Differences in Anthropometric and Clinical Features among Preschoolers, School-Age Children, and Adolescents with Obstructive Sleep Apnea—A Hospital-Based Study in Taiwan


 , ,
, ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Patient Selection and Grouping
2.3. Measurements
2.3.1. Anthropometrics
2.3.2. Blood Pressure
2.3.3. Tonsil Size and Adenoid Size
2.3.4. Systemic Inflammatory Markers
2.3.5. Polysomnography
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the Three Subgroups Stratified by Age
3.2. Associations between Patients’ Characteristics, Blood Pressure, Inflammatory Biomarkers, and Polysomnography Parameters in the Overall Cohort and Three Subgroups
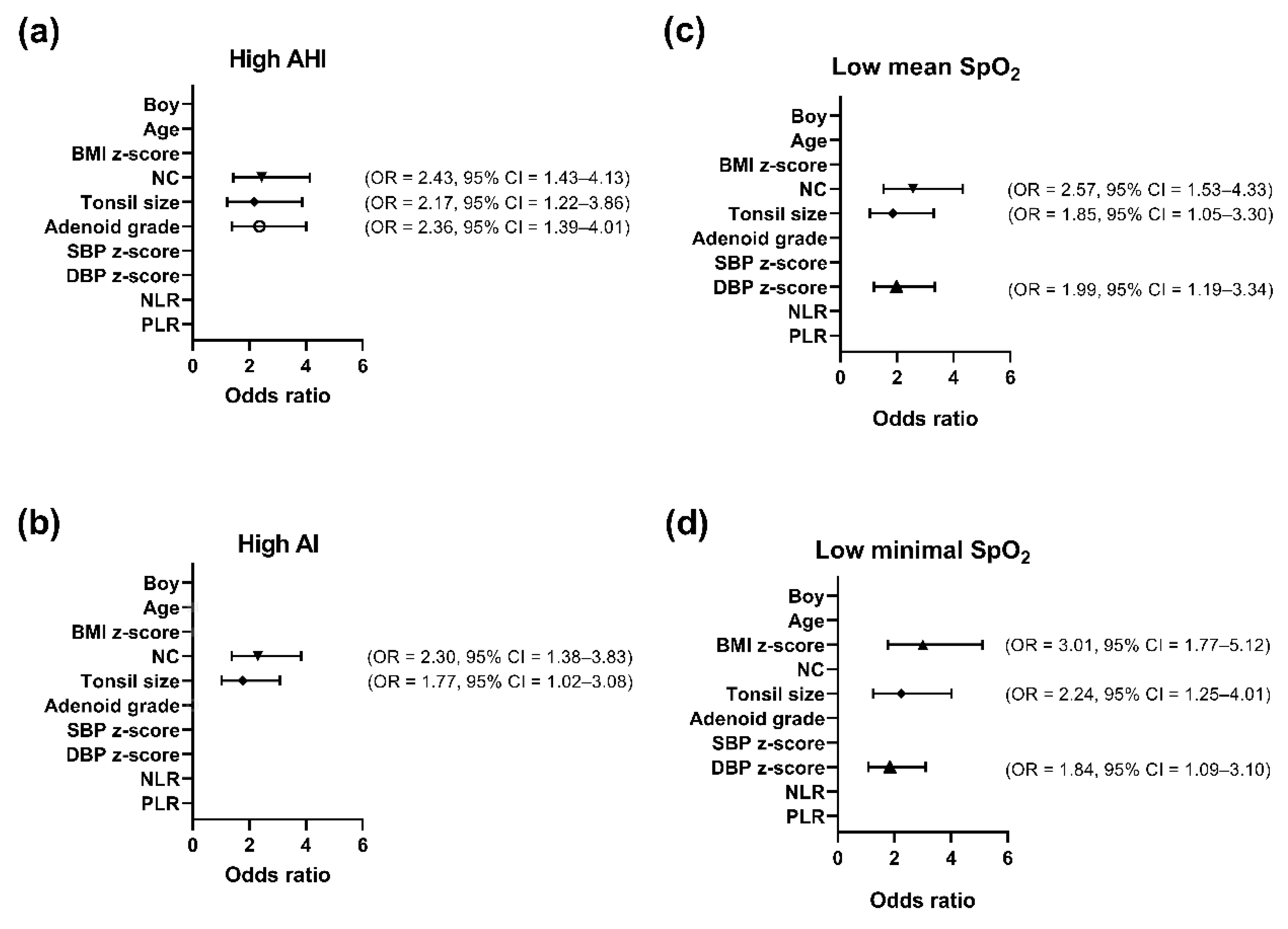
3.3. Variables Independently Associated with AHI, AI, Mean SpO2, or Minimal SpO2 in the Overall Cohort Using Multivariate Logistic Regression Analysis (Figure 1)
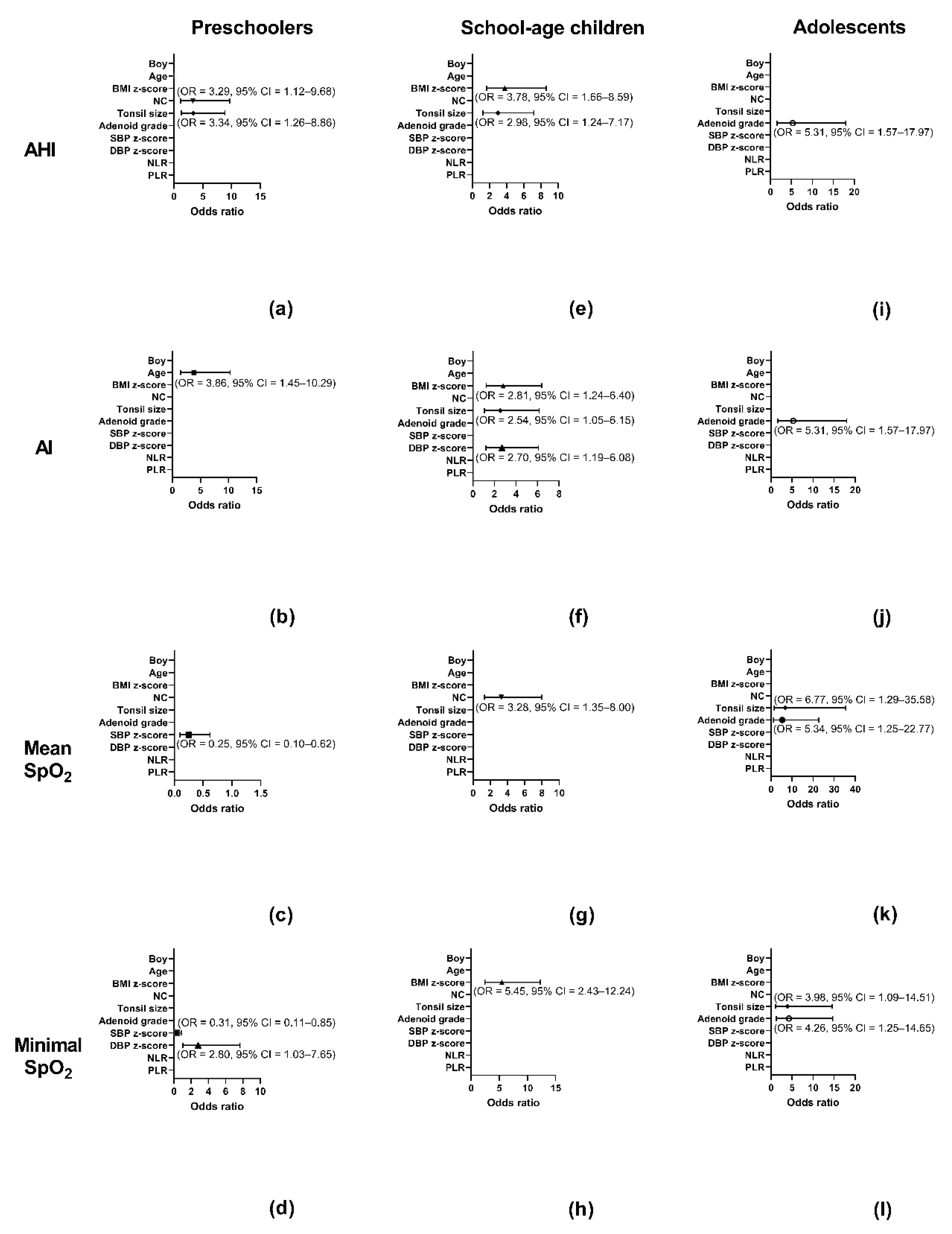
3.4. Independent Variables Associated with AHI, AI, Mean SpO2, or Minimal SpO2 in the Subgroups Using Multivariate Logistic Regression Analysis (Figure 1)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Senaratna, C.; Perret, J.L.; Lodge, C.; Lowe, A.; Campbell, B.E.; Matheson, M.; Hamilton, G.S.; Dharmage, S.C. Prevalence of Obstructive Sleep Apnea in the General Population: A Systematic Review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Franklin, K.; Lindberg, E. Obstructive Sleep Apnea Is a Common Disorder in the population—a Review on the Epidemiology of Sleep Apnea. J. Thorac. Dis. 2015, 7, 1311–1322. