Can the Neuromuscular Performance of Young Athletes Be Influenced by Hormone Levels and Different Stages of Puberty?

 ,
,  ,
, 
 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Sample
2.2. Ethics
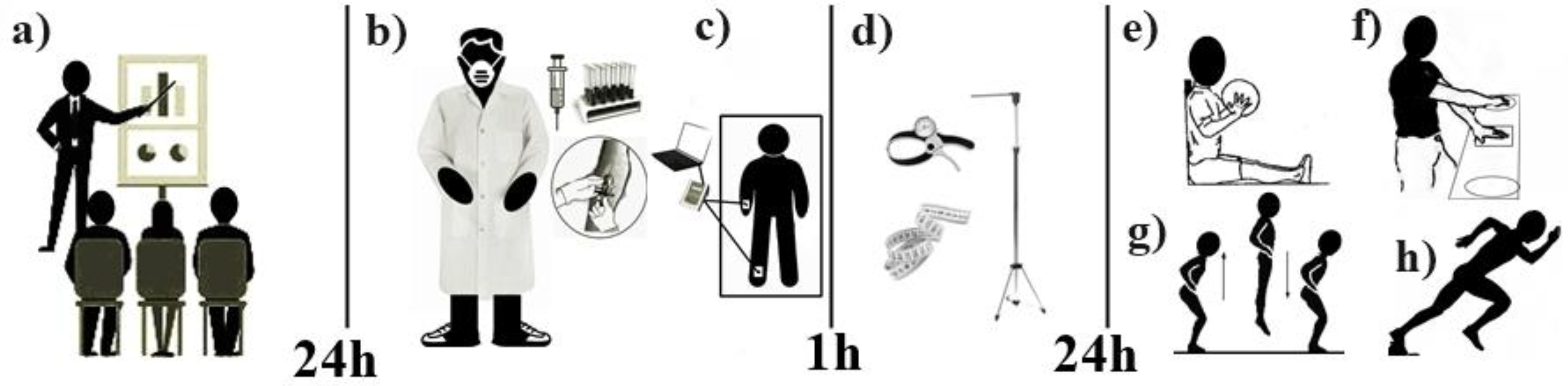
3. Procedures
4. Body Composition Assessment
5. Anthropometric Assessments
6. Biological Maturation Analysis
7. Neuromuscular Performance Analysis
7.1. Upper Limb Power
7.2. Lower Limb Power
7.3. Upper Limb Speed
7.4. Body Speed with Change of Direction
7.5. Biochemical Analyses of Hormone Levels
8. Statistics
9. Results
10. Discussion
11. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Malina, R.M.; Rogol, A.D.; Cumming, S.P.; Silva, D.R.; Figueiredo, A.J. Biological maturation of youth athletes: Assessment and implications. Br. J. Sports Med. 2015, 49, 852–859. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Christophi, C.A.; Farioli, A.; Baur, D.M.; Moffatt, S.; Zollinger, T.W.; Kales, S.N. Association Between Push-up Exercise Capacity and Future Cardiovascular Events Among Active Adult Men. JAMA Netw. Open 2019, 2, e188341. [Google Scholar] [CrossRef]
- Sañudo, B.; Sánchez-Hernández, J.; Bernardo-Filho, M.; Abdi, E.; Taiar, R.; Núñez, J. Abdi Integrative Neuromuscular Training in Young Athletes, Injury Prevention, and Performance Optimization: A Systematic Review. Appl. Sci. 2019, 9, 3839. [Google Scholar] [CrossRef]
- DiCesare, C.A.; Montalvo, A.; Foss, K.D.B.; Thomas, S.M.; Hewett, T.E.; Jayanthi, N.A.; Myer, G.D. Sport Specialization and Coordination Differences in Multisport Adolescent Female Basketball, Soccer, and Volleyball Athletes. J. Athl. Train. 2019, 54, 1105–1114. [Google Scholar] [CrossRef] [PubMed]
- Gillen, Z.M.; Shoemaker, M.E.; McKay, B.D.; Bohannon, N.A.; Gibson, S.M.; Cramer, J.T. Muscle strength, size, and neuromuscular function before and during adolescence. Eur. J. Appl. Physiol. 2019, 119, 1619–1632. [Google Scholar] [CrossRef]
- Bradley, S.H.; Lawrence, N.; Steele, C.; Mohamed, Z. Precocious puberty. Br. Med. J. 2020, 368, l6597. [Google Scholar] [CrossRef]
- Moodie, J.L.; Campisi, S.C.; Salena, K.; Wheatley, M.; Vandermorris, A.; Bhutta, Z.A. Timing of Pubertal Milestones in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Adv. Nutr. 2020, 11, 951–959. [Google Scholar] [CrossRef]
- Alfonsi, V.; Scarpelli, S.; D’Atri, A.; Stella, G.; De Gennaro, L. Later School Start Time: The Impact of Sleep on Academic Performance and Health in the Adolescent Population. Int. J. Environ. Res. Public Health 2020, 17, 2574. [Google Scholar] [CrossRef]
- Wondisford, F.E. Puberty Cases; Springer Science and Business Media LLC: Berlin, Germany, 2020; Volume 1, pp. 279–287. ISBN 978-3-030-39572-8. [Google Scholar] [CrossRef]
- Lloyd, R.S.; Oliver, J.L.; Faigenbaum, A.D.; Myer, G.D.; Croix, M.B.A.D.S. Chronological Age vs. Biological Maturation. J. Strength Cond. Res. 2014, 28, 1454–1464. [Google Scholar] [CrossRef]
- Cavarzere, P.; Gaudino, R.; Sandri, M.; Ramaroli, D.A.; Pietrobelli, A.; Zaffanello, M.; Guzzo, A.; Salvagno, G.L.; Piacentini, G.; Antoniazzi, F. Growth hormone retesting during puberty: A cohort study. Eur. J. Endocrinol. 2020, 182, 559–567. [Google Scholar] [CrossRef]
