Waiting Time between Breast Cancer Diagnosis and Treatment in Brazilian Women: An Analysis of Cases from 1998 to 2012


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
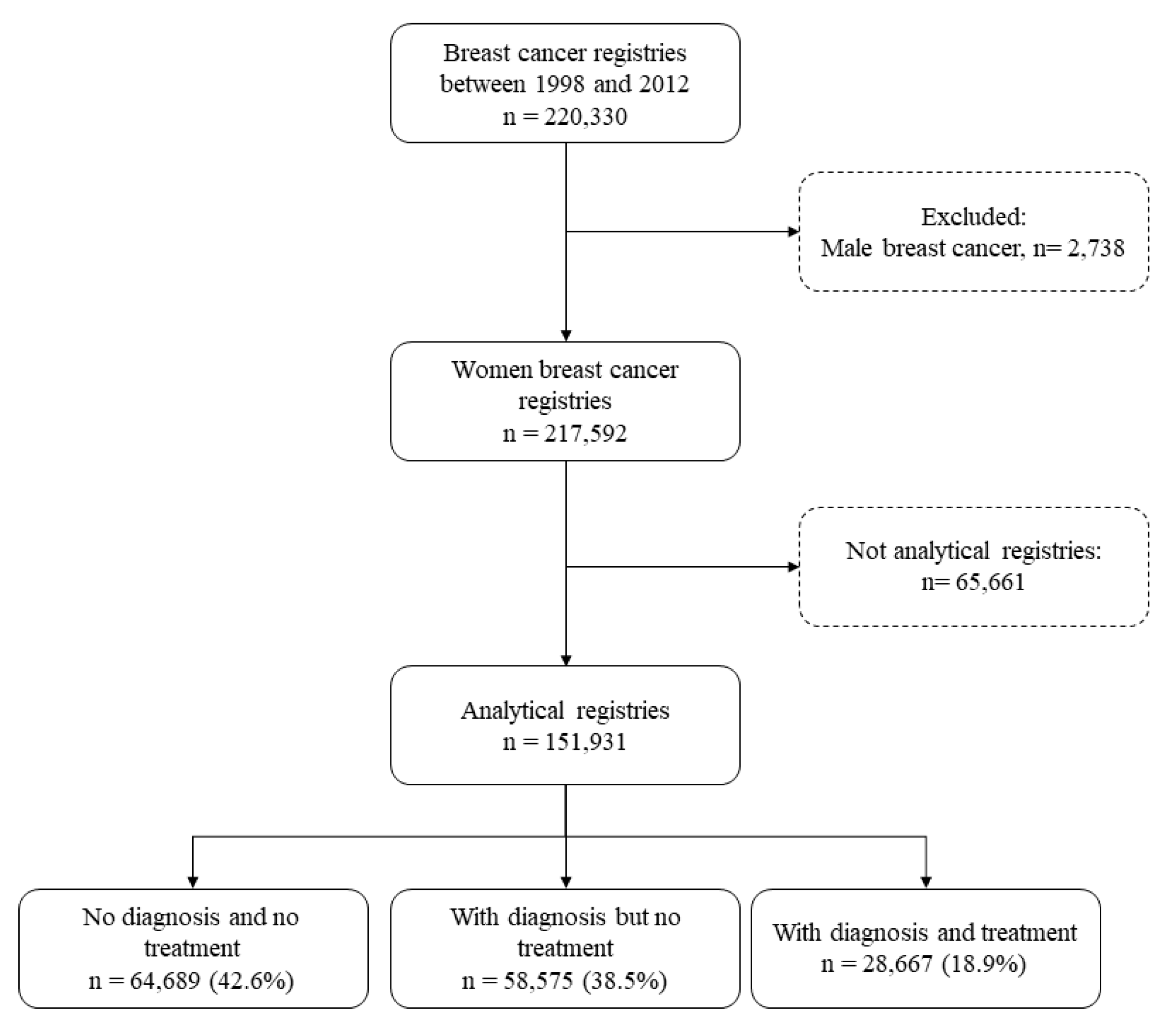
2.2. Participants
2.3. Source and Data Extraction
2.4. Ethical Issues
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. International Agency for Research on Cancer. Globocan 2012: Estimated Cancer Incidence, Mortality a Prevalence Worldwide in 2012. Available online: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx (accessed on 12 March 2014).
