Temporary Disability Pension, RTW-Intentions, and RTW-Behavior: Expectations and Experiences of Disability Pensioners over 17 Months



Abstract
1. Introduction
- (1)
- What is the likelihood of returning to work (RTW) when receiving temporary disability pension (TDP) in Germany, and what are the characteristics of those who returned to work?
- (2)
- What is the relationship between RTW-behavior and RTW-intention?
- (3)
- Is there an association between the duration of TDP and RTW-intention?
- (4)
- What socio-demographic and psychological factors predict RTW-intention?
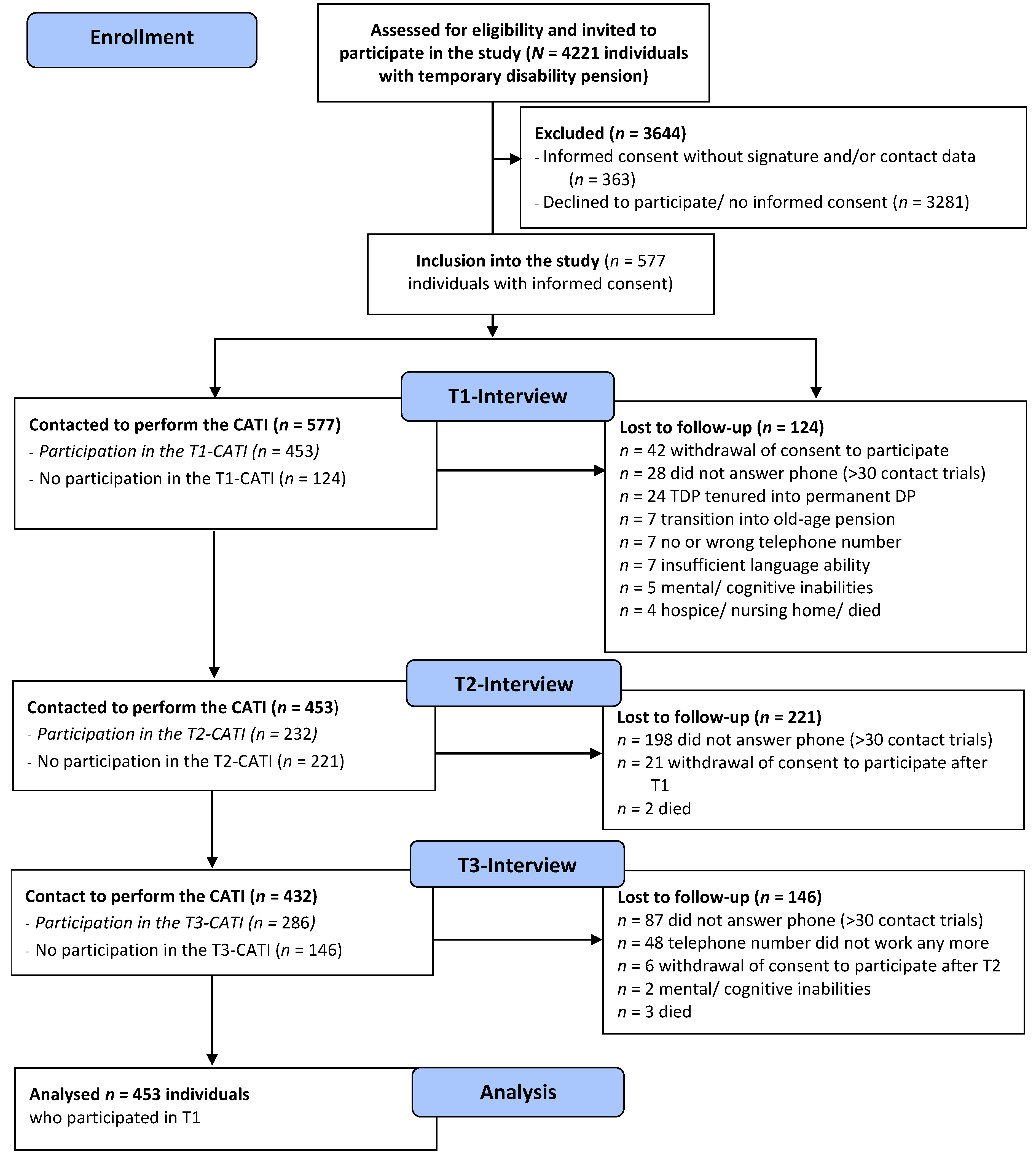
2. Materials and Methods
2.1. Measurements
2.2. Analyses
3. Results
3.1. Research Question 1: What is the Likelihood of Returning to Work (RTW) when Receiving a Temporary Disability Pension (TDP) in Germany, and What are the Characteristics of those who Returned to Work?
