Impact of Exercises and Chair Massage on Musculoskeletal Pain of Young Musicians


Abstract
1. Introduction
2. Methods
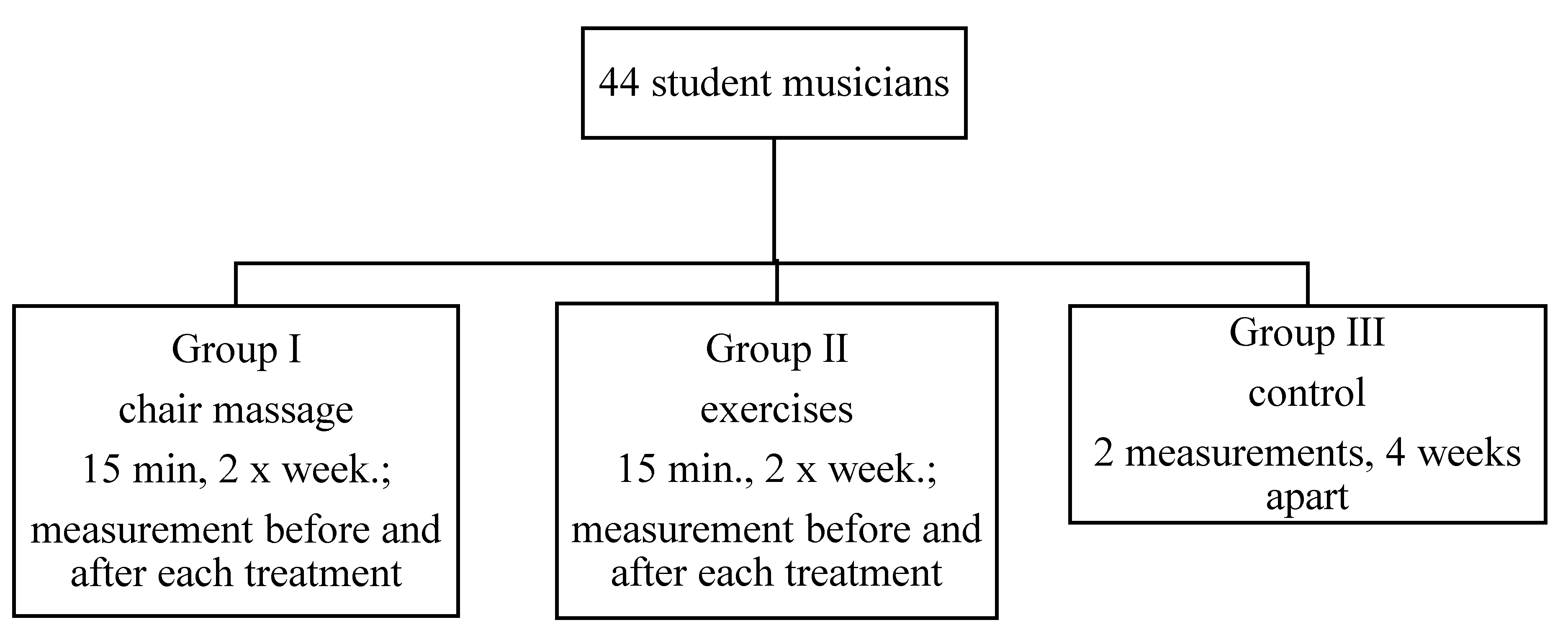
2.1. Study Population
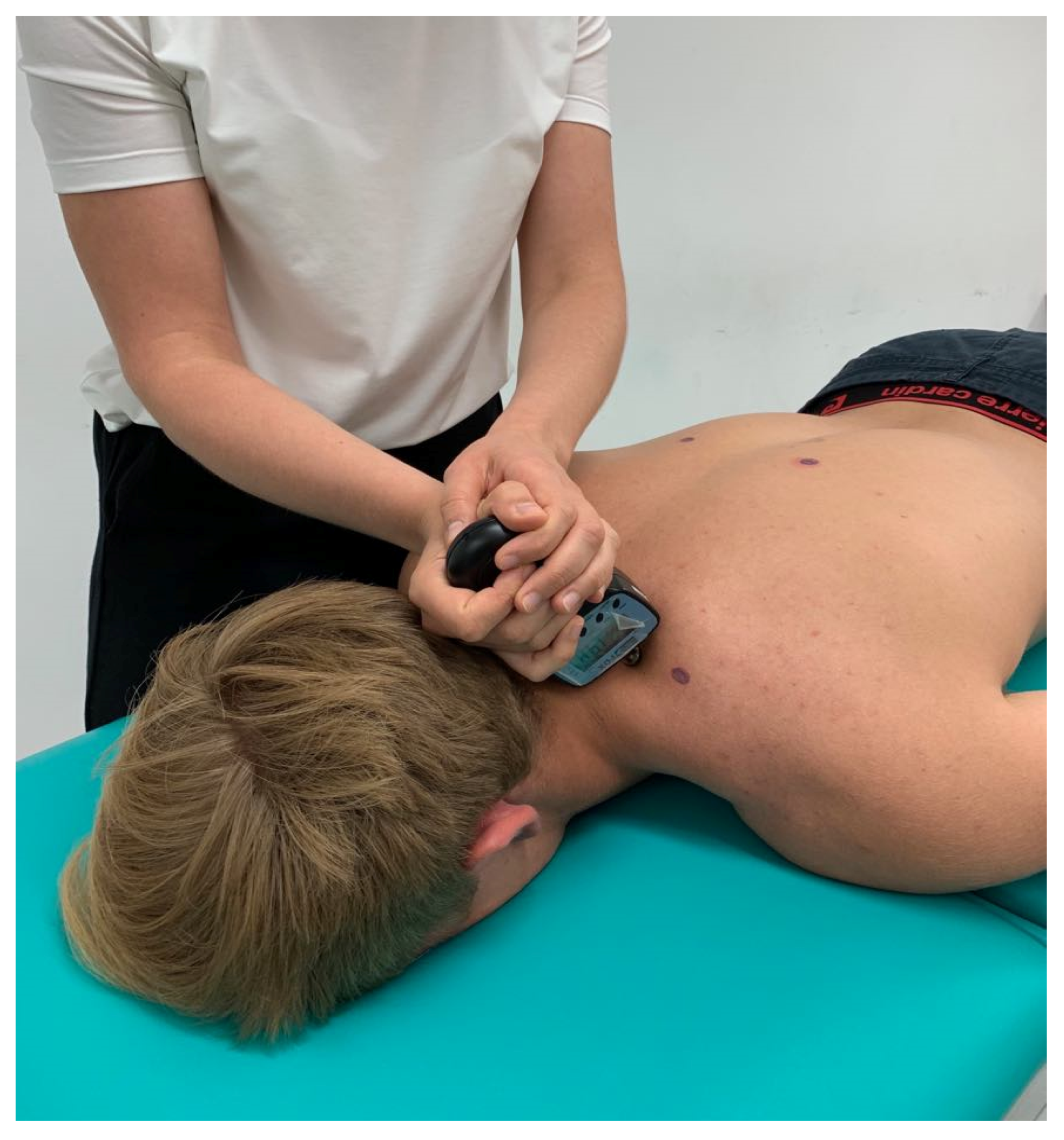
2.2. Physioprophylaxis Methods
2.3. Measurement Methods
2.4. Data Analysis
3. Results
3.1. Questionnaire Results
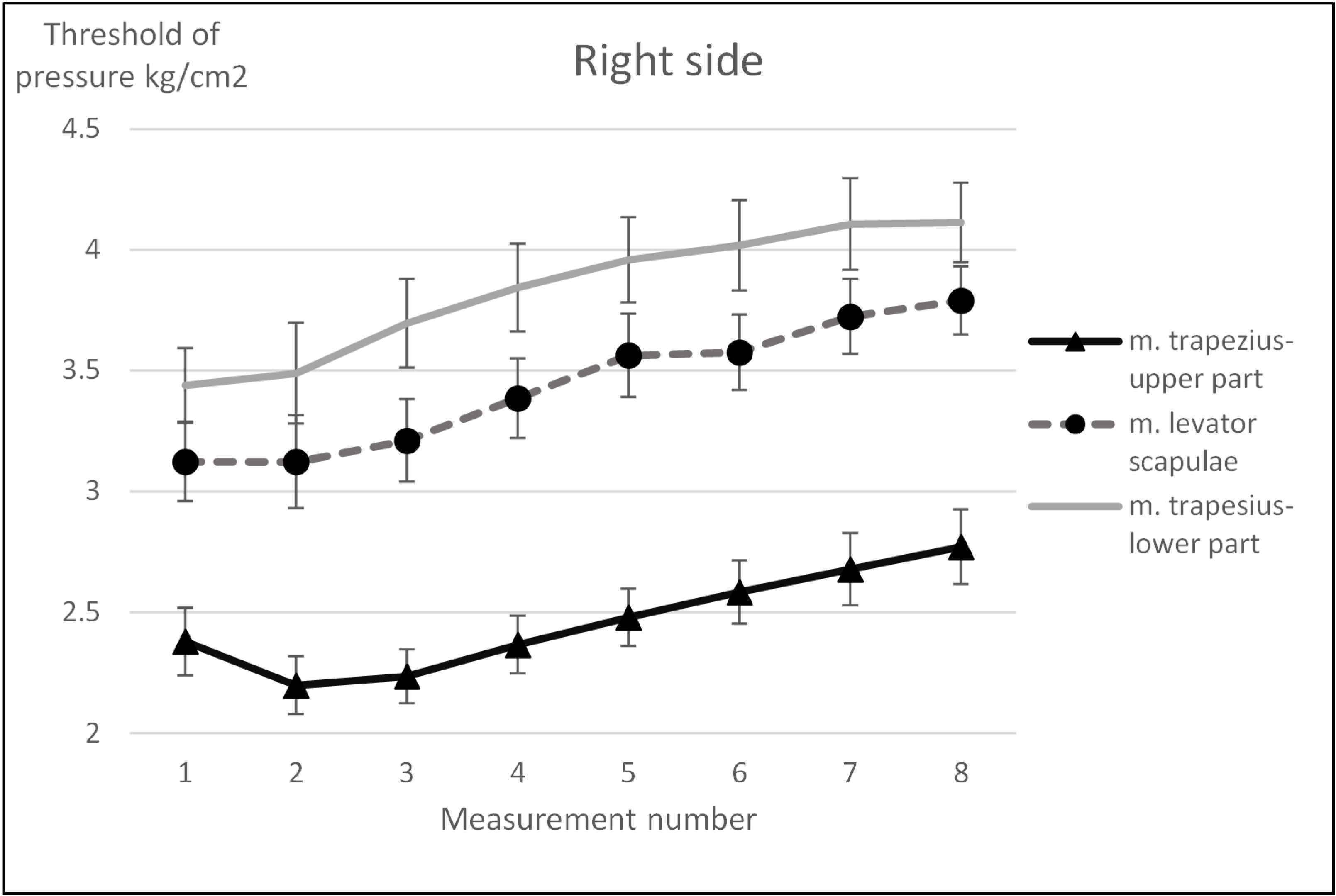
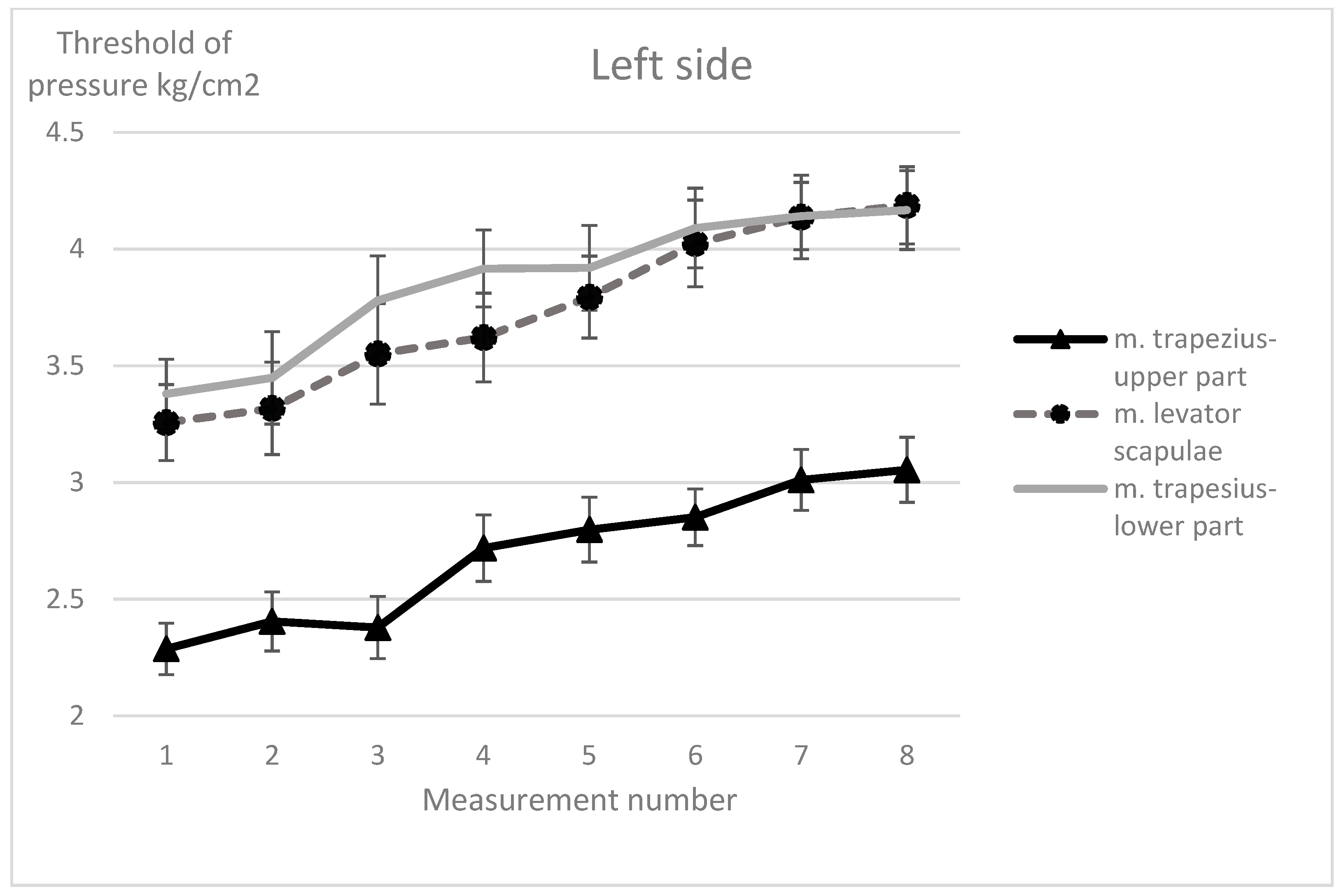
3.2. Algometry Measurements Results
4. Discussion
4.1. Study Limitation
4.2. Recommendations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ajidahun, A.T.; Mudzi, W.; Wood, W.-A.; Myezwa, H. Musculoskeletal problems among string instrumentalists in South Africa. S. Afr. J. Physiother. 2017, 73, 7. [Google Scholar] [CrossRef] [PubMed]
- Demaree, C.J.; Wang, K.; Lin, P.H. Thoracic outlet syndrome affecting high-performance musicians playing bowed string instruments. Vascular 2017, 25, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Piñeiro, P.; Díaz-Pereira, M.P.; Martínez, A. Common postural defects among music students. J. Bodyw. Mov. Ther. 2015, 19, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, A.; Tsuchida, E. Relationship Between Wind Instrument Playing Habits and Symptoms of Temporomandibular Disorders in Non-Professional Musicians. Open Dent. J. 2016, 10, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Piñeiro, P.; Díaz-Pereira, M.P.; Martínez, A. Musicians, postural quality and musculoskeletal health: A literature’s review. J. Bodyw. Mov. Ther. 2017, 21, 157–172. [Google Scholar] [CrossRef]
- Stanhope, J.; Tooher, R.; Pisaniello, D.; Weinstein, P. Have musicians’ musculoskeletal symptoms been thoroughly addressed? A systematic mapping review. Int. J. Occup. Med. Environ. Health 2019, 32, 291–331. [Google Scholar] [CrossRef] [PubMed]
