The Impact of a Dementia-Friendly Exercise Class on People Living with Dementia: A Mixed-Methods Study

 ,
, 
Abstract
1. Introduction
- Assess the impact of an exercise class on mobility, muscle strength, physical activity levels, independence, loneliness, mood, and quality of life for people with dementia and their carers.
- Investigate the perception of the impact of an exercise group from the perspective of people with dementia and their carers.
- Map the key components related to impact and participation of the exercise classes on people with dementia and their carers.
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Setting
2.4. Procedures
2.4.1. Repeated Measures Cohort
- (a)
- (b)
- Muscle Strength: hand held dynamometer [16]
- (c)
- Cognition: Hopkins Verbal Learning Test (HVLT) [17]
- (d)
- Physical activity levels: LASA Physical Activity Questionnaire (LAPAQ) [18]
- (e)
- Independence: Nottingham Extended ADL Scale (NEADL) [19]
- (f)
- Loneliness: UCLA Loneliness Scale [20]
- (g)
- Mood: Hospital Anxiety and Depression Scale (HADS) [21]
- (h)
- Quality of Life: Dementia Quality of Life Scale (DemQoL) [22]
2.4.2. Focus Groups
2.5. Data Analysis
2.5.1. Repeated Measures Cohort
2.5.2. Focus Groups
3. Results
3.1. Repeated Measures Cohort
3.2. Focus Group
Description of Sample
3.3. Themes
3.3.1. Benefits to Person with Dementia
Well I think it’s kept my mum continue to be mobile……..she can still go upstairs. So I don’t have to do anything for her. She gets dressed and undressed. So she’s still got muscle strength. So perhaps that would have deteriorated if she hadn’t been coming to the classes.(FG1 P1)
It’s almost like building up a bank of things…..You pick your activity just like you or I would do it. You wake up one day, you feel like doing something or you don’t. And it’s just to have the option of different things I think.(FG2 P3)
We try everything……I say….we’re going to go here, if you don’t like it we won’t go again, simple as that. That’s all you can do, but you’ve just got to give it a go, because what suits one doesn’t suit another does it?(FG2 P3)
3.3.2. Benefits to Carer
The things I’ve picked up have been so good. And the people we’ve got to know, you get really friendly with people in a short time, because you’re in a mess together, and you pick brains. And one of the guys told us about, he just said are you aware that you can get money back if you’ve altered powers of attorney?(FG2 P5)
Look here, we’ve met these lovely people I never want to be without.(FG2 P1)
Well the support, the people’s experience and their knowledge….the little bits of information that we got, I felt quite desperate to start with, what are we going to do? I’m always picking up on what people say.(FG2 P5)
