Abstract
Household expenditure surveys, routinely conducted in low—and middle-income countries (LMICs), usually include questions pertaining to recent household expenditures on key food groups. When child anthropometrics are also available, such expenditure data can provide insights into household food purchasing patterns that are associated with subsequent child growth measures. We used data from 6993 children, born around 2001, from Ethiopia, India, Peru, and Vietnam, from the Young Lives younger cohort. We compared associations between two weeks of household food expenditures (in PPP—Purchasing Power Parity adjusted dollars) on food groups and child height-for-age-Z score (HAZ) at subsequent time points to assess longitudinal associations. Total food expenditures, rural/urban residence, maternal and paternal schooling, and child sex were included in our adjusted models because they may affect the relations between household food group expenditures and future child HAZ. In Ethiopia, India, and Peru every extra PPP$ spent on fats was associated with 0.02–0.07 higher future HAZ. In Vietnam every extra PPP$ spent on starches, was significantly associated with a 0.01 lower future HAZ. Across countries, different patterns of food expenditure and procurement may be differentially critical for predicting child HAZ. Our results demonstrate how expenditures on specific food groups can be associated with children’s linear growth. This study provides additional evidence of the utility of longitudinal household food expenditure data in understanding child nutritional status.
1. Introduction
According to UNICEF estimates from 2019, approximately 144 million children under the age of 5 years were stunted [1]. Poor childhood nutritional status has been associated with cognitive deficits, impaired growth, lower lifetime educational achievements and earnings, and lower birth weights in the next generation [2]. While child undernutrition is a complex and multifactorial problem, inadequate food intake is considered one of two immediate major causes of child undernutrition [3,4]. Unfortunately, information on actual food consumption is often lacking, making it difficult to identify which aspects of food intake are most closely associated with better future child nutritional status. However, household choices about allocation of the household budget on food in general, and particular food groups, may be an additional source of information about child food intake [5].
Current analytic methods used to examine the effects of diet on child nutritional status at a population-level face limitations in dietary intake data [6,7]. The “gold standard” for measuring current food consumption are observed-weighed food records (OWFR) and 24-hour recall (24 h) surveys [6]. These methods require careful training of interviewers, rigorous technical and managerial support, and may be unrealistic at the population-level in low- and middle-income countries (LMICs) [6]. Historically, the principle data source for assessing population-level food consumption and undernutrition has been the Food and Agriculture Organization’s (FAO) Food Balance Sheets (FBS). However, these data are limited to average individual consumption at the national level and provide no information on how food is distributed regionally, locally or within households [8]. Nor do they provide longitudinal data on child nutritional status.
Another data source addressing food is available to researchers, as governments in over 125 LMICs conduct regular (generally every 3–5 years) household consumption and expenditure surveys (HCES). These surveys include information on household expenditures on key food groups [7]. HCES have been validated against traditional gold-standard nutrition methods and were found to provide useful information on patterns of food access [9,10,11]. In addition, researchers note these surveys may be a good proxy for 24 h dietary measures in LMICs [10,12]. A subset of these data sets includes longitudinal information on child anthropometry. This subset may help identify patterns of food expenditure that are associated with children’s linear growth [5].
This study fills a gap in the existing literature about how different food group expenditures relate to children’s subsequent nutritional status. We hypothesize that household food expenditures on the seven key dietary diversity food groups—starches, fruits and vegetables, legumes, eggs, dairy, meat, and fat—will have differential associations with future child HAZ, after adjusting for child, parental, household, and community characteristics that we hypothesize may modify the relations between food group expenditures and child HAZ. Specifically, we investigate the associations of household food group expenditures at 5 and 8 years with child HAZ at 8 and 12 years, respectively.
2. Materials and Methods
Figure 1 represents the conceptual framework guiding this research. We posit that household food expenditures across food groups predict subsequent child height-for-age Z-scores (HAZ), low values of which (<−2 relative to international medians for well-nourished populations) are a measure of stunting (chronic undernutrition). We capitalize on three survey rounds of Young Lives’ younger-cohort longitudinal data to understand how household food group expenditures at earlier ages predict children’s HAZ subsequently, adjusting for other factors such as child sex, and household, parental, and community characteristics that might influence the relations between household food group expenditures and subsequent child HAZ.
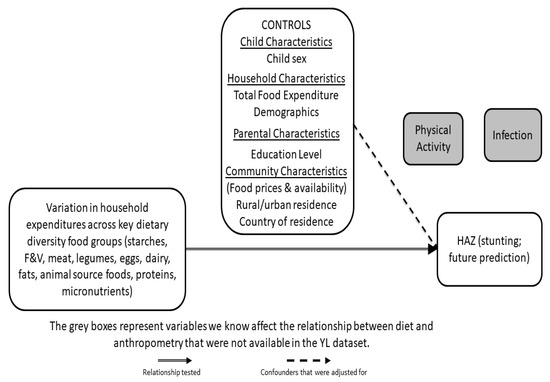
Figure 1.
Conceptual Framework: This figure highlights the relationship between child height (height-for-age Z score (HAZ) far right) and previous household expenditures on specific dietary food groups (far left), while controlling for key child, household and community characteristics (upper box). YL = Young Lives.
2.1. Study Design and Participants
This study used data from the Young Lives (YL) younger cohort, a study of approximately 8000 children in Ethiopia, India, Peru, and Vietnam. In 2002, 2000 children were enrolled from each of the four countries and followed up in three more rounds when children were 5 years, 8 years and 12 years. The YL team used multistage sampling designs with the first stage consisting of a selection of 20 sentinel sites. Sampling was pro-poor. For example, in Ethiopia, the most food-insecure districts were oversampled as part of the study design. In Peru, the richest 5% of districts were excluded from the sample. While poor clusters were moderately oversampled, the final samples were diverse samples of social, geographic, and demographic groups. The sample in India consisted only of households from Andhra Pradesh (since split into Andhra Pradesh and Telangana), whereas the three other countries used nationwide samples. Sampling methods have been previously reported [2,5]. Additional study details are described elsewhere [13,14]. From age 1 year to age 12 years, the YL country cohorts lost between 1.5% and 5.7% of participants to attrition (Ethiopia 114/1999; India 81/2011; Peru 106/2052; Vietnam 36/2000). Household food expenditure data were collected starting with round 2. Consequently, this study included data from rounds 2–4, which were the only rounds available at the time this analysis was undertaken.