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, L.M.; Holbrook, C.R.; Mervis, C.B.; Klaus, C.J.; Bruner, J.L.; Raffield, T.J.; Rutherford, J.; Mehl, R.C.; Wang, M.; Tuell, A.; et al. Sleep and Neurobehavioral Characteristics of 5- to 7-Year-Old Children with Parentally Reported Symptoms of Attention-deficit/Hyperactivity Disorder. Pediatrics 2003, 111, 554–563. [Google Scholar] [CrossRef]
- Bixler, E.O.; Vgontzas, A.N.; Lin, H.-M.; Liao, D.; Calhoun, S.; Vela-Bueno, A.; Fedok, F.; Vlasic, V.; Graff, G. Sleep Disordered Breathing in Children in a General Population Sample: Prevalence and Risk Factors. Sleep 2009, 32, 731–736. [Google Scholar] [CrossRef]
- Andersen, I.G.; Holm, J.; Homøe, P. Obstructive Sleep Apnea in Children and Adolescents with and Without Obesity. Eur. Arch. Oto-Rhino-Laryngology 2019, 276, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Ward, S.D.; Sheldon, S.H.; Shiffman, R.N.; et al. Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome. Pediatrics 2012, 130, e714–e755. [Google Scholar] [CrossRef]
- Zinchuk, A.V.; Gentry, M.; Concato, J.; Yaggi, H.K. Phenotypes in Obstructive Sleep Apnea: A Definition, Examples and Evolution of Approaches. Sleep Med. Rev. 2016, 35, 113–123. [Google Scholar] [CrossRef]
- Ayas, N.; Owens, R.L.; Kheirandish-Gozal, L. Update in Sleep Medicine 2014. Am. J. Respir. Crit. Care Med. 2015, 192, 415–420. [Google Scholar] [CrossRef]
- Keenan, B.T.; Kim, J.; Singh, B.; Bittencourt, L.R.A.; Chen, N.-H.; Cistulli, P.A.; Magalang, U.J.; McArdle, N.; Mindel, J.W.; Benediktsdóttir, B.; et al. Recognizable Clinical Subtypes of Obstructive Sleep Apnea across International Sleep Centers: A Cluster Analysis. Sleep 2018, 41, 41. [Google Scholar] [CrossRef]
