phase in competitive bodybuilders.
3. Results
The intrasession reliability of the sEMG RMS signal for muscle maximum voluntary isometric activation and for the concentric and eccentric phase of each exercise is provided in
Table 1. ICC and SEM% during the maximum activation ranged from 0.878 to 0.927 and 2.7% to 6.6%, respectively. During each exercise, ICC and SEM% were comprised between 0.795 and 0.904 and between 5.4% and 8.7% during the concentric phase, whereas spanned from 0.798 to 0.903 and 5.2% to 8.5% during the eccentric phase.
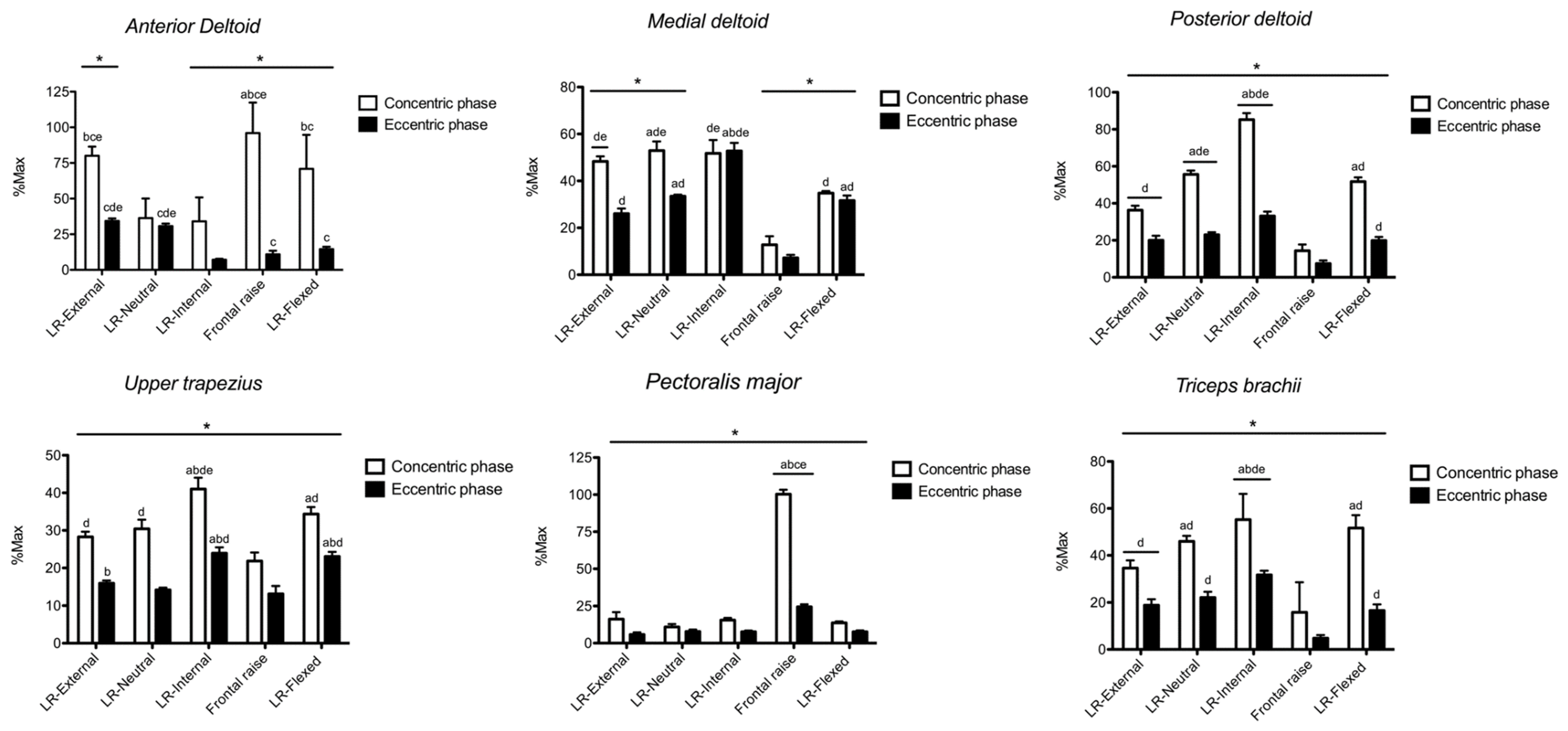
The sEMG RMS amplitude for
anterior deltoid is shown in
Figure 2. Exercise × phase interaction (
p < 0.001, F = 493.3, η
2 = 0.998) was found. With the exception of the LR-neutral, greater (
p < 0.05, F = 388.6, partial η
2 = 0.982) sEMG RMS was found during the concentric vs. eccentric phase in all other exercises. During the concentric phase, sEMG RMS was greater in frontal raise compared with LR-external (ES: 1.78, from 0.63 to 2.73), LR-neutral (ES: 5.30, from 3.27 to 6.87), LR-internal (ES: 6.72, from 4.26 to 6.82), and LR-flexed (ES: 1.95, from 0.81 to 2.91). LR-external showed greater sEMG RMS than LR-neutral (ES: 4.68, from 3.20 to 5.91), LR-internal (ES: 6.84, from 4.82 to 8.48), and LR-flexed (ES: 0.82, from 0.05 to 1.84). LR-flexed showed greater EMG RMS than LR-neutral (ES: 4.68, from 2.84 to 6.13) and LR-internal (ES: 6.84, from 4.34 to 8.76). During the eccentric phase, sEMG RMS in LR-external and LR-neutral was greater than LR-internal (ES: 13.04, from 8.72 to 16.46 and 10.66, from 6.92 to 13.49, respectively), frontal raise (ES: 5.94, from 3.72 to 7.95 and 4.31, from 2.68 to 5.68, respectively), and