Children Witnessing Domestic Violence in the Voice of Health and Social Professionals Dealing with Contrasting Gender Violence

 ,
,  ,
,  and
and 
Abstract
1. Introduction
1.1. Literature Review
1.1.1. Witnessing Domestic Violence (WDV): Consequences for Children
“Effective co-operation between all relevant state agencies, including the judiciary, public prosecutors, law enforcement agencies, local and regional authorities as well as non-governmental organizations and other relevant organizations and entities, in protecting and supporting victims and witnesses of all forms of violence”.(p. 31)
1.1.2. Taking Care of Children Witnessing Violence: Challenges and Obstacles
1.2. The Research
2. Materials and Methods
2.1. Aims
2.2. Participants
Ethical Issues
2.3. Procedures and Methodology
3. Results
3.1. WDV in the Experience of Health and Welfare Professionals
“If you ask a child who grew up in a violent family why he slapped his classmate or why his father spat in his face in a moment of anger, he answers ‘I don’t know’, because it’s like asking the reason for something that is done ‘automatically’, because it is always done in this way, there are no explicit explanations”.(Psychotherapist and Technical Office Consultant, Court of Naples and private specialist, M, 70 years old)
“They become the parents. They become the ones who protect the mother, the ones who distract the father, because they have learned to read the moment when the tension breaks out”.(Psychotherapist and Technical Office Consultant, Court of Naples and private specialist, M, 70 years old)
“… children don’t love dad or mom. Children love the couple. When the couple breaks up something in the children broke”.(Psychotherapist and Technical Office Consultant, Court of Naples and private specialist, M, 70 years old)
“They (children) often reported nightmares in which they dreamed of the father who removed them from their mother and wanted to kidnap them. Much younger children reported having dreamed of monsters, or they recurred in graphic production and drawings. Moreover, children talked about the classic stress symptoms, such as bedwetting, lack of appetite, difficulty eating, or difficulty concentrating in school, recreational activities, the continuous request for protection from the other parent”.(Social Worker, Minor and Family Service, F, 44 years old)
“And they worry about the mother, because they are afraid of the blood, of the wounds and of the threats, of the shouting etc., and the fear above all. They are children who are very scared [...] so when I comfort them, I hug them, they are also a little wary of this, however, they are children who suffer a lot”.(Social Worker, Minor and Family Service, F, 44 years old)
“Children are present and they are also very guilty of this thing, because maybe they feel guilty about this phenomenon, because they cannot understand the dynamics. They often become the cause of the quarrel, because going out with a child, or having accompanied him to school, can unleash jealousy etc.”.(Emergency Surgeon, ASL, F, 55 years old)
