Public Health Academic Alliance for COVID-19 Response: The Role of a National Medical Task Force in Puerto Rico

 ,
,  ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. MTF Development and Composition
2.2. MTF Organization and Development of Protocols and Recommendations
2.3. Measures of Impact and Projections
2.4. Statistical Methods
2.5. Healthcare Utilization Estimation Analysis
3. Results
3.1. To Provide Clinical Guidelines on the Appropriate Medical Management of Critically Ill and Non-Critically Ill Patients
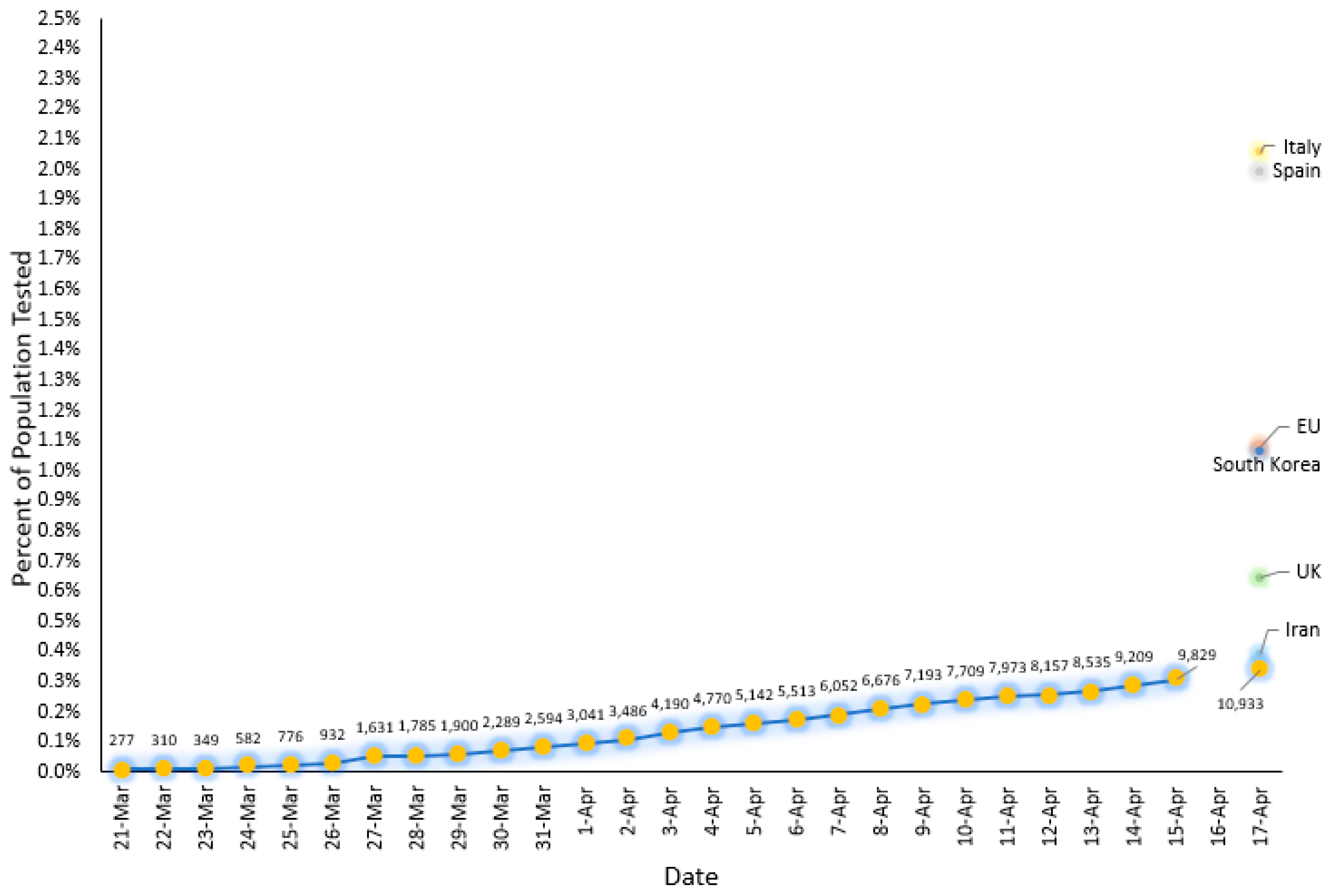
3.2. To Reduce the Transmission of the Virus by Doing Rapid Detection of Cases That Would Prevent Deaths
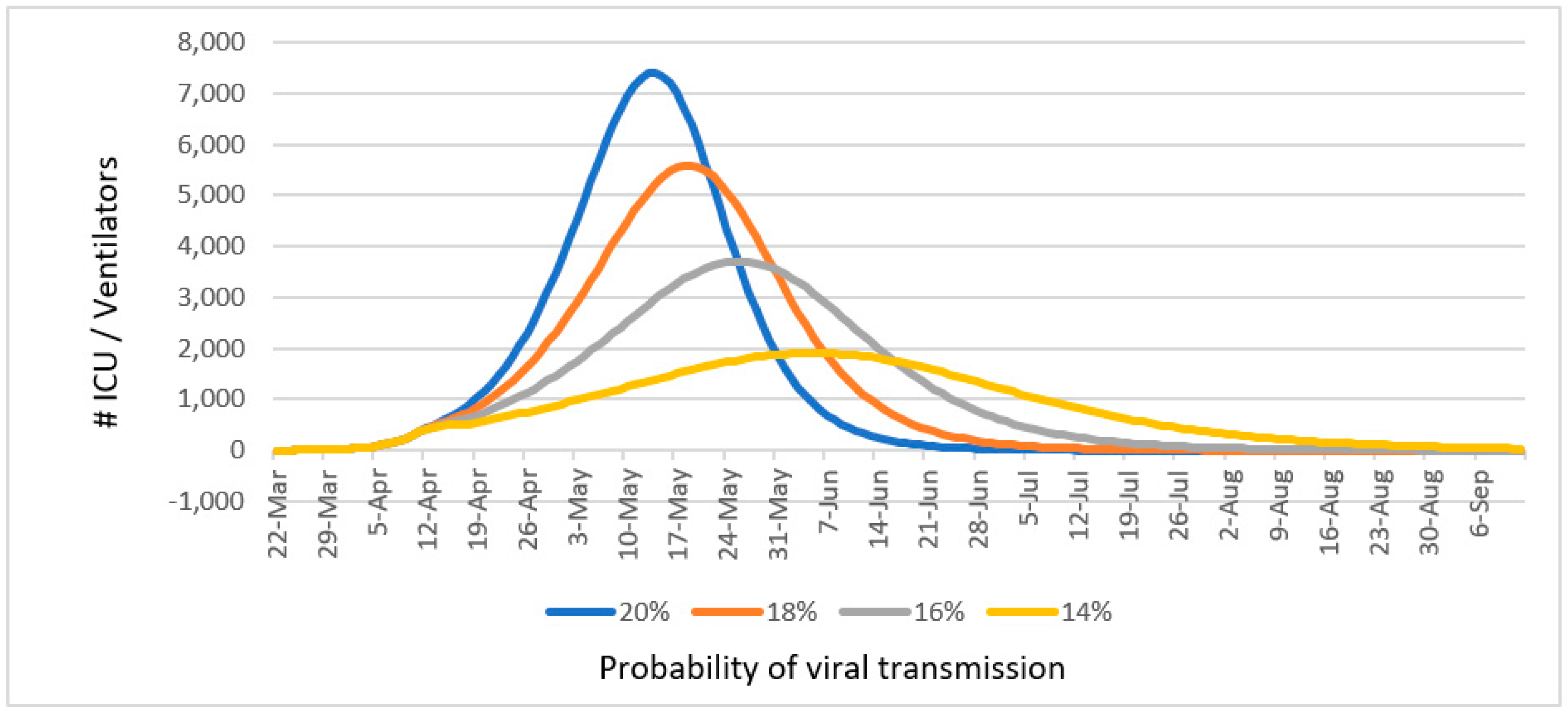
3.3. To Minimize the Impact the Epidemic Could Have on the Health System, Social Services, and the Community
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hedges, J.R.; Soliman, K.F.A.; D’Amour, G.; Liang, D.; Rodríguez-Díaz, C.E.; Thompson, K.; Romaguera, J.; Rabionet Sabater, S.E.; Yanagihara, R. Academic Response to Storm-Related Natural Disasters-Lessons Learned. Int. J. Environ. Res. Public Health 2018, 15, 1768. [Google Scholar] [CrossRef] [PubMed]
- Santos-Burgoa, C.; Sandberg, J.; Suárez, E.; Goldman-Hawes, A.; Zeger, S.; Garcia-Meza, A.; Pérez, C.M.; Estrada-Merly, N.; Colón-Ramos, U.; Nazario, C.M.; et al. Differential and persistent risk of excess mortality from Hurricane Maria in Puerto Rico: A time-series analysis. Lancet Planet. Health 2018, 2, 478–488. [Google Scholar] [CrossRef]