- Stanek, J.L.; Komes, K.D.; Murdock, F.A. A Cross-Sectional Study of Pain Among U.S. College Music Students and Faculty. Med. Probl. Perform. Artist. 2017, 32, 20–26. [Google Scholar] [CrossRef]
- Cygańska, A.; Truszczyńska-Baszak, A.; DrzalGrabiec, J.; Tarnowski, A. Assessment of body parameters’ symmetry in child violinists. J. Back Musculoskelet. Rehabil. 2017, 30, 1081–1086. [Google Scholar] [CrossRef]
- Aparicio, L.; Lã, F.; Silva, A. Pain and Posture of Children and Adolescents Who Learn the Accordion as Compared with Non-Musician Students. Med. Probl. Perform. Artist. 2016, 31, 187–192. [Google Scholar] [CrossRef]
- Árnason, K.; Arnason, A.; Briem, K. Playing-Related Musculoskeletal Disorders Among Icelandic Music Students: Differences Between Students Playing Classical vs Rhythmic Music. Med. Probl. Perform. Artists 2014, 29, 74–79. [Google Scholar] [CrossRef]
- Ballenberger, N.; Möller, D.; Zalpour, C. Musculoskeletal Health Complaints and Corresponding Risk Factors Among Music Students: Study Process, Analysis Strategies, and Interim Results from a Prospective Cohort Study. Med. Probl. Perform. Artists 2018, 33, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Kochem, F.B.; Silva, J.G. Prevalence and Associated Factors of Playing-Related Musculoskeletal Disorders in Brazilian Violin Players. Med. Probl. Perform. Artist. 2017, 32, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Kok, L.M.; Haitjema, S.; Groenewegen, K.A.; Rietveld, A.B.M. The Influence of a Sudden Increase in Playing Time on Playing-Related Musculoskeletal Complaints in High-Level Amateur Musicians in a Longitudinal Cohort Study. PLoS ONE 2016, 11, e0163472. [Google Scholar] [CrossRef]
