Do Feelings of Defeat and Entrapment Change over Time? An Investigation of the Integrated Motivational—Volitional Model of Suicidal Behaviour Using Ecological Momentary Assessments

 and
and
Abstract
1. Introduction
2. Materials and Methods
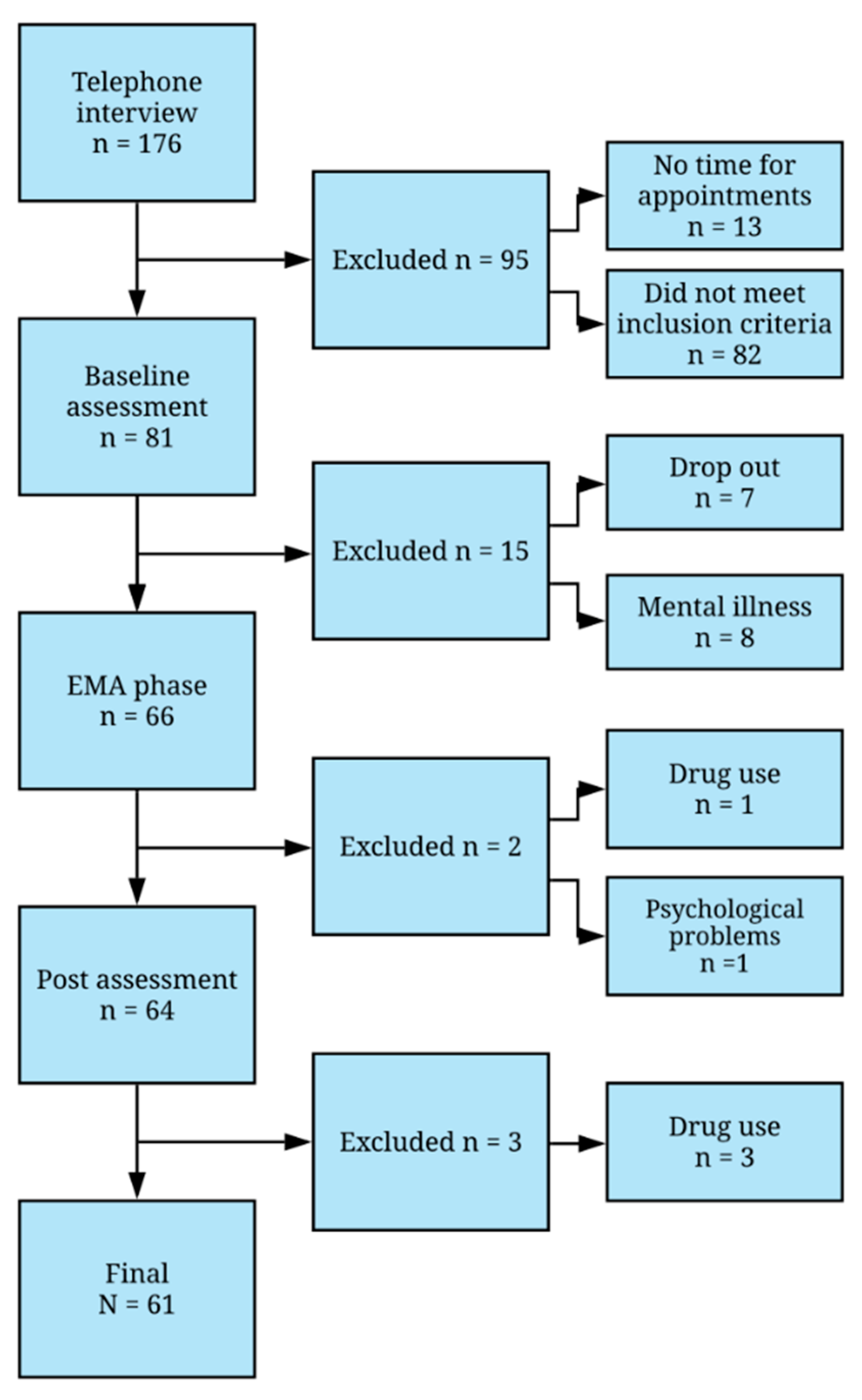
2.1. Sample
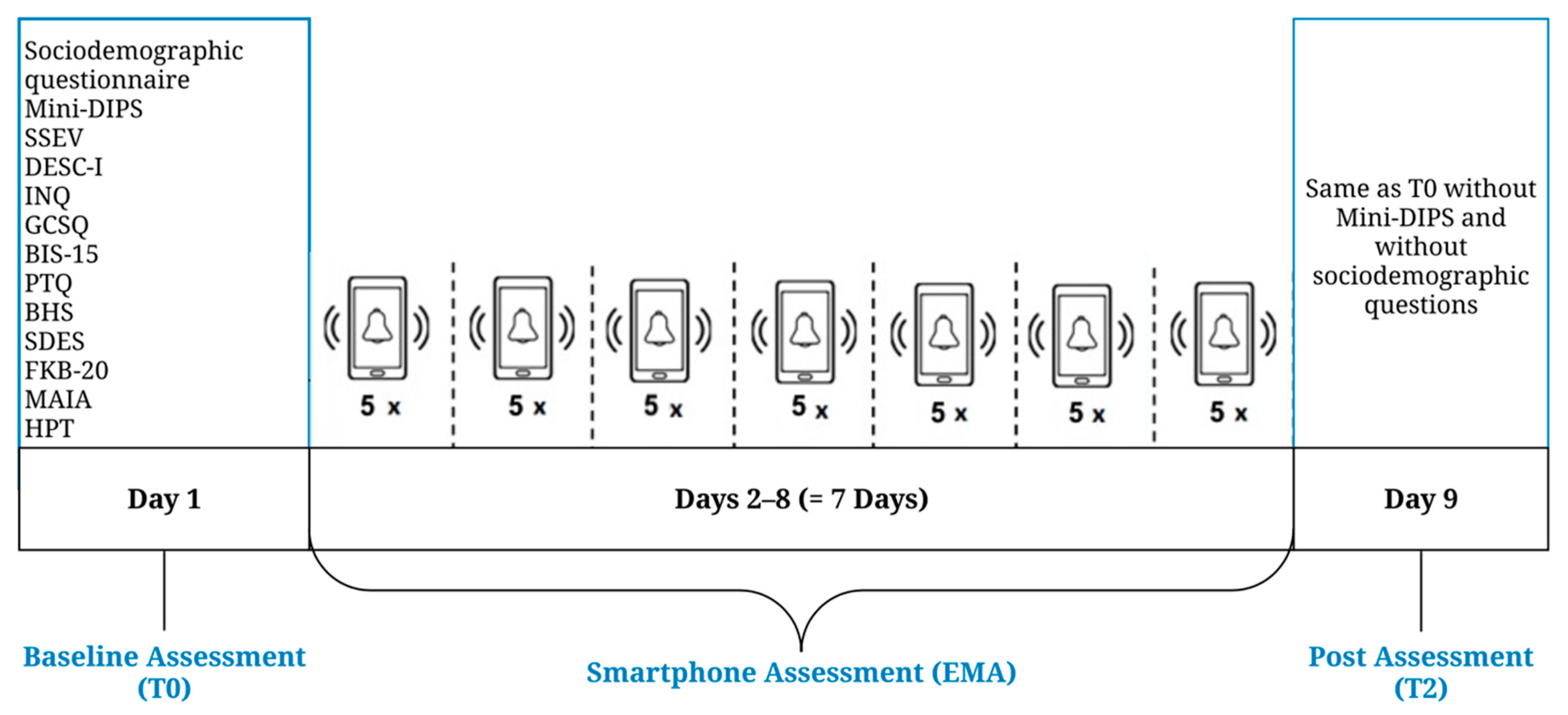
2.2. Measures and Procedure
2.2.1. Baseline Assessment (T0)
2.2.2. Ecological Momentary Assessment (EMA)
2.2.3. Post Assessment (T2)
2.3. Statistical Analysis
2.3.1. Variability of Defeat and Entrapment (Hypotheses 1a and 1b)
2.3.2. Relationship between Defeat and Entrapment According to the IMV Model (Hypotheses 2a and 2b)
3. Results
3.1. Variability of Defeat and Entrapment (Hypotheses 1a and 1b)
3.1.1. Variability of Defeat and Entrapment between Baseline and Post Assessment (Hypothesis 1a)
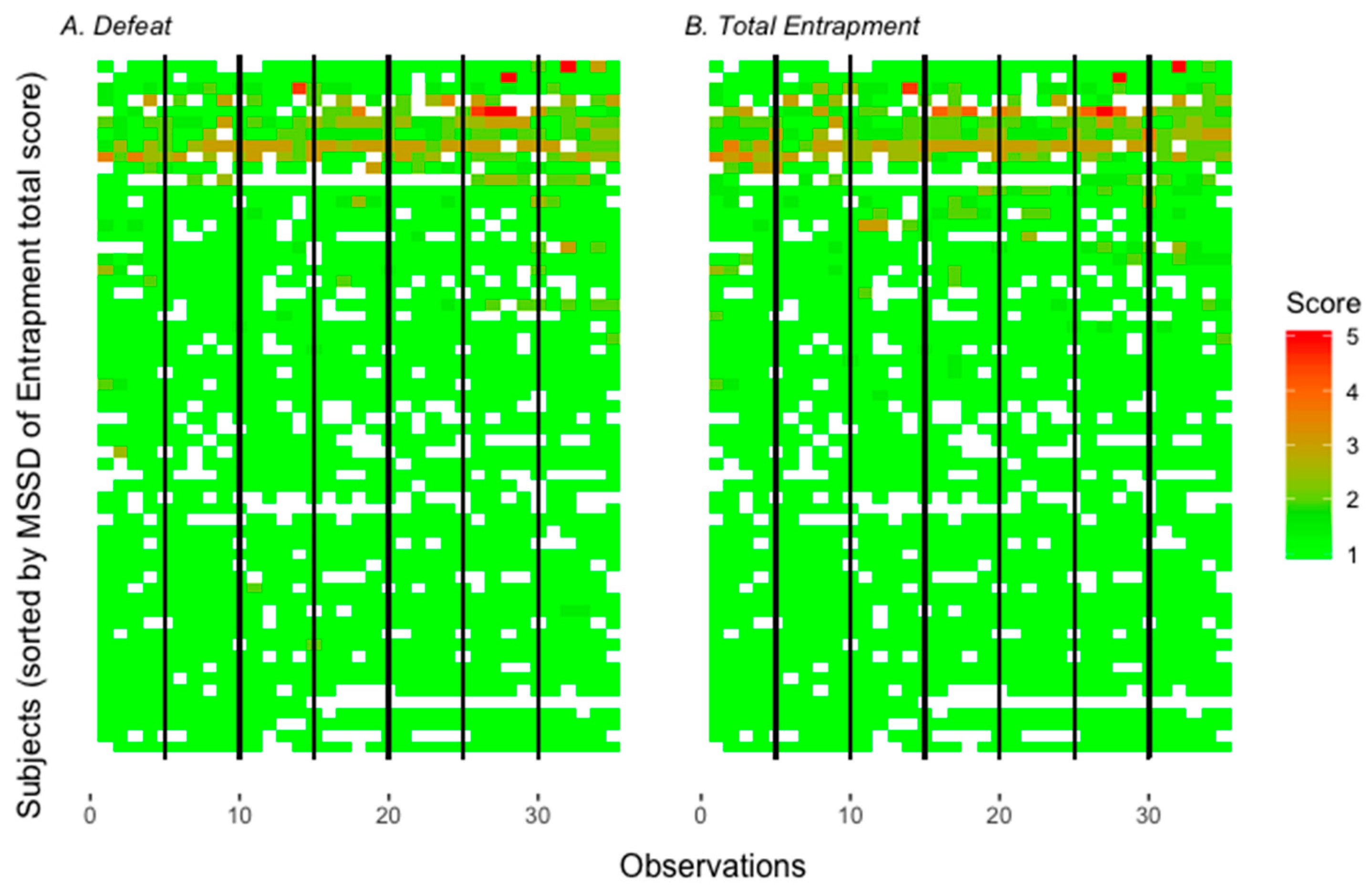
3.1.2. Variability of Defeat and Entrapment during EMA (Hypothesis 1b)
3.2. Relationship between Defeat and Entrapment According to the IMV Model (Hypotheses 2a and 2b)
4. Discussion
4.1. Variability of Defeat and Entrapment (Hypotheses 1a and 1b)
4.2. Relationship between Defeat and Entrapment According to the IMV Model (Hypotheses 2a and 2b)
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Preventing Suicide. A Global Imperative; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Nock, M.K.; Borges, G.; Ono, Y. Suicide. Global Perspectives from the WHO World Mental Health Survey; Cambridge University Press: Cambridge, UK, 2014. [Google Scholar]
- Forkmann, T.; Brähler, E.; Gauggel, S.; Glaesmer, H. Prevalence of Suicidal Ideation and Related Risk Factors in the German General Population. J. Nerv. Ment. Dis. 2012, 200, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Borges, G.; Bromet, E.J.; Cha, C.B.; Kessler, R.C.; Lee, S. Suicide and Suicidal Behavior. Epidemiol. Rev. 2008, 30, 133–154. [Google Scholar] [CrossRef]