Well getting out the house for a start. Sort of, I don’t know, the older you get you can’t be bothered to go out(FG1 P1)
Well it’s mixing with other people basically……. and we have a lot of fun.(FG2 P6)
3.3.3. Environmental Characteristics
I was a bit worried for quite a while about the parking, because I couldn’t make out where we would park. Anyway…….there is parking…….(FG1 P3)
There’s loads of toilets. And there’s disabled toilets. So I don’t think they’re lacking in anything are they really?(FG1 P1)
So to be able to extend it and know that John will have a lovely chat with his friends as well that just makes the whole experience last longer in my view.(FG2 P3)
They’ve just got so much confidence. They seem to know what they’re doing. And he enjoys it far more when he’s with somebody else than me.(FG2 P3)
I wouldn’t think of taking my mum to any exercise class unless it said it was specifically for dementia………you’d know that the people doing it would know about dementia and all what happens to people when they’ve got dementia and the different kinds and…. they’d know what to do(FG1 P1)
3.3.4. Exercise Class Characteristics
Well it said it was dementia friendly so I just assumed it would be……I hadn’t really wanted to go to things that people said oh it might have been with dementia and their partners, it just didn’t seem to appeal to me much. So I wasn’t very motivated to go to any of that, but I thought well an exercise class, anyone can do that. I’ll enjoy doing that as well.(FG1 P3)
I wouldn’t think of taking my mum to any exercise class unless it said it was specifically for dementia.(FG1 P1)
Forget me Nots does…..walking football, so we can do that once a month. But once a month, it’s not enough(FG2 P3)
And it’s nice the once a week as well, because a lot of things are only once every three weeks or four weeks. To have this nearly every week, and it’s just awesome.(FG2 P3)
It’s just the whole package. You can do as much or as little as you like. You can see that it’s got so much mileage in the class, because even if either you deteriorate or you’re not feeling great, you can just do whatever you want to do. It’s adaptable. And you know what, even if you do very little it’s still a social thing.(FG2 P1)
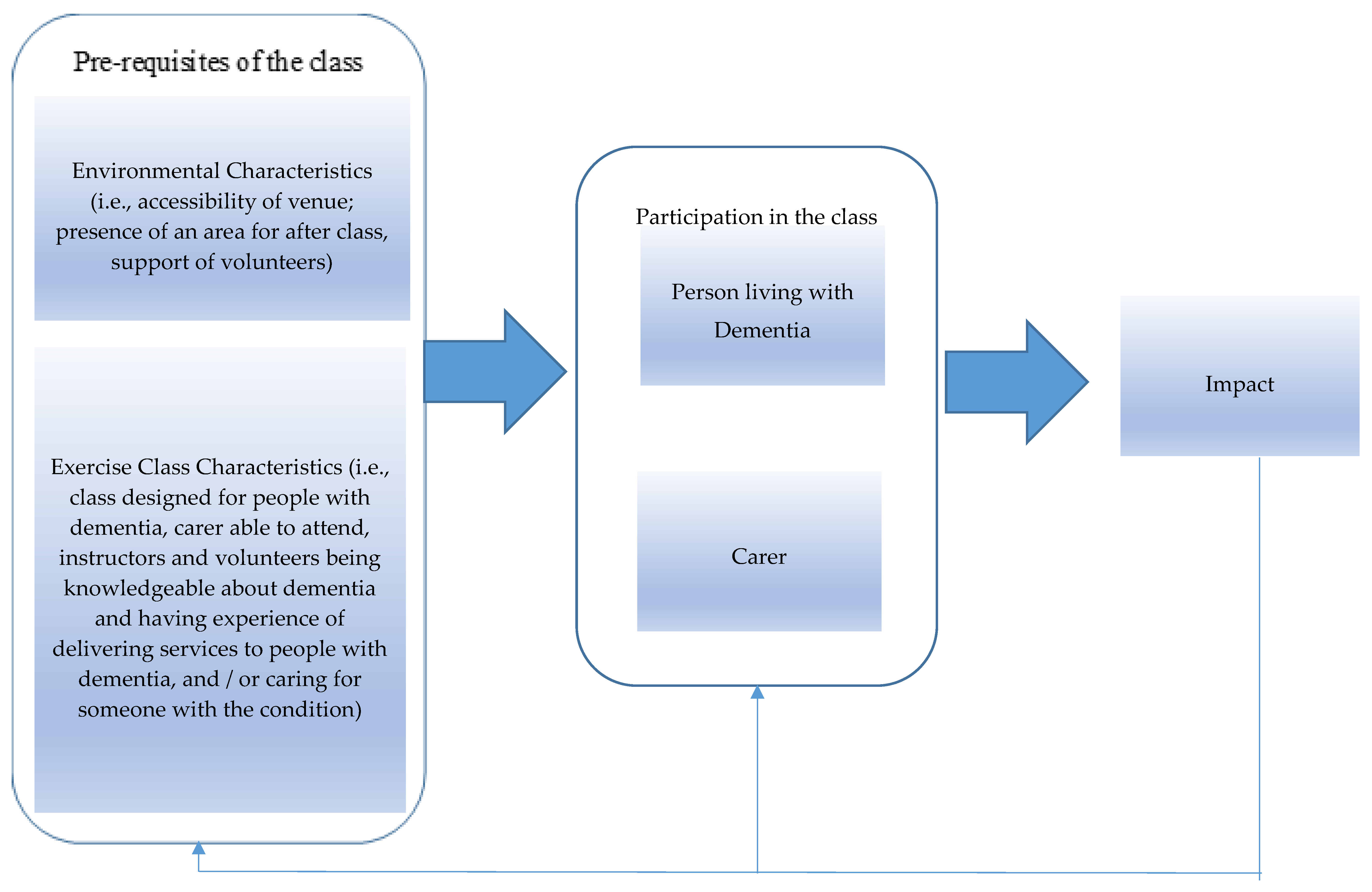
3.4. Exercise Class Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- Examples of Exercise Stations








Appendix B
- Focus Group Interview Schedule
- -
- What makes is suitable for you
- -
- Does is help that it is something that you could do together as opposed to something specifically for the person with dementia
- -
- Do you think that attending the class may help you progress back to things that you have had to stop doing?