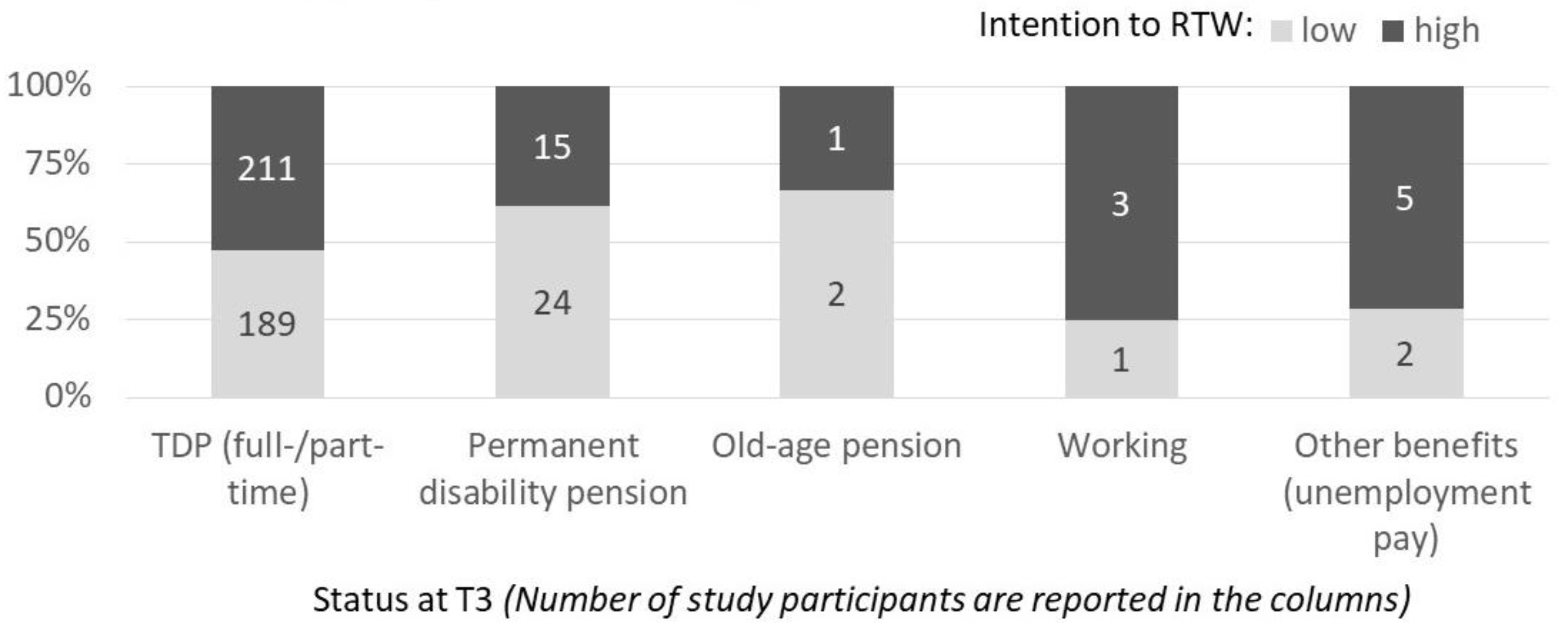
3.2. Research Question 2: How does RTW-Behavior Relate to RTW-Intention?
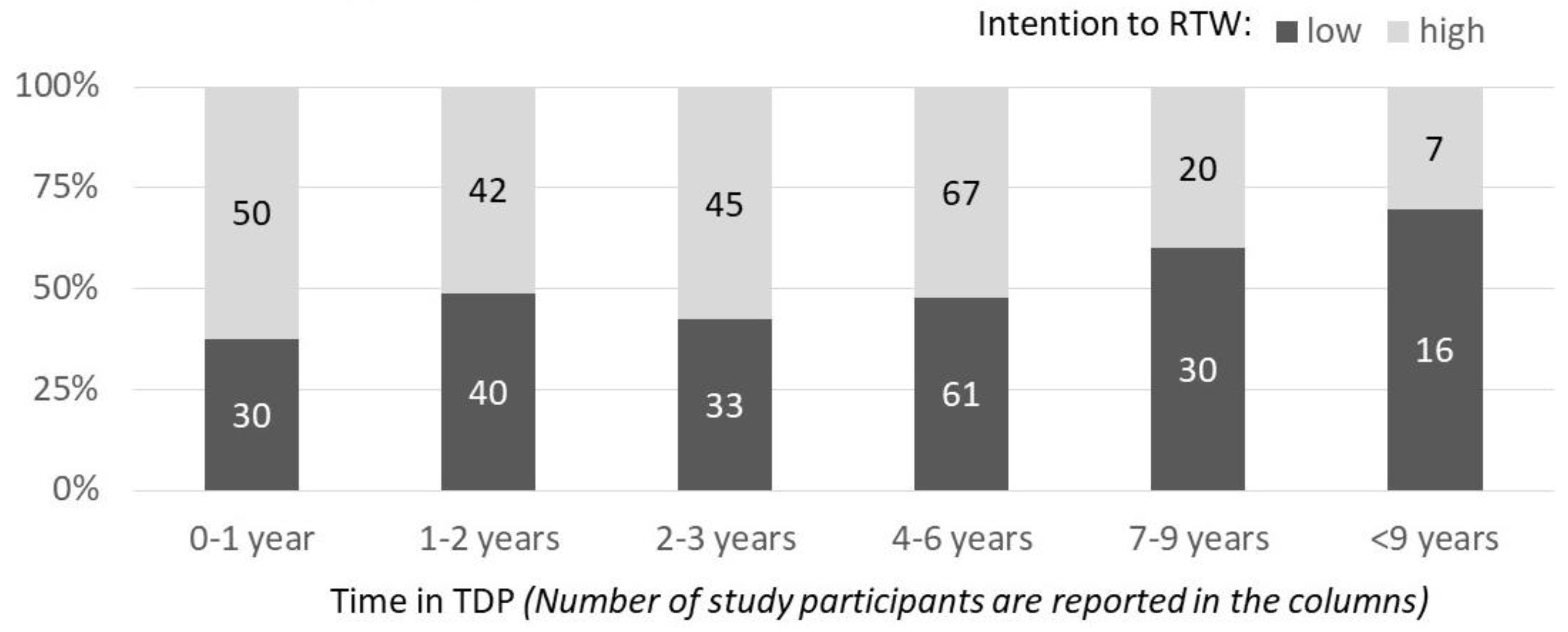
3.3. Research Question 3: Is There an Association between the Duration of TDP and the RTW-Intention?
3.4. Research Question 4: What Socio-Demographic and Psychological Factors Predict a High RTW-Intention?
4. Discussion
5. Conclusions
- Medical and vocational rehabilitation should be offered to a larger amount of disability pensioners in order to try to improve currently suboptimal RTW rates. Because RTW appeared to be related to previous RTW-intention, this should be considered when improving medical and vocational rehabilitation.
- RTW is more likely in the individuals who are younger and in TDP for a shorter period of time. However, these two factors appear to be rather independent of one another and rehabilitation should be offered as soon as possible, especially to younger people.
- Those who are younger and have been in TDP for less time have a higher RTW-intention. More effort has to be put into rehabilitation to help disability pensioners, especially those in older age, to increase their intention to RTW.
- Self-efficacy and OE to earn money, feel needed, and get a break from their family/home environment are important in the development of RTW-intentions. This should be addressed in rehabilitation with information and behavior change interventions.