“Even young boys are always told ’boys don’t cry or don’t act like a girl!”.(Psychotherapist, ASL, F, 65 years old)
“My father always asked me to prepare the table for meals and when I rebelled and I asked why me and never my brother, he said it was not a man thing!”.(Psychotherapist, ASL, F, 65 years old)
3.2. Psychological and Behavioural Effects of Witnessing Violence on Children
“They are children who certainly show great suffering, or closing up, and therefore, in practice they are extremely rejecting towards the outside world; they begin to give signals at school and very often it is the school that practically realizes, and brings attention to this behavior. Children carry out violent actions against their siblings or their reference companions. With parents they tend to be children who appear very split in behavior; they collude with one or the other parent and often they tend to please the stronger parent, because they are obviously afraid, especially in cases of witnessing violence”.(Social Worker, Minor and Family Service, F, 44 years old)
“What terrifies them most? Change. Seeing, perceiving that an atmosphere has changed, that there are no longer the well-known parameters that are part of everyday life; father, mother, children who stay at home, eat, watch TV… Change that means change of tone, behavior, language”.(Psychotherapist, ASL, F, 65 years old)
3.3. Difficult Parenting in Intimate Partner Violence (IPV) Cases
“Fatherhood is a breach in which a little bit of change can be inserted. At least you can try it”.(Psychotherapist and Technical Office Consultant, Court of Naples and private specialist, M, 70 years old)
“The first effort professionals have to make is to bring people to the awareness that the children are experiencing something abominable, terrible and painful”.(Psychotherapist, OLV, M, 31 years old)
“The woman is so destroyed that she cannot manage to contain even the smallest impetuosity of the child”.(Social Worker, Consultancy, F, 58 years old)
“We often face stories of threats and blackmail, where men often threaten to harm their children if women do not behave as they want”.(Psychotherapist, Private, M, 31 years old)
3.4. Intervention in Cases of IPV in Family Contexts and WDV: Representation of Resources, Deficits and Suggestions
“There is still no integration between those who work with women, perpetrators and those who work with children”.(Social Worker, Consultancy, F, 58 years old)
“We have a big problem; when you have to help a child, you need the authorization of the abuser who makes it a blackmail element. And therefore, that child is suspended there, with all his traumas, with all that he has experienced ”.(Social Worker, Consultancy, F, 58 years old)
“I believe that a space for them [men] is important, because at the basis of the violence there are emotions that are not really recognized, and then lead to very heavy experiences”.(Psychotherapist, OLV, F, 32 years old)
“I would work on opening a channel of understanding … that would allow the man to understand the pain it causes on his partner, but also on his children, right?”.(Social Worker, Consultancy, F, 58 years old)