- O’Connor, R.C. The Integrated Motivational-Volitional Model of Suicidal Behavior. Crisis 2011, 32, 295–298. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, R.; Kirtley, O. The integrated motivational-volitional model of suicidal behaviour. Philos. Trans. R. Soc. B 2018, 373, 20170268. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.M.G. Cry of Pain: Understanding Suicide and Self-Harm; Penguin Books: London, UK, 1997. [Google Scholar]
- Joiner, T. Why People Die by Suicide; Harvard University Press: Cambridge, MA, USA, 2005. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Wachtel, S.; Teismann, T. Die interpersonale Theorie suizidalen Verhaltens: Eine systematische Übersichtsarbeit [The interpersonal theory of suicidal behavior: A systematic review]. Z. Klin. Psychol. Psychother. 2013, 42, 96–106. [Google Scholar] [CrossRef]
- Teismann, T.; Forkmann, T. Rumination, Entrapment and Suicidal ideation: A Mediational Model. Clin. Psychol. Psychother. 2015, 24, 226–234. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Rasmussen, S.; Hawton, K. Distinguishing adolescents who think about self-harm from those who engage in self-harm. Br. J. Psychiatry 2012, 200, 330–335. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Smyth, R.; Ferguson, E.; Ryan, C.; Williams, J.M.G. Psychological processes and repeat suicidal behavior: A four-year prospective study. J. Consult. Clin. Psychol. 2013, 81, 1137–1143. [Google Scholar] [CrossRef]
- Siddaway, A.P.; Taylor, P.J.; Wood, A.M.; Schulz, J. A meta-analysis of perceptions of defeat and entrapment in depression, anxiety problems, posttraumatic stress disorder, and suicidality. J. Affect. Disord. 2015, 184, 149–159. [Google Scholar] [CrossRef]
- Gilbert, P.; Allan, S. The role of Defeat and Entrapment (arrested flight) in depression: An exploration of an evolutionary view. Psychol. Med. 1998, 28, 585–598. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.J.; Wood, A.M.; Gooding, P.; Tarrier, N. Are defeat and entrapment best defined as a single construct? Personal. Individ. Differ. 2009, 47, 795–797. [Google Scholar] [CrossRef]
