Effects of Ultrafine Particles in Ambient Air on Primary Health Care Consultations for Diabetes in Children and Elderly Population in Ljubljana, Slovenia: A 5-Year Time-Trend Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Period, and Area of Observation
2.2. Observed Population
2.3. Data Collection
2.3.1. Observed Health Outcomes
2.3.2. Observed UFP and PM Data and Meteorological Data
2.3.3. Data on Seasonal Factors and Pollen Concentration
2.4. Statistical Analysis
2.4.1. Data Description
2.4.2. Correlation Analysis
2.4.3. Temporal Relationship Analysis
3. Results
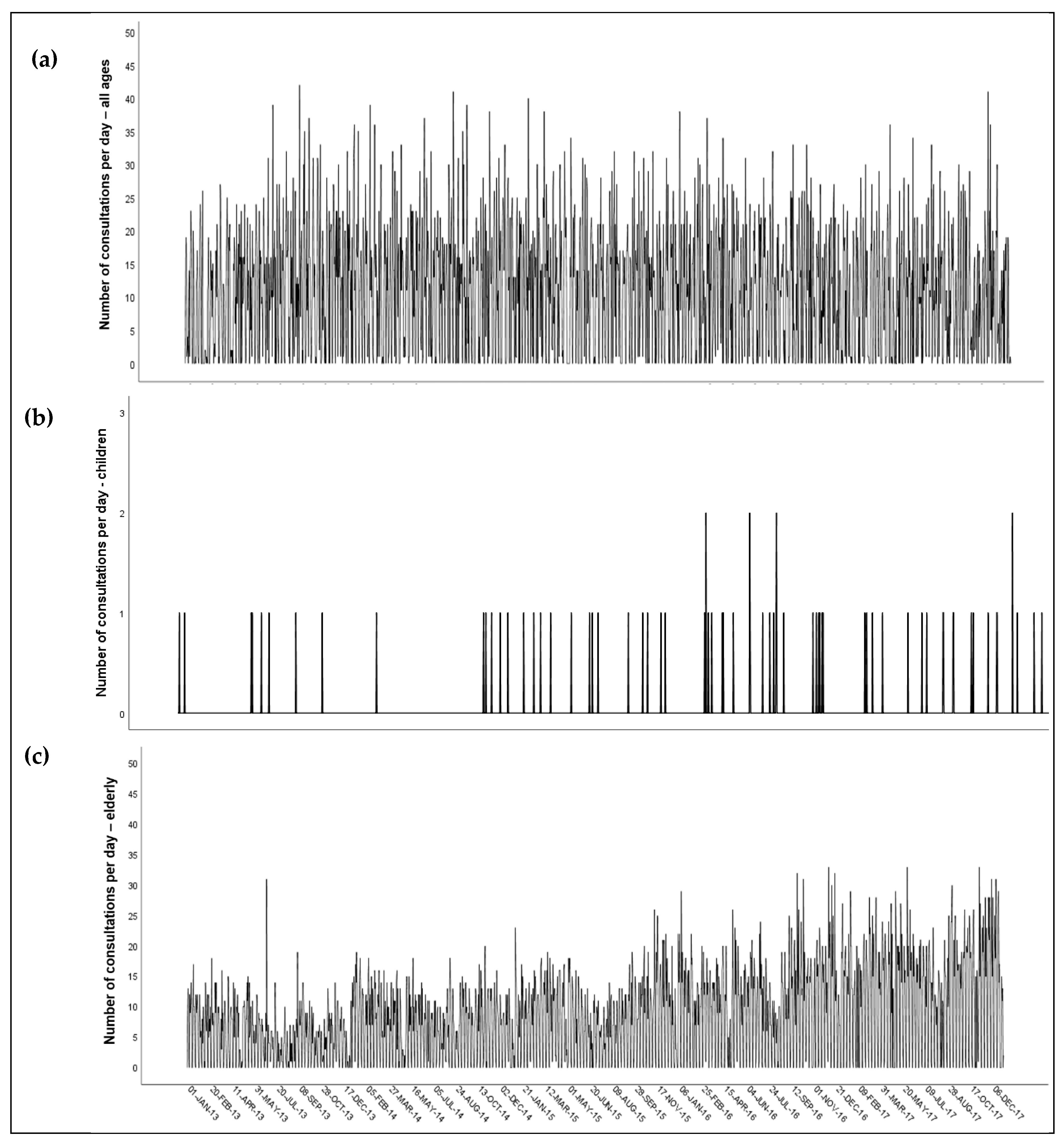
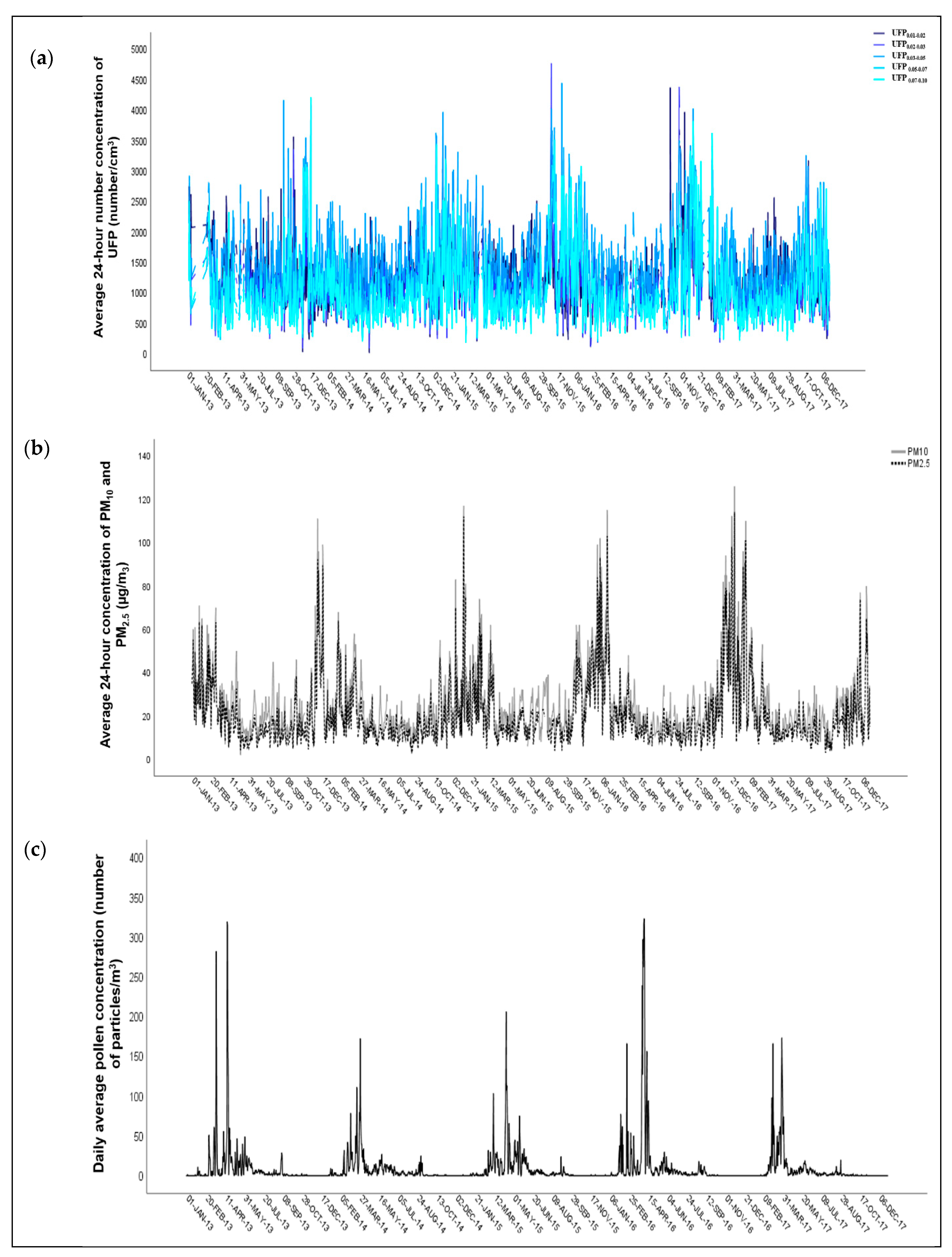
3.1. Data Description
3.2. Correlation Analysis
3.3. Relationship Analysis
4. Discussion
4.1. Limitations of the Study
4.2. Strenghts of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Li, Y.; Xu, L.; Shan, Z.; Teng, W.; Han, C. Association between air pollution and type 2 diabetes: An updated review of the literature. Ther. Adv. Endocrinol. Metab. 2019, 10, 1–15. [Google Scholar] [CrossRef] [PubMed]
- WHO. Air Pollution. Available online: https://www.who.int/health-topics/air-pollution#tab=tab_1 (accessed on 13 May 2020).