- Ye, L.; Pien, G.W.; Ratcliffe, S.; Björnsdottir, E.; Arnardottir, E.S.; Pack, A.I.; Benediktsdottir, B.; Gislason, T. The Different Clinical Faces of Obstructive Sleep Apnoea: A Cluster Analysis. Eur. Respir. J. 2014, 44, 1600–1607. [Google Scholar] [CrossRef]
- Kang, K.-T.; Lee, P.-L.; Weng, W.-C.; Hsu, W.-C. Body Weight Status and Obstructive Sleep Apnea in Children. Int. J. Obes. 2012, 36, 920–924. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, E.O.; Haddad, F.L.M.; Stefanini, R.; Moreira, G.A.; Rapoport, P.B.; Gregório, L.C.; Tufik, S.; Bittencourt, L.R.A. Clinicals and Upper Airway Characteristics in Obese Children with Obstructive Sleep Apnea. Sleep Sci. 2017, 10, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.-T.; Chou, C.-H.; Weng, W.-C.; Lee, P.-L.; Hsu, W.-C. Associations Between Adenotonsillar Hypertrophy, Age, and Obesity in Children with Obstructive Sleep Apnea. PLoS ONE 2013, 8, e78666. [Google Scholar] [CrossRef]
- Su, M.-S.; Zhang, H.-L.; Cai, X.-H.; Lin, Y.; Liu, P.-N.; Zhang, Y.-B.; Hu, W.-Z.; Li, C.-C.; Xiao, Y.-F. Obesity in Children with Different Risk Factors for Obstructive Sleep Apnea: A Community-Based Study. Eur. J. Nucl. Med. Mol. Imaging 2015, 175, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Brockmann, P.E.; Koren, D.; Kheirandish-Gozal, L.; Gozal, D. Gender Dimorphism in Pediatric OSA: Is It for Real? Respir. Physiol. Neurobiol. 2017, 245, 83–88. [Google Scholar] [CrossRef]
- Dayyat, E.; Kheirandish-Gozal, L.; Capdevila, O.S.; Maarafeya, M.M.A.; Gozal, D. Obstructive Sleep Apnea in Children. Chest 2009, 136, 137–144. [Google Scholar] [CrossRef]