- -
- What particularly are you enjoying about the exercise class?
- -
- Would it be helpful if the exercises changed every so often?
- -
- Specifically ask people with dementia what it is they enjoy (if they haven’t answered)
- -
- Do you tend to talk to the same people during the class?
- -
- Do you tend to go for coffee afterwards? If yes do you tend to talk to the same people then?
- -
- Do you find chatting to people afterwards useful/helpful?
- -
- Any further activities attended? Did they stem from attending this class?
- -
- Did attending this class give you more confidence to attend other activities/events? Why?
- -
- Do you think it would be useful for other people with dementia to have access to classes like this?
- -
- Would you attend a class for older people if it wasn’t marketed as dementia-friendly? If not, why not? Why is that important?
- -
- What makes it more comfortable for you to attend a class that is marketed/labelled as dementia friendly?
- -
- Do you think it is important that you could attend together?
- -
- Would you now feel more comfortable attending a class that wasn’t labelled as dementia friendly?
- -
- Has anything been useful with your day to day activities?
- -
- Do you think that there is a reason why those exercises haven’t transferred to everyday tasks?
- -
- If you could design at ideal class what would you put in place to enable people to attend
- -
- Is it helpful to have the extra staff/students to help with the class flow?
- -
- Why did having the University of Nottingham banding encourage you to attend the class
Appendix C

{kind=link}
| Code Book Code | Definition | Example of quotes |
|---|---|---|
| Able to attend together | Carer and person with dementia able to attend together | It would be something we could both enjoy. |
| Activity Transfer | Whether exercises were being transferred to everyday activities or not | I think the step, the one where you step up and down, I think that’s helpful to keep my mum going up and down the stairs, so that’s good. |
| Benefit of volunteers | Benefit of having extra volunteers for class | And the volunteers are wonderful. Of course. |
| Benefit of exercise | Benefits of exercise in general | Any amount of extra exercise is good for everybody. |
| Benefits of experience | Benefit of the overall experience of the class | It’s just the whole package really. |
| Changes in support network | Changes in support network since diagnosis | I’m amazed at some people we were very friendly with, we never see them, gone. |
| Class adaptable | Able to adapt exercises to own physical capability | You can do as much or as little as you like…it’s adaptable. |
| Coffee | Availability of coffee afterwards | We go for coffee afterwards to make the whole thing last a bit longer. |
| Continuing/Returning to previous activities | Whether exercise was helping people continue with previous activities or allowed them to return to activities they may have stopped | We’ve done this sort of thing, like waking for years and so on. And yeah so it’s carrying on. |
| Dealing with Diagnosis | Being able to deal with the specific diagnosis of dementia. | With the diagnosis it can be a relief. It was a relief. |
| Dementia Friendly Label | Class is specifically advertised as being for people living with dementia | I wouldn’t think of taking my mum to any class unless it said it was specifically for dementia. |
| Difficulties being a carer | Difficulties of caring for someone living with dementia | It’s so important for the carers as well as the people with the problem, and I do enjoy a bit of free time on my own. |
| Enjoyment of exercise | Enjoying the exercise itself | I quite like exercise |
| Environmental factors | Factors that were specific to this class environment | The space…and the light as well. |
| Fatigue | Lack of sleep and fatigue as a carer | And lack of sleep, it distorts everything. |
| Finding out useful information | Able to find out information on other classes/benefits/other groups from other attendees | It’s interesting what you find out as well from other people. |