- Ponzi, D.; Flinn, M.V.; Muehlenbein, M.P.; Nepomnaschy, P.A. Hormones and human developmental plasticity. Mol. Cell. Endocrinol. 2020, 505, 110721. [Google Scholar] [CrossRef] [PubMed]
- Pinto, V.C.M.; Dos Santos, P.G.M.D.; Dantas, M.P.; Araújo, J.P.D.F.; Cabral, S.D.A.T. Relationship between bone age, hormonal markers and physical capacity in adolescents. J. Hum. Growth Dev. 2017, 27, 77–83. [Google Scholar] [CrossRef]
- De Almeida-Neto, P.F.; Dantas, P.M.S.; Pinto, V.C.M.; Cesário, T.D.M.; Campos, N.M.R.; Santana, E.E.; De Matos, D.G.; Aidar, F.J.; Cabral, B.G.D.A.T. Biological Maturation and Hormonal Markers, Relationship to Neuromotor Performance in Female Children. Int. J. Environ. Res. Public Health 2020, 17, 3277. [Google Scholar] [CrossRef]
- Cole, T.J.; Ahmed, M.; Preece, M.; Hindmarsh, P.; Dunger, D.B. The relationship between Insulin-like Growth Factor 1, sex steroids and timing of the pubertal growth spurt. Clin. Endocrinol. 2015, 82, 862–869. [Google Scholar] [CrossRef]
- Forrest, G.F. Testosterone Combined with Electrical Stimulation and Standing: Effect on Muscle and Bone; Kessler Foundation West Orange United States: East Hanover, NJ, USA, 2017. [Google Scholar]
- Fink, J.E. The Role of Hormones in Exercise-Induced Muscle Hypertrophy. In Endocrinology of Physical Activity and Sport; Springer Science and Business Media LLC: Berlin, Germany, 2020; pp. 391–398. [Google Scholar] [CrossRef]
- Suchomel, T.; Nimphius, S.; Stone, M.H. The Importance of Muscular Strength in Athletic Performance. Sports Med. 2016, 46, 1419–1449. [Google Scholar] [CrossRef] [PubMed]
- Fraser, B.J.; Blizzard, L.; Cleland, V.; Schmidt, M.D.; Smith, K.J.; Gall, S.L.; Dwyer, T.; Venn, A.; Magnussen, C.G. Factors associated with muscular fitness phenotypes in Australian children: A cross-sectional study. J. Sports Sci. 2019, 38, 38–45. [Google Scholar] [CrossRef]
- Wang, D.X.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachex.-Sarcopenia Muscle 2019, 11, 3–25. [Google Scholar] [CrossRef]
- Goswami, B.; Roy, A.S.; Dalui, R.; Bandyopadhyay, A. Impact of Pubertal Growth on Physical Fitness. Am. J. Sports Sci. Med. 2014, 2, 34–39. [Google Scholar] [CrossRef]
- Tanner, J.M. Growth and maturation during adolescence. Nutr. Rev. 1981, 39, 43–55. [Google Scholar] [CrossRef]
- Arruda, A.; Aoki, M.S.; Freitas, C.G.; Spigolon, L.M.; Franciscon, C.; Moreira, A. Testosterone Concentration and Lower Limb Power Over an Entire Competitive Season in Elite Young Soccer Players. J. Strength Cond. Res. 2015, 29, 3380–3385. [Google Scholar] [CrossRef]
- Chavarro, J.E.; Watkins, D.J.; Afeiche, M.C.; Zhang, Z.; Sánchez, B.N.; Cantonwine, D.; Mercado-García, A.; Blank-Goldenberg, C.; Meeker, J.D.; Téllez-Rojo, M.M.; et al. Validity of Self-Assessed Sexual Maturation Against Physician Assessments and Hormone Levels. J. Pediatr. 2017, 186, 172–178.e3. [Google Scholar] [CrossRef] [PubMed]
- STROBE Checklist Strengthening the Reporting of Observational Studies in Epidemiology. Available online: https://www.strobe-statement.org/index.php?id=strobe-home (accessed on 15 March 2020).