- Good health is central to RTW-intention. (Work-related) medical rehabilitation can facilitate overcoming disability challenges and improving health status.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Overland, S.; Glozier, N.; Henderson, M.; Maeland, J.G.; Hotopf, M.; Mykletun, A. Health status before, during and after disability pension award: The hordaland health study (HUSK). Occup. Environ. Med. 2008, 65, 769–773. [Google Scholar] [CrossRef] [PubMed]
- Bethge, M. Work-related medical rehabilitation. Rehabilitation 2017, 56, 14. [Google Scholar] [CrossRef] [PubMed]
- Buschmann-Steinhage, R. Trends in der medizinischen Rehabilitation [Trends in medical rehabilitation]. Bundesgesundheitsblatt 2017, 60, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Knardahl, S.; Johannessen, H.A.; Sterud, T.; Harma, M.; Rugulies, R.; Seitsamo, J.; Borg, V. The contribution from psychological, social, and organizational work factors to risk of disability retirement: A systematic review with meta-analyses. BMC Public Health 2017, 17, 176. [Google Scholar] [CrossRef] [PubMed]
- Nigatu, Y.T.; Liu, Y.; Uppal, M.; McKinney, S.; Gillis, K.; Rao, S.; Wang, J. Prognostic factors for return to work of employees with common mental disorders: A meta-analysis of cohort studies. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 1205–1215. [Google Scholar] [CrossRef] [PubMed]
- Carrolli, C.; Rick, J.; Pilgrim, H.; Cameron, J.; Hillage, J. Workplace involvement improves return to work rates among employees with back pain on long-term sick leave: A systematic review of the effectiveness and cost-effectiveness of interventions. Disabil. Rehabil. 2010, 32, 607–621. [Google Scholar] [CrossRef] [PubMed]
- Haukenes, I.; Löve, J.; Hensing, G.; Knudsen, A.K.; Øverland, S.; Vahtera, J.; Sivertsen, B.; Tell, G.S.; Skogen, J.C. Inequity in disability pension: An intersectional analysis of the co-constitution of gender, education and age. the hordaland health study. Crit Public Health 2019, 29, 302–313. [Google Scholar] [CrossRef]
- Magnussen, L.; Strand, L.I.; Skouen, J.S.; Eriksen, H.R. Motivating disability pensioners with back pain to return to work—A randomized controlled trial. J. Rehabil. Med. 2007, 39, 81–87. [Google Scholar] [CrossRef] [PubMed]
- UN-CRPD—United Nations (2006). Convention on the Rights of Persons with Disabilities. Available online: http://www.un.org/disabilities/documents/convention/convoptprot-e.pdf (accessed on 21 September 2019).
- Van den Berg, T.I.; Elders, L.A.; Burdorf, A. Influence of health and work on early retirement. J. Occup. Environ. Med. 2010, 52, 576–583. [Google Scholar] [CrossRef]
- Lippke, S.; Pomp, S.; Fleig, L. Rehabilitants’ conscientiousness as a moderator of the intention-planning-behavior chain. Rehabil. Psychol. 2018, 63, 460–467. [Google Scholar] [CrossRef]
- Landstad, B.J.; Wendelborg, C.; Hedlund, M. Factors explaining return to work for long-term sick workers in Norway. Disabil. Rehabil. 2009, 31, 1215–1226. [Google Scholar] [CrossRef] [PubMed]