- Chuang, H.-H.; Huang, Y.-S.; Chen, N.-H.; Li, H.-Y.; Fang, T.-J.; Hsu, J.-F.; Lai, H.-C.; Chen, J.-Y.; Lee, L.-A.; Huang, C.-G.; et al. Relationships Among and Predictive Values of Obesity, Inflammation Markers, and Disease Severity in Pediatric Patients with Obstructive Sleep Apnea Before and After Adenotonsillectomy. J. Clin. Med. 2020, 9, 579. [Google Scholar] [CrossRef]
- Keefe, K.R.; Patel, P.N.; Levi, J.R. The Shifting Relationship Between Weight and Pediatric Obstructive Sleep Apnea: A Historical Review. Laryngoscope 2018, 129, 2414–2419. [Google Scholar] [CrossRef]
- Kaditis, A.; Kheirandish-Gozal, L.; Gozal, D. Algorithm for the Diagnosis and Treatment of Pediatric OSA: A Proposal of Two Pediatric Sleep Centers. Sleep Med. 2012, 13, 217–227. [Google Scholar] [CrossRef]
- Baugh, A.D.; Archer, S.M.; Mitchell, R.B.; Rosenfeld, R.M.; Amin, R.; Burns, J.J.; Darrow, D.H.; Giordano, T.; Litman, R.S.; Li, K.K.; et al. Clinical Practice Guideline: Tonsillectomy in Children. Otolaryngol. Neck Surg. 2011, 144, S1–S30. [Google Scholar] [CrossRef]
- Huang, Y.-S.; Guilleminault, C.; Lee, L.-A.; Lin, C.-H.; Hwang, F.-M. Treatment Outcomes of Adenotonsillectomy for Children with Obstructive Sleep Apnea: A Prospective Longitudinal Study. Sleep 2014, 37, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-S.; Guilleminault, C.; Hwang, F.-M.; Cheng, C.; Lin, C.-H.; Li, H.-Y.; Lee, L.-A. Inflammatory Cytokines in Pediatric Obstructive Sleep Apnea. Medicine 2016, 95, e4944. [Google Scholar] [CrossRef] [PubMed]
- CDC. Child Development-Positive Parenting Tips. Available online: https://www.cdc.gov/ncbddd/childdevelopment/positiveparenting/preschoolers.Html (accessed on 30 April 2020).