- Sturman, E.D. Involuntary subordination and its relation to personality, mood, and submissive behavior. Psychol. Assess. 2011, 23, 262–276. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, A.W.; Wood, A.M.; Maltby, J.; Taylor, P.J.; Tai, S. The prospective role of defeat and entrapment and depression and anxiety: A 12-month longitudinal study. Psychiatry Res. 2014, 216, 52–59. [Google Scholar] [CrossRef]
- Griffiths, A.W.; Wood, A.M.; Maltby, J.; Taylor, P.J.; Panagioti, M.; Tai, S. The development of the Short Defeat and Entrapment Scale (SDES). Psychol. Assess. 2015, 27, 1182–1194. [Google Scholar] [CrossRef]
- Forkmann, T.; Teismann, T.; Stenzel, J.S.; Glaesmer, H.; de Beurs, D. Defeat and entrapment: More than meets the eye? Applying network analysis to estimate dimensions of highly correlated constructs. BMC Med. Res. Methodol. 2018, 18. [Google Scholar] [CrossRef]
- Taylor, P.; Gooding, P.; Wood, A.M.; Johnson, J.; Tarrier, N. Prospective Predictors of Suicidality: Defeat and Entrapment lead to changes of suicidal ideation over time. Suicide Life Threat. Behav. 2011, 41, 297–306. [Google Scholar] [CrossRef]
- Cloos, M.; Di Simplicio, M.; Hammerle, F.; Steil, R. Mental images, entrapment and affect in young adults meeting criteria of nonsuicidal self-injury disorder (NSSID)—A daily diary study. Bord. Personal. Disord. Emot. Dysregul. 2020, 7. [Google Scholar] [CrossRef]
- Wetherall, K.; Robb, K.A.; O’Connor, R.C. An Examination of Social Comparison and Suicidal ideation Through the Lens of the Integrated Motivational-Volitional Model of Suicidal Behavior. Suicide Life Threat. Behav. 2018, 49, 167–182. [Google Scholar] [CrossRef]
- Schiffman, S.; Stone, A.A.; Hufford, M.R. Ecological momentary assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef]