- Irvin-Barnwell, E.A.; Cruz, M.; Maniglier-Poulet, C.; Cabrera, J.; Rivera Diaz, J.; De La Cruz Perez, R.; Forrester, C.; Shumate, A.; Mutter, J.; Graziano, L.; et al. Evaluating Disaster Damages and Operational Status of Health-Care Facilities During the Emergency Response Phase of Hurricane Maria in Puerto Rico. Disaster Med. Public Health Prep. 2020, 14, 80–88. [Google Scholar] [CrossRef] [PubMed]
- WHO Critical Preparedness, Readiness and Response Actions for COVID-19: Interim Guidance—March 19, 2020. Available online: https://www.who.int/publications-detail/critical-preparedness-readiness-and-response-actions-for-covid-19 (accessed on 20 March 2020).
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Coupland, H.; Mellan, T.A.; Zhu, H.; Berah, T.; Eaton, J.W.; Guzman, P.N.P.; et al. Estimating the Number of Infections and the Impact of Non-Pharmaceutical Interventions on COVID-19 in 11 European Countries—Imperial College London, 30 March 2020. Available online: https://www.imperial.ac.uk/media/imperial-college/medicine/mrc-gida/2020-03-30-COVID19-Report-13.pdf (accessed on 15 May 2020).
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannerburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Jia, P.; Yu, C.; Remais, J.V.; Stein, A.; Liu, Y.; Brownson, R.C.; Lakerveld, J.; Wu, T.; Yang, L.; Smith, M.; et al. Spatial Lifecourse Epidemiology Reporting Standards (ISLE-ReSt) Statement. Health Place 2020, 61, 102243. [Google Scholar] [CrossRef] [PubMed]
- Drapper, N.R.; Smith, H. Applied Regression Analysis, 3rd ed.; John Wiley & Sons, Inc.: New York, NY, USA, 1998. [Google Scholar]