- Lelieveld, J.; Klingmüller, K.; Pozzer, A.; Pöschl, U.; Fnais, M.; Daiber, A.; Münzel, T. Cardiovascular disease burden from ambient air pollution in Europe reassessed using novel hazard ratio functions. Eur. Heart. J. 2019, 40, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe. Noncommunicable diseases and air pollution. In Proceedings of the WHO European high-level Conference on Noncommunicable diseases, Ashgabat, Turkmenistan, 9–10 April 2019.
- WHO. Review of Evidence on Health Aspects of Air Pollution—REVIHAAP Project; Technical report; WHO Regional Office for Europe: Copenhagen, Denmark, 2013; Available online: http://www.euro.who.int/__data/assets/pdf_file/0004/193108/REVIHAAP-Final-technical-report-final-version.pdf?ua=1 (accessed on 13 May 2020).
- Polonsky, K.S. The past 200 years in diabetes. N. Engl. J. Med. 2012, 367, 1332–1340. [Google Scholar] [CrossRef]
- Nolan, C.J.; Damm, P.; Prentki, M. Type 2 diabetes across generations: From pathophysiology to prevention and management. Lancet 2011, 378, 169–181. [Google Scholar] [CrossRef]
- Balakumar, P.; Maung, U.K.; Jagadeesh, G. Prevalence and prevention of cardiovascular disease and diabetes mellitus. Pharm. Res. 2016, 11, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Andersn, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Air Quality in Europe—2019 Report; EEA Report No 10/2019; European Environment Agency: Copenhagen, Denmark, 2019; Available online: https://www.eea.europa.eu/publications/air-quality-in-europe-2019 (accessed on 13 May 2020).