2.2. Study Indicators
2.2.1. Household Food Expenditures
The respondent (usually the mother) was asked to report on consumption of food categories in the previous two weeks, ranging from 20 in Ethiopia, India and Vietnam, to 35 in Peru. For each food group, the respondent was asked to estimate the total monetary value of all foods in each of the food groups. To do this they were asked details of (a) expenditure on all individual foods in that food group consumed in the previous two weeks; (b) value of gifts received or food paid in lieu of wages in that food group; and (c) value of own stores used in that food group (which included foods from the household’s own production, shop or stocks). As previously reported [5], these food group expenditures were then aggregated to align with the seven food groups ((1) starches—bread, cereal, rice, grains and starchy vegetables; (2) fruits and vegetables; (3) legumes; (4) eggs; (5) dairy; (6) meat and fats; and (7) oils and oil seeds) in the WHO child dietary diversity measure [15]. At age 8 years, vitamin A-rich fruits and vegetables were recorded as separate categories as in the adult version of dietary diversity instrument [16,17]. Expenditures were adjusted to 2006 local currency and adjusted again to facilitate international comparability using purchasing power parity conversions (PPP) [5]. We summed total food expenditures across food groups and divided by the number of adult equivalents in the household to give total food expenditure per adult equivalent [18]. We winsorized expenditures in each food group to address outliers [19] for each of the four countries, replacing values below the 1st percentile with the 1st percentile, and replacing values above the 99th percentile with the 99th percentile. Expenditures for proteins, micronutrients, and animal source foods (ASF) were created by summing the appropriate categories to convey total expenditure on foods that contribute to those three food groupings. To create the protein expenditure variable, expenditures on legumes, meat, eggs, and dairy were summed. To create the micronutrient expenditure variable, expenditures on fruits and vegetables, legumes, meat and fish, eggs, and dairy were summed. To create the fat expenditure variable, expenditures on fats were summed. Finally, to create the ASF expenditure variable, expenditures on meat, eggs, and dairy were summed.
2.2.2. Child Anthropometry
Field workers measured height using locally-made stadiometers with standing plates and moveable head boards accurate to 1 mm. Height-for-age Z-score (HAZ) was calculated using WHO 2006 standards for children 0–59 months [20] and WHO 2007 standards for older children [21]. Birth dates were recorded from children’s health cards when available, and from mothers’ reports otherwise. Our analyses focused on HAZ as the main indicator of chronic undernutrition in children. Children are classified as stunted if they have HAZ that are less than −2.0 [20,22].
2.2.3. Control Variables
Other measures used to examine how certain characteristics might affect the relations between household food group expenditures and future child HAZ included children’s sex, rural/urban residence, total household food expenditures, and maternal and paternal schooling. Maternal and paternal schooling were coded as categorical variables for no schooling, 1–6 grades, 7–11 grades, and 12 or more grades of schooling.
2.2.4. Country-Level Per-Capita Available Calories Data
These data were downloaded from Food Balance Sheets available on the Food and Agriculture Organization Corporate Statistical Database website [23]. Food supply (in kcal/capita/day) as well as protein and fat supply (in g/capita/day) were retrieved for each of the four study countries for each of the three study years. Food, protein, and fat supplies were also broken out by source: either animal or vegetable products. These data were used to assess the heterogeneity in country-level food availability.
2.3. Statistical Methods
We used SAS software (Version 9.4. Copyright 2012, SAS Institute Inc., Cary, NC, USA) for all analyses. Results were considered statistically significant for p-values < 0.05. Statistical differences in food group expenditures by country, round, and rural/urban residence were assessed using the Wilcoxon Rank Sum test, and medians and interquartile ranges were reported to highlight the differences in expenditure patterns. Means and 95% confidence intervals (for continuous variables) and frequencies and percentages (for categorical variables) were reported by country and round for all other key study indicators. We present associations between household food group expenditures and child HAZ using single and multivariable ordinary least squares regressions, controlling for total food expenditures, rural/urban residence, maternal and paternal schooling, and sex of child. Our models assessed how expenditures at 5 years predict HAZ 8 years, and also how expenditures at 8 years predict HAZ at 12 years.
2.4. Ethical Review
The secondary analysis of de-identified public use data in this study was identified as exempt by the University of Pennsylvania Institutional Review Board under protocol number #814690.
3. Results
3.1. Country-Level Food Energy and Macronutrient Availability
Heterogeneity in the country-level food energy and macronutrient availability context is important to take into consideration as a backdrop to the additional country-level information and comparisons provided in this study. Based on FAOSTAT country-level food balance sheets, caloric availability varies across the four countries and rounds, with Ethiopia consistently showing the lowest overall energy intake and Vietnam consistently showing the highest (Figure 2). In addition, Vietnam has the highest consumption of animal products, and Ethiopia has the lowest.

Figure 2.
We present here the per capita availability of energy (kcal, left axis), protein and fat (grams, right axis) from animal and vegetable sources, in each of the four countries (Ethiopia, India, Peru, Vietnam) and each of the three years (2006, 2009, 2013) covered by this study. Per capita availability is taken from the food balance sheets of the Food and Agricultural Organization Statistical database [23].
3.2. Descriptive Characteristics
The child growth characteristics of these populations (Table 1) have been characterized extensively in previous publications and our analyses are consistent with previous reports [2,5,24]. Mean HAZ was negative in all countries in each round, and mean HAZ was less negative at 12 years than at 5 years in India (−1.65 to −1.44), Peru (−1.53 to −1.02) and Vietnam (−1.35 to −1.06), although it remained constant for Ethiopia (−1.48 to −1.47) (Table 1). The percentages of individuals who lived in rural areas in each country remained relatively constant in Ethiopia (59%, 60%), India (72–74%) and Vietnam (80%, 81%) across the three time periods included in the study. In contrast, Peru experienced greater rural to urban migration as demonstrated by a decrease from 44% rural residence in Round 2 to 27% in Round 4. The majority of mothers in Ethiopia (51%) and India (51%) reported no schooling. The proportion of mothers reporting completing 7–12 years of schooling was highest in Peru (42%) and Vietnam (47%). In Ethiopia, fathers were more likely to report schooling levels of 1–6 grades (46%), while in India (36%), Peru (49%), and Vietnam (53%), fathers were more likely to report schooling levels in the range of 7–12 grades (Table 1).

Table 1.
Descriptive Statistics of Key Study Variables by Country and Child Age at Time of Survey.