- Forkmann, T.; Spangenberg, L.; Rath, D.; Hallensleben, N.; Hegerl, U.; Kersting, A.; Glaesmer, H. Assessing Suicidality in Real Time: A Psychometric Evaluation of Self-Report Items for the Assessment of Suicidal Ideation and Its Proximal Risk Factors Using Ecological Momentary Assessments. J. Abnorm. Psychol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, S.J.W.; Hasmi, L.; Drukker, M.; van Os, J.; Delespaul, P.A.E.G. Use of the experience sampling method in the context of clinical trials. Evid. Based. Ment. Health 2016, 19, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, P.; Ebner-Priemer, U.; Trull, T.J. Experience sampling methods in clinical psychology. In The Oxford Handbook of Res.earch Strategies for Clinical Psychology; Comer, J., Kendall, P., Eds.; Oxford University Press: Oxford, UK, 2013; pp. 188–210. [Google Scholar]
- DeCou, C.R.; Schumann, M.E. On the latrogenic risk of Assessing Suicidality: A Meta-Analysis. Suicide Life Threat. Behav. 2017, 48, 531–543. [Google Scholar] [CrossRef]
- Franklin, J.C.; Ribeiro, J.D.; Fox, K.R.; Bentley, K.H.; Kleinman, E.M.; Huang, X.; Musaccio, K.M.; Jaroszewski, A.C.; Chang, B.P.; Nock, M.K. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychol. Bull. 2017, 143, 187–232. [Google Scholar] [CrossRef] [PubMed]
- De Beurs, D.; Kirtley, O.; Kerkhof, A.; Portzky, G.; ‚O’Connor, R.C. The Role of Mobile Phone Technology in Understanding and Preventing Suicidal Behavior. Crisis 2015, 36, 79–82. [Google Scholar] [CrossRef]
- Spangenberg, L.; Forkmann, T.; Glaesmer, H. Investigating dynamics and predictors of suicidal behaviors using ambulatory assessment. Neuropsychiatrie 2015, 29, 139–143. [Google Scholar] [CrossRef]
- Hallensleben, N.; Spangenberg, L.; Forkmann, T.; Rath, D.; Hegerl, U.; Kersting, A.; Kallert, T.W.; Glaesmer, H. Investigating the Dynamics of Suicidal Ideation. Crisis 2018, 39, 65–69. [Google Scholar] [CrossRef]