- National Cancer Institute. General Coordination of Strategic Actions. Coordination of Prevention and Surveillance. Estimate 2018: Incidence of Cancer in Brazil; INCA: Rio de Janeiro, Brazil, 2017. [Google Scholar]
- Ángeles-Llerenas, A.; Torres-Mejía, G.; Lazcano-Ponce, E.; Uscanga-Sánchez, S.; Mainero-Ratchelous, F.; Hernández-Ávila, J.E.; Morales-Carmona, E.; Hernández-Ávila, M. Effect of care-delivery delays on the survival of Mexican women with breast cancer. Salud Pública México 2016, 58, 237–250. [Google Scholar] [CrossRef]
- Ferreira, N.A.S.; De Carvalho, S.M.F.; Valenti, V.E.; Bezerra, I.M.P.; Batista, H.M.T.; De Abreu, L.C.; Matos, L.L.; Adami, F. Treatment delays among women with breast cancer in a low socio-economic status region in Brazil. BMC Women’s Health 2017, 17, 13. [Google Scholar] [CrossRef]
- Boukai, A.; Gonçalves, A.C.; Padoan, M.; Andrade, P.; Carvalho, N.; Lemos, F.; Almeida, T.; Salem, J.; Gauí, M.F.D.; Teich, N.; et al. Outcome of Patients with Breast Cancer Treated in a Private Health Care Institution in Brazil. J. Glob. Oncol. 2018, 4, 1–10. [Google Scholar] [CrossRef]
- Figueiredo, F.W.D.S.; Almeida, T.C.D.C.; Schoueri, J.H.M.; Luisi, C.; Adami, F. Association between primary care coverage and breast cancer mortality in Brazil. PLoS ONE 2018, 13, e0200125. [Google Scholar] [CrossRef] [PubMed]
- Trufelli, D.C.; Matos, L.L.; Santi, P.X.; Del Giglio, A. Adjuvant treatment delay in breast cancer patients. Revista da Associação Médica Brasileira 2015, 61, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Brazil. Presidency of the Republic. Civil House. Subchefia for Legal Affairs. Law No. 12,732 of 22 November 2012. Provides for the First Patient Treatment with Proven Malignancy and Sets Deadline for the Beginning. Official Gazette. 23 November 2012. Available online: http://www.planalto.gov.br/ccivil_03/_ato2011-2014/2012/lei/l12732.htm (accessed on 17 January 2014).
- Freitas, A.G.Q.; Weller, M. Patient delays and system delays in breast cancer treatment in developed and developing countries. Ciência Saúde Coletiva 2015, 20, 3177–3189. [Google Scholar] [CrossRef] [PubMed]
- Presidency of the Republic. Civil House. Subchefia for Legal Affairs. Law No. 8080, Dated 19 September 1990. Provides for the Conditions for the Promotion, Protection and Recovery of Health, the Organization and Operation of the Corresponding Services and other Measures. Official Gazette. 19 September 1990. Available online: http://www.planalto.gov.br/ccivil_03/leis/l8080.htm (accessed on 12 January 2019).
- Presidency of the Republic. Civil House. Subchefia for Legal Affairs. Constituição Da República Federativa Do Brasil De. Official Gazette. 5 October 1988. Available online: http://www.planalto.gov.br/ccivil_03/Constituicao/DOUconstituicao88.pdf (accessed on 12 January 2019).
- Ordinance No. 2439 of 8 December 2005. Establishes the National Cancer Care Policy. Available online: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2005/prt2439_08_12_2005.html (accessed on 4 March 2016).