3.3. Differences by Rural/Urban Residence
3.3.1. Ethiopia
When assessing the differences in 15-day household expenditure on key food groups by rural and urban residence (Table 2), urban households had significantly higher expenditures on starches, fruits and vegetables, meat, legumes, eggs, and fats compared to rural household across all rounds, with the exception of expenditures on eggs at 8 years. Dairy expenditures across all rounds did not differ by rural/urban residence with mean expenditures of less than 0.005 PPP$ for both groups. In both urban and rural settings, households spent the greatest amount on starches ($7–10/15 days), with the median expenditure for every other food group except urban legumes less than $1.0/15 days.
Table 2.
Differences in 15-day household food expenditure (adjusted PPP) by age on key dietary diversity food groups by rural/urban status.
3.3.2. India
Urban households generally had significantly higher expenditures on fruits and vegetables, dairy, and fats per adult equivalent compared to rural households, with the only exception being expenditures on starches at 5 years, for which rural households spent a significantly greater amount (Table 2). Expenditures on meat were not statistically different between rural and urban households at age 5 years and 12 years, but data at 8 years showed significantly larger expenditures on meat by rural households. With regard to eggs, a significant difference in expenditure by rural/urban residence was detected at 5 years, with urban households having larger expenditures on eggs. Legumes were the only food group significantly associated with greater expenditure by rural households at each age. Starches had the greatest absolute expenditure in both urban and rural households ($5–7/15 days).
3.3.3. Peru
Relative to rural households, urban households tended to expend significantly more resources across all rounds on fruits and vegetables, meats, and dairy. (Table 2). Rural households had greater expenditures on starches, legumes, and fats compared to urban households, with the only exceptions being expenditures on starches and legumes at 5 years, which were not significantly different between rural and urban households. Differences in expenditures on eggs varied across all rounds. The greatest absolute expenditures in rural and urban households in Peru were on starches ($13–18/15 days), with meats having the second greatest expenditures ($5–11/15 days).
3.3.4. Vietnam
Urban residents had significantly larger expenditures than rural residents on fruits and vegetables, meat, legumes, eggs, dairy, and fats across all three rounds (with the exception of expenditures on legumes at 8 years, which were not significantly different by rural/urban status) (Table 2). Expenditures on starches at 5 years and 8 years were significantly greater for rural households, while at 12 years, rural households had significantly smaller expenditures. The greatest absolute expenditures by rural and urban households were on meat ($9–21/15 days), with starch expenditures having the second largest absolute expenditures ($8–12/15 days).
3.4. Unadjusted and Food Group-Only Models
3.4.1. Ethiopia
Each of the 10 food group expenditures (fruits and vegetables, legumes, meat, eggs, dairy, starches, fats, proteins, micronutrients, and ASF) at 5 years had a significant unadjusted association with HAZ at 8 years (Table 3a). The unadjusted fats model had the highest adjusted R2 value, and the unadjusted coefficient suggested every $1 increase expenditure on fats at 5 years was associated with a 0.15 increase in HAZ at 8 years. The models for protein, micronutrient, and ASF expenditures (models included expenditures on all food groups encompassed by the aggregate group), showed that after including other food groups that provide similar nutritional components, only expenditures on legumes and fruits and vegetables at 5 years were significantly positively associated with HAZ at 8 years. Of those with significant univariate associations, fats had the highest R2 value (0.0183), and the largest coefficient (0.16). The models for proteins, micronutrients, and ASF expenditures suggest that meats, rather than legumes were the primary driver of the associations between protein and HAZ at 12 years. Before and after adjusting for other food groups, every additional $1 spent on meat at 8 years was associated with a 0.04 increase in HAZ at 12 years. Fruits and vegetables continued to have a significant association with future HAZ after including other micronutrient-rich food groups, suggesting that every extra $1 spent on fruits and vegetables at 8 years was associated with a 0.12 increase in future HAZ.
Table 3.
Single and Multiple Food Group Models Relating Child HAZ to Previous Expenditures on Key Food Groups in (a) Ethiopia; (b) India; (c) Peru; and (d) Vietnam.
3.4.2. India
Meat, dairy, fats, proteins, micronutrients, and ASF expenditures at 5 years all had significant associations with HAZ at 8 years (Table 3b). Similar to Ethiopia, expenditures on fats had the largest association with future HAZ for every extra $1 spent (β: 0.11), but expenditures on dairy at 5 years were associated with the greatest variation in HAZ at 8 years (adj R2: 0.0405). After adjusting for protein, micronutrient, and ASF food group expenditures in three separate models, dairy and meat expenditure continued to be significantly associated with HAZ at 8 years. Every additional $1 spent on dairy was associated with a 0.10 increase in future HAZ, while every additional $1 spent on meat was associated with approximately a 0.02 increase. When looking at food group expenditures at 8 years, dairy and fats continued to be significantly associated with future HAZ and with relatively high coefficients (dairy: 0.10; fats: 0.14) and R2 values (dairy: 0.0473; fats: 0.0212). Even after including other food group expenditures in the proteins, micronutrient, and ASF models, dairy expenditures were still significantly associated with HAZ at 12 years.
3.4.3. Peru
Expenditures on all food groups at 5 years except for legumes, starches, and fats had significant associations with HAZ at 8 years (Table 3c). Of all the associations, expenditure on eggs had the largest coefficient (0.09), while total expenditures on dairy had the highest adjusted R2 value (0.0718). After including the other food groups in the three composite models, the association between egg expenditures at 5 years and future HAZ was not significant. Interestingly, in both the protein and micronutrient analyses, legume expenditure was associated with a 0.04 decrease in HAZ at 8 years for every extra $1 spent. Fruits and vegetables, meat, and dairy expenditures were still significantly associated with HAZ at 8 years (with the exception of meat expenditures in the micronutrient model, which was only marginally significant). Similar patterns were noted for the analyses assessing relationship of expenditures at 8 years to HAZ at 12 years.
3.4.4. Vietnam
All food group expenditures at both 5 years and 8 years were significantly associated with future HAZ except for expenditures on starches (Table 3d). When investigating individual food groups rather than the composite protein, micronutrient and ASF expenditures, expenditures on meat, dairy, and fruits and vegetables at 5 years remained significantly associated with HAZ, while at 8 years expenditures on meat, eggs, fruits and vegetables remained significantly associated with future HAZ. For expenditures at 5 years, we found that fats had the largest association with higher HAZ for every dollar spent (β = 0.19), but micronutrient expenditures were associated with the most variation in HAZ at 8 years (R2 = 0.097). This micronutrient pattern was also observed with expenditures at 8 years, but instead of fats, the food group with the greatest association with future HAZ per dollar spent was eggs.