- Andersen, L.N.; Mann, S.; Juul-Kristensen, B.; Søgaard, K. Comparing the Impact of Specific Strength Training vs General Fitness Training on Professional Symphony Orchestra Musicians: A Feasibility Study. Med. Probl. Perform. Artist. 2017, 32, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.; Driscoll, T.; Ackermann, B. Development of a specific exercise programme for professional orchestral musicians. Inj. Prev. 2013, 19, 257–263. [Google Scholar] [CrossRef]
- Chan, C.; Driscoll, T.; Ackermann, B.J. Effect of a musicians’ exercise intervention on performance-related musculoskeletal disorders. Med. Probl. Perform. Artist. 2014, 29, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Spahn, C. Treatment and prevention of music performance anxiety. In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2015; Volume 217, pp. 129–140. [Google Scholar]
- Spahn, C.; Voltmer, E.; Mornell, A.; Nusseck, M. Health status and preventive health behavior of music students during university education: Merging prior results with new insights from a German multicenter study. Music Sci. 2017, 21, 213–229. [Google Scholar] [CrossRef]
- Árnason, K.; Briem, K.; Árnason, Á. Effects of an Education and Prevention Course for University Music Students on Their Body Awareness and Attitude toward Health and Prevention. Med. Probl. Perform. Artist. 2018, 33, 131–136. [Google Scholar] [CrossRef]
- Ralph, S. Therapeutic Chair Massage; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; ISBN 9780781742344. [Google Scholar]
- Cabak, A.; Mikicin, M.; Łyp, M.; Stanisławska, I.; Kaczor, R.; Tomaszewski, W. Preventive Chair Massage with Algometry to Maintain Psychosomatic Balance in White-Collar Workers. In Advances in Experimental Medicine and Biology; Springer: Berlin, Germany, 2017; Volume 1022, pp. 77–84. [Google Scholar]