- WHO. Recognizing Adolescence. Available online: https://apps.who.int/adolescent/second-decade/section2/page1/recognizing-adolescence.html (accessed on 30 April 2020).
- Nafiu, O.O.; Burke, C.; Lee, J.; Voepel-Lewis, T.; Malviya, S.; Tremper, K.K. Neck Circumference As a Screening Measure for Identifying Children With High Body Mass Index. Pediatrics 2010, 126, 306–310. [Google Scholar] [CrossRef]
- The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. Pediatrics 2004, 114, 555–576. [CrossRef]
- Brodsky, L. Modern Assessment of Tonsils and Adenoids. Pediatr. Clin. North Am. 1989, 36, 1551–1569. [Google Scholar] [CrossRef]
- Tagaya, M.; Nakata, S.; Yasuma, F.; Miyazaki, S.; Sasaki, F.; Morinaga, M.; Suzuki, K.; Otake, H.; Nakashima, T. Relationship Between Adenoid Size and Severity of Obstructive Sleep Apnea in Preschool Children. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 1827–1830. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.-A.; Huang, C.-G.; Chen, N.-H.; Wang, C.-L.; Fang, T.-J.; Li, H.-Y. Severity of Obstructive Sleep Apnea Syndrome and High-Sensitivity C-Reactive Protein Reduced After Relocation Pharyngoplasty. Otolaryngol. Neck Surg. 2011, 144, 632–638. [Google Scholar] [CrossRef]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef]
- Wimms, A.; Woehrle, H.; Ketheeswaran, S.; Ramanan, D.; Armitstead, J. Obstructive Sleep Apnea in Women: Specific Issues and Interventions. BioMed Res. Int. 2016, 2016, 1–9. [Google Scholar] [CrossRef]
- Bonsignore, M.R.; Saaresranta, T.; Riha, R.L. Sex Differences in Obstructive Sleep Apnoea. Eur. Respir. Rev. 2019, 28, 28. [Google Scholar]
- Rao, G. Diagnosis, Epidemiology, and Management of Hypertension in Children. Pediatrics 2016, 138, e20153616. [Google Scholar] [CrossRef] [PubMed]
- Sabri, M.; Gheissari, A.; Mansourian, M.; Mohammadifard, N.; Sarrafzadegan, N. Essential Hypertension in Children, a Growing Worldwide Problem. J. Res. Med Sci. 2019, 24, 109. [Google Scholar] [CrossRef]
- Mohan, B.; Verma, A.; Singh, K.; Singh, K.; Sharma, S.; Bansal, R.; Tandon, R.; Goyal, A.; Singh, B.; Chhabra, S.T.; et al. Prevalence of Sustained Hypertension and Obesity Among Urban and Rural Adolescents: A School-Based, Cross-Sectional Study in North India. BMJ Open 2019, 9, e027134. [Google Scholar] [CrossRef]
- Pede, S.; Lombardo, M. Cardiovascular Risk Stratification. Systolic, Diastolic or Pulse pressure? Ital. Heart J. Suppl. 2001, 2, 356–358. [Google Scholar] [PubMed]