LR-flexed (ES: 6.19, from 3.89 to 7.97 and 3.88, from 2.27 to 5.17, respectively). Frontal raise and LR-flexed had greater sEMG RMS than LR-internal (ES: 2.55, from 1.28 to 3.60 and 5.70, from 3.55 to 7.37, respectively). No further difference was observed.
The sEMG RMS amplitude for
medial deltoid is shown in
Figure 2. Exercise × phase interaction (
p = 0.002, F = 35.7, η
2 = 0.973) was found. With the exception of LR-internal, greater (
p < 0.05, F = 380.8, partial η
2 = 0.982) sEMG RMS was found during the concentric vs. eccentric phase. During the concentric phase, sEMG RMS was greater in LR-neutral than LR-external (ES: 1.47, from 0.43 to 2.38), frontal raise (ES: 10.28, from 6.67 to 13.01), and LR-flexed (ES: 6.41, from 4.04 to 8.23). Both LR-external and LR-internal had greater sEMG RMS than frontal raise (ES: 11.20, from 7.29 to 14.17 and ES: 8.00, from 5.13 to 10.19, respectively) and LR-flexed (ES: 8.10, from 5.20 to 10.32 and ES: 4.17, from 2.48 to 5.51, respectively). LR-flexed showed greater sEMG RMS than frontal raise (ES: 8.10, from 5.20 to 11.00). During the eccentric phase, LR-internal showed greater sEMG RMS than LR-external (ES: 9.32, from 6.03 to 11.83), LR-neutral (ES: 7.85, from 5.03 to 10.01), frontal raise (ES: 17.69, from 11.62 to 22.26), and LR-flexed (ES: 7.39, from 4.71 to 9.44). Both LR-neutral and LR-flexed had greater sEMG RMS than LR-external (ES: 4.58, from 2.77 to 6.00 and ES: 2.53, from 1.27 to 2.58, respectively) and frontal raise (ES: 15.62, from 6.88 to 22.19 and ES: 13.60, from 8.89 to 17.15, respectively). LR-external showed greater sEMG RMS than frontal raise (ES: 10.50, from 6.82 to 13.30). No further difference was observed.