- Karupaiah, T. Limited (ISAK) profiling The International Society for the Advancement of Kinanthropometry (ISAK). J. Ren. Nutr. Metab. 2018, 3, 11. [Google Scholar] [CrossRef]
- Cabral, S.D.A.T.; Cabral, B.G.D.A.T.; Pinto, V.C.M.; de Andrade, R.D.; de Oliveira Borges, M.V.; Dantas, P.M.S. Relationship between bone age and anthropometry and physical fitness in young volleyball players. Braz. J. Sport Sci. 2016, 38, 69–75. [Google Scholar]
- Medeiros, R.M.; Arrais, R.F.; Azevedo, J.C.; Pinto, V.C.; Ronque, E.R.; Dantas, P.M. Prediction of pubertal maturation from anthropometric variables: Proposal for a non-invasivemethod. J. Sports Med. Phys. Fit. 2018, 58, 638–643. [Google Scholar]
- Mirwald, R.L.; Baxter-Jones, A.D.; Bailey, D.A.; Beunen, G.P. An assessment of maturity from anthropometric measurements. Med. Sci. Sports Exerc. 2002, 34, 689–694. [Google Scholar] [PubMed]
- Mello, J.B.; Nagorny, G.A.K.; Haiachi, M.D.C.; Gaya, A.R. Projeto Esporte Brasil: Perfil da aptidão física relacionada ao desempenho esportivo de crianças e adolescentes. Rev. Bras. Cineantropom. Desempenho Hum. 2016, 18, 658–666. [Google Scholar] [CrossRef]
- Forza, J.; Edmundson, C.J. Comparison between Gyko inertial sensor and Chrono jump contact mat for the assessment of Squat Jump, Countermovement Jump and Abalakov Jump in amateur male volleyball players, amateur male rugby players and in high school students. J. Multi. Discip. Eng. Sci. Technol. 2019, 6, 9982–9988. [Google Scholar]
- Aboelwafa, H.S.; Elkilany, A.M.; Al-Hariri, M. Measurement of Physiological Fitness Level Among Male College Students in Dammam, Saudi Arabia Using the European Fitness Test–EuroFit. Glob. J. Health Sci. 2019, 11, 21. [Google Scholar] [CrossRef]
- Nimphius, S.; Callaghan, S.J.; Bezodis, N.E.; Lockie, R.G. Change of Direction and Agility Tests: Challenging our current measures of performance. Strength Cond. J. 2018, 40, 26–38. [Google Scholar] [CrossRef]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients. Anesthesia Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Santo, H.E.; Daniel, F.B. Calcular e apresentar tamanhos do efeito em trabalhos científicos (1): As limitações do p <0.05 na análise de diferenças de médias de dois grupos. Rev. Port. Investig. Comport. Soc. 2015, 1, 3–16. [Google Scholar] [CrossRef]
- Perini, T.A.; De Oliveira, G.L.; Ornellas, J.D.S.; De Oliveira, F.P. Cálculo do erro técnico de medição em antropometria. Rev. Bras. Med. Esporte 2005, 11, 81–85. [Google Scholar] [CrossRef]