- Ministry of Health. Secretary of Health Care. Ordinance No. 741, of 19 December 2005. Oncology Care Network and Structure of High Complexity Oncology Units and Centers in Oncology (UNACON and CACON) and High Complexity Reference Centers in Oncology. Available online: http://bvsms.saude.gov.br/bvs/saudelegis/sas/2005/prt0741_19_12_2005.html (accessed on 17 March 2019).
- National Cancer Institute, Ministry of Health. Information for the Advancement of Breast Cancer Control Actions in Brazil, 1st ed.; National Cancer Institute, Ministry of Health: Sao Paulo, Brazil, 2010.
- Ministry of Health. Secretary of Health Care, Ordinance No. 779, of 31 December 2008. Define as the Official Information System of the Ministry of Health, To Be Used for the Provision of Computerized Data of Procedures Related to Screening and Diagnostic Confirmation of Breast Cancer, the Breast Cancer Control Information System. Available online: http://bvsms.saude.gov.br/bvs/saudelegis/sas/2008/prt0779_31_12_2008.html (accessed on 21 May 2019).
- National Cancer Institute. Integrador Registro Hospitalar de Câncer. 2016. Available online: https://irhc.inca.gov.br/RHCNet/ (accessed on 4 March 2016).
- National Cancer Institute. Hospital Registry of Cancer: Planning and Management, 2nd ed.; National Cancer Institute (INCA): Rio de Janeiro, Brazil, 2010.
- Landolsi, A.; Gahbiche, S.; Chaafii, R.; Chabchoub, I.; Bem Fatma, L.; Hochlef, M.; Gharbi, O.; Ahmed, S.B. Reasons of diagnosis delay of breast cancer in Tunisian women (160 patients in central region of Tunisia). La Tunis. Med. 2010, 88, 894–897. [Google Scholar]
- Sheppard, V.B.; Isaacs, C.; Luta, G.; Willey, S.C.; Boisvert, M.; Harper, F.W.K.; Smith, K.; Horton, S.; Liu, M.C.; Jennings, Y.; et al. Narrowing Racial Gaps in Breast Cancer Chemotherapy Initiation: The Role of the Patient-Provider Relationship. Breast Cancer Res. Treat. 2013, 139, 207–216. [Google Scholar] [CrossRef]
- Fayanju, O.M.; Jeffe, N.B.; Elmore, L.; Ksiazek, D.N.; Margenthaler, J.A. Patient and process factors associated with late-stage breast cancer diagnosis in Safety-Net patients: A pilot prospective study. Ann. Surg. Oncol. 2012, 20, 723–732. [Google Scholar] [CrossRef][Green Version]
- Innos, K.; Padrik, P.; Valvere, V.; Eelma, E.; Kütner, R.; LehtsaarJ Tekkel, M. Identifying women at risk for delayed presentation of breast cancer: A cross-sectional study in Estonia. BMC Public Health 2013, 13, 947. [Google Scholar] [CrossRef] [PubMed]
- Memon, Z.A.; Shaikh, A.N.; Rizwan, S.; Sardar, M.B. Reasons for Patient’s Delay in Diagnosis of Breast Carcinoma in Pakistan. Asian Pac. J. Cancer Prev. 2013, 14, 7409–7414. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Shafique, S.; Khan, M.T.; Shahzad, M.F.; Iqbal, S. Presentation delay in breast cancer patients, identifying the barriers in North Pakistan. Asian Pac. J. Cancer Prev. 2015, 16, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Ghazali, S.M.; Othman, Z.; Cheong, K.C.; Hock, L.K.; Rozita, W.; Mahiyuddin, W.; Kamaluddin, M.A.; Yusoff, A.F.; Mustafa, A.N. Non-Practice of Breast Self Examination and Marital Status are Associated with Delayed Presentation with Breast Cancer. Asian Pac. J. Cancer Prev. 2013, 14, 1141–1145. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, A.G.; Perez-Stable, E.J.; A Talavera, G.; Penedo, F.J.; Carrillo, J.E.; Fernandez, M.E.; Munoz, E.; Parma, D.L.; Holden, A.E.C.; De Majors, S.S.M.; et al. Time to definitive diagnosis of breast cancer in Latina and non-Hispanic white women: The six cities study. SpringerPlus 2013, 2, 84. [Google Scholar] [CrossRef] [PubMed]
- George, P.; Chandwani, S.; Gabel, M.; Ambrosone, C.B.; Rhoads, G.; Bandera, E.V.; Demissie, K. Diagnosis and Surgical Delays in African American and White Women with Early-Stage Breast Cancer. J. Women’s Health 2015, 24, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Presidency of the Republic. Lei No. 8080/90, de 19 de Setembro de 1990. Dispõe Sobre as Condições Para a Promoção, Proteção e Recuperação da Saúde, a Organização e o Funcionamento dos Serviços Correspondentes e dá Outras Providências; Presidency of the Republic: Brasília, Brazil, 1990. [Google Scholar]
- Figueiredo, F.W.D.S.; Almeida, T.C.D.C.; Cardial, D.T.; Maciel, E.D.S.; Fonseca, F.L.A.; Adami, F. The role of health policy in the burden of breast cancer in Brazil. BMC Women’s Health 2017, 17, 121. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. More Health: Everyone’s Right. 2007. Available online: http://bvsms.saude.gov.br/bvs/pacsaude/programa.php (accessed on 4 January 2019).