The sEMG RMS amplitude for
posterior deltoid is shown in
Figure 2. Exercise × phase interaction (
p < 0.001, F = 234.4, η
2 = 0.996) was found. Whatever the exercise, greater (
p < 0.05, F = 151.9, partial η
2 = 0.995) sEMG RMS was found during the concentric vs. eccentric phase. During both the concentric and eccentric phase, LR-internal showed greater sEMG RMS compared with LR-external (ES: 16.48, from 10.72 to 20.86 and ES: 5.36, from 3.31 to 6.95, respectively), LR-neutral (ES: 10.34, from 6.71 to 13.09 and ES: 5.13, from 3.16 to 6.67, respectively), frontal raise (ES: 20.72, from 13.63 to 26.05 and ES: 12.28, from 6.01 to 18.51, respectively), and LR-flexed (ES: 11.41, from 7.43 to 14.42 and ES: 6.04, from 3.79 to 7.78, respectively). During both concentric and eccentric phase, LR-neutral showed greater sEMG RMS than LR-external (ES: 8.69, from 5.60 to 11.05 and ES: 1.51, from 0.46 to 2.43 respectively), frontal raise (ES: 14.74, from 9.66 to 18.58 and ES: 10.21, from 6.62 to 14.93, respectively), and LR-flexed (ES: 1.80, from 0.69 to 2.75 and ES: 1.89, from 0.77 to 2.85, respectively). During the concentric phase, LR-flexed showed greater sEMG RMS than LR-external (ES: 6.65, from 4.21 to 8.82) and frontal raise (ES: 12.99, from 8.49 to 16.39), and LR-external had greater sEMG RMS than frontal raise (ES: 7.55, from 4.82 to 9.63). During the eccentric phase, both LR-external and LR-flexed showed greater sEMG RMS than frontal raise (ES: 5.99, from 3.75 to 7.92 and ES: 6.89, from 4.37 to 8.82, respectively). No further difference was observed.
The sEMG RMS amplitude for
upper trapezius is shown in
Figure 2. Exercise × phase interaction (
p = 0.002, F = 37.3, η
2 = 0.974) was found. Whatever the exercise, greater (
p < 0.05, F = 165.8, partial η
2 = 0.996) sEMG RMS was found during the concentric vs. eccentric phase. During the concentric phase, sEMG RMS was greater in LR-internal compared with LR-external (ES: 5.43, from 3.37 to 7.04), LR-neutral (ES: 3.86, from 2.26 to 5.14), frontal raise (ES: 7.18, from 4.97 to 9.18), and LR-flexed (ES: 2.66, from 1.36 to 3.72). LR-flexed had greater sEMG RMS than LR-external (ES: 3.72, from 2.15 to 4.97) and frontal raise (ES: 6.03, from 3.78 to 7.77). Both LR-external and LR-neutral had greater sEMG RMS than frontal raise (ES: 3.44, from 1.95 to 4.63 and ES: 3.65, from 2.10 to 4.89, respectively). During the eccentric phase, both LR-internal and LR-flexed had greater sEMG RMS compared with LR-external (ES: 6.50, from 4.11 to 8.34 and ES: 7.11, from 4.53 to 9.10, respectively), LR-neutral (ES: 8.15, from 5.23 to 10.38 and ES: 9.26, from 5.98 to 11.75, respectively), and frontal raise (ES: 5.84, from 3.65 to 7.54 and ES: 5.83, from 3.65 to 7.53, respectively). No further difference was observed.
The sEMG RMS amplitude for
pectoralis major is shown in
Figure 2. Exercise × phase interaction (
p < 0.001, F = 111.4, η
2 = 0.999) was found. Whatever the exercise, greater (
p < 0.05, F = 115.2, partial η
2 = 0.996) sEMG RMS was found during the concentric vs. eccentric phase. During the concentric phase, sEMG RMS was very largely greater in frontal raise compared with LR-external (ES: 21.31, from 14.03 to 26.70), LR-neutral (ES: 29.90, from 19.72 to 37.55), LR-internal (ES: 30.39, from 20.04 to 38.16), and LR-flexed (ES: 34.21, from 22.57 to 42.96). During the eccentric phase, sEMG RMS of clavicular was very largely greater in frontal raise compared with LR-external (ES: 11.61, from 7.57 to 14.68), LR-neutral (ES: 11.01, from 7.16 to 13.92), LR-internal (ES: 12.46, from 8.13 to 15.74), and LR-flexed (ES: 12.36, from 8.07 to 15.61). No further difference was observed.
