Sex and Gender in Research on Healthcare Workers in Conflict Settings: A Scoping Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Protocol
2.3. Eligibility Criteria
- ▪
- Study Design: primary studies including quantitative (e.g., surveys, cross-sectional, cohort, case-control) and qualitative (e.g., interviews, focus groups). We excluded editorials, commentaries, reviews, and studies published only in abstract form.
- ▪
- Population of interest: Healthcare workers
- ▪
- Setting of interest: Conflict setting
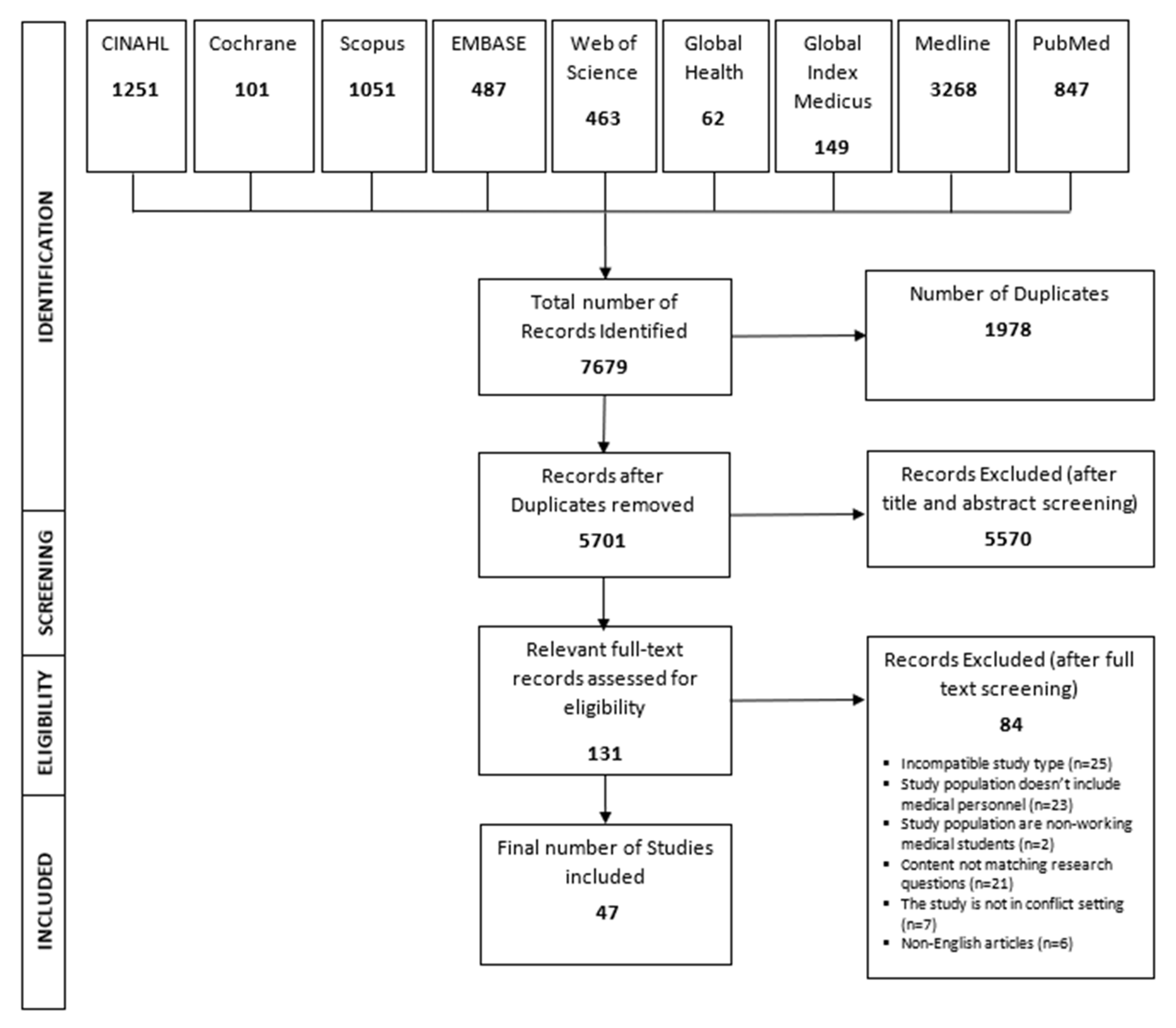
2.4. Literature Search
- ▪
- Keywords used for healthcare workers included: doctors, nurses, midwives, occupational therapists, hospital assistants and secretaries, emergency medical personnel, or any type of occupation that is related to healthcare and healthcare settings.
- ▪
- Keywords used for armed conflict included: war, warfare, terrorism, bioterrorism, battle, combat, or any other term used to describe political problems and conflicts causing political instability.
- ▪
- Keywords used for sex/gender included: sex, gender, men, women, male, female, sex/gender factors, sex/gender characteristics, sex/gender similarities, sex/gender differences, and related terms.
- ▪
- Keywords used for occupational health included: occupational health and safety, work safety, industrial hygiene, quality of working life, and other occupational terms used to describe health and safety of workers.
2.5. Selection Process
2.6. Data Abstraction
2.7. Data Synthesis
- Study sample: The male to female ratio was extracted for each study.
- Terminology: The terms used to refer to sex/gender of participants were identified along with the definition or justification for the use of the term, if available.
- Objectives: Studies were assessed on whether the objectives stated the aim to compare men and women or explore sex/gender similarities and differences.