- Benzekry, S.; Lamont, C.; Beheshti, A.; Tracz, A.; Ebos, J.M.L.; Hlatky, L.; Hahnfeldt, P. Classical Mathematical Models for Description and Prediction of Experimental Tumor Growth. PLoS Comput. Biol. 2014, 10, e1003800. [Google Scholar] [CrossRef] [PubMed]
- Walker, P.G.T.; Whittaker, C.; Watson, O.; Baguelin, M.; Ainslie, K.E.C.; Bhatia, S.; Bhatt, S.; Boonyasiri, A.; Boyd, O.; Cattarino, L.; et al. The Global Impact of COVID-19 and Strategies for Mitigation and Suppression. Imperial College London—26 March 2020. Available online: https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-Global-Impact-26-03-2020v2.pdf (accessed on 16 May 2020).
- Fraser, C. Estimating Individual and Household Reproduction Numbers in an Emerging Epidemic. PLoS ONE 2007, 2, e758. [Google Scholar] [CrossRef] [PubMed]
- CDC COVID Data Tracker. United States COVID-19 Cases and Deaths by State. Available online: https://www.cdc.gov/covid-data-tracker/#cases (accessed on 23 June 2020).
- DATA USA. Available online: https://datausa.io/profile/geo/puerto-rico/ (accessed on 23 June 2020).
- State of West Virginia Executive Order No. 9-20. Available online: https://coronavirus-wvgovstatus-cdn.azureedge.net/STAY_AT_HOME_ORDER.pdf (accessed on 23 June 2020).
- Hassell, J.; Mathieu, E.; Beltekian, D.; Macdonald, B.; Giattino, C.; Ortiz-Ospina, E.; Ritchie, H.; Roser, M. Statistics and Research—Coronavirus (COVID-19) Testing. Available online: https://ourworldindata.org/covid-testing (accessed on 16 May 2020).