“I lead music therapy groups with children here at the family center and we often make them draw, even while colleagues are sitting with their parents. Suffering experiences really emerge and children can say many things”.(Psychologist, Center for Families, F, 57 years old)
“I think that having care and respect for the workers of these Service is fundamental. It would take more attention, more funds and also more moments of comparison and training, also with other realities and other countries”.(Psychotherapist, OLV, F, 66 years old)
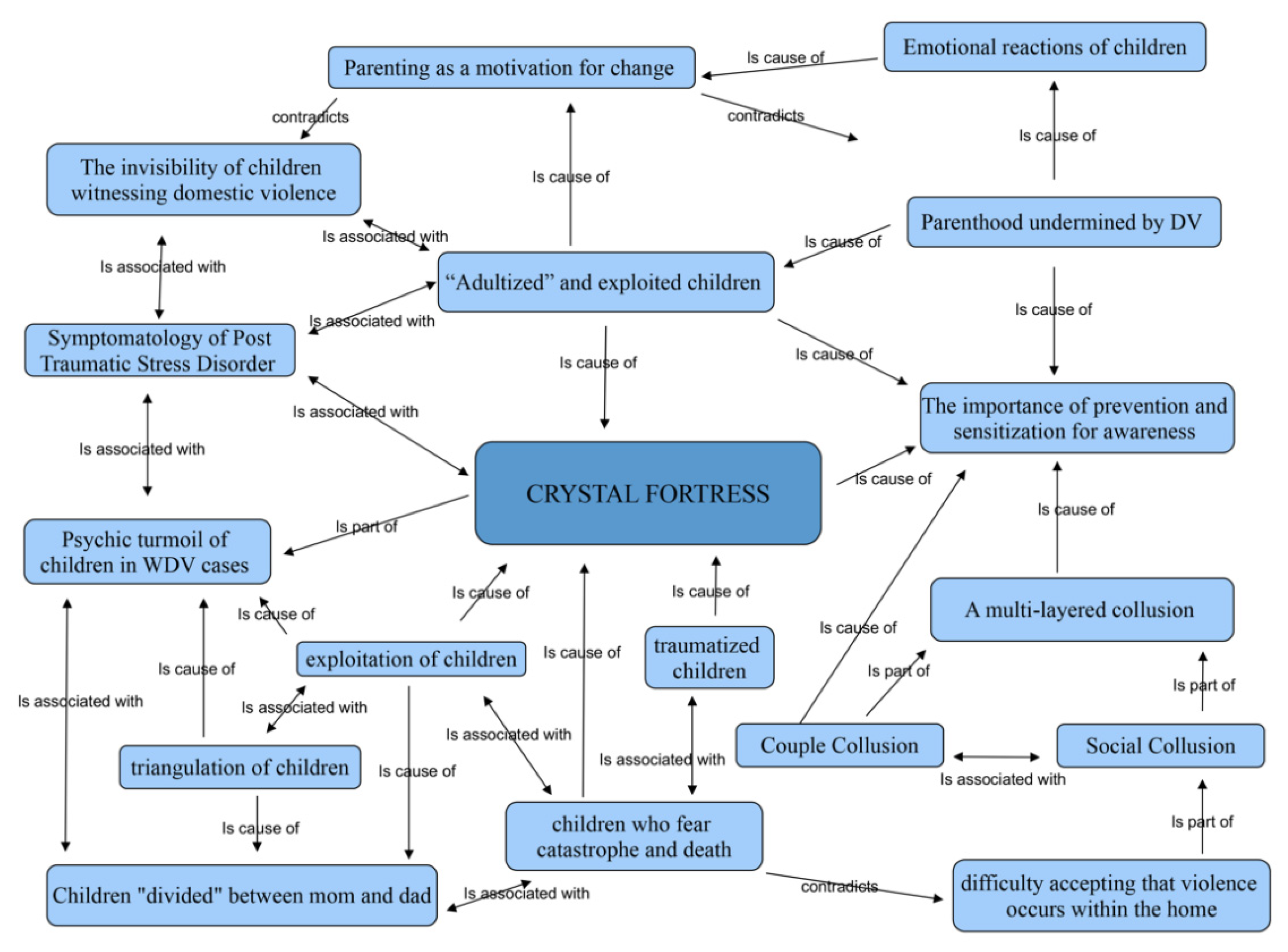
3.5. The Core Category
4. Discussion
Limitations and Future Perspectives
5. Conclusions
- To help parents become aware of the destructive dynamics and splitting mechanisms that activate and overshadow the child.
- To work on parental functions, activating a dialogue between parents and children that reassures children and help them in reconstructing the sense of their experience and bring down the crystal fortress that is harmful to their growth.
- To use a supportive and containing approach that allows the child to express his/her thoughts, fears, emotions and turmoil.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Child Welfare Information Gateway. Child Witnesses to Domestic Violence, 1st ed.; U.S. Department of Health and Human Services, Children’s Bureau: Washington, DC, USA, 2016.
- Save the Children. Children Witnesses of Gender Violence in the Domestic Context, 1st ed.; Save the Children: Madrid, Spain, 2011. [Google Scholar]
- Fantuzzo, J.W.; Boruch, R.; Beriama, A.; Atkins, M.; Marcus, S. Domestic violence and children: Prevalence and risk in five major U.S. cities. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Dargis, M.; Koenings, M. Witnessing domestic violence during childhood is associated with psychopathic traits in adult male criminal offenders. Law Hum. Behav. 2017, 41, 173–179. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Understanding and Addressing Violence Against Women. Intimate Partner Violence, 1st ed.; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Di Napoli, I.; Procentese, F.; Carnevale, S.; Esposito, C.; Arcidiacono, C. Ending intimate partner violence (IPV) and locating men at stake. An ecological approach. Int. J. Environ. Res. Public Health 2019, 16, 1652. [Google Scholar] [CrossRef] [PubMed]
- Osofsky, J.D. Children who witness domestic violence: The invisible victims. Soc. Policy Rep. 1995, 9, 1–16. [Google Scholar] [CrossRef]
- Holden, G.W.; Ritchie, K.L. Linking extreme marital discord, child rearing, and child behavior problems: Evidence from battered women. Child Dev. 1991, 62, 311–327. [Google Scholar] [CrossRef]
- Kitzmann, K.M.; Gaylord, N.K.; Holt, A.R.; Kenny, E.D. Child Witnesses to Domestic Violence: A Meta-Analytic Review. J. Consult. Clin. Psychol. 2003, 71, 339–352. [Google Scholar] [CrossRef]
- C.I.S.M.A.I. (Ed.) Requisiti Minimi Degli Interventi Nei Casi DI Violenza Assistita da Maltrattamento Sulle Madri. Available online: https://cismai.it/requisiti-minimi-degli-interventi-nei-casi-di-violenza-assistita/# (accessed on 25 April 2020).