- Data analysis: Studies were assessed to identify if and how sex/gender was incorporated in the analysis. The categories included: (1) sex/gender was a covariate or confounder in the analysis or (2) the analysis was stratified by sex/gender, in which the exposures and outcomes of interest were analyzed separately for male and female participants.
- Key findings: Sex/gender-related results were identified where available.
- Interpretation of findings: Sex/gender-related interpretation of results were identified where available.
3. Results
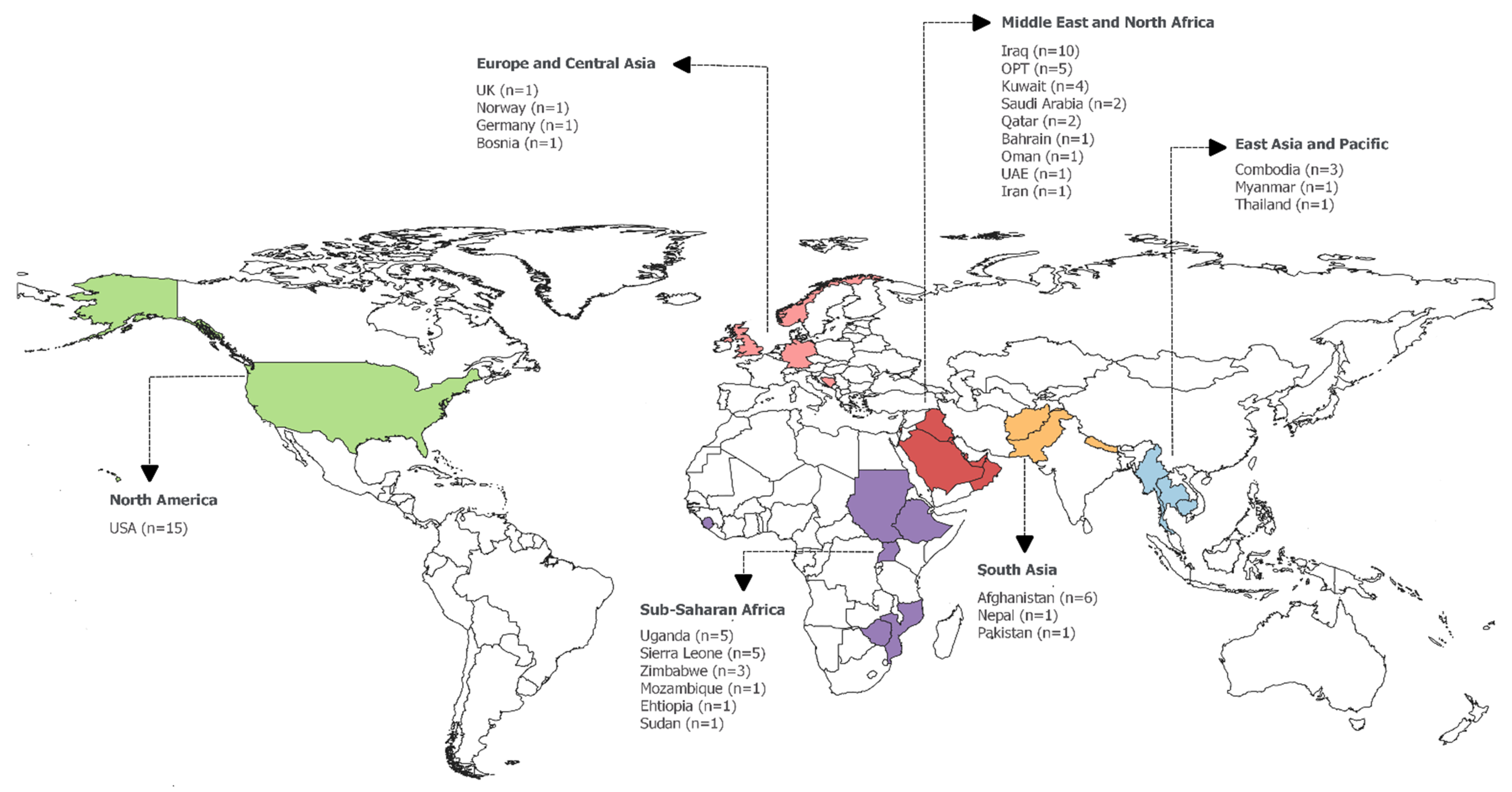
3.1. Characterstics of the Studies
3.2. Main Themes Covered in the Studies
3.2.1. Working Conditions
3.2.2. Workplace Violence
3.2.3. Physical Health
3.2.4. Mental and Social Health
4. Discussion
4.1. Working Conditions
4.2. Workplace Violence
4.3. Physical Health
4.4. Mental and Social Health
4.5. Integration of Sex/Gender in the Included Studies
4.6. Implication for Future Research
4.7. Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- The New Humanitarian. Mapped—A World at War. Available online: https://www.thenewhumanitarian.org/maps-and-graphics/2017/04/04/updated-mapped-world-war (accessed on 20 January 2020).
- Institute for Economics & Peace. Global Peace Index 2019: Measuring Peace in a Complex World, Sydney, June 2019. Available online: http://visionofhumanity.org/reports (accessed on 20 January 2020).