- Worldometer COVID-19 Data. Worldometers.info. Available online: https://www.worldometers.info/coronavirus/country/us/ (accessed on 25 June 2020).
- Intensive Care National Audit & Research Council (ICNARC). ICNARC Report on COVID-19 in Critical Care, 4 April 2020. Available online: https://www.icnarc.org/About/Latest-News/2020/04/04/Report-On-2249-Patients-Critically-Ill-With-Covid-19 (accessed on 4 April 2020).
- World Health Organization. Advice on the Use of Masks in the Context of COVID-19: Interim Guidance, 6 April 2020. Available online: https://apps.who.int/iris/handle/10665/331693 (accessed on 25 June 2020).
- CDC. Recommendation Regarding the Use of Cloth Face Coverings, Especially in Areas of Significant Community-Based Transmission, 3 April 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/cloth-face-cover (accessed on 25 June 2020).
- Zhang, R.; Li, Y.; Zhang, A.L.; Wang, Y.; Molina, M.J. Identifying Airborne Transmission as the Dominant Route for the Spread of COVID-19. Proc. Natl. Acad. Sci. USA 2020. [Google Scholar] [CrossRef] [PubMed]
- López, L.; Rodó, X. The end of social confinement and COVID-19 re-emergence risk. Nat. Hum. Behav. 2020. [Google Scholar] [CrossRef] [PubMed]
- Saddiqui, S. American College of Surgery’s COVID-19: Guidance for Triage of Non-Emergent Surgical Procedures. Available online: https://www.facs.org/covid-19/clinical-guidance/triage (accessed on 28 May 2020).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Committee | Protocols and Recommendations | Implementation Agencies |
|---|---|---|
| Emergency Response |
|
|
| Hospital Response and Management |
|
|
| Laboratory Tests for COVID-19 |
|
|
| Contact Tracing |
|
|
| Surveillance |
|
|
| Risk Communication and Community Engagement |
|
|
| Infection Prevention and Control |
|
|
| Societal Response |
|
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cruz-Correa, M.; Díaz-Toro, E.C.; Falcón, J.L.; García-Rivera, E.J.; Guiot, H.M.; Maldonado-Dávila, W.T.; Martínez, K.G.; Méndez-Latalladi, W.; Pérez, C.M.; Quiñones-Feliciano, M.L.; et al. Public Health Academic Alliance for COVID-19 Response: The Role of a National Medical Task Force in Puerto Rico. Int. J. Environ. Res. Public Health 2020, 17, 4839. https://doi.org/10.3390/ijerph17134839
Cruz-Correa M, Díaz-Toro EC, Falcón JL, García-Rivera EJ, Guiot HM, Maldonado-Dávila WT, Martínez KG, Méndez-Latalladi W, Pérez CM, Quiñones-Feliciano ML, et al. Public Health Academic Alliance for COVID-19 Response: The Role of a National Medical Task Force in Puerto Rico. International Journal of Environmental Research and Public Health. 2020; 17(13):4839. https://doi.org/10.3390/ijerph17134839
Chicago/Turabian StyleCruz-Correa, Marcia, Elba C. Díaz-Toro, Jorge L. Falcón, Enid J. García-Rivera, Humberto M. Guiot, Wanda T. Maldonado-Dávila, Karen G. Martínez, William Méndez-Latalladi, Cynthia M. Pérez, Myrna L. Quiñones-Feliciano, and et al. 2020. "Public Health Academic Alliance for COVID-19 Response: The Role of a National Medical Task Force in Puerto Rico" International Journal of Environmental Research and Public Health 17, no. 13: 4839. https://doi.org/10.3390/ijerph17134839
APA StyleCruz-Correa, M., Díaz-Toro, E. C., Falcón, J. L., García-Rivera, E. J., Guiot, H. M., Maldonado-Dávila, W. T., Martínez, K. G., Méndez-Latalladi, W., Pérez, C. M., Quiñones-Feliciano, M. L., Reyes, J. C., Rodríguez, P., Santana-Bagur, J., Torrellas, L. C., Vázquez, D., Vázquez, G. J., & Rodríguez-Quilichini, S. (2020). Public Health Academic Alliance for COVID-19 Response: The Role of a National Medical Task Force in Puerto Rico. International Journal of Environmental Research and Public Health, 17(13), 4839. https://doi.org/10.3390/ijerph17134839