- Lip, S.; Tan, L.E.; Jeemon, P.; McCallum, L.; Dominiczak, A.F.; Padmanabhan, S. Diastolic Blood Pressure J-Curve Phenomenon in a Tertiary-Care Hypertension Clinic. Hypertens. 2019, 74, 767–775. [Google Scholar] [CrossRef]
- Leonetti, G.; Cuspidi, C. Recent Knowledge on the Role of Diastolic Blood Pressure in Hypertensive Patients on treatment. Recenti progressi med. 2008, 99, 191–199. [Google Scholar]
- Mandaliya, H.; Jones, M.; Oldmeadow, C.; Nordman, I.I.C. Prognostic Biomarkers in Stage IV Non-Small Cell Lung Cancer (NSCLC): Neutrophil to Lymphocyte Ratio (NLR), Lymphocyte to Monocyte Ratio (LMR), Platelet to Lymphocyte Ratio (PLR) and Advanced Lung Cancer Inflammation Index (ALI). Transl. Lung Cancer Res. 2019, 8, 886–894. [Google Scholar] [CrossRef]
- Lalosevic, M.S.; Markovic, A.P.; Stankovic, S.; Lalosevic, M.S.; Dimitrijevic, I.; Vujacic, I.R.; Lalic, D.; Milovanovic, T.; Dumic, I.; Krivokapic, Z. Combined Diagnostic Efficacy of Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and Mean Platelet Volume (MPV) As Biomarkers of Systemic Inflammation in the Diagnosis of Colorectal Cancer. Dis. Markers 2019, 2019, 6036979–6036987. [Google Scholar] [CrossRef]
- Gasparyan, A.Y.; Ayvazyan, L.; Mukanova, U.; Yessirkepov, M.; Kitas, G.D. The Platelet-to-Lymphocyte Ratio as an Inflammatory Marker in Rheumatic Diseases. Ann. Lab. Med. 2019, 39, 345–357. [Google Scholar] [CrossRef]
- Koseoglu, H.I.; Altunkaş, F.; Kanbay, A.; Doruk, S.; Etikan, I.; Demir, O. Platelet–lymphocyte Ratio Is an Independent Predictor for Cardiovascular Disease in Obstructive Sleep Apnea Syndrome. J. Thromb. Thrombolysis 2014, 39, 179–185. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Preschoolers | School-age children | Adolescents | p-Value1 |
|---|---|---|---|---|
| Patients | n = 84 | n = 113 | n = 56 | |
| Boys (n) | 51 (60.7) | 88 (77.9) | 44 (78.6) | 0.014 |
| Age (years) | 5.0 (4.1–5.5) 2 | 7.0 (6.3–8.5) 2,3 | 11.0 (11.2–12.0) 2,3 | <0.001 |
| BMI (kg/m2) z-score | 0.24 (-0.55–1.01) 2 | 1.17 (−0.07–2.05) 2 | 1.41 (0.69–2.05) 2 | <0.001 |
| NC (cm) | 26.3 (25.0–2.05) 2 | 29.8 (26.4–31.8) 2,3 | 32.3 (30.8–35.0) 2,3 | <0.001 |
| Tonsil size | 3 (3–4) | 3 (3–4) | 3 (3–4) | 0.725 |
| Adenoid grade | 4 (3–4) 2 | 3 (3–4) | 3 (2–4) 2 | 0.026 |
| SBP (mmHg) z-score | 0.25 (−0.56–1.45) 2 | 0.45 (−0.54–1.80) | 0.85 (0.02–1.97) 2 | 0.046 |
| DBP (mmHg) z-score | 0.81 (0.30–1.49) 2 | 0.38 (−0.11–1.05) 2 | 0.42 (−0.10–1.05) 2 | 0.006 |
| NLR | 1.06 (0.82–1.53) 2 | 1.24 (0.92–1.64) 3 | 1.51 (1.07–2.01) 2,3 | 0.002 |
| PLR | 94.1 (79.2–117.2) 2 | 103.3 (86.5–129.5) | 110.2 (93.5–127.0) 2 | 0.024 |