- Izaguirre, A.; Cater, A. Child witnesses to intimate partner violence: Their descriptions of talking to people about the violence. J. Interpers. Violence 2018, 33, 3711–3731. [Google Scholar] [CrossRef]
- Taylor, A.K.; Gregory, A.; Feder, G.; Williamson, E. ‘We’re all wounded healers’: A qualitative study to explore the well-being and needs of helpline workers supporting survivors of domestic violence and abuse. Health Soc. Care Community 2019, 27, 856–862. [Google Scholar] [CrossRef]
- Arcidiacono, C. The community psychologist as a reflective plumber. Glob. J. Community Psychol. Pract. 2017, 8, 1–16. [Google Scholar] [CrossRef]
- Esposito, F. Practicing ethnography in migration-related detention centers: A reflexive account. J. Prev. Interv. Community 2017, 45, 57–69. [Google Scholar] [CrossRef]
- Gergen, K.J.; Gergen, M.M.; Sadi, M. La Costruzione Sociale Del Dialogo, 1st ed.; Logos Edizioni: Modena, Italy, 2005. [Google Scholar]
- Gergen, K.J.; Romaioli, D. Costruzione Sociale E Pratiche Terapeutiche. Dall’Oppressione Alla Collaborazione, 1st ed.; Franco Angeli: Milano, Italy, 2018. [Google Scholar]
- Mead, G.H. Social consciousness and the consciousness of meaning. Psychol. Bull. 1910, 7, 397–405. [Google Scholar] [CrossRef]
- Blumer, G.H. Symbolic Interactionism; Perspective and Method, 1st ed.; Prentice-Hall: Englewood Cliffs, NJ, USA, 1969. [Google Scholar]
- Rosenberg, M. Children of battered women: The effects of witnessing violence on their social problem-solving abilities. Behav. Ther. 1987, 10, 85–89. [Google Scholar]
- Fusco, R.A.; Fantuzzo, J.W. Domestic violence crimes and children: A population-based investigation of direct sensory exposure and the nature of involvement. Child Youth Serv. Rev. 2009, 31, 249–256. [Google Scholar] [CrossRef]
- Council of Europe. Convention on Preventing and Combating Violence Against Women and Domestic Violence. Available online: https://rm.coe.int/168008482e (accessed on 25 April 2020).
- Wolfe, D.A.; Crooks, C.V.; Lee, V.; McIntyre-Smith, A.; Jaffe, P.G. The effects of children’s exposure to domestic violence: A meta-analysis and critique. Clin. Child Fam. Psychol. Rev. 2003, 6, 171–187. [Google Scholar] [CrossRef]
- Evans, S.; Davies, C.; DiLillo, D. Exposure to Domestic Violence: A meta-analysis of child and adolescent outcomes. Aggress. Violent Behav. 2008, 13, 131–140. [Google Scholar] [CrossRef]
- FRA-European Union Agency for Fundamental Rights. Violence Against Women: An EU-Wide Survey-Survey Methodology, Sample and Fieldwork. Technical Report, 1st ed.; FRA: Vienna, Austria, 2014. [Google Scholar]
- Buckley, H.; Holt, S.; Whelan, S. Listen to me! Children’s experiences of domestic violence. Child Abuse Rev. 2007, 16, 296–310. [Google Scholar] [CrossRef]
- Överlien, C.; Hydén, M. Children’s actions when experiencing domestic violence. Childhood 2009, 16, 479–496. [Google Scholar] [CrossRef]
- Swanston, J.; Bowyer, L.; Vetere, A. Towards a richer understanding of school-age children’s experiences of domestic violence: The voices of children and their mothers. Clin. Child Psychol. Psychiatry 2014, 19, 184–201. [Google Scholar] [CrossRef]
- Sternberg, K.J.; Lamb, M.E.; Greenbaum, C.; Cicchetti, D.; Dawud, S.; Cortes, R.M.; Krispin, O.; Lorey, F. Effects of domestic violence on children’s behavior problems and depression. Dev. Psychol. 1993, 29, 44–52. [Google Scholar] [CrossRef]
- Tsavoussis, A.; Stawicki, S.P.A.; Stoicea, N.; Papadimos, T.J. Child-witnessed domestic violence and its adverse effects on brain development: A call for societal self-examination and awareness. Front Public Health. 2014, 2, 178. [Google Scholar] [CrossRef]
- Moylan, C.A.; Herrenkohl, T.I.; Sousa, C.; Tajima, E.A.; Herrenkohl, R.C.; Russo, M.J. The effects of child abuse and exposure to domestic violence on adolescent internalizing and externalizing behavior problems. J. Fam. Violence 2010, 25, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Williamson, V.; Halligan, S.L.; Coetzee, B.; Butler, I.; Tomlinson, M.; Skeen, S.; Stewart, J. Caregiver experiences of public services following child trauma exposure: A qualitative study. Int. J. Ment. Health Syst. 2018, 12, 15. [Google Scholar] [CrossRef] [PubMed]
- Fanslow, J.L.; Kelly, P.; Ministry of Health. Family Violence Assessment and Intervention Guideline: Child Abuse and Intimate Partner Violence, 2nd ed.; Ministry of Health: Wellington, New Zealand, 2016.