3.5. Adjusted Models Investigating Association of Key Food Expenditures and Future HAZ
Following preliminary analyses reported in Table 2 and Table 3 individual food groups were chosen for detailed review due to the relatively large accompanying coefficients and/or significance of these models compared to other variables (see Figure 3a–d; models for other food groups can be found in Tables S1–S16). Expenditures on fats at 5 years and 8 years, and how they were associated with future HAZ after adjusting for other key covariates are discussed for Ethiopia (Table 4a), India (Table 4b), and Peru (Table 4c). In Vietnam (Table 4d), expenditures on starches at 5 years and 8 years are highlighted due to the relative significance of the final, adjusted association compared to other food groups (models for other food group expenditures in Vietnam can be found in Tables S12–S16.

Figure 3.
Unadjusted and adjusted coefficients for food groups in association with HAZ at next age of measurement for each country (a–d). We present here the unadjusted (blue) and adjusted (red) coefficients for each food group in bivariate and multivariate regression analyses with HAZ at the next age of measurement (i.e., 8 years HAZ and 5 years food group expenditures; 12 years HAZ and 8 years food group expenditures). * = p value < 0.05.
Table 4.
Models of Child HAZ Assessing influence of Past Household Fats Expenditures in (a) Ethiopia, (b) India, (c) Peru and Past Household Starches Expenditures in (d) Vietnam.
3.5.1. Ethiopia
Fat expenditures had the highest coefficient in univariate models at both 5 years and 8 years (Table 4a, Models 1a and 1b). However, in models that included individual, household and community covariates fat expenditures were no longer significantly associated with future HAZ. Additionally, none of the models for individual food groups that adjusted for covariates had a significant association between the analyzed food expenditure group and child HAZ score at either round (See Tables S1–S4). When Total Food Expenditures were included, the individual food group expenditures were no longer significantly associated with future child HAZ. Fat expenditures, while not significant after adjusting for sex, rural/urban residence, total food expenditures, and maternal and paternal schooling, retained the highest coefficients compared to other food groups (Tables S1–S4).
After adjusting for the five aforementioned covariates, every additional $1 spent on fats at 5 years was associated with a 0.03 increase in HAZ at 8 years and each additional $1 spent on fats at 8 years was associated with a 0.02 increase in HAZ at 12 years. Child sex, rural/urban residence, total food expenditure, maternal schooling (except for mothers with 12 or more grades of schooling), and paternal schooling at 5 years were significantly associated with HAZ at 8 years, and individual food group expenditures were not. Children living in rural areas at 5 years had HAZ at 8 years that were, on average, lower by 0.19 compared to children living in urban areas. Additionally, parental schooling (1–12 grades for mothers and 1–12 or more grades for fathers) was associated with a 0.14–0.26 higher child HAZ at 8 years compared to those whose parents had no schooling. At 8 years, the only covariates that were significantly associated with HAZ at 12 years were rural/urban residence, and maternal schooling (except for mothers with 12 or more grades of schooling).
3.5.2. India
Adjusted expenditures on fats at 5 years and 8 years were significantly associated with future HAZ (Table 4b). After adjusting for sex, rural/urban residence, total food expenditures, and maternal and paternal schooling, every additional $1 spent on fats at 5 years was associated with a 0.07 increase in HAZ at 8 years. Of the variables included in the adjusted model at 5 years (Table 4b, Model 2a), all were significantly associated with HAZ at 8 years except for total food expenditures and paternal schooling of 1–6 grades. This model had a relatively high adjusted R2, with 12.2% of variation in HAZ at 8 years predicted. Expenditures on fats at 8 years showed a similar relationship with HAZ at 12 years (Table 4b, Model 2b), with every additional $1 spent on fats at 8 years associated with a 0.06 increase in 12 years HAZ. In the adjusted model at 12 years, however, compared to the adjusted model at 8 years (Table 4b, Model 2a), sex and several levels of maternal schooling were no longer significantly associated with future HAZ.
3.5.3. Peru
Expenditures on fats were significantly associated with HAZ at 8 years (Table 4c). After adjusting for all control variables, every extra $1 spent on fats at age 5 years was associated with a 0.05 increase in HAZ at 8 years (Table 4c, Model 2a), while every extra $1 spent on fats at 8 years was associated with a 0.04 increase in child HAZ at 12 years (Table 4c, Model 2b). Paternal schooling was not significantly associated with future child HAZ after adjusting for all other variables in the model.
3.5.4. Vietnam
Starches were the only significant food group expenditure associated with future HAZ at both 5 years and 8 years (Table 4d). Greater expenditure on starches was negatively associated with future HAZ. At age 5 years and 8 years, every extra $1 spent on starches, was significantly associated with a 0.01 decrease in future HAZ after adjusting for covariates (Table 4d, Models 2a and 2b). All covariates in both of these adjusted models, except for sex, were significantly associated with future HAZ. Maternal schooling had the largest estimated coefficients. Most notably, Vietnamese children with mothers who had 12 or more years of schooling, on average, had future HAZ scores that were 0.92–0.96 higher compared to children with mothers who had no schooling. These models had some of the highest R2 values reported for any of the food group models across the four countries. The adjusted model of starch expenditures at 5 years was associated with approximately 20% of the variation in future HAZ and the adjusted model of starch expenditures at 8 years was associated with approximately 17.5% of the variation in future HAZ.
4. Discussion
We used data on 6.993 children born around 2001 from Ethiopia, India, Peru, and Vietnam collected at ages 5, 8, and 12 years from the Young Lives younger cohort to assess the longitudinal associations between expenditures on key food groups at 5 years and 8 years (including starches, fats, legumes, meat, fruits and vegetables, eggs, dairy, animal source food, proteins, and micronutrients) and child HAZ at ages 8 years and 12 years, respectively. While there was much heterogeneity among the countries in terms of food energy and macronutrient availability, several cross-country similarities emerged from our analysis. Across three of the four countries, household expenditures on fats were associated with the largest changes in future child HAZ before and after adjusting for children’s sex, rural/urban residence, total food expenditures, and parental schooling.
Expenditures on animal source foods, proteins, and micronutrient rich foods had very small associations with future HAZ. Increased expenditures on starches were associated with lower HAZ in both Vietnam and Peru in unadjusted and adjusted models. Of all the adjusted Vietnam models, the associations of HAZ with starches at 5 years and 8 years were the only ones that reached significance. The addition of total food expenditures to models with expenditures on specific food groups dramatically altered patterns of significance, particularly in Ethiopia. Parental schooling of 7–12 grades or more was an important predictor of higher HAZ across all of the countries, with the exception of paternal schooling in Ethiopia at 8 years and Peru at both 5 years and 8 years. Finally, urban residence was associated with higher HAZ in every country.