- Kleiman, E.M.; Turner, B.J.; Fedor, S.; Beale, E.E.; Huffman, J.C.; Nock, M.K. Examination of real-time fluctuations in suicidal ideation and its risk factors: Results from two ecological momentary assessment studies. J. Abnorm. Psychol. 2017, 126, 726–738. [Google Scholar] [CrossRef]
- Hallensleben, N.; Glaesmer, H.; Forkmann, T.; Rath, D.; Strauss, M.; Kerting, A.; Spangenberg, L. Predicting suicidal ideation by interpersonal variables, hopelessness and depression in real-time. An ecological momentary assessment study in psychiatric inpatients with depression. Eur. Psychiatry 2019, 56, 43–50. [Google Scholar] [CrossRef]
- Walz, L.C.; Nata, M.H.; Aan Het Rot, M. Experience sampling and ecological momentary assessment for studying the daily lives of patients with anxiety disorders: A systematic review. J. Anxiety Disord. 2014, 28, 925–937. [Google Scholar] [CrossRef]
- Spangenberg, L.; Glaesmer, H.; Hallensleben, N.; Rath, D.; Forkmann, T. (In)stability of capability for suicide in psychiatric inpatients—Longitudinal assessment using ecological momentary assessments. Suicide Life Threat. Behav. 2019. [Google Scholar] [CrossRef] [PubMed]
- Margraf, J.; Cwik, J.C.; Pflug, V.; Schneider, S. Structured clinical interviews for mental disorders across the lifespan: Psychometric quality and further developments of the DIPS Open Access interviews. [Strukturierte klinische Interviews zur Erfassung psychischer Störungen über die Lebensspanne: Gütekriterien und Weiterentwicklungen der DIPS-Verfahren.]. Z. Klin. Psychol. Psychother. (Gott) 2017, 46. [Google Scholar] [CrossRef]
- Margraf, J.; Cwik, J.C. Mini-DIPS Open Access: Diagnostisches Kurzinterview bei Psychischen Störungen; Forschungs- und Behandlungszentrum für psychische Gesundheit, Ruhr-Universität Bochum: Bochum, Germany, 2017. [Google Scholar] [CrossRef]
- Höller, I.; Stenzel, J.S.; Rath, D.; Forkmann, T. Listen to your heart—Ecological Momentary Assessment of Interoceptive Accuracy. Aware. Sensib. submitted.