| AHI (events/h) | 11.2 (5.2–22.4) | 8.7 (3.6–20.4) | 9.8 (3.6–22.4) | 0.667 |
| AI (events/h) | 3.6 (1.5–8.1) | 2.8 (1.2–8.7) | 2.2 (1.2–9.5) | 0.549 |
| Mean SpO2 (%) | 97 (95–98) | 97 (95–98) 3 | 96 (94–97) 3 | 0.038 |
| Minimal SpO2 (%) | 85 (81–91) | 88 (83–92) | 87 (82–91) | 0.156 |
| Variables | Boys | Age | BMI z-Score | NC | Tonsil Size | Adenoid Grade | SBP z-Score | DBP z-Score | NLR | PLR |
|---|---|---|---|---|---|---|---|---|---|---|
| Overall Group (n = 253) | ||||||||||
| AHI (events/h) | 0.05 (0.454) | −0.01 (0.983) | 0.25 (<0.001) | 0.22 (<0.001) | 0.23 (<0.001) | 0.28 (<0.001) | 0.09 (0.154) | 0.17 (0.007) | 0.10 (0.127) | −0.05 (0.413) |
| AI (events/h) | 0.01 (0.989) | −0.01 (0.975) | 0.19 (0.002) | 0.17 (0.006) | 0.16 (0.012) | 0.23 (<0.001) | 0.04 (0.530) | 0.12 (0.049) | 0.09 (0.152) | −0.03 (0.694) |
| Mean SpO2 (%) | 0.01 (0.989) | −0.14 (0.023) | −0.24 (<0.001) | −0.23 (<0.001) | −0.04 (0.511) | −0.09 (0.175) | −0.01 (0.866) | −0.20 (0.001) | −0.15 (0.017) | −0.01 (0.859) |
| Minimal SpO2 (%) | −0.04 (0.518) | 0.04 (0.582) | −0.29 (<0.001) | −0.26 (<0.001) | −0.17 (0.008) | −0.17 (0.006) | −0.07 (0.268) | −0.19 (0.003) | −0.10 (0.111) | −0.01 (0.972) |
| Preschoolers (n = 84) | ||||||||||
| AHI (events/h) | 0.18 (0.099) | 0.12 (0.284) | 0.15 (0.174) | 0.20 (0.070) | 0.34 (0.002) | 0.25 (0.023) | −0.07 (0.524) | 0.08 (0.469) | 0.02 (0.882) | 0.03 (0.785) |
| AI (events/h) | 0.11 (0.314) | 0.16 (0.138) | 0.12 (0.298) | 0.10 (0.360) | 0.21 (0.057) | 0.10 (0.360) | −0.14 (0.212) | 0.03 (0.799) | 0.04 (0.724) | 0.08 (0.446) |
| Mean SpO2 (%) | −0.09 (0.400) | −0.3 (0.798) | −0.10 (0.377) | −0.09 (0.399) | −0.04 (0.728) | −0.02 (0.896) | 0.21 (0.059) | −0.10 (0.354) | −0.02 (0.874) | −0.17 (0.123) |
| Minimal SpO2 (%) | −0.04 (0.726) | 0.13 (0.249) | −0.18 (0.101) | −0.21 (0.058) | −0.19 (0.085) | −0.09 (0.422) | 0.10 (0.358) | −0.17 (0.131) | 0.03 (0.802) | −0.20 (0.067) |
| School−Age Children (n = 113) | ||||||||||
| AHI (events/h) | −0.08 (0.376) | 0.08 (0.374) | 0.31 (0.001) | 0.30 (0.001) | 0.20 (0.037) | 0.18 (0.063) | 0.23 (0.016) | 0.27 (0.004) | 0.07 (0.476) | −0.07 (0.473) |
| AI (events/h) | −0.09 (0.326) | 0.10 (0.295) | 0.25 (0.008) | 0.29 (0.002) | 0.13 (0.169) | 0.16 (0.088) | 0.15 (0.103) | 0.20 (0.039) | 0.10 (0.302) | −0.03 (0.726) |
| Mean SpO2 (%) | 0.07 (0.496) | −0.16 (0.101) | −0.31 (<0.001) | −0.29 (0.002) | −0.03 (0.757) | −0.07 (0.486) | −0.09 (0.344) | −0.31 (0.001) | −0.18 (0.054) | 0.07 (0.480) |