- Murthy, R.S.; Lakshminarayana, R. Mental health consequences of war: A brief review of research findings. World Psychiatry 2006, 5, 25–30. [Google Scholar]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Keeping health workers and facilities safe in war. Bull. World Health Organ. 2012, 90, 1–74. [Google Scholar]
- Afzal, M.H.; Jafar, A.J.N. A scoping review of the wider and long-term impacts of attacks on healthcare in conflict zones. Med. Confl. Surviv. 2019, 35, 43–64. [Google Scholar] [CrossRef]
- Fouad, F.M.; Sparrow, A.; Tarakji, A.; Alameddine, M.; El-Jardali, F.; Coutts, A.P.; El Arnaout, N.; Karroum, L.B.; Jawad, M.; Roborgh, S.; et al. Health workers and the weaponisation of health care in Syria: A preliminary inquiry for The Lancet–American University of Beirut Commission on Syria. Lancet 2017, 390, 2516–2526. [Google Scholar] [CrossRef]
- Bou-Karroum, L.; Daou, K.N.; Nomier, M.; El Arnaout, N.; Fouad, F.M.; El-Jardali, F.; Akl, E.A. Health Care Workers in the setting of the “Arab Spring”: A scoping review for the Lancet-AUB Commission on Syria. J. Glob. Health 2019, 9, 010402. [Google Scholar] [CrossRef]
- Al Sheibani, B.I.; Hadi, N.R.; Hasoon, T. Iraq lacks facilities and expertise in emergency medicine. BMJ 2006, 333, 847. [Google Scholar] [CrossRef]
- Donaldson, R.I.; Mulligan, D.A.; Nugent, K.; Cabral, M.; Saleeby, E.R.; Ansari, W.; Tajer, S.; Gausche-Hill, M. Using tele-education to train civilian physicians in an area of active conflict: Certifying Iraqi physicians in Pediatric Advanced Life Support from the United States. J. Pediatr. 2011, 159, 507–509.e1. [Google Scholar] [CrossRef]
- ReliefWeb. Impunity Remains: Attacks on Health Care in 23 Countries in Conflict in 2018. Available online: https://reliefweb.int/report/world/impunity-remains-attacks-health-care-23-countries-conflict-2018 (accessed on 20 January 2020).
- Medecins San Frontieres. Review of Attack on Al Quds Hospital in Aleppo City. Available online: https://www.msf.org/sites/msf.org/files/al_quds_report.pdf (accessed on 18 March 2020).
- Reichard, A.A.; Marsh, S.M.; Tonozzi, T.R.; Konda, S.; Gormley, M.A. Occupational Injuries and Exposures among Emergency Medical Services Workers. Prehosp. Emerg. Care 2017, 21, 420–431. [Google Scholar] [CrossRef]
- Maguire, B.J.; Smith, S. Injuries and Fatalities among Emergency Medical Technicians and Paramedics in the United States. Prehosp. Disaster Med. 2013, 28, 376–382. [Google Scholar] [CrossRef]
- Patterson, P.D.; Weaver, M.D.; Frank, R.C.; Warner, C.W.; Martin-Gill, C.; Guyette, F.X.; Fairbanks, R.J.; Hubble, M.W.; Songer, T.J.; Callaway, C.W.; et al. Association Between Poor Sleep, Fatigue, and Safety Outcomes in Emergency Medical Services Providers. Prehosp. Emerg. Care 2012, 16, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Roggenkamp, R.; Andrew, E.; Nehme, Z.; Cox, S.; Smith, K. Descriptive Analysis of Mental Health-Related Presentations to Emergency Medical Services. Prehosp. Emerg. Care 2018, 22, 399–405. [Google Scholar] [CrossRef]
- United States Institute of Peace. Gender, War and Peacebuilding. Academy for International Conflict Management and Peacebuilding, Washington DC. Available online: https://www.usip.org/publications/2012/09/gender-war-and-peacebuilding (accessed on 20 January 2020).
- Wizemann, T.M.; Pardue, M.L. (Eds.) Exploring the Biological Contributions to Human Health: Does Sex Matter? National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- Habib, R.R.; Hojeij, S.; Elzein, K. Gender in occupational health research of farmworkers: A systematic review. Am. J. Ind. Med. 2014, 57, 1344–1367. [Google Scholar] [CrossRef]
- Messing, K.; Punnett, L.; Bond, M.; Alexanderson, K.; Pyle, J.; Zahm, S.; Wegman, D.; Stock, S.R.; de Grosbois, S. Be the fairest of them all: Challenges and recommendations for the treatment of gender in occupational health research. Am. J. Ind. Med. 2003, 43, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Messing, K.; Stock, S.; Côté, J.; Tissot, F. Is Sitting Worse Than Static Standing? How a Gender Analysis Can Move Us Toward Understanding Determinants and Effects of Occupational Standing and Walking. J. Occup. Environ. Hyg. 2015, 12, D11–D17. [Google Scholar] [CrossRef] [PubMed]
- International Labor Organization. Gender and Occupational Safety and Health. Occupational Safety and Health. Available online: https://www.ilo.org/safework/areasofwork/gender-and-occupational-safety-and-health/lang--en/index.htm (accessed on 20 January 2020).