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio-respiratory mortality: A review. Environ. Health 2013, 12. [Google Scholar] [CrossRef]
- Lu, F.; Xu, D.; Cheng, Y.; Dong, S.; Guo, C.; Jiang, X.; Zheng, X. Systematic review and meta-analysis of the adverse health effects of ambient PM2.5 and PM10 pollution in the Chinese population. Environ. Res. 2015, 136, 196–204. [Google Scholar] [CrossRef]
- Mustafic, H.; Jabre, P.; Caussin, C.; Murad, M.H.; Escolano, S.; Tafflet, M.; Perier, M.-C.; Marijon, E.; Vernerey, D.; Empana, J.-P.; et al. Main air pollutants and myocardial infarction: A systematic review and meta-analysis. J. Am. Med. Assoc. 2012, 307, 713–721. [Google Scholar] [CrossRef]
- Shah, A.S.; Langrish, J.P.; Nair, H.; McAllister, D.A.; Hunter, A.L.; Donaldson, K.; Newby, D.E.; Mills, N.L. Global association of air pollution and heart failure: A systematic review and meta-analysis. Lancet 2013, 382, 1039–1048. [Google Scholar] [CrossRef]
- Raaschou-Nielsen, O.; Andersen, Z.J.; Beelen, R.; Samoli, E.; Staffogia, M.; Weinmayr, G.; Hoffmann, B.; Fischer, P.; Nieuwenhuijsen, M.J.; Brunekreef, B.; et al. Air pollution and lung cancer incidence in 17 European cohorts: Prospective analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). Lancet Oncol. 2013, 14, 813–822. [Google Scholar] [CrossRef]
- Cesaroni, G.; Forastiere, F.; Stafoggia, M.; Andersen, Z.J.; Badaloni, C.; Beelen, R.; Caracciolo, B.; de Faire, U.; Erbel, R.; Eriksen, K.T.; et al. Long term exposure to ambient air pollution and incidence of acute coronary events: Prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ 2014, 348, f7412. [Google Scholar] [CrossRef] [PubMed]
- Beelen, R.; Raaschou-Nielsen, O.; Stafoggia, M.; Andersen, Z.J.; Weinmayr, G.; Hoffmann, B.; Wolf, K.; Samoli, E.; Fischer, P.; Nieuwenhuijsen, M.; et al. Effects of long-term exposure to air pollution on natural-cause mortality: An analysis of 22 European cohorts within the multicentre ESCAPE project. Lancet 2014, 383, 785–795. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate matter air pollution and cardiovascular disease an update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef]
- Rajagopalan, S.; Brook, R.D. Air pollution and type 2 diabetes: Mechanistic insights. Diabetes 2012, 61, 3037–3045. [Google Scholar] [CrossRef]
- Liu, C.; Ying, Z.; Harkema, J.; Sun, Q.; Rajagopalan, S. Epidemiological and experimental links between air pollution and type 2 diabetes. Toxicol. Pathol. 2013, 41, 361–373. [Google Scholar] [CrossRef]
- Liu, C.; Xu, X.; Bai, Y.; Tse-Yao, W.; Rao, X.; Wang, A.; Sun, L.; Ying, Z.; Gushchina, L.; Maiseyeu, A.; et al. Air pollution-mediated susceptibility to inflammation and insulin resistance: Influence of CCR2 pathways in mice. Environ. Health Perspect. 2014, 122, 17–26. [Google Scholar] [CrossRef]
- Zheng, Z.; Xu, X.; Zhang, X.; Wang, A.; Zhang, C.; Hüttemann, M.; Grossman, L.I.; Chen, L.C.; Rajagopalan, S.; Sun, Q.; et al. Exposure to ambient particulate matter induces a NASH-like phenotype and impairs hepatic glucose metabolism in an animal model. J. Hepatol. 2013, 58, 148–154. [Google Scholar] [CrossRef]
- Sun, Q.; Yue, P.; Deiuliis, J.A.; Lumeng, C.N.; Kampfrath, T.; Mikolaj, M.B.; Cai, Y.; Ostrwski, M.C.; Lu, B.; Parthasarathy, S.; et al. Ambient air pollution exaggerates adipose inflammation and insulin resistance in a mouse model of diet-induced obesity. Circulation 2009, 119, 538–546. [Google Scholar] [CrossRef]
- Park, S.K.; Wang, W. Ambient Air Pollution and Type 2 Diabetes: A Systematic Review of Epidemiologic Research. Curr. Environ. Health Rep. 2014, 1, 275–286. [Google Scholar] [CrossRef]
- Wang, B.; Xu, D.; Jing, Z.; Liu, D.; Yan, S.; Wang, Y. Effect of long-term exposure to air pollution on type 2 diabetes mellitus risk: A systemic review and meta-analysis of cohort studies. Eur. J. Endocrinol. 2014, 171, R173–R182. [Google Scholar] [CrossRef]
- Eze, I.C.; Hemkens, L.G.; Bucher, H.C.; Hoffmann, B.; Schindler, C.; Künzli, N.; Schilowski, T.; Probst-Hensch, N.M. Association between ambient air pollution and diabetes mellitus in Europe and North America: Systematic review and meta-analysis. Environ. Health Perspect. 2015, 123, 381–389. [Google Scholar] [CrossRef]
- He, D.; Wu, S.; Zhao, H.; Qiu, H.; Fu, Y.; Li, X.; He, Y. Association between particulate matter 2.5 and diabetes mellitus: A meta-analysis of cohort studies. J. Diabetes Investig. 2017, 8, 687–696. [Google Scholar] [CrossRef]
- Yang, B.Y.; Qian, Z.M.; Li, S.; Chen, G.; Bloom, M.S.; Elliott, M.; Syberg, K.W.; Heinrich, J.; Markevych, I.; Wang, S.Q.; et al. Ambient air pollution in relation to diabetes and glucose-homoeostasis markers in China: A cross-sectional study with findings from the 33 Communities Chinese Health Study. Lancet Planet Health 2018, 2, e64–e73. [Google Scholar] [CrossRef]
- Diaz, E.; Marien, K.; Manahan, L.; Fox, J. Summary of Health Research on Ultrafine Particles; Report; Washington State Department of Health: Seattle, WA, USA, December 2019. Available online: https://www.doh.wa.gov/Portals/1/Documents/4000/334-454.pdf (accessed on 13 May 2020).