- Unger-Saldaña, K. Challenges to the early diagnosis and treatment of breast cancer in developing countries. World J. Clin. Oncol. 2014, 5, 465–477. [Google Scholar] [CrossRef]
- Sharma, K.; Costas, A.; Shulman, L.N.; Meara, J.G. A Systematic Review of Barriers to Breast Cancer Care in Developing Countries Resulting in Delayed Patient Presentation. J. Oncol. 2012, 2012, 1–8. [Google Scholar] [CrossRef]
- Richards, M.A.; Smith, P.; Ramirez, A.J.; Fentiman, I.S.; Rubens, R.D. The influence on survival of delay in the presentation and treatment of symptomatic breast cancer. Br. J. Cancer 1999, 79, 858–864. [Google Scholar] [CrossRef]
- Gebrim, L.H. A detecção precoce do câncer de mama no Brasil. Cadernos Saúde Pública 2016, 32. [Google Scholar] [CrossRef]
- Figueiredo, F.W.D.S.; Cardial, D.T.; Almeida, T.C.D.C.; Cardial, C.D.S.; De Carvalho, L.E.W.; Adami, F. Socioeconomic changes in Brazil impacted breast cancer indexes at the beginning of the 21st century? J. Cancer Policy 2018, 16, 39–42. [Google Scholar] [CrossRef]
- Figueiredo, F.W.D.S.; Adami, F. Income Inequality and Mortality Owing to Breast Cancer: Evidence from Brazil. Clin. Breast Cancer 2018, 18, e651–e658. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | n | % |
|---|---|---|
| Entry Status | ||
| Group I—No Diagnosis/No Treatment (referred to hospital for diagnosis) | 64,689 | 42.6 |
| Group II—With Diagnosis/No Treatment (referred to hospital for treatment) | 58,575 | 38.5 |
| Group III—With Diagnosis/With Treatment (referred to hospital for continued treatment) | 28,667 | 18.9 |
| Stage | ||
| I | 19,972 | 17.6 |
| II | 45,954 | 40.6 |
| III | 36,549 | 32.2 |
| IV | 10,816 | 9.6 |
| Routing Source | ||
| UHS | 100,168 | 74.7 |
| Private health plan | 28,152 | 21.0 |
| Of own accord | 5796 | 4.3 |
| Family history of breast cancer | ||
| No | 5333 | 5.6 |
| Yes | 44,704 | 47.5 |
| No information | 44,142 | 46.9 |
| Time between diagnosis and treatment | ||
| ≤60 days | 100,984 | 81.6 |
| >60 days | 22,814 | 18.4 |
| Characteristic | n | % |
|---|---|---|
| Region | ||
| North | 6837 | 4.4 |
| Northeast | 48,712 | 31.3 |
| Midwest | 7237 | 4.7 |
| Southeast | 48,066 | 30.9 |
| South | 44,567 | 28.7 |
| Marital status | ||
| Single | 31,589 | 23.4 |
| Married | 71,781 | 53.1 |
| Widowed/Divorced | 31,735 | 23.5 |
| Education | ||
| None | 11,438 | 10.5 |
| Elementary School | 65,501 | 60.0 |
| High School | 21,410 | 19.6 |
| Higher Education | 10,723 | 9.9 |
| Race | ||
| Nonwhite | 77,306 | 49.7 |
| White | 78,113 | 50.3 |
| Age group (years) | ||