- Quinn, M.M.; Smith, P.M. Gender, Work, and Health. Ann. Work Expo. Health 2018, 62, 389–392. [Google Scholar] [CrossRef]
- Sorrentino, E.; Vona, R.; Monterosso, D.; Giammarioli, A.M. Gender issues on occupational safety and health. Annali dell’Istituto Superiore di Sanita 2016, 52, 190–197. [Google Scholar] [CrossRef]
- Cruz Rios, F.; Chong, W.K.; Grau, D. The need for detailed gender-specific occupational safety analysis. J. Saf. Res. 2017, 62, 53–62. [Google Scholar] [CrossRef]
- Armstrong, P.; Messing, K. Taking Gender into Account in Occupational Health Research: Continuing Tensions. Policy Pract. Health Saf. 2014, 12, 3–16. [Google Scholar] [CrossRef]
- Johnson, J.L.; Greaves, L.; Repta, R. Better Science with Sex and Gender: A Primer for Health Research; Women’s Health Research Network: Vancouver, BC, Canada, 2007. [Google Scholar]
- George, A. Nurses, community health workers, and home carers: Gendered human resources compensating for skewed health systems. Glob. Public Health 2008, 3, 75–89. [Google Scholar] [CrossRef]
- Boniol, M.; Mclsaac, M.; Xu, L.; Wuliji, T.; Diallo, K.; Campbell, J. Gender Equity in the Health Workforce: Analysis of 104 Countries. Working Paper 1; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Barbosa, R.E.C.; Assunção, A.Á.; de Araújo, T.M. Musculoskeletal pain among healthcare workers: An exploratory study on gender differences. Am. J. Ind. Med. 2013, 56, 1201–1212. [Google Scholar] [CrossRef] [PubMed]
- Ariza-Montes, A.; Muniz, N.M.; Montero-Simó, M.J.; Araque-Padilla, R.A. Workplace Bullying among Healthcare Workers. Int. J. Environ. Res. Public Health 2013, 10, 3121–3139. [Google Scholar] [CrossRef] [PubMed]
- Ghandour, R.; Husseini, A.; Sibai, A.M.; Abu-Rmeileh, N.M.E. Cardiovascular disease research in the Arab world: A scoping review from seven Arab countries (2000–2018). Public Health 2019, 175, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Colquhoun, H.L.; Levac, D.; O’Brien, K.K.; Straus, S.; Tricco, A.C.; Perrier, L.; Kastner, M.; Moher, D. Scoping reviews: Time for clarity in definition, methods, and reporting. J. Clin. Epidemiol. 2014, 67, 1291–1294. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Baldini Soares, C.; Khalil, H.; Parker, D. Scoping Reviews. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2017; Chapter 11; Available online: https://reviewersmanual.joannabriggs.org/ (accessed on 15 January 2020).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Najafizada, S.A.; Labonte, R.; Bourgeault, I.L. Community health workers of Afghanistan: A qualitative study of a national program. Confl. Health 2014, 8, 26. [Google Scholar] [CrossRef]
- Witter, S.; Namakula, J.; Wurie, H.; Chirwa, Y.; So, S.; Vong, S.; Ros, B.; Buzuzi, S.; Theobald, S. The gendered health workforce: Mixed methods analysis from four fragile and post-conflict contexts. Health Policy Plann. 2017, 32, V52–V62. [Google Scholar] [CrossRef]
- Macera, C.A.; Aralis, H.J.; Highfill-McRoy, R.; Rauh, M.J. Posttraumatic stress disorder after combat zone deployment among navy and marine corps men and women. J. Women’s Health 2014, 23, 499–505. [Google Scholar] [CrossRef]
- Maes, K.; Kalofonos, I. Becoming and remaining community health workers: Perspectives from Ethiopia and Mozambique. Soc. Sci. Med. 2013, 87, 52–59. [Google Scholar] [CrossRef]
- Witter, S.; Wurie, H.; Namakula, J.; Mashange, W.; Chirwa, Y.; Alonso-Garbayo, A.; Alonso-Garbayo, A. Why do people become health workers? Analysis from life histories in 4 post-conflict and post-crisis countries. Int. J. Health Plan. Manag. 2018, 33, 449–459. [Google Scholar] [CrossRef]
- Namakula, J.; Witter, S. Living through conflict and post-conflict: Experiences of health workers in northern Uganda and lessons for people-centred health systems. Health Policy Plan 2014, 29 (Suppl. 2), ii6–ii14. [Google Scholar] [CrossRef]
- Namakula, J.; Witter, S.; Ssengooba, F. Health worker experiences of and movement between public and private not-for-profit sectors-findings from post-conflict Northern Uganda. Hum. Resour. Health 2016, 14, 18. [Google Scholar] [CrossRef]
- Wurie, H.R.; Samai, M.; Witter, S. Retention of health workers in rural Sierra Leone: Findings from life histories. Hum. Resour. Health 2016, 14, 3. [Google Scholar] [CrossRef] [PubMed]
- Raven, J.; Wurie, H.; Witter, S. Health workers’ experiences of coping with the Ebola epidemic in Sierra Leone’s health system: A qualitative study. BMC Health Serv. Res. 2018, 18, 251. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Gimbel, S.; Malik, E.; Hassen, S.; Hagopian, A. The experience of Chinese physicians in the national health diplomacy programme deployed to Sudan. Glob. Public Health 2012, 7, 196–211. [Google Scholar] [CrossRef] [PubMed]