- Tan, V.; Cheatle, M.D.; Mackin, S.; Moberg, P.J.; Esterhai, J.L., Jr. Goal setting as a predictor of return to work in population of chronic musculoskeletal pain patients. Int. J. Neurosci. 1997, 92, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Storm, V.; Paech, J.; Ziegelmann, J.P.; Lippke, S. Physical exercise, sickness absence and subjective employability: An 8-year longitudinal observational study among musculoskeletal patients. J. Rehabil. Med. 2016, 48, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Lammerts, L.; Van Dongen, J.M.; Schaafsma, F.G.; Van Mechelen, W.; Anema, J.R. A participatory supportive return to work program for workers without an employment contract, sick-listed due to a common mental disorder: An economic evaluation alongside a randomized controlled trial. BMC Public Health 2017, 17, 162. [Google Scholar] [CrossRef]
- Ota, A.; Fujisawa, A.; Kawada, K.; Yatsuya, H. Recent status and methodological quality of return-to-work rates of cancer patients reported in Japan: A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 1461. [Google Scholar] [CrossRef]
- Mika, T. Consequences of interrupted employment careers on early retirement and pension entitlements. Z. Gerontol. Geriatr. 2019, 52, 78–90. [Google Scholar] [CrossRef]
- Dekkers-Sanchez, P.M.; Wind, H.; Sluiter, J.K.; Frings-Dresen, M.H. What factors are most relevant to the assessment of work ability of employees on long-term sick leave? The physicians’ perspective. Int. Arch. Occup. Environ. Health 2013, 86, 509–518. [Google Scholar] [CrossRef]
- Berglind, H.; Gerner, U. Motivation and return to work among the long-term sicklisted: An action theory perspective. Disabil. Rehabil. 2002, 24, 719–726. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. The job demands-resources model: State of the art. J. Manag. Psychol. 2007, 22, 309–328. [Google Scholar] [CrossRef]
- Haveraaen, L.A.; Skarpaas, L.S.; Berg, J.E.; Aas, R.W. Do psychological job demands, decision control and social support predict return to work three months after a return-to-work (RTW) programme? The rapid-RTW cohort study. Work 2016, 53, 61–71. [Google Scholar] [CrossRef]
- Topa, G.; Depolo, M.; Alcover, C.M. Early retirement: A meta-analysis of its antecedent and subsequent correlates. Front. Psychol. 2018, 8, 2157. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Asih, S.R.; Polatin, P.B. Understanding motivation to return to work: The economy of gains and losses. In Handbook of Return to Work; Schultz, I.Z., Gatchel, R.J., Eds.; Springer: Boston, MA, USA, 2016; pp. 67–79. [Google Scholar]
- Märtin, S. Materielle Absicherung bei Erwerbsminderung im Kontext der Lebensform: Eine Empirische Analyse auf Basis von Befragungs- und Routinedaten (Material Protection in the Context of Reduced Earning Capacity in the Form of Life: An Empirical Analysis Based on Survey and Routine Data); Springer-Verlag: Berlin, Germany, 2017. [Google Scholar]
- Laaksonen, M.; Gould, R. Return to work after temporary disability pension in Finland. J. Occup. Rehabil. 2015, 25, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Zschucke, E.; Hessel, A.; Lippke, S. Befristete Erwerbsminderungsrente aus Sicht der Betroffenen: Subjektiver Gesundheitszustand, Rehabilitationserfahrungen und Pläne zur Rückkehr ins Erwerbsleben (Temporary disability pension from the perspective of the individual: Self-reported physical and mental health, medical rehabilitation, and return to work plans). Rehabilitation 2016, 55, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Kobelt, A.; Grosch, E.; Hesse, B.; Gebauer, E.; Gutenbrunner, C. Do people with mental disorders who, due to complete reduction in earning capacity, receive a temporary pension want to return into active employment? Psychother. Psychosom. Med. Psychol. 2009, 59, 273–280. [Google Scholar] [CrossRef]