India showed variations in significance of unadjusted associations between food groups and future HAZ across study ages. After adjusting for children’s sex, rural/urban residence, total food expenditure, maternal schooling, and paternal schooling, expenditure on fats was the only food group in India significant across both ages, and also had the greatest magnitudes of associations compared to the other food groups. While a few studies have linked fat expenditures in India to higher stature, there are few studies demonstrating a link between fat consumption and child HAZ [24]. One study identified a co-movement of declining calorie, protein, and fat intake for both adults and children and a corresponding lack of progress in improving nutritional outcomes for children [25]. Another study, conducted in South Africa, found that intake of fat, along with calcium, phosphorous, vitamin D, riboflavin, and vitamin B12 (nutrients that typically occur in milk), was significantly lower in stunted children compared to non-stunted children [26]. A third study found that diets that provide < 22% of energy from fat and that are low in animal fats may restrict growth [27].
In Vietnam, after adjusting for sex, rural/urban residence, total food expenditure, maternal schooling, and paternal schooling, starches were the only food group expenditure category that was significantly associated with future HAZ at both age 5 years and 8 years. The findings regarding starch expenditures in Vietnam were consistent with several other studies that concluded that greater expenditures on rice and grains increased the odds and prevalence, respectively, of child stunting [28,29]. Consumption of starches has been associated with lower dietary diversity, particularly in poor populations in low-income countries, where diets are often unbalanced and composed primarily of starchy staples [30]. There is a large body of research from various countries linking dietary diversity to child growth [30,31,32,33,34].
In Ethiopia the expenditures on specific food groups were not significant when total food expenditure was included in the model, although this was not consistently the case in other countries. When both total food expenditure and expenditures on fat were included in the model in India and Peru (at age 5 years and 8 years), expenditures on fat remained significant. This suggests that total resources spent on food may be more important than expenditures on specific food groups in Ethiopia. Total food expenditures are considered a proxy for household income [32], so this pattern may point to household income and total food availability as key limiting factors for child HAZ in Ethiopia.
Higher parental schooling (both maternal and paternal) was generally associated with higher future HAZ in children, although there were several exceptions. In Ethiopia the highest level of maternal schooling (greater than 12 grades) was not significantly associated with future HAZ at either age and no levels of paternal schooling was associated with HAZ at 12 years. Peruvian households showed no significant association between paternal schooling and future HAZ across all food groups. The associations of mothers’ schooling with child health and nutrition has been well documented [4,35,36], as well as the significance of fathers’ schooling in predicting lower probabilities of stunting [37]. Mothers, though, are more likely than fathers to allocate family resources in ways that promote their children’s nutrition [38], which may help to explain the insignificant paternal schooling associations.
Children residing in urban areas had higher future HAZ compared to children living in rural areas in all four countries. In the final adjusted models for all food groups across all countries, urban residence was associated with a 0.19 to 0.47 increase in future HAZ. These magnitudes of association were second only to those for parental schooling and are consistent with the large body of literature that shows rural children have worse health outcomes compared to their urban-dwelling peers [4,39,40,41].
There are several cross-sectional studies that have demonstrated significant associations between household food expenditures and concurrent child nutritional status. A study conducted using nationally representative survey data from 2007 in Indonesia found that a higher mean proportion of household expenditure on soybeans was significantly associated with lower odds of being wasted (low weight-for-height) and underweight (low weight for age) [42]. Additionally, a lower mean proportion of household expenditure on sugar and cooking oil was significantly associated with lower odds of being wasted or underweight [42]. Another more recent study, also from Indonesia, examined associations between dietary diversity and stunting, but found an unadjusted association between food group expenditures (food groups not specified) and stunting [34]. This was the only significant independent variable not directly assessing food or nutrient consumption used in the study to demonstrate a significant association with child stunting [34]. Research conducted using nutritional surveillance data from 2000 to 2005 in Bangladesh found that for children aged 6–59 months, household expenditure on rice was significantly associated with increased odds of stunting, and expenditure on non-rice foods was significantly associated with decreased odds of stunting [28]. Thus, households in higher quintiles of expenditures on non-rice foods and lower quintiles of expenditures on rice had a lower prevalence of child stunting [28]. Finally, a study conducted using nutritional surveillance data from 1999–2003 in Indonesia found that rural households and urban households drawn from poor communities that spent a greater proportion of their resources on animal source and non-grain foods had a lower prevalence of child stunting [29].
Several previous supplementation trials demonstrated the impact of lipid-based nutrient supplementation in young children on future HAZ, which is likely due in large part to increased caloric intake [43,44,45]. Another possible pathway is that fats may be associated with children’s linear growth due to their importance in ensuring the bioavailability of vitamins such as vitamin A and vitamin D [46,47]. However, studies on dietary fat intake in school-age children are primarily focused on overweight and the reduction of fat intake [48,49]. Our analyses suggest that dietary fat intake may still be a limiting factor for linear growth in some populations.
Limitations
There are several limitations to this study. First, the YL dataset does not provide information on how purchased foods are distributed within the household so that the actual quantity of food each child consumed is unknown. This study focused primarily on how food expenditures were associated with future child height, but there is an extensive literature highlighting the importance of non-food influences on child height [50,51,52,53,54,55]. Many of our models had relatively low R2 values, which speaks to the complexity of child growth and the multiplicity of influences on child HAZ over time. We were limited by the food categorizations used for collecting food expenditure data. Fat expenditures were limited to oil and oil seeds. Other food groups, including dairy (butter, cheese, whole milk products), animal products, and legumes, nuts and seeds (nuts) have additional fats. Thus, the analysis was not able to isolate fat expenditures completely. While we cannot attribute a direct effect of increased spending on oils to an increase in linear growth the results provoke exploration of possible pathways or associations that may explain this robust association. For instance, does increased spending on oil mean increased consumption of higher energy density foods? Further understanding of this association might help us understand more about how dietary patterns that go beyond food ingredients may influence linear growth. Additionally, our analyses using expenditures at any given age (5 years or 8 years) did not consider patterns of spending before or after that age. For this analysis we used expenditures at each age to assess associations with HAZ at the next observed age. This analysis focused on linear growth as the outcome. Future work should incorporate analysis of BMI as an important indicator of healthy growth, given the growing concerns about BMI and risk of obesity in children in countries such as Peru.