- Witter, S.; Wurie, H.; Chandiwana, P.; Namakula, J.; So, S.; Alonso-Garbayo, A.; Ssengooba, F.; Raven, J. How do health workers experience and cope with shocks? Learning from four fragile and conflict-affected health systems in Uganda, Sierra Leone, Zimbabwe and Cambodia. Health Policy Plan. 2017, 32, iii3–iii13. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, R.I.; Shanovich, P.; Shetty, P.; Clark, E.; Aziz, S.; Morton, M.; Hasoon, T.; Evans, G. A survey of national physicians working in an active conflict zone: The challenges of emergency medical care in Iraq. Prehosp. Disaster Med. 2012, 27, 153–161. [Google Scholar] [CrossRef]
- Sousa, C.; Hagopian, A. Conflict, health care and professional perseverance: A qualitative study in the West Bank. Glob. Public Health 2011, 6, 520–533. [Google Scholar] [CrossRef]
- Burnham, G.; Malik, S.; Al-Shibli, A.S.; Mahjoub, A.R.; Baqer, A.Q.; Baqer, Z.Q.; Al Qaraghuli, F.; Doocy, S. Understanding the impact of conflict on health services in Iraq: Information from 401 Iraqi refugee doctors in Jordan. Int. J. Health Plan. Manag. 2012, 27, e51–e64. [Google Scholar] [CrossRef]
- Devkota, B.; van Teijlingen, E. Demystifying the Maoist barefoot doctors of Nepal. Med. Confl. Surviv. 2010, 26, 108–123. [Google Scholar] [CrossRef]
- Lewis, P.C.; Stewart, D.; Brown, W. Deployment experiences of Army nurse practitioners. Mil. Med. 2012, 177, 889–893. [Google Scholar] [CrossRef] [PubMed]
- Footer, K.H.; Meyer, S.; Sherman, S.G.; Rubenstein, L. On the frontline of eastern Burma’s chronic conflict--listening to the voices of local health workers. Soc. Sci. Med. 2014, 120, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Aldrich, T.K.; Gustave, J.; Hall, C.B.; Cohen, H.W.; Webber, M.P.; Zeig-Owens, R.; Cosenza, K.; Christodoulou, V.; Glass, L.; Al-Othman, F.; et al. Lung function in rescue workers at the World Trade Center after 7 years. N. Engl. J. Med. 2010, 362, 1263–1272. [Google Scholar] [CrossRef] [PubMed]
- Berrios-Torres, S.I.; Greenko, J.A.; Phillips, M.; Miller, J.R.; Treadwell, T.; Ikeda, R.M. World Trade Center rescue worker injury and illness surveillance, New York, 2001. Am. J. Prev. Med. 2003, 25, 79–87. [Google Scholar] [CrossRef]
- Smith, E.C.; Burkle, F.M., Jr. Paramedic and emergency medical technician reflections on the ongoing impact of the 9/11 terrorist attacks. Prehosp. Disaster Med. 2019, 34, 56–61. [Google Scholar] [CrossRef]
- Wheeler, K.; McKelvey, W.; Thorpe, L.; Perrin, M.; Cone, J.; Kass, D.; Farfel, M.; Thomas, P.; Brackbill, R. Asthma diagnosed after 11 September 2001 among rescue and recovery workers: Findings from the World Trade Center Health Registry. Environ. Health Perspect. 2007, 115, 1584–1590. [Google Scholar] [CrossRef]
- Crowley, L.E.; Herbert, R.; Moline, J.M.; Wallenstein, S.; Shukla, G.; Schechter, C.; Skloot, G.S.; Udasin, I.; Luft, B.J.; Harrison, D.; et al. “Sarcoid like” granulomatous pulmonary disease in World Trade Center disaster responders. Am. J. Ind. Med. 2011, 54, 175–184. [Google Scholar] [CrossRef]
- Daly, E.S.; Gulliver, S.B.; Zimering, R.T.; Knight, J.; Kamholz, B.W.; Morissette, S.B. Disaster mental health workers responding to Ground Zero: One year later. J. Trauma Stress 2008, 21, 227–230. [Google Scholar] [CrossRef]
- Slusarcick, A.L.; Ursano, R.J.; Fullerton, C.S.; Dinneen, M.P. Stress and coping in male and female health care providers during the Persian Gulf War: The USNS Comfort hospital ship. Mil. Med. 1999, 164, 166–173. [Google Scholar] [CrossRef][Green Version]
- Michlig, G.J.; Lafta, R.; Al-Nuaimi, M.; Burnham, G. Providing healthcare under ISIS: A qualitative analysis of healthcare worker experiences in Mosul, Iraq between June 2014 and June 2017. Glob. Public Health 2019, 14, 1414–1427. [Google Scholar] [CrossRef]
- Hamdan, M.; Abu Hamra, A. Workplace violence towards workers in the emergency departments of Palestinian hospitals: A cross-sectional study. Hum. Resour. Health 2015, 13, 28. [Google Scholar] [CrossRef] [PubMed]
- Kitaneh, M.; Hamdan, M. Workplace violence against physicians and nurses in Palestinian public hospitals: A cross-sectional study. BMC Health Serv. Res. 2012, 12, 469. [Google Scholar] [CrossRef] [PubMed]
- Lafta, R.K.; Falah, N. Violence against health-care workers in a conflict affected city. Med. Confl. Surviv. 2019, 35, 65–79. [Google Scholar] [CrossRef]
- Vossbrinck, M.; Zeig-Owens, R.; Hall, C.B.; Schwartz, T.; Moir, W.; Webber, M.P.; Cohen, H.W.; Nolan, A.; Weiden, M.D.; Christodoulou, V.; et al. Post-9/11/2001 lung function trajectories by sex and race in World Trade Center-exposed New York City emergency medical service workers. Occup. Environ. Med. 2017, 74, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Yip, J.; Zeig-Owens, R.; Webber, M.P.; Kablanian, A.; Hall, C.B.; Vossbrinck, M.; Xiaoxue, L.; Weakley, J.; Schwartz, T.; Kelly, K.J.; et al. World Trade Center-related physical and mental health burden among New York City Fire Department emergency medical service workers. Occup. Environ. Med. 2016, 73, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Thomyangkoon, P.; Kongsakon, R.; Pornputkul, V.; Putthavarang, T. Quality of life, needs and the mode of coping of the health personnel at Naradhiwasrajanagarindra Hospital in terrorism influence area in Thailand. J. Med Assoc. Thail. 2012, 95 (Suppl. 3), S102–S108. [Google Scholar]