- Crewther, B.T.; Obminski, Z.; Cook, C. The Effect of Steroid Hormones on the Physical Performance of Boys and Girls during an Olympic Weightlifting Competition. Pediatr. Exerc. Sci. 2016, 28, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.-Y.; Soelaiman, I.-N.; Mohamed, I.N.; Shahar, S.; Teng, N.I.M.F.; Ramli, E.S.M.; Ahmad, F.; Aminuddin, A.; Ngah, W.Z.W. Testosterone is associated with age-related changes in bone health status, muscle strength and body composition in men. Aging Male 2012, 15, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Aslam, S. Endocrine Events Involved in Puberty: A Revisit to Existing Knowledge. Life Sci. 2020, 1, 12. [Google Scholar] [CrossRef]
- Dantas, M.P.; Silva, L.F.; Gantois, P.; Silva, L.M.; Dantas, R.N.; Cabral, B.T. Relationship between maturation and explosive strength in young rowers. Motricidade 2018, 14, 112–121. [Google Scholar]
- Scheffler, C.; Hermanussen, M. Growth in childhood and adolescence. Int. Encycl. Biol. Anthropol. 2018, 1–11. [Google Scholar] [CrossRef]
- Massarani, F.A.; Canella, D.S.; Brito, F.B.; Citelli, M.; Koury, J.C. Assessment of trends of nutritional status, central obesity, and growth profile using anthropometric measurements in adolescent athletes from a sport-oriented public school. J. Sports Med. Phys. Fit. 2019, 59, 1885–1891. [Google Scholar] [CrossRef] [PubMed]
- Rogol, A.D. Human sex chromosome aneuploidies: The hypothalamic–pituitary–gonadal axis. Am. J. Med Genet. Part C Semin. Med. Genet. 2020, 184, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Wirth, K.; Mickel, C.; Hartmann, H.; Keiner, M. Muscle and bone development. Elite Youth Cycl. 2018, 3–35. [Google Scholar] [CrossRef]
- Vinaik, R.; Gus, E.I.; Jeschke, M.G. Anabolic and Anticatabolic Agents in Burns. In Handbook of Burns; Springer: Cham, Germay, 2019; pp. 287–297. [Google Scholar]
- Pasiakos, S.; Shankaran, M.; Berryman, C.; Margolis, L.; Lieberman, H.; Karl, J.P.; Young, A.; Montano, M.; Matthews, M.; Bizieff, A.A.; et al. Effects of Testosterone on Mixed Muscle Protein Synthesis and Proteome Dynamics During Energy Deficit. Curr. Dev. Nutr. 2020, 4, 649. [Google Scholar] [CrossRef]
- Distefano, L.J.; Martinez, J.; Crowley, E.; Matteau, E.; Kerner, M.S.; Boling, M.C.; Nguyen, A.-D.; Trojian, T. Maturation and Sex Differences in Neuromuscular Characteristics of Youth Athletes. J. Strength Cond. Res. 2015, 29, 2465–2473. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Values |
|---|---|
| N° Sample (%) | 37 (100%) |
| Bodyweight (kg) | 37.3 ± 9.68 |
| Stature (cm) | 145.0 ± 7.57 |
| Bodymass index (m²) | 17.4 ± 3.67 |
| Fat (%) | 22.7 ± 9.21 |
| Lean Mass (kg) | 28.4 ± 5.84 |
| Fat Mass (kg) | 8.96 ± 5.43 |
| Chronological age | 11.3 ± 0.96 |