- Anderson, S.; Kinsey, R.; Loader, I.; Smith, C. Cautionary Tales: Young People, Crime and Policing in Edinburgh, 1st ed.; Routledge: London, UK, 2017. [Google Scholar]
- Marchueta, G. I figli della violenza. In Gli Abusi All’Infanzia: I Diversi Interventi Possibili, 1st ed.; Montecchi, F., Ed.; Franco Angeli: Milano, Italy, 2005; pp. 303–323. [Google Scholar]
- Howell, K.H. Resilience and psychopathology in children exposed to family violence. Aggress. Violent Behav. 2011, 16, 562–569. [Google Scholar] [CrossRef]
- Gewirtz, A.H.; Edleson, J.L. Young children’s exposure to intimate partner violence: Towards a developmental risk and resilience framework for research and intervention. J. Fam. Violence 2007, 22, 151–163. [Google Scholar] [CrossRef]
- Miller-Graff, L.E.; Cater, A.K.; Howell, K.H.; Graham-Bermann, S.A. Parent-child warmth as a potential mediator of childhood exposure to intimate partner violence and positive adulthood functioning. Anxiety Stress Coping 2015, 29, 259–273. [Google Scholar] [CrossRef] [PubMed]
- Denham, S.A. Social-emotional competence as support for school readiness: What is it and how do we assess it? Early Educ. Dev. 2006, 17, 57–59. [Google Scholar] [CrossRef]
- Cater, A.K. Children’s meaning-conciliation of their fathers’ violence related to fathers and violence in general. J. Scand. Stud. Criminol. Crime Prev. 2007, 8, 41–55. [Google Scholar] [CrossRef]
- DeBoard-Lucas, R.L.; Grych, J.H. Children’s perceptions of intimate partner violence: Causes, consequences, and coping. J. Fam. Violence 2011, 26, 343–354. [Google Scholar] [CrossRef]
- Münger, A.C.; Markström, A.M. School and child protection services professionals’ views on the school’s mission and responsibilities for children living with domestic violence–tensions and gaps. J. Fam. Violence 2019, 34, 385–398. [Google Scholar] [CrossRef]
- Choi, G. Organizational impacts on the secondary traumatic stress of social workers assisting family violence or sexual assault survivors. Adm. Soc. Work 2011, 35, 225–242. [Google Scholar]
- Amodeo, A.L.; Rubinacci, D.; Scandurra, C. Il ruolo del genere nel lavoro con gli uomini autori di violenza: Affetti e rappresentazioni dei professionisti della salute. La Camera blu. Rivista di Studi di Genere 2018, 19, 5–24. [Google Scholar]
- Procentese, F.; Di Napoli, I.; Arcidiacono, C.; Cerqua, M. Lavorare in centri per uomini violenti affrontandone l’invisibilità della violenza. Psicologia della Salute 2019, 3, 123–136. [Google Scholar] [CrossRef]
- Autiero, M.; Procentese, F.; Carnevale, C.; Arcidiacono, C.; Di Napoli, I. Personnel Fighting Against Gender Violence in Emergency Unit, Prevention and Care Services. Int. J. Environ. Res. Public Health. under review.