- Glaser, M.S.; Shah, N.; Webber, M.P.; Zeig-Owens, R.; Jaber, N.; Appel, D.W.; Hall, C.B.; Weakley, J.; Cohen, H.W.; Shulman, L.; et al. Obstructive sleep apnea and World Trade Center exposure. J. Occup. Environ. Med. 2014, 56 (Suppl. 10), S30–S34. [Google Scholar] [CrossRef]
- Putman, B.; Zeig-Owens, R.; Singh, A.; Hall, C.B.; Schwartz, T.; Webber, M.P.; Cohen, H.W.; Prezant, D.J.; Bachert, C.; Weiden, M.D. Risk factors for post-9/11 chronic rhinosinusitis in Fire Department of the City of New York workers. Occup. Environ. Med. 2018, 75, 884–889. [Google Scholar] [CrossRef]
- Webber, M.P.; Glaser, M.S.; Weakley, J.; Soo, J.; Ye, F.; Zeig-Owens, R.; Weiden, M.D.; Nolan, A.; Aldrich, T.K.; Kelly, K.; et al. Physician-diagnosed respiratory conditions and mental health symptoms 7–9 years following the World Trade Center disaster. Am. J. Ind. Med. 2011, 54, 661–671. [Google Scholar] [CrossRef]
- Webber, M.P.; Moir, W.; Crowson, C.S.; Cohen, H.W.; Zeig-Owens, R.; Hall, C.B.; Berman, J.; Qayyum, B.; Jaber, N.; Matteson, E.L.; et al. Post-September 11, 2001, Incidence of Systemic Autoimmune Diseases in World Trade Center-Exposed Firefighters and Emergency Medical Service Workers. Mayo Clin. Proc. 2016, 91, 23–32. [Google Scholar] [CrossRef]
- Yip, J.; Zeig-Owens, R.; Hall, C.B.; Webber, M.P.; Olivieri, B.; Schwartz, T.; Kelly, K.J.; Prezant, D.J. Health Conditions as Mediators of the Association between World Trade Center Exposure and Health-Related Quality of Life in Firefighters and EMS Workers. J. Occup. Environ. Med. 2016, 58, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, S.W.; Hickling, E.J.; Barnett, S.D.; Herbig-Wall, P.L.; Watts, D.D. Gender differences in response to deployment among military healthcare providers in Afghanistan and Iraq. J. Women’s Health (Larchmt). 2012, 21, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Maupin, G.M.; Tvaryanas, A.P.; White, E.D.; Mahaney, H.J. Assessment of Deployment-Related Exposures on Risk of Incident Mental Health Diagnoses Among Air Force Medical Service Personnel: Nested Case-Control Study. Mil. Med. 2018, 183, e123–e132. [Google Scholar] [CrossRef] [PubMed]
- Biggs, Q.M.; Fullerton, C.S.; Reeves, J.J.; Grieger, T.A.; Reissman, D.; Ursano, R.J. Acute Stress Disorder, Depression, and Tobacco Use in Disaster Workers Following 9/11. Am. J. Orthopsychiat. 2010, 80, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Misra, M.; Greenberg, N.; Hutchinson, C.; Brain, A.; Glozier, N. Psychological impact upon London Ambulance Service of the 2005 bombings. Occup. Med. (Lond.) 2009, 59, 428–433. [Google Scholar] [CrossRef]
- Tvaryanas, A.P.; Maupin, G.M.; Fouts, B.L. Assessment of Deployment-Related Exposures on Risk of Incident Mental Health Diagnoses Among Air Force Critical Care Providers: Nested Case-Control Study. Mil. Med. 2016, 181, 143–151. [Google Scholar] [CrossRef][Green Version]
- Kolkow, T.T.; Spira, J.L.; Morse, J.S.; Grieger, T.A. Post-traumatic stress disorder and depression in health care providers returning from deployment to Iraq and Afghanistan. Mil. Med. 2007, 172, 451–455. [Google Scholar] [CrossRef]
- Pedersen, M.J.B.; Gjerland, A.; Rund, B.R.; Ekeberg, Ø.; Skogstad, L. Emergency preparedness and role clarity among rescue workers during the terror attacks in Norway July 22, 2011. PLoS ONE 2016, 11. [Google Scholar] [CrossRef]
- Veronese, G. Self-perceptions of well-being in professional helpers and volunteers operating in war contexts. J. Health Psychol. 2013, 18, 911–925. [Google Scholar] [CrossRef]
- Sargent, P.; Millegan, J.; Delaney, E.; Roesch, S.; Sanders, M.; Mak, H.; Mallahan, L.; Raducha, S.; Webb-Murphy, J. Health Care Provider Burnout in a United States Military Medical Center During a Period of War. Mil. Med. 2016, 181, 136–142. [Google Scholar] [CrossRef]
- Hamdan, M.; Hamra, A.A. Burnout among workers in emergency Departments in Palestinian hospitals: Prevalence and associated factors. BMC Health Serv. Res. 2017, 17, 407. [Google Scholar] [CrossRef] [PubMed]
- Razik, S.; Ehring, T.; Emmelkamp, P.M. Psychological consequences of terrorist attacks: Prevalence and predictors of mental health problems in Pakistani emergency responders. Psychiatry Res. 2013, 207, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Webster, P.C. The deadly effects of violence against medical workers in war zones. CMAJ 2011, 183, E981–E982. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Campos-Serna, J.; Ronda-Pérez, E.; Artazcoz, L.; Moen, B.E.; Benavides, F.G. Gender inequalities in occupational health related to the unequal distribution of working and employment conditions: A systematic review. Int. J. Equity Health 2013, 12, 57. [Google Scholar] [CrossRef]