| Skeletalmaturation (bone age) | 10.3 ± 1.21 |
| Sexual maturation | −2.13 ± 0.90 |
| Somaticmaturation (PSG) | −2.61 ± 0.77 |
| Testosterone(ng/dL) | 106.6 ± 103.4 |
| Estradiol (ng/dL) | 33.2 ± 42.6 |
| Growthhormone(ng/dL) | 2.62 ± 2.93 |
| Upperlimbpower (m) | 1.70 ± 0.43 |
| SquatJump (W/kg) | 25.8 ± 6.95 |
| Upperlimbspeed (s) | 12.5 ± 3.67 |
| BScD (s) | 8.42 ± 0.71 |
| Variables | TRT (ng/dL) | EST (ng/dL) | GH (ng/dL) | |||
|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | |
| Leanmass (kg) | 0.40 * | 0.02 | −0.08 | 0.6 | 0.37 * | 0.02 |
| Fat (%) | −0.27 | 0.09 | −0.30 | 0.06 | −0.43 * | 0.006 |
| Sexualmaturation | 0.30 | 0.06 | 0.08 | 0.6 | 0.28 | 0.1 |
| Skeletalmaturation | 0.27 | 0.2 | 0.10 | 0.5 | 0.17 | 0.2 |
| Somaticmaturation | 0.27 | 0.09 | 0.08 | 0.6 | 0.19 | 0.2 |
| ULP (m) | 0.23 | 0.1 | −0.09 | 0.5 | 0.09 | 0.5 |
| SJ (W/kg) | 0.28 | 0.08 | −0.33 * | 0.04 | −0.07 | 0.6 |
| ULS (s) | −0.06 | 0.7 | 0.18 | 0.2 | 0.03 | 0.8 |
| BScD’s (s) | 0.07 | 0.6 | 0.33 * | 0.04 | −0.20 | 0.9 |
| Control of the effect of Sexual Maturation | ||||||
| r | p-Value | r | p-Value | r | p-Value | |
| Leanmass (kg) | 0.24 | 0.2 | 0.23 | 0.1 | 0.21 | 0.2 |
| Fat (%) | 0.20 | 0.2 | 0.29 | 0.08 | −0.38 * | 0.02 |
| ULP (m) | 0.08 | 0.6 | 0.16 | 0.3 | 0.06 | 0.7 |
| SJ (W/kg) | 0.13 | 0.4 | 0.49 * | 0.002 | −0.31 | 0.05 |
| ULS (s) | 0.02 | 0.8 | 0.22 | 0.1 | 0.12 | 0.4 |
| COD’s (s) | 0.10 | 0.5 | 0.34 * | 0.04 | −0.00 | 0.9 |
| Control of the effect of skeletal maturation | ||||||
| r | p-Value | r | p-Value | r | p-Value | |
| Leanmass (kg) | 0.24 | 0.1 | 0.27 | 0.09 | 0.10 | 0.5 |
| Fat (%) | 0.23 | 0.1 | 0.28 | 0.09 | −0.41 * | 0.01 |
| ULP (m) | 0.10 | 0.5 | 0.18 | 0.2 | 0.00 | 0.9 |
| SJ (W/kg) | 0.16 | 0.3 | 0.49 * | 0.002 | 0.22 | 0.1 |
| ULS (s) | 0.02 | 0.8 | 0.24 | 0.1 | 0.10 | 0.5 |
| BScD’s (s) | 0.08 | 0.6 | 0.33 * | 0.04 | 0.01 | 0.9 |
| Control of the effect of somatic maturation | ||||||
| r | p-Value | r | p-Value | r | p-Value | |
| Leanmass (kg) | 0.24 | 0.1 | 0.30 | 0.07 | 0.17 | 0.3 |
| Fat (%) | 0.25 | 0.1 | 0.29 | 0.08 | −0.42 * | 0.009 |
| ULP (m) | 0.08 | 0.6 | 0.18 | 0.2 | 0.03 | 0.8 |
| SJ (W/kg) | 0.16 | 0.3 | 0.46 * | 0.004 | 0.22 | 0.1 |
| ULS (s) | 0.01 | 0.9 | 0.22 | 0.1 | 0.09 | 0.5 |
| BScD’s (s) | 0.08 | 0.6 | 0.33 * | 0.04 | 0.01 | 0.9 |
| Variables | Sexual Maturation | Skeletal Maturarion | Somatic Maturation | |||
|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | |
| Lean Mass (kg) | 0.77 * | <0.0001 | 0.78 * | <0.0001 | 0.84 * | <0.0001 |
| Fat (%) | −0.32 | 0.05 | −0.21 | 0.1 | −0.11 | 0.4 |