5. Conclusions
Our results suggest different facets of food expenditure and procurement may be important for future child HAZ in different countries. In Ethiopia, results pointed to total food expenditure being a critical and significant component associated with subsequent child heights, though expenditures on fats had larger associations with subsequent child heights than other food groups. In India and Peru, expenditure on one specific food group—fats—was significantly positively associated with future HAZ. Finally, in Vietnam, starches were significantly negatively associated with future HAZ, which may relate to the importance of dietary diversity for this country. Stunting and, in general, child undernutrition are complex and multifaceted problems that food expenditure and subsequent consumption can only partly explain. Our results are useful in that they pinpoint specific facets of the diet that may have had the greatest impact on child growth for each country. They also point to the importance of examining context, and caution about generalizing from one country’s situation to others. These results highlight the usefulness of longitudinal household food expenditure survey data that include measures of children’s anthropometrics in analyzing children’s nutrition at the country level. They further provide useful information for child food and nutrition policies in these four countries.
Supplementary Materials
The following are available online at https://www.mdpi.com/1660-4601/17/13/4739/s1: Tables S1–S4: Unadjusted and Adjusted Models for Predicting Child HAZ Using Past Household Starches (S1), Protein (S2), Micronutrients (S3) and ASF (S4) Expenditures in Ethiopia; Tables S5–S8: Unadjusted and Adjusted Models for Predicting Child HAZ Using Past Household Starches (S5), Protein, (S6), Micronutrients (S7) and ASF (S8) Expenditures in India; Tables S9–S12: Unadjusted and Adjusted Models for Predicting Child HAZ Using Past Household Starches (S9), Protein (S10), Micronutrients (S11) and ASF (S12) Expenditures in Peru; Tables S13–S16: Unadjusted and Adjusted Models for Predicting Child HAZ Using Past Household Fats (S13), Protein (S14), Micronutrients (S15) and ASF (S16) Expenditures in Vietnam.
Author Contributions
Conceptualization, D.L.H., J.R.B., M.E.P., B.T.C., K.A.D.; Methodology, D.L.H., J.R.B., M.E.P., B.T.C., K.A.D. and S.E.W.; Software, S.E.W.; Validation, D.L.H. and S.E.W.; Formal analysis, S.E.W.; Data curation, D.L.H. and S.E.W.; Writing—original draft preparation, S.E.W.; Writing—review and editing, all; Visualization, S.E.W. and D.L.H.; Supervision, D.L.H.; Funding acquisition, J.R.B. and K.A.D. All authors have read and agreed to the published version of the manuscript.
Funding
This study is based on research funded by the Bill & Melinda Gates Foundation (Global Health Grant OPP1032713), Eunice Shriver Kennedy National Institute of Child Health and Development (Grant R01 HD070993) and Grand Challenges Canada (Grant 0072-03). The data used in this study come from Young Lives, a 15-year survey investigating the changing nature of childhood poverty in Ethiopia, India (Andhra Pradesh and Telangana), Peru and Vietnam (www.younglives.org.uk). Young Lives was core-funded by the UK Department for International Development (DFID) and was co-funded from 2010 to 2014 by the Netherlands Ministry of Foreign Affairs. The findings and conclusions contained within are those of the authors and do not necessarily reflect positions or policies of the Bill & Melinda Gates Foundation, the Eunice Shriver Kennedy National Institute of Child Health and Development, Grand Challenges Canada, Young Lives, DFID or other funders.
Conflicts of Interest
The authors declare no conflict of interest.
References
- United Nations Children’s Fund; World Health Organization; The World Bank Group (Eds.) UNICEF/WHO/The World Bank Group Joint Child Malnutrition Estimates, Levels and Trends in Child Malnutrition; Key Findings of the 2020 Edition; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Humphries, D.L.; Dearden, K.A.; Crookston, B.T.; Fernald, L.C.; Stein, A.D.; Woldehanna, T.; Penny, M.E.; Behrman, J.R.; The Young Lives Determinants and Consequences of Child Growth Project Team. Cross-Sectional and Longitudinal Associations between Household Food Security and Child Anthropometry at Ages 5 and 8 Years in Ethiopia, India, Peru, and Vietnam. J. Nutr. 2015, 145, 1924–1933. [Google Scholar]
- Martorell, R. The Nature of Child Malnutrition and its Long-Term Implications. Food Nutr. Bull. 1999, 20, 288–292. [Google Scholar] [CrossRef]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Humphries, D.L.; Dearden, K.A.; Crookston, B.T.; Woldehanna, T.; Penny, M.E.; Behrman, J.R.; Young Lives Determinants and Consequences of Child Growth Project Team. Household food group expenditure patterns are associated with child anthropometry at ages 5, 8 and 12 years in Ethiopia, India, Peru and Vietnam. Econ. Hum. Biol. 2017, 26, 30–41. [Google Scholar] [CrossRef]
- Fiedler, J.L.; Lividini, K. Monitoring population diet quality and nutrition status with household consumption and expenditure surveys: Suggestions for a Bangladesh baseline. Food Secur. 2017, 9, 63–88. [Google Scholar] [CrossRef]
- Fiedler, J.L.; Lividini, K.; Bermudez, O.I.; Smitz, M.F. Household Consumption and Expenditures Surveys (HCES): A primer for food and nutrition analysts in low- and middle-income countries. Food Nutr. Bull. 2012, 33 (Suppl. 3), S170–S184. [Google Scholar] [CrossRef]
- Fiedler, J.L.; Martin-Prevel, Y.; Moursi, M. Relative costs of 24-hour recall and Household Consumption and Expenditures Surveys for nutrition analysis. Food Nutr. Bull. 2013, 34, 318–330. [Google Scholar] [CrossRef]
- Jariseta, Z.R.; Dary, O.; Fiedler, J.L.; Franklin, N. Comparison of estimates of the nutrient density of the diet of women and children in Uganda by Household Consumption and Expenditures Surveys (HCES) and 24-hour recall. Food Nutr. Bull. 2012, 33 (Suppl. 3), S199–S207. [Google Scholar] [CrossRef] [PubMed]
- Engle-Stone, R.; Brown, K.H. Comparison of a Household Consumption and Expenditures Survey with Nationally Representative Food Frequency Questionnaire and 24-hour Dietary Recall Data for Assessing Consumption of Fortifiable Foods by Women and Young Children in Cameroon. Food Nutr. Bull. 2015, 36, 211–230. [Google Scholar] [CrossRef] [PubMed]
- Naska, A.; Vasdekis, V.G.; Trichopoulou, A. A preliminary assessment of the use of household budget survey data for the prediction of individual food consumption. Public Health Nutr. 2001, 4, 1159–1165. [Google Scholar] [PubMed]
- Dary, O.; Jariseta, Z.R. Validation of dietary applications of Household Consumption and Expenditures Surveys (HCES) against a 24-hour recall method in Uganda. Food Nutr. Bull. 2012, 33 (Suppl. 3), S190–S198. [Google Scholar] [CrossRef] [PubMed]
- Barnett, I.; Ariana, P.; Petrou, S.; Penny, M.E.; Duc le, T.; Galab, S.; Woldehanna, T.; Escobal, J.A.; Plugge, E.; Boyden, J. Cohort profile: The Young Lives study. Int. J. Epidemiol. 2013, 42, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Oxford Department of International Development. Young Lives: A Longitudinal Study into Children and Youth around the World. Available online: https://www.younglives.org.uk/ (accessed on 26 June 2020).