| Frequency | Class happens weekly as opposed to fortnightly or monthly | To have this nearly every week it’s just awesome. |
| Getting out of the house | Being able to get out of the house | It’s getting out isn’t it? |
| Increasing activities | Exercises leading to a general increase in activity level | I walk more. |
| Increasing confidence | Increasing general levels of confidence | I just went to the lady that runs them and just said look, if it’s a problem just say. |
| Instructor knowledge and experience | The knowledge and experience of the instructor | Well the support, the people’s experience and their knowledge. |
| Interaction with others | Being able to see and chat to other people | Well it’s mixing with other people basically. |
| Keeping Moving | Generally keeping you moving | I think it’s kept my mum continue to be mobile. |
| Lack of other activities | Difficulties finding other activities to do together | We didn’t have a lot, mum wasn’t doing a lot. |
| Legitimacy of UoN Banding | Class is marketed as being at the University | The leaflet we were given originally because it said University of Nottingham that might have had an influence on why we came. |
| Level of facilities | The level of facilities available at this class | The quality of everything you’ve got. |
| Maintaining abilities | Maintenance of current functional abilities | Perhaps that would have deteriorated if she hadn’t been coming to the classes. |
| Parking | Availability of suitable parking | I was a bit worried for a while about the parking…..eventually Vicky did say there is parking. |
| Participation in other activities | Exercises led to participation in other activities elsewhere | There’s a singing class that we go to as well and another exercise class that Vicky has. |
| Preventing deterioration | Preventing a deterioration of current functional abilities | Whereas if we didn’t keep doing it he would probably deteriorate. |
| Supportive Community | People attending the group | We’ve met these lovely people I never want to be without. |
References
- Dowrick, A.; Southern, A. Dementia 2014: Opportunity for Change. 2014. Available online: https://www.alzheimers.org.uk/sites/default/files/migrate/downloads/dementia_2014_opportunity_for_change.pdf (accessed on 21 September 2019).
- Forbes, D.; Forbes, S.C.; Blake, C.M.; Thiessen, E.J.; Forbes, S. Exercise programs for people with dementia. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Chen, K.M.; Kuo, C.C.; Chang, Y.H.; Huang, H.T.; Cheng, Y.Y. Resistance Band Exercises Reduce Depression and Behavioral Problems of Wheelchair-Bound Older Adults with Dementia: A Cluster-Randomized Controlled Trial. J. Am. Geriatr. Soc. 2017, 65, 356–363. [Google Scholar] [CrossRef]
- Pitkälä, K.H.; Pöysti, M.M.; Laakkonen, M.L.; Tilvis, R.S.; Savikko, N.; Kautiainen, H.; Strandberg, T.E. Effects of the Finnish Alzheimer Disease Exercise Trial (FINALEX): A randomized controlled trial. JAMA Intern. Med. 2013, 173, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Vseteckova, J.; Deepak-Gopinath, M.; Borgstrom, E.; Holland, C.; Draper, J.; Pappas, Y.; McKeown, E.; Dadova, K.; Gray, S. Barriers and facilitators to adherence to group exercise in institutionalized older people living with dementia: A systematic review. Eur. Rev. Aging Phys. Act. 2018, 15, 11. [Google Scholar] [CrossRef] [PubMed]
- Estabrooks, P.A.; Carron, A.V. Group cohesion in older adult exercisers: Prediction and intervention effects. J. Behav. Med. 1999, 22, 575–588. [Google Scholar] [CrossRef] [PubMed]
- Costello, E.; Kafchinski, M.; Vrazel, J.; Sullivan, P. Motivators, barriers, and beliefs regarding physical activity in an older adult population. J. Geriatr. Phys. Ther. 2011, 34, 138–147. [Google Scholar] [CrossRef]
- Dickens, A.P.; Richards, S.H.; Greaves, C.J.; Campbell, J.L. Interventions targeting social isolation in older people: A systematic review. BMC Public Health 2011, 11, 647. [Google Scholar] [CrossRef]
- Bowes, A.; Dawson, A.; Jepson, R.; McCabe, L. Physical activity for people with dementia: A scoping study. BMC Geriatr. 2013, 13, 129. [Google Scholar] [CrossRef]