- Engen, D.J.; Wahner-Roedler, D.L.; Vincent, A.; Chon, T.Y.; Cha, S.S.; Luedtke, C.A.; Loehrer, L.L.; Dion, L.J.; Rodgers, N.J.; Bauer, B.A. Feasibility and effect of chair massage offered to nurses during work hours on stress-related symptoms: A pilot study. Complement. Ther. Clin. Pract. 2012, 18, 212–215. [Google Scholar] [CrossRef]
- Park, G.; Kim, C.W.; Park, S.B.; Kim, M.J.; Jang, S.H. Reliability and usefulness of the pressure pain threshold measurement in patients with myofascial pain. Ann. Rehabil. Med. 2011, 35, 412–417. [Google Scholar] [CrossRef]
- Fischer, A.A. Pressure algometry over normal muscles. Standard values, validity and reproducibility of pressure threshold. Pain 1987, 30, 115–126. [Google Scholar] [CrossRef]
- Akamine, R.T.; Hirotsu, C.; Andersen, M.L.; Tufik, S. Musicians and Dystonia: Is Sleep Part of the Problem? Med. Probl. Perform. Artist. 2015, 30, 117. [Google Scholar] [CrossRef]
- Nie, H.; Kawczynski, A.; Madeleine, P.; Arendt-Nielsen, L. Delayed onset muscle soreness in neck/shoulder muscles. Eur. J. Pain 2005, 9, 653. [Google Scholar] [CrossRef] [PubMed]
- Kenny, D.; Ackermann, B. Performance-related musculoskeletal pain, depression and music performance anxiety in professional orchestral musicians: A population study. Psychol. Music 2015, 43, 43–60. [Google Scholar] [CrossRef]
- Cruder, C.; Falla, D.; Mangili, F.; Azzimonti, L.; Araújo, L.S.; Williamon, A.; Barbero, M. Profiling the Location and Extent of Musicians’ Pain Using Digital Pain Drawings. Pain Pract. 2018, 18, 53–66. [Google Scholar] [CrossRef] [PubMed]
- Woldendorp, K.H.; Boonstra, A.M.; Arendzen, J.H.; Reneman, M.F. Variation in occupational exposure associated with musculoskeletal complaints: A cross-sectional study among professional bassists. Int. Arch. Occup. Environ. Health 2018, 91, 215–223. [Google Scholar] [CrossRef]