The sEMG RMS amplitude for
triceps brachii is shown in
Figure 2. Exercise × phase interaction was found (
p = 0.003, F = 28.2, η
2 = 0.966). Whatever the exercise, greater (
p < 0.05, F = 229.0, partial η
2 = 0.970) sEMG RMS was found during the concentric vs. eccentric phase. sEMG RMS was greater in LR-internal during the concentric and eccentric phase compared with LR-external (ES: 2.54, from 1.28 to 3.59 and ES: 5.81, from 3.63 to 7.50, respectively), LR-neutral (ES: 1.17, from 0.17 to 2.06 and ES: 4.45, from 2.67 to 5.84, respectively), frontal raise (ES: 3.31, from 1.86 to 4.49 and ES: 17.07, from 11.21 to 21.49, respectively), and LR-flexed (ES: 0.91, from 0.09 to 1.78 and ES: 6.73, from 4.26 to 8.62, respectively). During the concentric phase, LR-external and LR-flexed showed greater sEMG RMS than LR-external (ES: 3.98, from 2.66 to 5.08 and ES: 3.78, from 2.50 to 4.85, respectively) and frontal raise (ES: 3.29, from 2.12 to 4.29 and ES: 3.66, from 2.41 to 4.71, respectively). LR-external had greater sEMG RMS than frontal raise (ES: 2.02, from 1.09 to 2.84). During the eccentric phase, sEMG RMS was greater in LR-external (ES: 6.93, from 4.40 to 8.87), LR-neutral (ES: 8.81, from 5.86 to 11.20), and LR-flexed (ES: 5.85, from 3.66 to 7.55) vs. frontal raise. No further difference was observed.
4. Discussion
The present study investigated the sEMG RMS in several agonist muscles in a range of shoulder raise exercises during the concentric and eccentric phase of each exercise. During the concentric phase, sEMG RMS in anterior deltoid was greater during frontal raise and LR-external. Medial deltoid was more active during the lateral raises, particularly when the humerus had a neutral or internal rotation. Posterior deltoid had greater sEMG RMS in LR-internal compared with all other exercises. Upper trapezius had greater sEMG RMS during LR-internal compared with all other exercises. The clavicular head of the pectoralis major was more active during frontal raise compared with all other exercises. Lastly, the lateral head of triceps brachii was more active in LR-internal compared with all other exercises. Although this muscle activity pattern was overall similar during the eccentric phase, anterior deltoid had similar activation in LR-external and LR-neutral and medial deltoid in LR-internal compared with all other exercises. The present findings showed unique muscle activation for each LR variations and frontal raise. Practitioners should thus select these exercises depending on the shoulders muscles that need to be activated at each occasion.
LR-external, LR-neutral, and LR-internal are performed abducting the humerus, which is rotated, respectively, externally, neutrally, or internally for the entire range of motion. For LR-external, the present results showed that the deltoids sEMG RMS was ~80% in
anterior, > ~48% in
medial, > ~36% in the
posterior head. For LR-neutral, sEMG RMS was similar in
medial and
posterior (~55% and ~52%), but lower in
anterior deltoid (~36%). For LR-internal, sEMG RMS was ~85% in
posterior, ~52% in
medial, and ~34% in
anterior deltoid, in line with previous results [
10]. Although
anterior,
medial, and
posterior deltoids act synergistically as humerus abductors on the frontal plane,
anterior deltoid is an internal, while
posterior deltoid is an external rotator of the humerus [
5]. The internal or external rotation of the humerus generates an increment in moment arm for
posterior and
anterior deltoid, respectively, thus increasing their activity [
5]. Additionally, bi-articular muscles show greater sEMG RMS at long compared with short muscle length [
27,
28], possibly because of changes in moment arm and muscle architecture [
29], modifications in both spinal and supraspinal mechanisms [
30], or also changes in the characteristics of motoneurons pool when a muscle is lengthened [
28]. Interestingly, although a computational study found that the humerus rotation could have led to negligible differences, here, the present competitive bodybuilders might have been able to increase the muscle activation for each exercise [
3]. Therefore, the present results seemed to confirm the data reported in the literature. It should be noted that, during the eccentric phase,
anterior deltoid showed similar sEMG RMS in LR-external vs. LR-neutral, possibly because of the greater control needed to decelerate the humerus, as reported previously [
9]. Similarly, during the eccentric phase, the greatest
medial deltoid activity was found in LR-internal, which possibly needs greater control [
8]. The
triceps brachii activation was overall greater in LR-internal > LR-neutral > LR-external. The greater the internal rotation of the humerus, the greater the weight of the forearm + wrist + dumbbell system becomes against the gravity. Indeed, the internal rotation of the humerus lets the elbow’s mobility be free against the gravity, whereas the external rotation puts the elbow’s extension in favor of the gravity, fixing the elbow joint. Therefore, because all exercises were performed at a fixed elbow angle,
triceps brachii increased its elbow-stabilizer role when rotating internally the humerus. The internal rotation of the humerus also increased the role of
upper trapezius in LR-internal > LR-neutral/LR-external. Indeed, when rotating internally the humerus, the scapulae are elevated and rotated upward [
11], thus augmenting the
upper trapezius activity. Lastly, the clavicular head of the
pectoralis major showed similar low activity in all LR variations, indicating that it plays a marginal role when the humerus is abducted laterally.