- Bajwa, R.K.; Goldberg, S.E.; Van der Wardt, V.; Burgon, C.; Di Lorito, C.; Godfrey, M.; Dunlop, M.; Logan, P.; Masud, T.; Gladman, J.; et al. A randomised controlled trial of an exercise intervention promoting activity, independence and stability in older adults with mild cognitive impairment and early dementia (PrAISED)—A Protocol. Trials 2019, 20, 1–11. [Google Scholar] [CrossRef]
- Moore Associates Physiotherapy Ltd. Dementia Friendly Exercise Class; University of Nottingham: Nottingham, UK, 2017. [Google Scholar]
- Clare, L. Rehabilitation for people living with dementia: A practical framework of positive support. PLoS Med. 2017, 14, e1002245. [Google Scholar] [CrossRef]
- Di Lorito, C.; Long, A.; Byrne, A.; Harwood, R.H.; Gladman, J.R.; Schneider, S.; Logan, P.; Bosco, A.; van der Wardt, V. Exercise interventions for older adults: A systematic review of meta-analyses. J. Sport Health Sci. 2020, (in press). [CrossRef] [PubMed]
- Berg, K.; Wood-Dauphine, S.; Williams, J.I.; Gayton, D. Measuring balance in the elderly: Preliminary development of an instrument. Physiother. Canada. 1989, 41, 304–311. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [PubMed]
- Abizanda, P.; Navarro, J.L.; García-Tomás, M.I.; López-Jiménez, E.; Martínez-Sánchez, E.; Paterna, G. Validity and usefulness of hand-held dynamometry for measuring muscle strength in community-dwelling older persons. Arch. Gerontol. Geriatr. 2012, 54, 21–27. [Google Scholar] [CrossRef]
- Brandt, J. The Hopkins Verbal Learning Test: Development of a new memory test with six equivalent forms. Clin. Neuropsychol. 1991, 5, 125–142. [Google Scholar] [CrossRef]
- Siebeling, L.; Wiebers, S.; Beem, L.; Puhan, M.A.; Ter Riet, G. Validity and reproducibility of a physical activity questionnaire for older adults: Questionnaire versus accelerometer for assessing physical activity in older adults. Clin. Epidemiol. 2012, 4, 171. [Google Scholar] [CrossRef]
- Nouri, F.M.; Lincoln, N.B. An extended activities of daily living scale for stroke patients. Clin. Rehabil. 1987, 1, 301–305. [Google Scholar] [CrossRef]
- Russell, D.W. UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. J. Personal. Assess. 1996, 66, 20–40. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Mulhern, B.; Rowen, D.; Brazier, J.; Smith, S.; Romeo, R.; Tait, R.; Watchurst, C.; Chua, K.C.; Loftus, V.; Young, T.; et al. Development of DEMQOL-U and DEMQOL-PROXY-U: Generation of preference-based indices from DEMQOL and DEMQOL-PROXY for use in economic evaluation. Health Technol. Assess. 2013, 17, 1–140. [Google Scholar] [CrossRef]
- Stewart, D.W.; Shamdasani, P.N. Focus Groups: Theory and Practice; Sage Publications: Thousand Oaks, CA, USA, 2014; Volume 20. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 24.0; IBM Corp: Chicago, IL, USA, 2016. [Google Scholar]
- NVivo. Nvivo 12 for Windows. NVivo Qualitative Data Analysis Software; QSR International Pty Ltd.: Daresbury, Cheshire, UK, 2018. [Google Scholar]
- Clarke, V.; Braun, V.; Weate, P. Using Thematic Analysis in Sport and Exercise Research. In Routledge Handbook of Qualitative Research in Sport and Exercise; Routledge: Danvers, MA, USA, 2016. [Google Scholar]
- Smith, R.; Drennan, V.; Mackenzie, A.; Greenwood, N. Volunteer peer support and befriending for carers of people living with dementia: An exploration of volunteers’ experiences. Health Soc. Care Community 2018, 26, 158–166. [Google Scholar] [CrossRef]
- Innes, A.; Page, S.J.; Cutler, C. Barriers to leisure participation for people with dementia and their carers: An exploratory analysis of carer and people with dementia’s experiences. Dementia 2016, 15, 1643–1665. [Google Scholar] [CrossRef]
- Spector, A.; Gardner, C.; Orrell, M. The impact of Cognitive Stimulation Therapy groups on people with dementia: Views from participants, their carers and group facilitators. Aging Ment. Health 2011, 15, 945–949. [Google Scholar] [CrossRef] [PubMed]
- Alzheimers Disease International. Principles of a Dementia Friendly Community. Dementia Friendly Communities. 2020. Available online: https://www.alz.co.uk/dementia-friendly-communities/principles (accessed on 16 June 2020).