- Baadjou, V.A.; Verbunt, J.A.; van Eijsden-Besseling, M.D.; Samama-Polak, A.L.; de Bie, R.A.; Smeets, R.J. PREvention STudy On preventing or reducing disability from musculoskeletal complaints in music school students (PRESTO): Protocol of a randomised controlled trial. J. Physiother. 2014, 60, 232. [Google Scholar] [CrossRef]
- Lee, S.-H.; Carey, S.; Dubey, R.; Matz, R. Intervention program in college instrumental musicians, with kinematics analysis of cello and flute playing: A combined program of yogic breathing and muscle strengthening-flexibility exercises. Med. Probl. Perform. Artist. 2012, 27, 85–94. [Google Scholar] [CrossRef]
- Klein, S.D.; Bayard, C.; Wolf, U. The Alexander Technique and musicians: A systematic review of controlled trials. BMC Complement. Altern. Med. 2014, 14, 414. [Google Scholar] [CrossRef]
- Rocha, S.F.; Marocolo, M.; Corrêa, E.N.V.; Morato, G.S.G.; da Mota, G.R. Physical activity helps to control music performance anxiety. Med. Probl. Perform. Artist. 2014, 29, 111–112. [Google Scholar] [CrossRef]
- Terry Loghmani, M.; Bayliss, A.J.; Clayton, G.; Gundeck, E. Successful treatment of a guitarist with a finger joint injury using instrument-assisted soft tissue mobilization: A case report. J. Man. Manip. Ther. 2015, 23, 246–253. [Google Scholar] [CrossRef][Green Version]
- Ying, L.F.; Evens, G.I.; Hashim, M.N.; Chiat, L.F. Tension Release in Piano Playing: Teaching Alexander Technique to Undergraduate Piano Majors. Procedia Soc. Behav. Sci. 2015, 174, 2413–2417. [Google Scholar] [CrossRef]
- Roos, M.; Roy, J.-S. Effect of a rehabilitation program on performance-related musculoskeletal disorders in student and professional orchestral musicians: A randomized controlled trial. Clin. Rehabil. 2018, 32, 1656–1665. [Google Scholar] [CrossRef] [PubMed]