LR-flexed, compared to the other LR variations, was performed with the flexed elbow at 90°, and the humerus rotated neutrally. However: (i) the length of the lever on the frontal plane was shorter than the other LR-variations, and (ii) the forearm was placed forward on the sagittal plane. Firstly, considering the point (i), the sEMG RMS of
medial deltoid was hence lower compared to the other LR variations, where the arm was lifted almost straight on the frontal plane, increasing the length of the lever. Secondly, considering the point (ii), the forearm placed forward on the sagittal plan increased the activity of
anterior deltoid as frontal humerus flexors. Indeed, greater sEMG RMS compared to LR-neutral and LR-internal was found here. Moreover, because of the forward weight that leads the humerus to rotate internally, the
posterior deltoid had to counteract as an external rotator, thus stabilizing the rotation of the humerus [
29]. Therefore, the sEMG RMS was similar to LR-neutral and greater than LR-external. Such an internal rotation of the humerus also led to elevate the external rotation of the scapulae [
5], so that
upper trapezius was more active during both the concentric and eccentric phase compared to LR-external and LR-neutral. It should be also noted that the flexed elbow increased the muscle length at which
triceps brachii had to contract to stabilize the elbow joint [
27]. This might have led to similar and greater sEMG RMS in LR-flexed compared with LR-neutral and LR-external, respectively, in line with previous results [
27]. Lastly, the clavicular head of the
pectoralis major seemed to play a marginal role in LR-flexed, as pointed out by the low level of activation.
Frontal raise was performed on the sagittal plane, lifting up the upper limb in neutral rotation by a frontal flexion, with a straight elbow. As a whole, frontal raise appears to mainly require the activation of the
anterior deltoid and the clavicular head of the
pectoralis major. Indeed, both muscles showed the greatest activity compared with all the remaining exercises. In line, when the humerus moved towards a flexion across the sagittal plane, the sEMG RMS in
anterior deltoid and the clavicular head of the
pectoralis major was reported to increase [
14]. In contrast, given the low activation level recorded here, both
medial and
posterior deltoids appeared to play a negligible role in frontal raise, in line with previous results [
9].
Upper trapezius showed relatively low activity, possibly because, when flexing the humerus, the scapulae tend to rotate internally and to be depressed [
11]. Interestingly, albeit the least active compared with all exercises during the concentric phase, the sEMG RMS in
upper trapezius was similar to LR-external and LR-neutral during the eccentric phase. This might depend on the need to stabilize the scapula when the upper limb was accelerating downward, as previously reported [
9]. Lastly,
triceps brachii showed poor activation, possibly due to the neutral humerus rotation that
per se stabilized the elbow joint on the craniocaudal axis.
Some limitations accompany the present procedures. Firstly, the data shown are specific for the population involved and the technical requirements provided to perform each exercise. Nonetheless, although it is acknowledged that different populations may result in different findings, the present population made us confident about the goodness of the technique and muscle recruitment. Similarly, even though greater load could result in different outcomes, this may also reduce the quality of the technique execution for each exercise, and we are confident that here the load was suitable for the population. Moreover, although a dedicated authority continuously monitored the use of steroids, we could not have controlled for, and we do not know how the possible use of steroids would affect muscle activation. Lastly, some authors have divided
deltoid muscle into seven different parts [
31]. However, sEMG was not able to distinguish each of them, so we made the traditional 3-part subdivision.

 ,
, 






{kind=link}
{kind=link}