| TRT (ng/dL) | 0.30 | 0.06 | 0.27 | 0.1 | 0.27 | 0.9 |
| EST (ng/dL) | 0.08 | 0.6 | 0.10 | 0.5 | 0.08 | 0.6 |
| GH (ng/dL) | 0.26 | 0.1 | 0.17 | 0.2 | 0.19 | 0.2 |
| ULP (cm) | 0.52 * | 0.0008 | 0.54 * | 0.0004 | 0.59 * | 0.0001 |
| SJ (W/kg) | 0.61 * | <0.0001 | 0.58 | 0.0001 | 0.55 * | 0.0003 |
| ULS (s) | −0.28 | 0.08 | −0.33 * | 0.04 | −0.27 | 0.9 |
| BScD (s) | −0.07 | 0.6 | −0.03 | 0.8 | −0.04 | 0.8 |
| Control of the Effect of TRT (ng/dL) | ||||||
| r | p-Value | r | p-Value | r | p-Value | |
| Lean Mass (kg) | 0.74 * | <0.0001 | 0.76 * | <0.0001 | 0.83 * | <0.0001 |
| Gordura (%) | 0.25 | 0.1 | 0.15 | 0.3 | 0.04 | 0.7 |
| ULP (m) | 0.48 * | 0.002 | 0.51 * | 0.001 | 0.56 * | 0.0003 |
| SJ (W/kg) | 0.57 * | 0.0002 | 0.54 * | 0.0005 | 0.51 * | 0.001 |
| ULS (s) | −0.27 | 0.09 | −0.33 * | 0.04 | −0.26 | 0.1 |
| BScD (s) | −0.09 | 0.5 | −0.05 | 0.7 | −0.06 | 0.7 |
| Control of the Effect of EST (ng/dL) | ||||||
| r | p-Value | r | p-Value | r | p-Value | |
| Lean Mass (kg) | 0.78 * | <0.0001 | 0.80 * | <0.0001 | 0.85 * | <0.0001 |
| Gordura (%) | −0.31 | 0.06 | 0.19 | 0.2 | −0.09 | 0.5 |
| ULP (m) | 0.53 * | 0.0007 | 0.56 * | 0.0003 | 0.60 * | <0.0001 |
| SJ (W/kg) | 0.68 * | <0.0001 | 0.66 * | <0.0001 | 0.62 * | <0.0001 |
| ULS (s) | −0.30 | 0.06 | −0.36 * | 0.02 | −0.29 | 0.07 |
| BScD (s) | −0.10 | 0.5 | −0.07 | 0.6 | −0.07 | 0.6 |
| Control of the Effect of GH (ng/dL) | ||||||
| r | p-Value | r | p-Value | r | p-Value | |
| Lean Mass (kg) | 0.78 * | <0.0001 | 0.78 * | <0.0001 | 0.85 * | <0.0001 |
| Gordura (%) | −0.23 | 0.1 | 0.15 | 0.3 | −0.03 | 0.8 |
| ULP (m) | 0.52 * | 0.001 | 0.54 * | 0.0006 | 0.59 * | 0.0001 |
| SJ (W/kg) | 0.65 * | <0.0001 | 0.60 * | <0.0001 | 0.58 * | 0.0001 |
| ULS (s) | −0.30 | 0.06 | −0.34 * | 0.03 | −0.28 | 0.08 |
| BScD (s) | 0.08 | 0.6 | 0.33 * | 0.04 | 0.01 | 0.9 |
| Variables | Sexual Maturation | Skeletal Maturarion | Somatic Maturation | ||||||
|---|---|---|---|---|---|---|---|---|---|
| r² | β | p | r² | β | p | r² | β | p | |
| Leanmass (kg) | 0.59 * | 0.11 | 0.00 | 0.61 * | 0.15 | 0.00 | 0.71 * | 0.10 | 0.00 |
| Fat (%) | 0.10 | −0.03 | 0.05 | 0.04 | −0.02 | 0.1 | 0.01 | −0.00 | 0.4 |
| TRT (ng/dL) | 0.09 | 0.00 | 0.06 | 0.07 | 0.00 | 0.1 | 0.07 | 0.00 | 0.09 |
| EST (ng/dL) | 0.00 | 0.00 | 0.6 | 0.11 | 0.00 | 0.5 | 0.00 | 0.00 | 0.6 |
| GH (ng/dL) | 0.07 | 0.08 | 0.1 | 0.03 | 0.07 | 0.2 | 0.03 | 0.05 | 0.24 |
| ULP (m) | 0.27 * | 1.06 | 0.00 | 0.29 * | 1.38 | 0.00 | 0.35 * | 0.95 | 0.00 |
| SJ (W/kg) | 0.37 * | 0.07 | 0.00 | 0.33 * | 0.09 | 0.00 | 0.30 * | 0.05 | 0.00 |
| ULS (s) | 0.08 | −0.07 | 0.08 | 0.11 * | −0.10 | 0.04 | 0.07 | −0.05 | 0.09 |