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices Part II: Measurement; World Health Organization Department of Child and Adolescent Health and Development: Geneva, Switzerland, 2010. [Google Scholar]
- Kennedy, G.; Ballard, T.; Dop, M.; Nutrition Consumer Protection Division FAO. Guidelines for Measuring Household and Individual Dietary Diversity; Food and Agriculture Organization of the United Nations: Rome, Italy, 2013. [Google Scholar]
- Kennedy, G.; Fanou-Fogny, N.; Seghieri, C.; Arimond, M.; Koreissi, Y.; Dossa, R.; Kok, F.J.; Brouwer, I.D. Food groups associated with a composite measure of probability of adequate intake of 11 micronutrients in the diets of women in urban Mali. J. Nutr. 2010, 140, 2070S–2078S. [Google Scholar] [CrossRef]
- Glewwe, P.; Twum-Baah, K.A. The Distribution of Welfare in Ghana, 1987–1988; World Bank Living Standards Measurement Study Working Paper; The World Bank: Washington, DC, USA, 1991; Volume 75. [Google Scholar]
- Reifman, A.; Keyton, K. Winsorize. In Encyclopedia of Research Design; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2010; pp. 1636–1638. [Google Scholar]
- WHO Child Growth Standards Based on Length/Height, Weight and Age. Acta Paediatr. 2006, 95, 76–85.
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- de Onis, M.; Blössner, M. WHO Global Database on Child Growth and Malnutrition; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Food and Agriculture Organization. FAOSTAT: Food and Agriculture Data. Available online: http://www.fao.org/faostat/en/#home (accessed on 31 May 2017).
- Al-Agha, A.; Al-Baradi, W.; Al-Rahmani, D.; Simbawa, B. Associations between various nutritional elements and weight, height and bmi in children and adolescents. J. Pat. Care 2016, 2, 2. [Google Scholar]
- Maitra, P.; Rammohan, A.; Ray, R.; Robitaille, M.-C. Food consumption patterns and malnourished Indian children: Is there a link? Food Policy 2013, 38, 70–81. [Google Scholar] [CrossRef]
- Van Stuijvenberg, M.E.; Nel, J.; Schoeman, S.E.; Lombard, C.J.; du Plessis, L.M.; Dhansay, M.A. Low intake of calcium and vitamin D, but not zinc, iron or vitamin A, is associated with stunting in 2- to 5-year-old children. Nutrition 2015, 31, 841–846. [Google Scholar] [CrossRef]
- Uauy, R.; Mize, C.E.; Castillo-Duran, C. Fat intake during childhood: Metabolic responses and effects on growth. Am. J. Clin. Nutr. 2000, 72 (Suppl. 5), 1354s–1360s. [Google Scholar] [CrossRef]
- Campbell, A.A.; de Pee, S.; Sun, K.; Kraemer, K.; Thorne-Lyman, A.; Moench-Pfanner, R.; Sari, M.; Akhter, N.; Bloem, M.W.; Semba, R.D. Household rice expenditure and maternal and child nutritional status in Bangladesh. J. Nutr. 2010, 140, 189S–194S. [Google Scholar] [CrossRef]
- Sari, M.; de Pee, S.; Bloem, M.W.; Sun, K.; Thorne-Lyman, A.L.; Moench-Pfanner, R.; Akhter, N.; Kraemer, K.; Semba, R.D. Higher household expenditure on animal-source and nongrain foods lowers the risk of stunting among children 0–59 months old in Indonesia: Implications of rising food prices. J. Nutr. 2010, 140, 195S–200S. [Google Scholar] [CrossRef] [PubMed]
- Busert, L.K.; Neuman, M.; Rehfuess, E.A.; Dulal, S.; Harthan, J.; Chaube, S.S.; Bhandari, B.; Costello, H.; Costello, A.; Manandhar, D.S.; et al. Dietary Diversity Is Positively Associated with Deviation from Expected Height in Rural Nepal. J. Nutr. 2016, 146, 1387–1393. [Google Scholar] [CrossRef] [PubMed]
- Rah, J.H.; Akhter, N.; Semba, R.D.; de Pee, S.; Bloem, M.W.; Campbell, A.A.; Moench-Pfanner, R.; Sun, K.; Badham, J.; Kraemer, K. Low dietary diversity is a predictor of child stunting in rural Bangladesh. Eur. J. Clin. Nutr. 2010, 64, 1393–1398. [Google Scholar] [CrossRef] [PubMed]
- Thorne-Lyman, A.L.; Valpiani, N.; Sun, K.; Semba, R.D.; Klotz, C.L.; Kraemer, K.; Akhter, N.; de Pee, S.; Moench-Pfanner, R.; Sari, M. Household dietary diversity and food expenditures are closely linked in rural Bangladesh, increasing the risk of malnutrition due to the financial crisis. J. Nutr. 2010, 140, 182S–188S. [Google Scholar] [CrossRef]
- Motbainor, A.; Worku, A.; Kumie, A. Stunting Is Associated with Food Diversity while Wasting with Food Insecurity among Underfive Children in East and West Gojjam Zones of Amhara Region, Ethiopia. PLoS ONE 2015, 10, e0133542. [Google Scholar] [CrossRef]
- Mahmudiono, T.; Sumarmi, S.; Rosenkranz, R.R. Household dietary diversity and child stunting in East Java, Indonesia. Asia Pac. J. Clin. Nutr. 2017, 26, 317–325. [Google Scholar]
- Abuya, B.A.; Ciera, J.; Kimani-Murage, E. Effect of mother’s education on child’s nutritional status in the slums of Nairobi. BMC Pediatr. 2012, 12, 80. [Google Scholar] [CrossRef]
- Makoka, D.; Masibo, P.K. Is there a threshold level of maternal education sufficient to reduce child undernutrition? Evidence from Malawi, Tanzania and Zimbabwe. BMC Pediatr. 2015, 15, 96. [Google Scholar] [CrossRef]