- Köckerling, E.; Sauzet, O.; Hesse, B.; Körner, M.; Razum, O. Return to work aus einer zeitlich befristeten Erwerbsminderungsrente (Return to work after temporary disability pension). Gesundheitswesen 2019. efirst. [Google Scholar] [CrossRef]
- Ahlgren, A.; Broman, L.; Bergroth, A.; Ekholm, J. Disability pension despite vocational rehabilitation? A study from six social insurance offices of a county. Int. J. Rehabil. Res. 2005, 28, 33–42. [Google Scholar] [CrossRef]
- Dunstan, D.A.; Covic, T.; Tyson, G.A. What leads to the expectation to return to work? Insights from a theory of planned behavior (TPB) model of future work outcomes. Work 2013, 46, 25–37. [Google Scholar] [CrossRef]
- Drews, B.; Nielsen, C.V.; Rasmussen, M.S.; Hjort, J.; Bonde, J.P. Improving motivation and goal setting for return to work in a population on sick leave: A controlled study. Scand. J. Public Health 2007, 35, 86–94. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| T1: All Study Participants Were in TDP | T3 | Total | |||||
|---|---|---|---|---|---|---|---|
| TDP (Full-/Part-Time) | Permanent Disability Pension | Old-age Pension | Working | Other Benefits (Unemploy-Ment Pay) | |||
| T2 TDP (full-/part-time) | number | 396 (149) | 26 (8) | 1 (1) | 3 (1) | 4 (2) | 430 (161) |
| % | 87.4% (86.1%) | 5.7% (4.6%) | 0.2% (0.6%) | 0.7% (0.6%) | 0.9% (1.2%) | 94.9% (93.1%) | |
| Permanent disability pension | number | 3 (3) | 13 (5) | 0 (0) | 0 (0) | 0 (0) | 16 (8) |
| % | 0.7% (1.7%) | 2.9% (2.9%) | 0% (0%) | 0% (0%) | 0% (0%) | 3.5% (4.6%) | |
| Old-age pension | number | 0 (0) | 0 (0) | 2 (2) | 0 (0) | 0 (0) | 2 (2) |
| % | 0% (0%) | 0% (0%) | 0.4% (1.2%) | 0% (0%) | 0% (0%) | 0.4% (1.2%) | |
| Working | number | 0 (0) | 0 (0) | 0 (0) | 1 (0) | 0 (0) | 1 (0) |
| % | 0% (0%) | 0% (0%) | 0% (0%) | 0.2% (0) | 0% (0%) | 0.2% (0%) | |
| Other benefits (unemployment pay) | number | 1 (1) | 0 (0) | 0 (0) | 0 (0) | 3 (1) | 4 (2) |
| % | 0.2% (0.6%) | 0% (0%) | 0% (0%) | 0% (0%) | 0.7% (1.7%) | 0.9% (1.2%) | |
| Total | number | 400 (153) | 39 (13) | 3 (3) | 4 (1) | 7 (3) | 453 (173) |
| % | 88.3% (88.4%) | 8.6% (7.5%) | 0.7% (1.7%) | 0.9% (0.6%) | 1.5% (1.7%) | 100.0% (100%) | |
| Characteristics | TDP (Full-/Part-Time) | Permanent Disability Pension | Old-age Pension | Working | Other Benefits (Unemploy-Ment Pay) | Total |
|---|---|---|---|---|---|---|
| N ≤ 400 | N ≤ 39 | N ≤ 3 | N ≤ 4 | N ≤ 7 | N ≤ 453 | |
| Gender (males) | 178 (44.5%) | 22 (56.4%) | 2 (66.7%) | 3 (75%) | 5 (71.4%) | 210 (46.4%) |
| Age (in years) | 49.96 (7.89) 27–63 | 53.85 (6.58) 35–62 | 61.67 (3.06) 59–65 | 46.00 (12.73) 28–58 | 52.43 (6.27) 41–59 | 50.38 (7.90) 27–65 |
| Body Mass Index | 29.23 (7.45) 16.53–60.14 | 27.09 (5.14) 17.32–38.70 | 27.51 (4.97) 23.99–31.02 | 27.87 (3.14) 24.93–31.56 | 32.98 (8.40) 22.59–47.02 | 29.08 (7.28) 16.53–60.14 |