- Hussein, T.; Puustinen, A.; Aalto, P.P.; Mäkelä, J.M.; Hämeri, K.; Kulmala, M. Urban aerosol number size distributions. Atmos. Chem. Phys. 2004, 4, 391–411. [Google Scholar] [CrossRef]
- Shi, J.P.; Evans, D.E.; Khan, A.A.; Harrison, R.M. Sources and concentration of nanoparticles (<10 nm diameter) in the urban atmosphere. Atmos. Environ. 2001, 35, 1193–1202. [Google Scholar]
- Baldauf, R.W.; Devlin, R.B.; Gehr, P.; Giannelli, R.; Hassett-Sipple, B.; Jung, H.; Martini, G.; McDonald, J.; Sacks, J.; Walker, K. Ultrafine particle metrics and research considerations: Review of the 2015 UFP workshop. Int. J. Environ. Res. Public Health 2016, 13, 1054. [Google Scholar] [CrossRef]
- Manigrasso, M.; Natale, C.; Vitali, M.; Protano, C.; Avino, P. Pedestrians in Traffic Environments: Ultrafine Particle Respiratory Doses. Int. J. Environ. Res. Public Health 2017, 14, 288. [Google Scholar] [CrossRef]
- Marcias, G.; Fostinelli, J.; Catalani, S.; Uras, M.; Sanna, A.M.; Avataneo, G.; De Palma, G.; Fabbri, D.; Paganelli, M.; Lecca, L.I.; et al. Composition of Metallic Elements and Size Distribution of Fine and Ultrafine Particles in a Steelmaking Factory. Int. J. Environ. Res. Public Health 2018, 15, 1192. [Google Scholar] [CrossRef] [PubMed]
- Kreyling, W.G.; Semmler-Behnke, M.; Möller, W. Ultrafine particle-lung interactions: Does size matter? J. Aerosol. Med. 2006, 19, 74–83. [Google Scholar] [CrossRef]
- Li, N.; Georas, S.; Alexis, N.; Fritz, P.; Xia, T.; Williams, M.A.; Horner, E.; Nel, A. A work group report on ultrafine particles (AAAAI) why ambient ultrafine and engineered nanoparticles should receive special attention for possible adverse health outcomes in humans. J. Allergy Clin. Immunol. 2016, 138, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Sioutas, C.; Cho, A.; Schmitz, D.; Misra, C.; Sempf, J.; Wang, M.; Oberley, T.; Froines, J.; Nel, A. Ultrafine particulate pollutants induce oxidative stress and mitochondrial damage. Environ. Health Perspect. 2003, 111, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, A.; Tamrakar, S.; Aglawe, A.; Lad, H.; Srivastava, R.K.; Mishra, D.K.; Tiwri, R.; Chaudhury, K.; Goryacheva, I.Y.; Mishra, P.K. Ultrafine particulate matter impairs mitochondrial redox homeostasis and activates phosphatidylinositol 3-kinase mediated DNA damage responses in lymphocytes. Environ. Pollut. 2018, 234, 406–419. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Saffari, A.; Sioutas, C.; Forman, H.J.; Morgan, T.E.; Finch, C.E. Nano-scale particulate matter from urban traffic rapidly induces oxidative stress and inflammation in olfactory epithelium with concomitant effects on brain. Environ. Health Perspect. 2016, 124, 1537–1546. [Google Scholar] [CrossRef] [PubMed]
- Tyler, C.R.; Zychoowski, K.E.; Snchez, B.N.; Rivero, V.; Lucas, S.; Herbert, G.; Liu, J.; Irshad, H.; McDonald, J.D.; Bleske, B.E. Surface area-dependence of gas-particle interactions influences pulmonary and neuroinflammatory outcomes. Part. Fibre Toxicol. 2016, 13, 64. [Google Scholar] [CrossRef]
- Zhang, H.; Liu, H.; Davies, K.J.A.; Siutas, C.; Finch, C.E.; Morgan, T.E.; Forman, H.J. Nrf2-regulated phase II enzymes are induced by chronic ambient nanoparticle exposure in young mice with age-related impairments. Free Radic. Biol. Med. 2012, 52, 2038–2046. [Google Scholar] [CrossRef]
- Seagrave, J.; Campen, M.J.; McDonald, J.D.; Mauderly, J.L.; Rohr, A.C. Oxidative stress, inflammation, and pulmonary function assessment in rats exposed to laboratory-generated pollutant mixtures. J. Toxicol. Environ. Health 2008, 71, 1352–1362. [Google Scholar] [CrossRef]
- Weissenberg, A.; Sydlik, U.; Peuschel, H.; Schroeder, P.; Schneider, M.; Schins, R.P.F.; Abel, J.; Unfried, K. Reactive oxygen species as mediators of membrane-dependent signaling induced by ultrafine particles. Free Radic. Biol Med. 2010, 49, 597–605. [Google Scholar] [CrossRef]
- Morgan, T.E.; Davis, D.A.; Iwata, N.; Tanner, J.A.; Snyder, D.; Ning, Z.; Kam, W.; Hsu, Y.-T.; Winkler, J.W.; Chen, J.-C.; et al. Glutamatergic neurons in rodent models respond to nanoscale particulate urban air pollutants in vivo and in vitro. Environ. Health Perspect. 2011, 119, 1003–1009. [Google Scholar] [CrossRef]
- Kleinman, M.T.; Araujo, J.; Nel, A.; Siutas, C.; Campbell, A.; Cong, P.Q.; Li, H.; Bondy, S.C. Inhaled ultrafine particulate matter affects CNS inflammatory processes and may act via MAP kinase signaling pathways. Toxicol. Lett. 2008, 178, 127–130. [Google Scholar] [CrossRef]
- Allen, J.L.; Liu, X.; Weston, D.; Prince, L.; Oberdörster, G.; Finkelstein, J.N.; Johnston, C.J.; Cory-Slechta, D.A. Developmental exposure to concentrated ambient ultrafine particulate matter air pollution in mice results in persistent and sex-dependent behavioral neurotoxicity and glial activation. Toxicol. Sci. 2014, 140, 160–178. [Google Scholar] [CrossRef] [PubMed]