- Pillips, J.P. Workplace Violence against Health Care Workers in the United States. N. Engl. J. Med. 2015, 374, 1661–1669. [Google Scholar] [CrossRef]
- Sun, P.; Zhang, X.; Sun, Y.; Ma, H.; Jiao, M.; Xing, K.; Kang, Z.; Ning, N.; Fu, Y.; Wu, Q.; et al. Workplace Violence against Health Care Workers in North Chinese Hospitals: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2017, 14, 96. [Google Scholar] [CrossRef] [PubMed]
- Acquadro Maran, D.; Cortese, C.G.; Pavanelli, P.; Fornero, G.; Gianino, M.M. Gender differences in reporting workplace violence: A qualitative analysis of administrative records of violent episodes experienced by healthcare workers in a large public Italian hospital. BMJ Open 2019, 9, e031546. [Google Scholar] [CrossRef]
- Steege, R.; Taegtmeyer, M.; McCollum, R.; Hawkins, K.; Ormel, H.; Kok, M.; Rashid, S.; Otiso, L.; Sidat, M.; Chikaphupha, K.; et al. How do gender relations affect the working lives of close to community health service providers? Empirical research, a review and conceptual framework. Soc. Sci. Med. 2018, 209, 1–13. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Gender disparities and mental health: The Facts. Available online: https://www.who.int/mental_health/prevention/genderwomen/en/ (accessed on 19 March 2020).
- Seidler, Z.E.; Dawes, A.J.; Rice, S.M.; Oliffe, J.L.; Dhillon, H.M. The role of masculinity in men’s help-seeking for depression: A systematic review. Clin. Psychol. Rev. 2016, 49, 106–118. [Google Scholar] [CrossRef]
- Messing, K.; Stock, S.R.; Tissot, F. Should studies of risk factors for musculoskeletal disorders be stratified by gender? Lessons from the 1998 Quebec Health and Social Survey. Scand. J. Work Environ. Health 2009, 35, 96–112. [Google Scholar] [CrossRef]
- Messing, K.; Chatigny, C.; Courville, J. ‘Light’ and ‘heavy’ work in the housekeeping service of a hospital. Appl. Ergon. 1998, 29, 451–459. [Google Scholar] [CrossRef]
- Day, S.; Mason, R.; Lagosky, S.; Rochon, P.A. Integrating and evaluating sex and gender in health research. Health Res. Policy Syst. 2016, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Habib, R.R.; Elzein, K.; Younes, N. Intersectionality: The value for occupational health research. In Handbook on Gender and Health; Edward Elgar Publishing: Cheltenham, UK, 2016. [Google Scholar] [CrossRef]
- Messing, K.; Mager Stellman, J. Sex, gender and women’s occupational health: The importance of considering mechanism. Environ. Res. 2006, 101, 149–162. [Google Scholar] [CrossRef]
- International Labor Organization. 10 Keys for Gender Sensitive OSH Practice Guidelines for Gender Mainstreaming in Occupational Safety and Health; International Labor Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Heise, L.; Greene, M.E.; Opper, N.; Stavropoulou, M.; Harper, C.; Nascimento, M.; Zewdie, D.; Darmstadt, G.L.; Greene, M.E.; Hawkes, S.; et al. Gender inequality and restrictive gender norms: Framing the challenges to health. Lancet 2019, 393, 2440–2454. [Google Scholar] [CrossRef]
- Artazcoz, L.; Cortès-Franch, I.; Escribà-Agüir, V. Gender, work and health: A step forward in women’s occupational health. In Handbook on Gender and Health; Edward Elgar Publishing: Cheltenham, UK, 2016. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Number of Studies | Percentage |
|---|---|---|
| Study design | ||
| Quantitative studies | ||
| Cross-sectional surveys | 16 | 34 |
| Cohort | 14 | 30 |
| Case-control | 2 | 4 |
| Qualitative studies | ||
| Cross-sectional | 12 | 26 |
| Mixed methods | 3 | 6 |
| Region * | ||
| Middle East and North Africa | 15 | 32 |
| North America | 15 | 32 |
| Sub-Saharan Africa | 9 | 19 |
| South Asia | 8 | 17 |
| East Asia and Pacific | 5 | 11 |
| Europe and Central Asia | 3 | 6 |
| Type of healthcare workers | ||
| Healthcare staff in hospital settings | 22 | 47 |
| Emergency medical service personnel | 16 | 34 |
| Deployed military medical staff | 9 | 19 |
| Sample size * | ||
| <50 | 12 | 26 |
| 50–99 | 3 | 6 |
| 100–499 | 18 | 38 |
| 500–999 | 6 | 13 |
| ≥1000 | 10 | 21 |
| Theme * | ||
| Mental and social health | 23 | 49 |
| Working conditions | 21 | 45 |
| Physical health | 15 | 32 |
| Workplace violence | 3 | 6 |
| Sex/Gender Considerations | Number of Studies | Percentage |
|---|---|---|
| Male/female ratio in study participants * | ||
| More males than females 1 | 21 | 43 |
| More females than males 2 | 10 | 23 |
| Almost equal 3 | 8 | 17 |
| Male only 4 | 5 | 11 |
| Sex/gender not specified | 3 | 6 |
| Justification for male/female ratio in sample | ||
| Almost equal | ||
| Yes | 1 | 2 |
| No | 7 | 15 |
| Unequal ratios | ||
| Yes | 6 | 13 |
| No | 25 | 53 |
| Only male participants | ||
| Yes | 0 | 0 |
| No | 5 | 6 |
| Not Applicable ** | 3 | 6 |
| Term used to refer to sex/gender of participants | ||