- van der Wardt, V.; Hancox, J.; Pollock, K.; Logan, P.; Vedhara, K.; Harwood, R.H. Physical activity engagement strategies in people with mild cognitive impairment or dementia–a focus group study. Aging Ment. Health 2019, 1–8. [Google Scholar] [CrossRef]
- UK Active. Reimagining Ageing. 2018. Available online: https://www.ukactive.com/wp-content/uploads/2018/09/Reimagining_Ageing.pdf (accessed on 24 February 2020).
- Barnes, D.E.; Mehling, W.; Wu, E.; Beristianos, M.; Yaffe, K.; Skultety, K.; Chesney, M.A. Preventing loss of independence through exercise (PLIE): A pilot clinical trial in older adults with dementia. PLoS ONE 2015, 10, e0113367. [Google Scholar] [CrossRef]
- Lamb, S.E.; Sheehan, B.; Atherton, N.; Nichols, V.; Collins, H.; Mistry, D.; Dosanjh, S.; Slowther, A.M.; Khan, I.; Petrou, S.; et al. Dementia And Physical Activity (DAPA) trial of moderate to high intensity exercise training for people with dementia: Randomised controlled trial. BMJ 2018, 361, k1675. [Google Scholar] [CrossRef] [PubMed]
- Telenius, E.W.; Engedal, K.; Bergland, A. Inter-rater reliability of the Berg Balance Scale, 30 s chair stand test and 6 m walking test, and construct validity of the Berg Balance Scale in nursing home residents with mild-to-moderate dementia. BMJ Open 2015, 5, e008321. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Plano, C.; Vicki, L.; Gutmann, M.L.; Hanson, W.E. Advanced Mixed Methods Research Designs in Tashakkori, A. et Teddlie, C. (coord.). In Handbook of Mixed Methods in Social and Behavioral Research; Sage: Thousand Oaks, CA, USA, 2003; pp. 209–240. [Google Scholar]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed]
- IEtikan, I.; Musa, S.A.; Alkassim, R.S. Comparison of Convenience Sampling and Purposive Sampling. J. Theor. Appl. Stat. 2016, 5, 1–4. [Google Scholar] [CrossRef]
- Cations, M.; Laver, K.E.; Crotty, M.; Cameron, I.D. Rehabilitation in dementia care. Age Ageing 2018, 47, 171–174. [Google Scholar] [CrossRef]
- Ravn, M.B.; Petersen, K.S.; Thuesen, J. Rehabilitation for People Living with Dementia: A Scoping Review of Processes and Outcomes. J. Aging Res. 2019, 2019, 4141050. [Google Scholar] [CrossRef] [PubMed]

| Number | Percentage (%) | ||
|---|---|---|---|
| Gender | Male | 7 | 44 |
| Female | 9 | 56 | |
| Carer relationship | Spouse | 6 | 75 |
| Child | 2 | 25 | |
| Diagnosis | Alzheimer’s Disease | 5 | 62 |
| Vascular Dementia | 1 | 12 | |
| Parkinson’s Dementia | 1 | 12 | |
| Lewy Body Dementia | 1 | 12 | |
| Ethnicity | White-British | 16 | 100 |
| Outcome Measure | Baseline (n = 16) (mean ± SD) | Follow Up (n = 16) (mean ± SD) | Mean Difference [95% CI] |
|---|---|---|---|
| Cognition | |||