- Woodward, N.C.; Pakbin, P.; Saffari, A.; Shirmohammadi, F.; Haghani, A.; Sioutas, C.; CCacciottolo, M.; Morgan, T.E.; Caleb, E.F. Traffic-related air pollution impact on mouse brain accelerates myelin and neuritic aging changes with specificity for CA1 neurons. Neurobiol. Aging 2017, 53, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Klocke, C.; Allen, J.L.; Sobolewski, M.; Mayer-Pröschel, M.; Blum, J.L.; Lauterstein, D.; Zelikoff, J.T.; Cory-Slechta, D.A. Neuropathological Consequences of Gestational Exposure to Concentrated Ambient Fine and Ultrafine Particles in the Mouse. Toxicol. Sci. 2017, 156, 492–508. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.L.; Conrad, K.; Oberdörster, G.; Johnston, C.J.; Sleezer, B.; Cory-Slechta, D.A. Developmental exposure to concentrated ambient particles and preference for immediate reward in mice. Environ. Health Perspect. 2013, 121, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Davis, D.A.; Bortolato, M.; Godar, S.C.; Sander, T.K.; Iwata, N.; Pakbin, P.; Shih, J.C.; Berhane, K.; McConnell, R.; Siutas, C.; et al. Prenatal exposure to urban air nanoparticles in mice causes altered neuronal differentiation and depression-like responses. PLoS ONE 2013, 8, e64128. [Google Scholar] [CrossRef] [PubMed]
- Fonken, L.K.; Xu, X.; Weil, Z.M.; Chen, G.; Sun, Q.; Rajagopalan, S.; Nelson, R.J. Air pollution impairs cognition, provokes depressive-like behaviors and alters hippocampal cytokine expression and morphology. Mol. Psychiatry 2011, 16, 973, 987–995. [Google Scholar] [CrossRef]
- Suzuki, T.; Oshio, S.; Iwata, M.; Saburi, H.; Odagiri, T.; Udagawa, T.; Sugawara, I.; Umezawa, M.; Takeda, K. In utero exposure to a low concentration of diesel exhaust affects spontaneous locomotor activity and monoaminergic system in male mice. Part. Fibre Toxicol. 2010, 7. [Google Scholar] [CrossRef]
- Li, N.; Harkema, J.R.; Lewandowski, R.P.; Wang, M.; Bramble, L.A.; Gookin, G.R.; Ning, Z.; Kleinman, M.T.; Sioutas, C.; Nel, A.E. Ambient ultrafine particles provide a strong adjuvant effect in the secondary immune response: Implication for traffic-related asthma flares. Am. J. Physiol. Lung Cell Mol. Physiol. 2010, 299, 374–383. [Google Scholar] [CrossRef]
- Kleinman, M.; Hamade, A.; Meacher, D.; Oldham, M.; Sioutas, C.; Chakrabarti, B.; Stram, D.; Froines, J.R.; Cho, A.K. Inhalation of concentrated ambient particulate matter near a heavily trafficked road stimulates antigen-induced airway responses in mice. J. Air Waste Manag. Assoc. 2005, 55, 1277–1288. [Google Scholar] [CrossRef][Green Version]
- Saleh, Y.; Antherieu, S.; Dusautoir, R.; Alleman, L.Y.; Sotty, J.; De Sousa, C.; Platel, A.; Perdrix, E.; Riffault, V.; Fronval, I.; et al. Exposure to Atmospheric Ultrafine Particles Induces Severe Lung Inflammatory Response and Tissue Remodeling in Mice. Int. J. Environ. Res. Public Health 2019, 16, 1210. [Google Scholar] [CrossRef]
- Li, C.; Li, X.; Jigami, J.; Hasegawa, C.; Suzuki, A.K.; Zhang, Y.; Fujitani, Y.; Nagaoka, K.; Watanabe, G.; Taya, K. Effect of nanoparticle-rich diesel exhaust on testosterone biosynthesis in adult male mice. Inhal. Toxicol. 2012, 24, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Laurent, O.; Hu, J.; Li, L.; Cockburn, M.; Escobedo, L.; Kleeman, M.J.; Wu, J. Sources and contents of air pollution affecting term low birth weight in Los Angeles County, California, 2001–2008. Environ. Res. 2014, 134, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Laurent, O.; Hu, J.; Li, L.; Kleeman, M.J.; Bartell, S.M.; Cockburn, M.; Ecsobedo, L.; Wu, J. A statewide nested case-control study of preterm birth and air pollution by source and composition: California, 2001–2008. Environ. Health Perspect. 2016, 124, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.C.; Cole, T.B.; Costa, L.G. Prenatal and early-life diesel exhaust exposure causes autism-like behavioral changes in mice. Part. Fibre Toxicol. 2018, 15, 18. [Google Scholar] [CrossRef]
- Bourdon, M.; Torres-Rovira, L.; Monniaux, D.; Faure, C.; Levy, R.; Tarrade, A.; Rousseau-Ralliard, D.; Chavatte-Palmer, P.; Jolivet, G. Impact of a gestational exposure to diesel exhaust on offspring gonadal development: Experimental study in the rabbit. J. Dev. Orig. Health Dis. 2018, 9, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Integrated Science Assessment (ISA) For Particulate Matter; Final Report; U.S. Environmental Protection Agency: Washington, DC, USA, December 2009. Available online: https://cfpub.epa.gov/ncea/risk/recordisplay.cfm?deid=216546 (accessed on 14 May 2020).