| BScD (s) | 0.00 | −0.08 | 0.6 | 0.00 | −0.05 | 0.8 | 0.00 | −0.04 | 0.8 |
| TRT (ng/dL) | EST (ng/dL) | GH (ng/dL) | |||||||
| r² | β | p | r² | β | p | r² | β | p | |
| Leanmass (kg) | 0.13 * | 6.31 | 0.02 | 0.00 | −0.65 | 0.6 | 0.00 | 0.03 | 0.6 |
| Fat (%) | 0.07 | −3.24 | 0.09 | 0.09 | −1.48 | 0.06 | 0.19 * | −0.13 | 0.00 |
| Sexual maturation | 0.09 | 34.7 | 0.06 | 0.00 | 3.95 | 0.6 | 0.07 | 0.81 | 0.1 |
| Skeletalmaturation | 0.07 | 24.6 | 0.1 | 0.01 | 4.17 | 0.5 | 0.03 | 0.43 | 0.2 |
| Somaticmaturation | 0.07 | 39.7 | 0.09 | 0.00 | 5.20 | 0.6 | 0.03 | 0.75 | 0.2 |
| ULP (m) | 0.05 | 53.0 | 0.1 | 0.00 | −9.12 | 0.5 | 0.00 | 0.56 | 0.5 |
| SJ (W/kg) | 0.08 | 4.26 | 0.08 | 0.11 * | −2.11 | 0.04 | 0.00 | −0.03 | 0.6 |
| ULS (s) | 0.00 | −1.90 | 0.7 | 0.03 | 2.36 | 0.2 | 0.00 | 0.02 | 0.8 |
| BScD (s) | 0.00 | 10.2 | 0.6 | 0.11 * | 19.8 | 0.04 | 0.00 | −0.07 | 0.9 |
| Variables | TRT (ng/dL) | EST (ng/dL) | GH (ng/dL) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| U | %E | |P% | U | %E | |P% | U | %E | |P% | |
| Leanmass (kg) | 1 * | 50.5 | 49.5 | 0 | 77.4 | 22.6 | 1 * | 77.9 | 22.05 |
| Fat (%) | 1 * | 83.0 | 17.0 | 1 * | 94.6 | 5.34 | 0 | 85.0 | 15.0 |
| Sexual maturation | 0 | 80.3 | 19.7 | 0 | 99.9 | 0.06 | 1 * | 99.9 | 0.02 |
| Skeletalmaturation | 1 * | 90.0 | 10.0 | 0 | 95.9 | 4.10 | 0 | 97.3 | 2.62 |
| Somaticmaturation | 1 * | 87.4 | 12.6 | 1 * | 99.5 | 0.46 | 1 * | 99.1 | 0.84 |
| ULP (m) | 1 * | 51.0 | 49.0 | 0 | 89.7 | 10.22 | 0 | 97.3 | 1.65 |
| SJ (W/kg) | 1 * | 78.6 | 23.4 | 1 * | 90.5 | 9.42 | 1 * | 98.5 | 1.44 |
| ULS (s) | 1 * | 75.4 | 24.6 | 1 * | 73.7 | 26.3 | 1 * | 98.5 | 1.45 |
| BScD (s) | 1 * | 80.4 | 19.6 | 1 * | 97.8 | 2.16 | 1 * | 94.9 | 5.09 |
| Sexual maturarion | Skeletalmaturation | Somaticmaturation | |||||||
| U | %E | |P% | U | %E | |P% | U | %E | |P% | |
| Leanmass (kg) | 0 | 67.5 | 32.5 | 1 * | 64.9 | 35.1 | 1 * | 16.9 | 83.1 |
| Fat (%) | 1 * | 74.8 | 25.2 | 1 * | 79.3 | 20.7 | 1 * | 84.8 | 15.2 |
| TRT (ng/dL) | 1 * | 72.6 | 27.4 | 1 * | 80.7 | 19.3 | 0 | 85.0 | 15.0 |
| EST (ng/dL) | 0 | 85.7 | 14.3 | 1 * | 86.6 | 13.4 | 1 * | 87.5 | 12.5 |
| GH (ng/dL) | 1 * | 94.2 | 5.73 | 1 * | 95.0 | 5.00 | 1 * | 94.8 | 5.2 |
| ULP (m) | 1 * | 48.3 | 51.7 | 1 * | 44.6 | 55.4 | 1 * | 40.0 | 60.0 |
| SJ (W/kg) | 0 | 70.3 | 29.7 | 1 * | 66.0 | 34.0 | 0 | 69.7 | 30.3 |
| ULS (s) | 0 | 97.7 | 2.30 | 1 * | 96.6 | 3.35 | 1 * | 98.5 | 1.5 |
| BScD (s) | 0 | 99.1 | 0.90 | 1 * | 98.2 | 1.75 | 1 * | 97.0 | 3.00 |
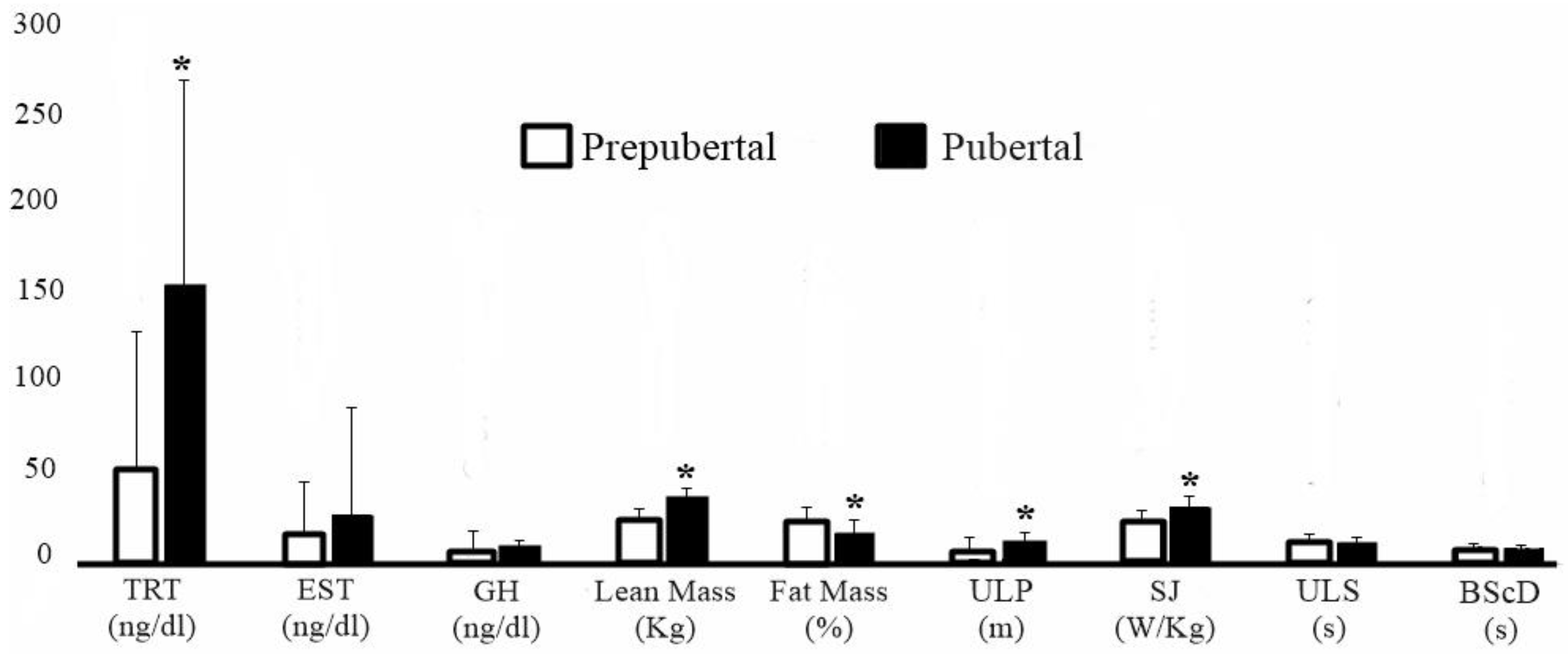
| Variables | TRT < 100 (ng/dL) | TRT > 100 (ng/dL) | ES | IC (95%) | p |
|---|---|---|---|---|---|