- Herbert, B.M.; Muth, E.R.; Pollatos, O.; Herbert, C. Interoception across Modalities: On the Relationship between Cardiac Awareness and the Sensitivity for Gastric Functions. PLoS ONE 2012. [Google Scholar] [CrossRef] [PubMed]
- World Medical Associatiton. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull. World Health Organ. 2001, 79, 373. [Google Scholar]
- Teismann, T.; Forkmann, T.; Glaesmer, H.; Juckel, G.; Cwik, J. Skala Suizidales Erleben und Verhalten (SSEV). Faktorstruktur und psychometrische Eigenschaften. submitted.
- Forkmann, T.; Boecker, M.; Wirtz, M.; Glaesmer, H.; Braehler, E.; Norra, C.; Gauggel, S. Validation of the Rasch-based Depression Screening in a large scale German general population sample. Health Qual. Life Outcomes 2010, 8. [Google Scholar] [CrossRef]
- Forkmann, T.; Boecker, M.; Wirtz, M.; Eberle, N.; Westhofen, M.; Schauerte, P.; Mischke, K.; Kircher, T.; Gauggel, S.; Norra, C. Development and validation of the Rasch-based Depression Screening (DESC) using Rasch-based analysis and structural equation modelling. J. Behav. Ther. Exp. Psychiatry 2009, 40, 468–478. [Google Scholar] [CrossRef]
- Van Orden, K.A.; Cukrowicz, K.C.; Witte, T.K.; Joiner, T.E. Thwarted belongingness and perceived burdensomeness: Construct validity and psychometric properties of the Interpersonal Needs Questionnaire. Psychol. Assess. 2012, 24, 197–215. [Google Scholar] [CrossRef]
- Glaesmer, H.; Spangenberg, L.; Scherer, A.; Forkmann, T. Die Erfassung von Suizidwünschen: Erste psychometrische Befunde zur deutschen Version des Interpersonal Needs Questionnaire (INQ). Psychiatr. Prax. 2014, 41, 250–256. [Google Scholar] [CrossRef]
- Wachtel, S.; Vocks, S.; Edel, M.-A.; Nyhuis, P.; Willutzki, U.; Teismann, T. Validation and psychometric properties of the German capability for suicide questionnaire. Compr. Psychiatry 2014, 55, 1292–1302. [Google Scholar] [CrossRef] [PubMed]
- Spinella, M. Normative data and a short form of the Barratt Impulsiveness Scale. Int. J. Neurosci. 2007, 117, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Meule, A.; Claus, V.; Kübler, A. Psychometric evaluation of the German Barratt Impulsiveness Scale—Short Version (BIS-15). Diagnostica 2011, 57, 126–133. [Google Scholar] [CrossRef]
- Ehring, T.; Zetsche, U.; Weidacker, K.; Wahl, K.; Schönfeld, S.; Ehlers, A. The Perseverative Thinking Questionnaire (PTQ): Validation of a content-independent measure of repetitive negative thinking. J. Behav. Ther. Exp. Psychiatry 2011, 42, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Weissman, A.; Lester, D.; Trexler, L. The measurement of pessimism: The hopelessness scale. J. Consult. Clin. Psychol. 1974, 42, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Kliem, S.; Brähler, E. Beck Hoffnungslosigkeits-Skala [Beck Hopelessness Scale]; Hogrefe: Göttingen, Germany, 2016. [Google Scholar]
- Clement, U.; Löwe, B. Die Validierung des FKB-20 als Instrument zur Erfassung von Körperbildstörungen bei psychosomatischen Patienten. Psychother. Psychosom. Med. Psychol. 1996, 46, 254–259. [Google Scholar]
- Mehling, W.E.; Price, C.; Daubenmier, J.J.; Acree, M.; Bartmess, E.; Stewart, A. The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS ONE 2012, 7, e48230. [Google Scholar] [CrossRef]
- Bornemann, B.; Mehling, W. Multidimensional Assessment of Interoceptive Awareness (MAIA). German Translation, 2012. Available online: https://osher.ucsf.edu/sites/osher.ucsf.edu/files/inline-files/MAIAGerman.pdf (accessed on 25 May 2020).