- Ohlwein, S.; Kappeler, R.; Kutlar Joss, M.; Künzli, N.; Hoffmann, B. Health effects of ultrafine particles: A systematic literature review update of epidemiological evidence. Int. J. Public Health 2019, 64, 547–559. [Google Scholar] [CrossRef]
- HEI Review Panel on Ultrafine Particles. Understanding the Health Effects of Ambient Ultrafine Particles. HEI Perspectives 3; Health Effects Institute: Boston, MA, USA, 2013; Available online: https://www.healtheffects.org/publication/understanding-health-effects-ambient-ultrafine-particles (accessed on 14 May 2020).
- Population by Age and Sex, Municipalities, Slovenia, Half-Yearly. The Statistical Office of the Republic of Slovenia (SURS). Available online: https://pxweb.stat.si/SiStatDb/pxweb/en/10_Dem_soc/10_Dem_soc__05_prebivalstvo__10_stevilo_preb__20_05C40_prebivalstvo_obcine/05C4002S.px/. (accessed on 15 May 2020).
- SOER. Air Pollution. Slovenian Environment Agency. Available online: https://www.arso.gov.si/en/soer/air_pollution.html (accessed on 15 May 2020).
- WHO. International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). Available online: https://icd.who.int/browse10/2010/en (accessed on 15 May 2020).
- UFIREG. Data Collection and Methods; Report; UFIREG: Dresden, Germany, 2014; Available online: http://www.umwelt.sachsen.de/umwelt/download/UFIREG_Handbook_2014_final.pdf (accessed on 15 May 2020).
- Slovenian Environment Agency. Available online: https://www.arso.gov.si (accessed on 14 November 2019).
- Epidemiološko Spremljanje Nalezljivih Bolezni (Epidemiological Surveillance of Communicable Diseases in Slovenia). Nacionalni Inštitut za Javno Zdravje (National Institute of Public Health of the Republic of Slovenia). Available online: https://www.nijz.si/sl/epidemiolosko-spremljanje-nalezljivih-bolezni-letna-in-cetrtletna-porocila (accessed on 15 May 2020).
- National Laboratory of Health, Environment and Food (Nacionalni Laboratorij za Zdravje, Okolje in Hrano). Zbirka Dve-Urnih Koncentracij Cvetnega Prahu (Two-Hour Collection of Pollen Concentrations). Available online: https://www.nlzoh.si (accessed on 1 August 2019).
- Morgenstern, H.; Thomas, D. Principles of study design in environmental epidemiology. Environ. Health Perspect. 1993, 101, 23–38. [Google Scholar]
- De Souza Tadano, Y.; Ugaya, C.M.L.; Franco, A.T. Methodology to assess air pollution impact on human health using the generalized linear model with Poisson Regression. In Air Pollution-Monitoring, Modelling and Health; Khare, M., Ed.; In Tech: Rijeka, Croatia, 2012. [Google Scholar]
- Lanzinger, S.; Schneider, A.; Breitner, S.; Stafoggia, M.; Erzen, I.; Dostal, M.; Pastorkova, A.; Bastian, S.; Cyrys, J.; Zscheppang, A.; et al. Ultrafine and Fine Particles and hospital admission in Central Europe. Results from the UFIREG study. Am. J. Respir. Crit Med. 2016, 194, 1233–1241. [Google Scholar] [CrossRef]
- Bai, L.; Chen, H.; Hatzopoulou, M.; Jerrett, M.; Kwong, J.C.; Burnett, R.T.; van Donkelaar, A.; Copes, R.; Martin, R.V.; Van Ryswyk, K.; et al. Exposure to Ambient Ultrafine Particles and Nitrogen Dioxide and Incident Hypertension and Diabetes. Epidemiology 2018, 29, 323–332. [Google Scholar] [CrossRef]
- Karottki, D.G.; Bekö, G.; Clausen, G.; Madsen, A.M.; Andersen, Z.J.; Massling, A.; Ketzel, M.; Ellermann, T.; Lund, R.; Sigsgaard, T.; et al. Cardiovascular and lung function in relation to outdoor and indoor exposure to fine and ultrafine particulate matter in middle-aged subjects. Environ. Int. 2014, 73, 372–381. [Google Scholar] [CrossRef]
- Li, Y.; Lane, K.J.; Corlin, L.; Patton, A.P.; Durant, J.L.; Thanikachalam, M.; Woodin, M.; Wang, M.; Brugge, D. Association of Long-Term Near-Highway Exposure to Ultrafine Particles with Cardiovascular Diseases, Diabetes and Hypertension. Int. J. Environ. Res. Public Health 2017, 14, 461. [Google Scholar] [CrossRef] [PubMed]
- Johansson, C.; Norman, M.; Gidhagen, L. Spatial & temporal variations of PM10 and particle number concentrations in urban air. Environ. Monit. Assess. 2007, 127, 477–487. [Google Scholar]
- Cyrys, J.; Pitz, M.; Heinrich, J.; Wichmann, H.-E.; Peters, A. Spatial and temporal variation of particle number concentration in Augsburg, Germany. Sci. Total Environ. 2008, 401, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Birmili, W.; Tomsche, L.; Sonntag, A.; Opelt, C.; Weinhold, K.; Nordmann, S.; Schmidt, W. Variability of aerosol particles in the urban atmosphere of Dresden (Germany): Effects of spatial scale and particle size. Meteorol. Z. 2013, 22, 195–211. [Google Scholar] [CrossRef]