- van Selms, M.K.A.; Ahlberg, J.; Lobbezoo, F.; Visscher, C.M. Evidence-based review on temporomandibular disorders among musicians. Occup. Med. (Chic. Ill) 2017, 67, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Engen, D.J.; Wahner-Roedler, D.L.; Nadolny, A.M.; Persinger, C.M.; Oh, J.K.; Spittell, P.C.; Loehrer, L.L.; Cha, S.S.; Bauer, B.A. The effect of chair massage on muscular discomfort in cardiac sonographers: A pilot study. BMC Complement. Altern. Med. 2010, 10, 50. [Google Scholar] [CrossRef]
- Šiško, P.K.; Videmšek, M.; Karpljuk, D. The Effect of a Corporate Chair Massage Program on Musculoskeletal Discomfort and Joint Range of Motion in Office Workers. J. Altern. Complement. Med. 2011, 17, 617–622. [Google Scholar] [CrossRef]
- Pelfort, X.; Torres-Claramunt, R.; Sánchez-Soler, J.F.; Hinarejos, P.; Leal-Blanquet, J.; Valverde, D.; Monllau, J.C. Pressure algometry is a useful tool to quantify pain in the medial part of the knee: An intra- and inter-reliability study in healthy subjects. Orthop. Traumatol. Surg. Res. 2015, 101, 559–563. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Massage | Exercises | Control | p-Value |
|---|---|---|---|---|
| (n = 16) | (n = 14) | (n = 14) | ||
| Age (years) | 20.6 ± 1.2 | 21.07 ± 2.0 | 20.1 ± 1.1 | 0.26 |
| Body mass (kg) | 58.7 ± 8.4 | 63.6 ± 12.9 | 61.48 ± 11.0 | 0.57 |
| Body height (cm) | 168 ± 6.9 | 170.4 ± 8.2 | 169.8 ± 6.8 | 0.78 |
| Weekly playing time (hours) | 24.8 ± 10.8 | 21.4 ± 10.4 | 24.1 ± 10.3 | 0.74 |
| Duration of playing (years) | 11.9 ± 3.4 | 11.9 ± 2.6 | 11.8 ± 2.6 | 0.63 |
| Participants reporting current PRMD (n) | 10 | 9 | 10 | 0.87 |
| Variable | Massage (n = 16) | Exercises (n = 14) | Control (n = 14) | |||
|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | |
| Right Side | ||||||
| m. trapezius (upper part) | 2.3 ± 0.8 | 2.8 ± 0.9 | 2.3 ± 0.9 | 2.4 ± 0.8 | 2.8 ± 0.9 | 2.5 ± 1.0 |
| m. levator scapulae C | 3.1 ± 0.9 | 3.8 ± 0.9 | 3.0 ± 1.0 | 3.4 ± 0.9 | 3.5 ± 0.9 | 3.1 ± 0.9 |
| m. trapezius (lower part) C | 3.3 ± 0.8 | 4.0 ± 1.4 | 3.6 ± 0.9 | 3.9 ± 1.0 | 4.2 ± 1.2 | 3.5 ± 1.2 |
| Left Side | ||||||
| m. trapezius (upper part) B | 2.4 ± 0.7 | 3.0 ± 0.8 | 2.1 ± 0.4 | 2.6 ± 0.9 | 2.5 ± 0.7 | 2.5 ± 0.9 |
| m. levator scapulae B,C | 3.3 ± 1.1 | 4.3 ± 0.9 * | 3.0± 0.8 | 3.7± 0.8 | 3.5 ± 0.9 | 3.0 ± 1.0 |
| m. trapezius (lower part) | 3.4 ± 1.0 | 4.0 ± 0.7 | 3.3 ± 0.8 | 3.7 ± 1.0 | 4.1 ± 1.1 | 3.6 ± 1.1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cygańska, A.; Truszczyńska-Baszak, A.; Tomaszewski, P. Impact of Exercises and Chair Massage on Musculoskeletal Pain of Young Musicians. Int. J. Environ. Res. Public Health 2020, 17, 5128. https://doi.org/10.3390/ijerph17145128
Cygańska A, Truszczyńska-Baszak A, Tomaszewski P. Impact of Exercises and Chair Massage on Musculoskeletal Pain of Young Musicians. International Journal of Environmental Research and Public Health. 2020; 17(14):5128. https://doi.org/10.3390/ijerph17145128
Chicago/Turabian StyleCygańska, Anna, Aleksandra Truszczyńska-Baszak, and Paweł Tomaszewski. 2020. "Impact of Exercises and Chair Massage on Musculoskeletal Pain of Young Musicians" International Journal of Environmental Research and Public Health 17, no. 14: 5128. https://doi.org/10.3390/ijerph17145128
APA StyleCygańska, A., Truszczyńska-Baszak, A., & Tomaszewski, P. (2020). Impact of Exercises and Chair Massage on Musculoskeletal Pain of Young Musicians. International Journal of Environmental Research and Public Health, 17(14), 5128. https://doi.org/10.3390/ijerph17145128