- Schandry, R. Heartbeat perception and Emotional Experience. Psychophysiology 1981, 18, 483–488. [Google Scholar] [CrossRef]
- Höller, I.; Teismann, T.; Cwik, J.C.; Glaesmer, H.; Spangenberg, L.; Hallensleben, N.; Paashaus, L.; Rath, D.; Schönfelder, A.; Juckel, G.; et al. Short Defeat and Entrapment scale: A psychometric investigation in three German samples. Compr. Psychiatry 2020, 98, 152160. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Taylor and Francis: Hboken, NJ, USA, 1988. [Google Scholar]
- Forkmann, T.; Stenzel, J.-S.; Rath, D.; Glaesmer, H.; Teismann, T. Vom Leben geschlagen—Valdierung der deutschen Version der Defeat Scale (DS-d). Psychother. Psychosom. Med. Psychol. 2018, 68. [Google Scholar] [CrossRef]
- Trachsel, M.; Krieger, T.; Gilbert, P.; Grosse Holtforth, M. Testing a German Adaption of the Entrapment Scale and Assessing the Relation to Depression. Depress. Res. Treat. 2010. [Google Scholar] [CrossRef] [PubMed]
- Kleiman, E.M. Power Curves for Multi-Level Studies. Available online: https://ekleiman.shinyapps.io/powercurves (accessed on 22 March 2020).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 22 March 2020).
- Fox, J.; Weisberg, S. An {R} Companion to Applied Regression, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2019. [Google Scholar]
- Bates, D.; Maechler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. lmerTest Package: Tests in Linear Mixed Effects Models. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar] [CrossRef]
- Hox, J.H. Multilevel Analysis: Techniques and Application, 2nd ed.; Routledge: New York, NY, USA, 2010. [Google Scholar]
- Woyshville, M.J.; Lackamp, J.M.; Eisengart, J.A.; Gilliiland, J.A. On the meaning and measurement of affective instability: Clues from chaos theory. Biol. Psychiatry 1999, 45, 261–269. [Google Scholar] [CrossRef]
- Revelle, W. Psych: Procedures for Personality and Psychological Research, 1.8.12 ed.; Northwestern University: Evanston, IL, USA, 2018; Available online: https://CRAN.R-project.org/package=psych (accessed on 22 March 2020).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Hox, J. Multilevel modeling: When and why. In Classification, Data Analysis and Data Highways; Balderjahn, I., Mathar, R., Schader, M., Eds.; Springer: New York, NY, USA, 1998; pp. 147–154. [Google Scholar]
- Raudenbush, S.W.; Bryk, A.S. Hierarchical Linear Models, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Hayes, A.F. A primer on multilevel modeling. Hum. Commun. Res. 2006, 32, 385–410. [Google Scholar] [CrossRef]
- Enders, C.K.; Tofighi, D. Centering predictor variables in cross-sectional multilevel models: A new look at an old issue. Psychol. Methods 2007, 12, 121–138. [Google Scholar] [CrossRef]
- Snijders, T.A.B.; Bosker, R.J. Multilevel Analysis. An Introduction to Basic and Advanced Multilevel Modeling, 2nd ed.; SAGE Publications Ltd.: London, UK, 2011. [Google Scholar]
- Anderson, D. Hierarchical Linear Modeling (HLM): An Introduction to Key Concepts within Cross-Sectional and Growth Modeling Frameworks, Technical Report #1308; Behavioral Research and Teaching, University of Oregon: Eugene, OR, USA, 2012. [Google Scholar]
- O’Connor, R.C. Suicidal Behaviour as a Cry of Pain: Test of a Psychological Model. Arch. Suicide Res. 2003, 7, 297–308. [Google Scholar] [CrossRef]
- Rogers, M.L.; Stanley, I.H.; Hom, M.A.; Chiurliza, B.; Podlogar, M.C.; Joiner, T.E. Conceptual and empirical scrutiny of covarying depression out of suicidal ideation. Assessment 2018, 25, 159–172. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| M | SD | Range | M MSSD | SD MSSD | Min MSSD | Max MSSD | ICC | ||