- Weinmayr, G.; Hennig, F.; Fuks, K.; Nonnemacher, M.; Jacobs, H.; Möhlenkamp, S.; Erbel, R.; Jöckel, K.-H.; Hoffman, B.; Moebus, S. Long-term exposure to fine particulate matter and incidence of type 2 diabetes mellitus in a cohort study: Effects of total and traffic-specific air pollution. Environ. Health 2015, 14. [Google Scholar] [CrossRef] [PubMed]
- Strak, M.; Janssen, N.; Beelen, R.; Schmitz, O.; Vaartjes, I.; Karssenberg, D.; van den Brink, C.; Bots, M.L.; Dijst, M.; Brunekreef, B.; et al. Long-term exposure to particulate matter, NO2 and the oxidative potential of particulates and diabetes prevalence in a large national health survey. Environ. Int. 2017, 108, 228–236. [Google Scholar] [CrossRef]
- Sun, S.; Qiu, H.; Ho, K.-F.; Tian, L. Chemical components of respirable particulate matter associated with emergency hospital admissions for type 2 diabetes mellitus in Hong Kong. Environ. Int. 2016, 97, 93–99. [Google Scholar] [CrossRef]
- Zanobetti, A.; Franklin, M.; Koutrakis, P.; Schwartz, J. Fine particulate air pollution and its components in association with cause-specific emergency admissions. Environ. Health 2009, 8, 58. [Google Scholar] [CrossRef]
- Kukec, A.; Zaletel-Kragelj, L.; Bizjak, M.; Fink, R.; Jereb, G.; Košnik, M.; Poljšak, B.; Zadnik, V.; Farkaš-Lainščak, J. A Study of Linkage of Environmental and Health Data in Zasavje as a Model Study to Support the Development and Implementation of Cross-Sectoral Policies on the Environment and Health; Final Report; Chair of Public Health: Ljubljana, Slovenia, 2012. (In Slovene) [Google Scholar]
- Bhaskaran, K.; Gasparrini, A.; Shakoor, H.; Smeeth, L.; Armstrong, B. Time series regression studies in environmental epidemiology. Int. J. Epidemiol. 2013, 42, 1187–1195. [Google Scholar] [CrossRef]
- Šimac, N. Air Pollution by Ozone in Nova Gorica Region—Assessment of the Impact on Human Health; Specialistic Study Thesis; Regional Institute of Public Health: Nova Gorica, Slovenia, 2008. (In Slovene) [Google Scholar]
- Šimac, N.; Hladnik, M.; Zaletel-Kragelj, L. The impact of temperature on tropospheric ozone in the Nova Gorica region. Zdr. Var. 2011, 50, 121–130. [Google Scholar] [CrossRef][Green Version]
- Rems-Novak, M.M. Effects of air pollution with ozone on primary health care consultations for respiratory tract diseases in children in Koper Municipality. Master’s Thesis, University of Nova Gorica, Graduate School of Environmental Sciences, Nova Gorica, Slovenia, 2013. [Google Scholar]
- Kukec, A.; Eržen, I.; Farkaš, J.; Zaletel Kragelj, L. Impact of air pollution with PM10 on primary health care consultations for respiratory diseases in children in Zasavje, Slovenia: A time-trend study. Zdr. Var. 2014, 53, 55–68. [Google Scholar] [CrossRef]
- Paulin, S.; Nadrag, P.; Kelšin, N.; Truden-Dobrin, P.; Korošec, A.; Simončič, M.; Zaletel, M.; Zupanc, I.; Eržen, I.; Zaletal, J.; et al. Ožji Nabor Kazalnikov za Spremljanje Obvladovanja Sladkorne Bolezni v Sloveniji; Nacionalni Inštitut za Javno Zdravje: Ljubljana, Slovenia, 2019; Available online: https://www.nijz.si/ (accessed on 24 June 2020).
- IDF Diabetes Atlas. Ninth Edition. 2019. Available online: https://www.diabetesatlas.org (accessed on 25 June 2020).




{kind=link}
{kind=link}
{kind=link}
| n | Mean | SD | Min. | Q1 | Median | Q3 | Max. | |
|---|---|---|---|---|---|---|---|---|
| Daily number of consultations due to diabetes mellitus: all age groups, children, elderly | ||||||||
| All age groups | 1826 | 11.21 | 9.35 | 0.00 | 1.00 | 11.00 | 18.00 | 42.0 |
| Children | 1826 | 0.04 | 0.21 | 0.00 | 0.00 | 0.00 | 0.00 | 2.00 |
| Elderly | 1826 | 8.17 | 7.19 | 0.00 | 1.00 | 8.00 | 13.00 | 33.00 |
| Average 24-h number concentration of UFP (number/cm3) | ||||||||
| UFP0.01–0.02 | 1655 | 1230.53 | 478.28 | 16.50 | 915.30 | 1172.30 | 1482.50 | 4370.40 |
| UFP0.02–0.03 | 1655 | 1086.93 | 434.30 | 88.10 | 809.50 | 1031.30 | 1308.20 | 4769.40 |
| UFP0.03–0.05 | 1655 | 1517.34 | 605.96 | 247.50 | 1113.00 | 1420.30 | 1819.20 | 4446.20 |
| UFP0.05–0.07 | 1655 | 1039.73 | 467.17 | 198.10 | 732.200 | 932.40 | 1224.20 | 3446.70 |