| HVLT Recall (/36) a | 15.63 ± 10.85 | 16.75 ± 11.48 | 1.13 [−2.74, 0.22] |
| HVLT Recognition (/12) a | 7.88 ± 4.94 | 7.94 ± 3.80 | 0.06 [−1.80, 1.67] |
| Quality of Life | |||
| DEMQoL (/116) a | 93.00 ± 10.33 | 92.00 ± 11.60 | −1.00 [−4.62, 6.62] |
| Mobility | |||
| TUG (secs) b | 9.72 ± 3.67 | 11.02 ± 8.44 | −1.29 [−5.28, 2.69] |
| Berg Balance (/56) a | 50.38 ± 6.29 | 49.13 ± 6.90 | −1.25 [−0.43, 2.93] |
| Strength | |||
| Grip Strength R (kg) a | 24.44 ± 6.76 | 24.15 ± 6.19 | −0.29 [−1.53, 2.11] |
| Grip Strength L (kg) a | 22.81 ± 5.48 | 23.69 ± 7.28 | 0.89 [−2.98, 1.21] |
| Independence | |||
| NEADL (/22) a | 14.31 ± 7.51 | 13.56 ± 8.30 | −0.75 [−06–1.56] |
| Mood | |||
| HADS (/42) b | 13.00 ± 6.69 | 11.67 ± 7.90 | 1.33 [−1.44, 4.11] |
| Physical Activity | |||
| LAPAQ (/MET hrs/wk) a | 45.42 ± 28.53 | 49.86 ± 41.03 | 4.44 [−23.03, 14.14] |
| Loneliness | |||
| UCLA Loneliness Scale (/80) b | 44.17 ± 10.45 | 42.42 ± 10.79 | 1.75 [−1.24, 4.74] |
| Pseudonym | Carer/PWD | Diagnosis | Gender |
|---|---|---|---|
| FG1 P1 | Carer | n/a | Female |
| FG1 P2 | PWD | Vascular Dementia | Female |
| FG1 P3 | Carer | n/a | Female |
| FG1 P4 | PWD | Alzheimer’s | Male |
| FG2 P1 | Carer | n/a | Female |
| FG2 P2 | PWD | Alzheimer’s | Male |
| FG2 P3 | Carer | n/a | Female |
| FG2 P4 | PWD | Alzheimer’s | Male |
| FG2 P5 | Carer | n/a | Male |
| FG2 P6 | PWD | Alzheimer’s | Female |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Long, A.; Di Lorito, C.; Logan, P.; Booth, V.; Howe, L.; Hood-Moore, V.; van der Wardt, V. The Impact of a Dementia-Friendly Exercise Class on People Living with Dementia: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2020, 17, 4562. https://doi.org/10.3390/ijerph17124562
Long A, Di Lorito C, Logan P, Booth V, Howe L, Hood-Moore V, van der Wardt V. The Impact of a Dementia-Friendly Exercise Class on People Living with Dementia: A Mixed-Methods Study. International Journal of Environmental Research and Public Health. 2020; 17(12):4562. https://doi.org/10.3390/ijerph17124562
Chicago/Turabian StyleLong, Annabelle, Claudio Di Lorito, Pip Logan, Vicky Booth, Louise Howe, Vicky Hood-Moore, and Veronika van der Wardt. 2020. "The Impact of a Dementia-Friendly Exercise Class on People Living with Dementia: A Mixed-Methods Study" International Journal of Environmental Research and Public Health 17, no. 12: 4562. https://doi.org/10.3390/ijerph17124562
APA StyleLong, A., Di Lorito, C., Logan, P., Booth, V., Howe, L., Hood-Moore, V., & van der Wardt, V. (2020). The Impact of a Dementia-Friendly Exercise Class on People Living with Dementia: A Mixed-Methods Study. International Journal of Environmental Research and Public Health, 17(12), 4562. https://doi.org/10.3390/ijerph17124562