| Sexual maturation | −2.13 ± 0.90 | −1.49 ± 0.95 | −0.69 | [−1.41–0.01] | 0.05 |
| Skeletal maturation | 10.3 ± 1.21 | 11.0 ± 1.07 | −0.59 | [−1.30–0.12] | 0.08 |
| Somaticmaturation | −2.61 ± 0.77 | −2.18 ± 0.65 | −0.58 | [−1.29–0.13] | 0.08 |
| Fat (%) | 22.7 ± 9.21 | 15.6 ± 8.06 * | 0.80 | [0.07–1.52] | 0.02 |
| Leanmass (kg) | 28.4 ± 5.84 | 31.9 ± 6.45 | −0.58 | [−1.29–0.13] | 0.1 |
| TRT (ng/dL) | 40.0 ± 26.4 | 221.7 ± 91.8 * | 3.13 | [2.11–4.15] | <0.0001 |
| EST (ng/dL) | 20.7 ± 55.1 | 20.7 ± 22.8 | 0.00 | [−0.69–0.69] | 0.9 |
| GH (ng/dL) | 2.27 ± 3.10 | 3.26 ± 2.58 | −0.36 | [−1.03–0.36] | 0.3 |
| ULP (m) | 1.70 ± 0.43 | 1.85 ± 0.54 * | 0.28 | [−0.41–0.98] | 0.04 |
| SJ (W/kg) | 25.8 ± 6.95 | 30.2 ± 7.54 * | 0.60 | [−1.32–0.10] | 0.03 |
| ULS (s) | 12.5 ± 3.67 | 12.3 ± 3.81 | 0.05 | [−0.64–0.75] | 0.8 |
| BScD(s) | 8.42 ± 0.71 | 8.64 ± 0.88 | −0.29 | [−0.99–0.41] | 0.4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida-Neto, P.F.d.; de Matos, D.G.; Pinto, V.C.M.; Dantas, P.M.S.; Cesário, T.d.M.; da Silva, L.F.; Bulhões-Correia, A.; Aidar, F.J.; Cabral, B.G.d.A.T. Can the Neuromuscular Performance of Young Athletes Be Influenced by Hormone Levels and Different Stages of Puberty? Int. J. Environ. Res. Public Health 2020, 17, 5637. https://doi.org/10.3390/ijerph17165637
Almeida-Neto PFd, de Matos DG, Pinto VCM, Dantas PMS, Cesário TdM, da Silva LF, Bulhões-Correia A, Aidar FJ, Cabral BGdAT. Can the Neuromuscular Performance of Young Athletes Be Influenced by Hormone Levels and Different Stages of Puberty? International Journal of Environmental Research and Public Health. 2020; 17(16):5637. https://doi.org/10.3390/ijerph17165637
Chicago/Turabian StyleAlmeida-Neto, Paulo Francisco de, Dihogo Gama de Matos, Vanessa Carla Monteiro Pinto, Paulo Moreira Silva Dantas, Tatianny de Macêdo Cesário, Luíz Felipe da Silva, Alexandre Bulhões-Correia, Felipe José Aidar, and Breno Guilherme de Araújo Tinôco Cabral. 2020. "Can the Neuromuscular Performance of Young Athletes Be Influenced by Hormone Levels and Different Stages of Puberty?" International Journal of Environmental Research and Public Health 17, no. 16: 5637. https://doi.org/10.3390/ijerph17165637
APA StyleAlmeida-Neto, P. F. d., de Matos, D. G., Pinto, V. C. M., Dantas, P. M. S., Cesário, T. d. M., da Silva, L. F., Bulhões-Correia, A., Aidar, F. J., & Cabral, B. G. d. A. T. (2020). Can the Neuromuscular Performance of Young Athletes Be Influenced by Hormone Levels and Different Stages of Puberty? International Journal of Environmental Research and Public Health, 17(16), 5637. https://doi.org/10.3390/ijerph17165637