- Semba, R.D.; de Pee, S.; Sun, K.; Sari, M.; Akhter, N.; Bloem, M.W. Effect of parental formal education on risk of child stunting in Indonesia and Bangladesh: A cross-sectional study. Lancet 2008, 371, 322–328. [Google Scholar] [CrossRef]
- Pfeiffer, J.; Gloyd, S.; Ramirez Li, L. Intrahousehold resource allocation and child growth in Mozambique: An ethnographic case-control study. Soc. Sci. Med. 2001, 53, 83–97. [Google Scholar] [CrossRef]
- Senbanjo, I.O.; Olayiwola, I.O.; Afolabi, W.A.; Senbanjo, O.C. Maternal and child under-nutrition in rural and urban communities of Lagos state, Nigeria: The relationship and risk factors. BMC Res. Notes 2013, 6, 286. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, C.S.; Zanello, G.; Shankar, B. Rural-urban disparities in child nutrition in Bangladesh and Nepal. BMC Public Health 2013, 13, 581. [Google Scholar] [CrossRef] [PubMed]
- Mussa, R. A matching decomposition of the rural-urban difference in malnutrition in Malawi. Health Econ. Rev. 2014, 4, 11. [Google Scholar] [CrossRef] [PubMed]
- Mauludyani, A.V.; Fahmida, U.; Santika, O. Relationship between household expenditures on strategic foods and prevalence of undernutrition among children 0 to 23 months of age in Indonesia. Food Nutr. Bull. 2014, 35, 440–448. [Google Scholar] [CrossRef]
- Dewey, K.G.; Arimond, M. Lipid-based nutrient supplements: How can they combat child malnutrition? PLoS Med. 2012, 9, e1001314. [Google Scholar] [CrossRef]
- Dewey, K.G.; Mridha, M.K.; Matias, S.L.; Arnold, C.D.; Cummins, J.R.; Khan, M.S.; Maalouf-Manasseh, Z.; Siddiqui, Z.; Ullah, M.B.; Vosti, S.A. Lipid-based nutrient supplementation in the first 1000 d improves child growth in Bangladesh: A cluster-randomized effectiveness trial. Am. J. Clin. Nutr. 2017, 105, 944–957. [Google Scholar] [CrossRef]
- Mridha, M.K.; Matias, S.L.; Chaparro, C.M.; Paul, R.R.; Hussain, S.; Vosti, S.A.; Harding, K.L.; Cummins, J.R.; Day, L.T.; Saha, S.L.; et al. Lipid-based nutrient supplements for pregnant women reduce newborn stunting in a cluster-randomized controlled effectiveness trial in Bangladesh. Am. J. Clin. Nutr. 2016, 103, 236–249. [Google Scholar] [CrossRef]
- Ciresi, A.; Giordano, C. Vitamin D across growth hormone (GH) disorders: From GH deficiency to GH excess. Growth Horm. IGF Res. 2017, 33, 35–42. [Google Scholar] [CrossRef]
- Roberts, J.L.; Stein, A.D. The Impact of Nutritional Interventions beyond the First 2 Years of Life on Linear Growth: A Systematic Review and Meta-Analysis. Adv. Nutr. 2017, 8, 323–336. [Google Scholar] [CrossRef]
- Perichart-Perera, O.; Balas-Nakash, M.; Rodriguez-Cano, A.; Munoz-Manrique, C.; Monge-Urrea, A.; Vadillo-Ortega, F. Correlates of dietary energy sources with cardiovascular disease risk markers in Mexican school-age children. J. Am. Diet. Assoc. 2010, 110, 253–260. [Google Scholar] [CrossRef]
- Villalpando, S.; Lara Zamudio, Y.; Shamah-Levy, T.; Mundo-Rosas, V.; Manzano, A.C.; Lamadrid-Figueroa, H. Substitution of whole cows’ milk with defatted milk for 4 months reduced serum total cholesterol, HDL-cholesterol and total apoB in a sample of Mexican school-age children (6–16 years of age). Br. J. Nutr. 2015, 114, 788–795. [Google Scholar] [CrossRef] [PubMed]
- Dangour, A.D.; Watson, L.; Cumming, O.; Boisson, S.; Che, Y.; Velleman, Y.; Cavill, S.; Allen, E.; Uauy, R. Interventions to improve water quality and supply, sanitation and hygiene practices, and their effects on the nutritional status of children. Cochrane Database Syst. Rev. 2013, 8, CD009382. [Google Scholar] [CrossRef] [PubMed]
- Fikadu, T.; Assegid, S.; Dube, L. Factors associated with stunting among children of age 24 to 59 months in Meskan district, Gurage Zone, South Ethiopia: A case-control study. BMC Public Health 2014, 14, 800. [Google Scholar] [CrossRef] [PubMed]
- Shinsugi, C.; Matsumura, M.; Karama, M.; Tanaka, J.; Changoma, M.; Kaneko, S. Factors associated with stunting among children according to the level of food insecurity in the household: A cross-sectional study in a rural community of Southeastern Kenya. BMC Public Health 2015, 15, 441. [Google Scholar] [CrossRef]
- Griffen, A.S. Height and calories in early childhood. Econ. Hum. Biol. 2016, 20, 55–69. [Google Scholar] [CrossRef] [PubMed]
- Krishna, A.; Fink, G.; Berkman, L.F.; Subramanian, S.V. Short- and long-run associations between birth weight and children’s height. Econ. Hum. Biol. 2016, 21, 156–166. [Google Scholar] [CrossRef]
- Dearden, K.A.; Schott, W.; Crookston, B.T.; Humphries, D.L.; Penny, M.E.; Behrman, J.R.; Young Lives Determinants and Consequences of Child Growth Project Team. Children with access to improved sanitation but not improved water are at lower risk of stunting compared to children without access: A cohort study in Ethiopia, India, Peru, and Vietnam. BMC Public Health 2017, 17, 110. [Google Scholar] [CrossRef]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).