| Minimal SpO2 (%) | 0.02 (0.844) | −0.18 (0.059) | −0.43 (<0.001) | −0.43 (<0.001) | −0.15 (0.112) | −0.09 (0.344) | −0.20 (0.039) | −0.24 (0.012) | −0.19 (0.048) | 0.07 (0.447) |
| Adolescents (n = 56) | ||||||||||
| AHI (events/h) | 0.21 (0.130) | 0.17 (0.21) | 0.37 (0.005) | 0.34 (0.010) | 0.18 (0.186) | 4.0 (0.002) | 0.07 (0.630) | 0.02 (0.860) | 0.34 (0.010) | 0.01 (0.956) |
| AI (events/h) | 0.07 (0.615) | 0.23 (0.085) | 0.24 (0.074) | 0.22 (0.104) | 0.16 (0.242) | 0.41 (0.002) | 0.12 (0.375) | 0.06 (0.645) | 0.20 (0.143) | −0.04 (0.785) |
| Mean SpO2 (%) | 0.04 (0.750) | −0.24 (0.081) | −0.17 (0.219) | −0.24 (0.081) | −0.13 (0.359) | −0.29 (0.030) | −0.06 (0.640) | −0.18 (0.180) | −0.19 (0.154) | 0.04 (0.768) |
| Minimal SpO2 (%) | −0.24 (0.071) | −0.07 (0.594) | −0.34 (0.010) | −0.36 (0.006) | −0.20 (0.132) | −0.34 (0.010) | −0.05 (0.700) | 0.01 (0.992) | −0.22 (0.102) | −0.02 (0.869) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chuang, H.-H.; Hsu, J.-F.; Chuang, L.-P.; Chen, N.-H.; Huang, Y.-S.; Li, H.-Y.; Chen, J.-Y.; Lee, L.-A.; Huang, C.-G. Differences in Anthropometric and Clinical Features among Preschoolers, School-Age Children, and Adolescents with Obstructive Sleep Apnea—A Hospital-Based Study in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 4663. https://doi.org/10.3390/ijerph17134663
Chuang H-H, Hsu J-F, Chuang L-P, Chen N-H, Huang Y-S, Li H-Y, Chen J-Y, Lee L-A, Huang C-G. Differences in Anthropometric and Clinical Features among Preschoolers, School-Age Children, and Adolescents with Obstructive Sleep Apnea—A Hospital-Based Study in Taiwan. International Journal of Environmental Research and Public Health. 2020; 17(13):4663. https://doi.org/10.3390/ijerph17134663
Chicago/Turabian StyleChuang, Hai-Hua, Jen-Fu Hsu, Li-Pang Chuang, Ning-Hung Chen, Yu-Shu Huang, Hsueh-Yu Li, Jau-Yuan Chen, Li-Ang Lee, and Chung-Guei Huang. 2020. "Differences in Anthropometric and Clinical Features among Preschoolers, School-Age Children, and Adolescents with Obstructive Sleep Apnea—A Hospital-Based Study in Taiwan" International Journal of Environmental Research and Public Health 17, no. 13: 4663. https://doi.org/10.3390/ijerph17134663
APA StyleChuang, H.-H., Hsu, J.-F., Chuang, L.-P., Chen, N.-H., Huang, Y.-S., Li, H.-Y., Chen, J.-Y., Lee, L.-A., & Huang, C.-G. (2020). Differences in Anthropometric and Clinical Features among Preschoolers, School-Age Children, and Adolescents with Obstructive Sleep Apnea—A Hospital-Based Study in Taiwan. International Journal of Environmental Research and Public Health, 17(13), 4663. https://doi.org/10.3390/ijerph17134663