|---|---|---|---|---|---|---|---|---|---|
| Min | Max | ||||||||
| Defeat | 1.15 | 0.47 | 1 | 5 | 0.13 | 0.27 | 0 | 1.40 | 0.52 |
| Item 1 | 1.17 | 0.53 | 1 | 5 | 0.19 | 0.35 | 0 | 1.60 | 0.49 |
| Item 2 | 1.13 | 0.47 | 1 | 5 | 0.13 | 0.28 | 0 | 1.33 | 0.46 |
| Entrapment | 1.17 | 0.49 | 1 | 5 | 0.13 | 0.27 | 0 | 1.14 | 0.54 |
| Item 1 | 1.14 | 0.49 | 1 | 5 | 0.16 | 0.35 | 0 | 1.51 | 0.46 |
| Item 2 | 1.20 | 0.56 | 1 | 5 | 0.18 | 0.28 | 0 | 1.45 | 0.52 |
| Model | Fixed Effects | Random Effects | Deviance | |||||
|---|---|---|---|---|---|---|---|---|
| Predictors | Est. | 95% CI (Est.) | SE | t(df) | p | Slopes >0 1 | Variance | |
| Model 2—Random Slopes | 153.97 | |||||||
| Intercept | 1.17 | 0.05 | 25.07 (60) | <0.001 | 0.13 | |||
| Defeat | 0.52 | −0.2–1.24 | 0.08 | 6.71 (60) | <0.001 | 92.22% | 0.13 | |
| Deviance test 2: x2(2) = 92.66, p < 0.001 Quasi R2: Predictors of model 2 account for 51.81% of residual variance in entrapment at level 1 3 | ||||||||
| Model 4—Random Slopes | 965.97 | |||||||
| Intercept | 1.17 | 0.05 | 24.74 (60) | <0.001 | 0.13 | |||
| Defeat (t − 1) | 0.08 | −0.37–0.53 | 0.06 | 1.30 (60) | 0.20 | 63.68% | 0.05 | |
| Deviance test 2: x2(2) = 80.62, p < 0.001 Quasi R2: Predictors of model 4 account for 1.46% of residual variance in entrapment at level 1 3 | ||||||||
| Model 6—Random Slopes | 883.73 | |||||||
| Intercept | 1.17 | 0.05 | 24.73 (60) | <0.001 | 0.13 | |||
| Defeat (t − 1) | −0.02 | −0.32–0.28 | 0.05 | −0.41 (60) | 0.68 | 44.83% | 0.02 | |
| Entrapment (t − 1) | 0.25 | −0.33–0.83 | 0.08 | 3.26 (60) | 0.002 | 79.95% | 0.09 | |
| Deviance test 2: x2(2) = 137.02, p < 0.001 Quasi R2: Predictors of model 6 account for 10.2% of residual variance in entrapment at level 1 3 | ||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stenzel, J.-S.; Höller, I.; Rath, D.; Hallensleben, N.; Spangenberg, L.; Glaesmer, H.; Forkmann, T. Do Feelings of Defeat and Entrapment Change over Time? An Investigation of the Integrated Motivational—Volitional Model of Suicidal Behaviour Using Ecological Momentary Assessments. Int. J. Environ. Res. Public Health 2020, 17, 4685. https://doi.org/10.3390/ijerph17134685
Stenzel J-S, Höller I, Rath D, Hallensleben N, Spangenberg L, Glaesmer H, Forkmann T. Do Feelings of Defeat and Entrapment Change over Time? An Investigation of the Integrated Motivational—Volitional Model of Suicidal Behaviour Using Ecological Momentary Assessments. International Journal of Environmental Research and Public Health. 2020; 17(13):4685. https://doi.org/10.3390/ijerph17134685
Chicago/Turabian StyleStenzel, Jana-Sophie, Inken Höller, Dajana Rath, Nina Hallensleben, Lena Spangenberg, Heide Glaesmer, and Thomas Forkmann. 2020. "Do Feelings of Defeat and Entrapment Change over Time? An Investigation of the Integrated Motivational—Volitional Model of Suicidal Behaviour Using Ecological Momentary Assessments" International Journal of Environmental Research and Public Health 17, no. 13: 4685. https://doi.org/10.3390/ijerph17134685
APA StyleStenzel, J.-S., Höller, I., Rath, D., Hallensleben, N., Spangenberg, L., Glaesmer, H., & Forkmann, T. (2020). Do Feelings of Defeat and Entrapment Change over Time? An Investigation of the Integrated Motivational—Volitional Model of Suicidal Behaviour Using Ecological Momentary Assessments. International Journal of Environmental Research and Public Health, 17(13), 4685. https://doi.org/10.3390/ijerph17134685