- Kulkarni, S.; Herman-Smith, R.; Caldwell Ross, T. Measuring intimate partner violence (IPV) Service providers’ attitudes: The development of the survivor-defined advocacy scale (SDAS). J. Fam. Violence 2015, 30, 911–921. [Google Scholar] [CrossRef]
- Graham-Bermann, S.A.; Kulkarni, M.R.; Kanukollu, S.N. Is disclosure therapeutic for children following exposure to traumatic violence? J. Interpers. Violence 2011, 26, 1056–1076. [Google Scholar] [CrossRef] [PubMed]
- Howell, K.H.; Cater, A.K.; Miller-Graff, L.E.; Graham-Bermann, S.A. The process of reporting and receiving support following exposure to intimate partner violence during childhood. J. Interpers. Violence 2014, 30, 2886–2907. [Google Scholar] [CrossRef]
- Cater, A.K. Children’s descriptions of participation processes in intervention for children exposed to intimate partner violence. Child Adolesc. Soc. Work 2014, 31, 455–473. [Google Scholar] [CrossRef]
- Mullender, A. What children tell us: “He said he was going to kill our mum”. In Domestic Violence and Child Protection: Directions for Good Practice, 1st ed.; Humphreys, C., Stanley, N., Eds.; Sage: London, UK, 2006; pp. 53–73. [Google Scholar]
- Finkelhor, D.; Ormrod, R.K.; Turner, H.A. Polyvictimization and trauma in a national longitudinal cohort. Dev. Psychopathol. 2007, 19, 149–166. [Google Scholar] [CrossRef]
- Solberg, A. Hur förhåller sig barn till våld I hemmet? (How do children respond to violence in their home?). In Barn Somupplevervåld, Nordisk Forskningochpraktik (Children Who Experience Violence: Nordic Research and Practice), 1st ed.; Eriksson, M., Ed.; Gothia Publishers: Stockholm, Sweden, 2007; pp. 25–37. [Google Scholar]
- Georgsson, A.; Almqvist, K.; Broberg, A.G. Naming the unmentionable: How children exposed to intimate partner violence articulate their experiences. J. Fam. Violence 2011, 26, 117–129. [Google Scholar] [CrossRef]
- Crits-Christoph, P.; Baber, J.P.; Kurcias, J.S. The accuracy of Therapists’ interpretations and the development of the therapeutic alliance. Psychother. Res. 1993, 3, 25–35. [Google Scholar] [CrossRef]
- Horvath, A.O.; Luborsky, L. The role of the therapeutic alliance in psychotherapy. J. Consult. Clin. Psychol. 1993, 61, 561–573. [Google Scholar] [CrossRef] [PubMed]
- Carli, R.; Paniccia, R.M. Analisi Della Domanda. Teoria E Tecnica Dell’Intervento; Società Editrice Il Mulino: Roma, Italy, 2003. [Google Scholar]
- Carli, R.; Paniccia, R.M.; Giovagnoli, F.; Dolcetti, F.; Gurrieri, R. La Cultura Locale di Roma e delle sue periferie urbane nella rappresentazione dei resti archeologici. Rivista in Psicologia Clinica 2016, 2, 99–118. [Google Scholar]
- Corbin, J.; Strauss, A. Basics of Qualitative Research; SAGE: London, UK, 2008. [Google Scholar]
- Morse, J.M. Strategies for sampling. In Qualitative Nursing Research: A Contemporary Dialogue, 1st ed.; Morse, J.M., Ed.; Sage Publications Inc: Newbury Park, CA, USA, 1991; pp. 127–145. [Google Scholar]
- Draucker, C.B.; Martsolf, D.S.; Ross, R.; Rusk, T.B. Theoretical sampling and category development in grounded theory. Qual. Health Res. 2007, 17, 1137–1148. [Google Scholar] [CrossRef]
- Robinson, O.C. Sampling in interview-based qualitative research: A theoretical and practical guide. Qual. Res. Psychol. 2014, 11, 25–41. [Google Scholar] [CrossRef]
- Patton, M.Q. Qualitative Research & Evaluation Methods: Integrating Theory and Practice, 4th ed.; SAGE: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Merton, R.K.; Kendal, P.L. L’intervista Focalizzata, 1st ed.; Kurumuny: Lecce, Italy, 2012. [Google Scholar]