| UFP0.07–0.10 | 1655 | 1070.34 | 578.18 | 181.20 | 696.400 | 924.30 | 1251.40 | 4207.90 |
| Average 24-h concentration of PM10 and PM2.5 (µg/m3) | ||||||||
| PM10 | 1765 | 25.46 | 16.62 | 2.00 | 15.00 | 20.00 | 30.00 | 126.00 |
| PM2.5 | 1742 | 20.67 | 15.25 | 3.00 | 11.00 | 16.00 | 24.00 | 114.00 |
| Average 24-h of temperature (°C) and relative humidity (%) | ||||||||
| Temperature | 1826 | 12.06 | 8.107 | −7.90 | 5.80 | 12.50 | 18.32 | 30.00 |
| Relative humidity | 1826 | 75.99 | 13.66 | 31.00 | 65.00 | 76.00 | 88.00 | 100.00 |
| Daily average pollen concentration (number of particles/m3) | ||||||||
| Pollen concentration | 1826 | 8.99 | 27.36 | 0.00 | 0.00 | 1.00 | 7.00 | 323.00 |
| Pollutants | Model 1 a | Model 2 b | ||||||
|---|---|---|---|---|---|---|---|---|
| IRR | 95% CI | p | IRR | 95% CI | p | |||
| UFP0.01–0.02_lag0 | 1.001 | 1.000 | 1.003 | <0.001 | 1.001 | 1.000 | 1.003 | <0.001 |
| UFP0.02–0.03_lag0 | 1.001 | 1.000 | 1.003 | <0.001 | 1.001 | 1.000 | 1.003 | <0.001 |
| UFP0.03–0.05_lag0 | 1.000 | 1.000 | 1.000 | <0.001 | 1.000 | 1.000 | 1.000 | 0.133 |
| UFP0.05–0.07_lag0 | 1.000 | 1.000 | 1.000 | <0.001 | 1.000 | 1.000 | 1.000 | 0.590 |
| UFP0.07–0.10_lag0 | 1.000 | 1.000 | 1.000 | <0.001 | 1.000 | 1.000 | 1.000 | 0.689 |
| PM2.5_lag2 | 1.002 | 1.002 | 1.003 | <0.001 | 1.001 | 1.000 | 1.002 | 0.130 |
| PM10_lag0 | 1.002 | 1.001 | 1.003 | <0.001 | 1.001 | 1.000 | 1.002 | 0.606 |
| Pollutants | Model 1 a | Model 2 b | ||||||
|---|---|---|---|---|---|---|---|---|
| IRR | 95% CI | p | IRR | 95% CI | p | |||
| UFP0.01–0.02_lag0 | 1.000 | 1.000 | 1.001 | 0.164 | 1.000 | 1.000 | 1.001 | 0.663 |
| UFP0.02–0.03_lag0 | 1.000 | 1.000 | 1.001 | 0.045 | 1.000 | 1.000 | 1.001 | 0.377 |
| UFP0.03–0.05_lag0 | 1.000 | 1.000 | 1.001 | 0.023 | 1.000 | 1.000 | 1.001 | 0.237 |
| UFP0.05–0.07_lag0 | 1.000 | 1.000 | 1.001 | 0.154 | 1.000 | 1.000 | 1.001 | 0.534 |
| UFP0.07–0.10_lag0 | 1.000 | 1.000 | 1.000 | 0.676 | 1.000 | 0.999 | 1.001 | 0.873 |
| PM2.5_lag2 | 1.004 | 0.988 | 1.018 | 0.571 | 1.004 | 0.985 | 1.021 | 0.668 |
| PM10_lag0 | 1.000 | 0.985 | 1.013 | 0.996 | 0.997 | 0.978 | 1.013 | 0.699 |
| Pollutants | Model 1 a | Model 2 b | ||||||
|---|---|---|---|---|---|---|---|---|
| IRR | 95% CI | p | IRR | 95% CI | p | |||
| UFP0.01–0.02_lag0 | 1.001 | 1.000 | 1.003 | <0.001 | 1.001 | 1.000 | 1.003 | <0.001 |
| UFP0.02–0.03_lag0 | 1.001 | 1.000 | 1.003 | <0.001 | 1.001 | 1.000 | 1.003 | <0.001 |
| UFP0.03–0.05_lag0 | 1.000 | 1.000 | 1.000 | <0.001 | 1.000 | 1.000 | 1.000 | 0.065 |
| UFP0.05–0.07_lag0 | 1.000 | 1.000 | 1.000 | <0.001 | 1.000 | 1.000 | 1.000 | 0.419 |
| UFP0.07–0.10_lag0 | 1.000 | 1.000 | 1.000 | <0.001 | 1.000 | 1.000 | 1.000 | 0.560 |
| PM2.5_lag2 | 1.003 | 1.002 | 1.004 | <0.001 | 1.001 | 1.000 | 1.003 | 0.057 |
| PM10_lag0 | 1.002 | 1.001 | 1.003 | <0.001 | 1.000 | 0.999 | 1.001 | 0.795 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viher Hrženjak, V.; Kukec, A.; Eržen, I.; Stanimirović, D. Effects of Ultrafine Particles in Ambient Air on Primary Health Care Consultations for Diabetes in Children and Elderly Population in Ljubljana, Slovenia: A 5-Year Time-Trend Study. Int. J. Environ. Res. Public Health 2020, 17, 4970. https://doi.org/10.3390/ijerph17144970
Viher Hrženjak V, Kukec A, Eržen I, Stanimirović D. Effects of Ultrafine Particles in Ambient Air on Primary Health Care Consultations for Diabetes in Children and Elderly Population in Ljubljana, Slovenia: A 5-Year Time-Trend Study. International Journal of Environmental Research and Public Health. 2020; 17(14):4970. https://doi.org/10.3390/ijerph17144970
Chicago/Turabian StyleViher Hrženjak, Vesna, Andreja Kukec, Ivan Eržen, and Dalibor Stanimirović. 2020. "Effects of Ultrafine Particles in Ambient Air on Primary Health Care Consultations for Diabetes in Children and Elderly Population in Ljubljana, Slovenia: A 5-Year Time-Trend Study" International Journal of Environmental Research and Public Health 17, no. 14: 4970. https://doi.org/10.3390/ijerph17144970
APA StyleViher Hrženjak, V., Kukec, A., Eržen, I., & Stanimirović, D. (2020). Effects of Ultrafine Particles in Ambient Air on Primary Health Care Consultations for Diabetes in Children and Elderly Population in Ljubljana, Slovenia: A 5-Year Time-Trend Study. International Journal of Environmental Research and Public Health, 17(14), 4970. https://doi.org/10.3390/ijerph17144970