| Sex | 6 | 14 |
| Gender | 27 | 57 |
| Sex and gender | 9 | 19 |
| Male/female | 3 | 6 |
| Men/women | 2 | 4 |
| Justification for the use of sex and gender terms | ||
| Sex | ||
| Yes | 0 | 0 |
| No | 6 | 13 |
| Gender | ||
| Yes | 1 | 2 |
| No | 26 | 55 |
| Sex and gender | ||
| Yes | 0 | 0 |
| No | 9 | 19 |
| Not Applicable *** | 5 | 11 |
| Sex/gender-related objectives | ||
| Yes | 8 | 17 |
| No | 39 | 83 |
| Sex/gender in the analysis | ||
| Quantitative Analyses | ||
| Confounder or covariate in multivariate models | 12 | 26 |
| Explanatory variable in univariate models | 4 | 9 |
| Stratified analysis by sex/gender | 3 | 6 |
| No consideration of sex/gender in statistical models | 4 | 9 |
| No statistical models—only descriptive analysis | 4 | 9 |
| Males only in the study | 5 | 11 |
| Qualitative Analyses | ||
| Sex/gender analysis | 3 | 6 |
| No sex/gender analysis | 12 | 26 |
| Sex/gender-related findings | ||
| Yes | 30 | 64 |
| No | 17 | 36 |
| Interpretation of sex/gender-related findings **** | ||
| Yes | 1 | 32 |
| No | 15 | 32 |
| Theme | Sex/Gender-Related Key Findings |
|---|---|
| Working Conditions | Females predominate low-paying and un-paid healthcare positions; males predominate managerial and policy-maker positions Motivations for joining the profession include: escape from poverty, higher salaries, personal calling, status, and a sense of deservingness for both males and females Work challenges include: limited supplies and equipment, insufficient medications, shortage of qualified personnel, increase in workload, and economic insecurity for both males and females Exposure to environmental and occupational hazards including: (1) physical hazards including violence, injury and combat exposures, (2) chemical hazards including dust and smoke containing air pollutants, toxic clouds, particulate matter, and demolition rubbles, and (3) psychological hazards including trauma for both males and females Stress-related exposures for both males and females—increased levels reported by females Demotivating factors for practicing in conflict zones including limited financial incentives, difficult working conditions, and lack of career progression for both males and females; separation from family more demotivating for females |
| Workplace Violence | Exposure to workplace violence for both males and females; males reported more exposure to physical violence |
| Physical Health | Poorer health status reported by males compared to females Health conditions including: chronic respiratory illnesses, allergies, asthma, gastroesophageal problems, eye problems, neurological problems, musculoskeletal and systematic auto-immune disorders, and cancer reported by both males and females Rhinosinusitis, gastroesophageal reflux disease, obstructive airway disease reported more among females than males Lung function decline for both male and female emergency medical workers |
| Mental and Social Health | Post-traumatic stress disorder (PTSD), anxiety, depression, and probable autism spectrum disorder reported by both male and female deployed HCWs; increased rated of PTSD, depression, and post-deployment mental health in females compared to males Increased levels of burnout in males compared to females Increased rates of separation and divorce after return from deployment for females compared to males Mental health help-seeking behavior more predominant in females than in males (example: seeking help for PTSD) Coping strategies and stress reduction methods including: individual resources (such as optimism, spirituality, religiosity, hope, resilience, commitment, and trust in personal abilities), psychological support, sharing with friends and co-workers, borrowing money, and working in two jobs, for both males and females |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Habib, R.R.; Halwani, D.A.; Mikati, D.; Hneiny, L. Sex and Gender in Research on Healthcare Workers in Conflict Settings: A Scoping Review. Int. J. Environ. Res. Public Health 2020, 17, 4331. https://doi.org/10.3390/ijerph17124331
Habib RR, Halwani DA, Mikati D, Hneiny L. Sex and Gender in Research on Healthcare Workers in Conflict Settings: A Scoping Review. International Journal of Environmental Research and Public Health. 2020; 17(12):4331. https://doi.org/10.3390/ijerph17124331
Chicago/Turabian StyleHabib, Rima R., Dana A. Halwani, Diana Mikati, and Layal Hneiny. 2020. "Sex and Gender in Research on Healthcare Workers in Conflict Settings: A Scoping Review" International Journal of Environmental Research and Public Health 17, no. 12: 4331. https://doi.org/10.3390/ijerph17124331
APA StyleHabib, R. R., Halwani, D. A., Mikati, D., & Hneiny, L. (2020). Sex and Gender in Research on Healthcare Workers in Conflict Settings: A Scoping Review. International Journal of Environmental Research and Public Health, 17(12), 4331. https://doi.org/10.3390/ijerph17124331