- Arcidiacono, C.; Di Napoli, I. Sono Caduta per Le Scale.; Franco Angeli: Milano, Italy, 2012. [Google Scholar]
- Arcidiacono, C. Psicologia DI Comunità per Le Città. Rigenerazione Urbana a Porta Capuana; Liguori: Napoli, Italy, 2017. [Google Scholar]
- Charmaz, K.; Belgrave, L. Thinking about data with grounded theory. Qual. Inq. 2018, 25, 743–753. [Google Scholar] [CrossRef]
- Erikson, M.C.; Christianson, S.Å. Professionals’ experiences with and perceptions of children exposed to severe and homicidal violence in Sweden. Vict. Offender 2017, 12, 1–31. [Google Scholar] [CrossRef]
- Walker, L.E. Post-traumatic stress disorder in women: Diagnosis and treatment of battered woman syndrome. Psychother. Theor. Res. Pract. Train. 1991, 28, 21–29. [Google Scholar] [CrossRef]
- Kendall-Tackett, K.A.; Ruglass, L.M. Women’s Mental Health Across the Lifespan: Challenges, Vulnerabilities, and Strengths, 1st ed.; Taylor & Francis: Abingdon, UK, 2017. [Google Scholar]
- Sullivan, T.P.; Weiss, N.H.; Price, C.; Pugh, N.; Hansen, N.B. Strategies for coping with individual PTSD symptoms: Experiences of African American victims of intimate partner violence. Psychol. Trauma. 2018, 10, 336–344. [Google Scholar] [CrossRef]
- Procentese, F.; Fasanelli, R.; Esposito, C.; Pisapia, N.; Arcidiacono, C.; Di Napoli, I. Downside: The Perpetrator of Violence. Manuscript in preparation.
- Rollero, C. The social dimensions of intimate partner violence. A qualitative study with male perpetrators. Sex. Cult. 2019, 24, 749–763. [Google Scholar] [CrossRef]
- Esposito, C.; Di Napoli, I.; Esposito, C.; Carnevale, S.; Arcidiacono, C. Violence against women: A not in my backyard (NIMBY) Phenomenon. Violence Gend. 2020. [Google Scholar] [CrossRef]


{kind=link}
| Features | Percentages/Frequencies |
|---|---|
| Gender N % | 13 F 81 |
| 3 M 19 | |
| Professional Role % | 69 Psychologists and Psychotherapists 25 Social Workers 6 Doctors |
| Work Context % | 31.25 Center for Families 18.75 Health Consultants 18.75 Private Professionals 12.5 OLV (Project “Oltre La Violenza”) 18.75 Other |
| Years of Service % (range) | 18.75 (1 ≥ 5) 0 (6 ≥ 10) 0 (11 ≥ 15) 81.25 (>15) Mean 27.5 |
| Years in Dealing with Violence % (range) | 6.25 (<1) 12.5 (1 ≥ 5) 18.75 (6 ≥ 10) 0 (11 ≥ 15) 62.5 (>15) Mean 18.31 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carnevale, S.; Di Napoli, I.; Esposito, C.; Arcidiacono, C.; Procentese, F. Children Witnessing Domestic Violence in the Voice of Health and Social Professionals Dealing with Contrasting Gender Violence. Int. J. Environ. Res. Public Health 2020, 17, 4463. https://doi.org/10.3390/ijerph17124463
Carnevale S, Di Napoli I, Esposito C, Arcidiacono C, Procentese F. Children Witnessing Domestic Violence in the Voice of Health and Social Professionals Dealing with Contrasting Gender Violence. International Journal of Environmental Research and Public Health. 2020; 17(12):4463. https://doi.org/10.3390/ijerph17124463
Chicago/Turabian StyleCarnevale, Stefania, Immacolata Di Napoli, Ciro Esposito, Caterina Arcidiacono, and Fortuna Procentese. 2020. "Children Witnessing Domestic Violence in the Voice of Health and Social Professionals Dealing with Contrasting Gender Violence" International Journal of Environmental Research and Public Health 17, no. 12: 4463. https://doi.org/10.3390/ijerph17124463
APA StyleCarnevale, S., Di Napoli, I., Esposito, C., Arcidiacono, C., & Procentese, F. (2020). Children Witnessing Domestic Violence in the Voice of Health and Social Professionals Dealing with Contrasting Gender Violence. International Journal of Environmental Research and Public Health, 17(12), 4463. https://doi.org/10.3390/ijerph17124463