| 18–39 | 17,635 | 11.3 |
| 40–49 | 40,664 | 26.2 |
| 50–69 | 71,790 | 46.2 |
| ≥70 | 25,330 | 16.3 |
| Characteristic | Diagnosis to Treatment ≥ 60 Days | Logistic Regression |
|---|---|---|
| OR (95% CI) | p-Value | |
| Age group (years) | ||
| 18–39 | ref. | ref. |
| 40–49 | 1.12 (1.06–1.18) | <0.001 |
| 50–69 | 1.28 (1.21–1.34) | <0.001 |
| ≥70 | 1.29 (1.21–1.36) | <0.001 |
| Race | ||
| Nonwhite | ref. | ref. |
| White | 0.95 (0.94–0.97) | <0.001 |
| Education level | ||
| None | ref. | ref. |
| Elementary School | 1.15 (1.10–1.21) | <0.001 |
| High School | 1.00 (0.94–1.07) | 0.862 |
| Higher Education | 1.04 (0.97–1.13) | 0.234 |
| Region | ||
| Northern | ref. | ref. |
| Northeast | 0.53 (0.50–0.57) | <0.001 |
| Midwest | 0.35 (0.32–0.38) | <0.001 |
| Southeast | 0.71 (0.66–0.76) | <0.001 |
| South | 0.80 (0.75–0.85) | <0.001 |
| Routing Source | ||
| UHS | ref. | ref. |
| Private/health plan | 0.93 (0.90–0.97) | 0.001 |
| Of own accord | 0.35 (0.32–0.39) | <0.001 |
| Stage | ||
| I | ref. | ref. |
| II | 0.96 (0.91–1.01) | 0.076 |
| III | 0.73 (0.69–0.77) | <0.001 |
| IV | 0.70 (0.65–0.75) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, N.A.S.; Schoueri, J.H.M.; Sorpreso, I.C.E.; Adami, F.; dos Santos Figueiredo, F.W. Waiting Time between Breast Cancer Diagnosis and Treatment in Brazilian Women: An Analysis of Cases from 1998 to 2012. Int. J. Environ. Res. Public Health 2020, 17, 4030. https://doi.org/10.3390/ijerph17114030
Ferreira NAS, Schoueri JHM, Sorpreso ICE, Adami F, dos Santos Figueiredo FW. Waiting Time between Breast Cancer Diagnosis and Treatment in Brazilian Women: An Analysis of Cases from 1998 to 2012. International Journal of Environmental Research and Public Health. 2020; 17(11):4030. https://doi.org/10.3390/ijerph17114030
Chicago/Turabian StyleFerreira, Naidhia Alves Soares, Jean Henri Maselli Schoueri, Isabel Cristina Esposito Sorpreso, Fernando Adami, and Francisco Winter dos Santos Figueiredo. 2020. "Waiting Time between Breast Cancer Diagnosis and Treatment in Brazilian Women: An Analysis of Cases from 1998 to 2012" International Journal of Environmental Research and Public Health 17, no. 11: 4030. https://doi.org/10.3390/ijerph17114030
APA StyleFerreira, N. A. S., Schoueri, J. H. M., Sorpreso, I. C. E., Adami, F., & dos Santos Figueiredo, F. W. (2020). Waiting Time between Breast Cancer Diagnosis and Treatment in Brazilian Women: An Analysis of Cases from 1998 to 2012. International Journal of Environmental Research and Public Health, 17(11), 4030. https://doi.org/10.3390/ijerph17114030