| Income available to the household | 2.16 (0.89) 1–4 | 2.42 (0.64) 1–4 | 2.67 (0.58) 2–3 | 2.25 (0.50) 2–3 | 1.83 (0.75) 1–3 | 2.18 (0.87) 1–4 |
| Time in TDP (months) | 40.30 (31.01) 1.00-170 | 54.90 (49.70) 6.00-277.00 | 57.00 (51.00) 6.00-108.00 | 28.25 (29.19) 12.00-72.00 | 73.29 (73.71) 9.00-218.00 | 42.08 (34.40) 1.00-277.00 |
| Pension due to full TDP | 86.7% | 90.5% | 100.0% | 50.0% | 80.0% | 86.8% |
| Subjective health | 1.99 (0.69) 1–4 | 1.85 (0.67) 1–4 | 2.67 (1.16) 2–4 | 2.25 (0.50) 2–3 | 1.71 (0.76) 1–3 | 1.98 (0.69) 1–4 |
| Children | 281 (70.6%) | 24 (63.2%) | 2 (66.7%) | 4 (100%) | 6 (85.7%) | 317 (70.4%) |
| No vocational qualification | 77 (19.3%) | 8 (20.5%) | 1 (33.3%) | 0 (0.0%) | 0 (0.0%) | 86 (19.1%) |
| Last job was……Full time | 57.0% | 56.4% | 33.3% | 75.0% | 71.4% | 57.2% |
| …Part-time | 20.3% | 12.8% | 33.3% | 25.0% | 0.0% | 19.4% |
| …By the hours/unregularly | 4.1% | 0.0% | 0.0% | 0.0% | 0.0% | 3.3% |
| …Unemploy-ment pay/ | 12.3% | 17.9% | 33.3% | 0.0% | 28.6% | 12.3% |
| …Homemaker/Caretaking 1 | 2.8% | 5.1% | 0.0% | 0.0% | 0.0% | 2.9% |
| Participation in medical rehabilitation | 248 (62.0%) | 26 (66.7%) | 2 (66.7%) | 0 (0.0%) | 5 (71.4%) | 281 (62.0%) |
| Predictor Variables | Step 1 Prediction T1 RTW-Intention 1 | Step 2 Prediction T1 RTW-Intention 1 | Step 3 Prediction T3 RTW-Intention Change 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI for Lower | 95% CI for Upper | OR | 95% CI for Lower | 95% CI for Upper | OR | 95% CI for Lower | 95% CI for Upper | |
| Sex | 1.259 | 0.760 | 2.086 | 0.967 | 0.549 | 1.705 | 0.763 | 0.315 | 1.848 |
| Age | 0.930** | 0.899 | 0.962 | 0.947** | 0.912 | 0.983 | 0.909** | 0.857 | 0.964 |
| Body Mass Index | 1.017 | 0.982 | 1.054 | 1.015 | 0.975 | 1.056 | 1.015 | 0.960 | 1.073 |
| Time in TDP | 0.782* | 0.645 | 0.947 | 0.790* | 0.640 | 0.977 | 0.825 | 0.600 | 1.135 |
| Income available to the household | 0.753* | 0.566 | 0.999 | 0.951 | 0.678 | 1.335 | 1.552 | 0.947 | 2.544 |
| Self-efficacy | 1.261** | 1.106 | 1.438 | 1.139 | 0.981 | 1.322 | 1.073 | 0.850 | 1.354 |
| Social support | 1.062 | 0.970 | 1.163 | 1.018 | 0.920 | 1.126 | 0.962 | 0.840 | 1.101 |
| Job autonomy | 1.108 | 0.881 | 1.394 | 1.069 | 0.829 | 1.379 | 1.213 | 0.817 | 1.802 |
| Job demand | 1.044 | 0.822 | 1.326 | 1.023 | 0.785 | 1.334 | 0.923 | .621 | 1.371 |
| OE to earn money | 1.987** | 1.295 | 3.048 | 1.673 | 0.874 | 3.201 | |||
| OE to feel needed | 1.710** | 1.143 | 2.558 | 1.174 | 0.554 | 2.490 | |||
| OE enjoyment of work | 0.983 | 0.585 | 1.652 | 1.505 | 0.563 | 4.024 | |||
| OE to get a break | 1.409* | 1.058 | 1.876 | 1.393 | 0.886 | 2.189 | |||
| Subjective health | 0.990 | 0.643 | 1.526 | 2.369* | 1.182 | 4.749 | |||
| Expectation of medical rehabilitation | 1.547** | 1.186 | 2.017 | 1.330 | 0.918 | 1.926 | |||
| T1 RTW-Intention | 1.742 | 0.698 | 4.347 | ||||||
| R2 | 0.20 | 0.37 | 0.32 | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lippke, S.; Schüz, N.; Zschucke, E. Temporary Disability Pension, RTW-Intentions, and RTW-Behavior: Expectations and Experiences of Disability Pensioners over 17 Months. Int. J. Environ. Res. Public Health 2020, 17, 238. https://doi.org/10.3390/ijerph17010238
Lippke S, Schüz N, Zschucke E. Temporary Disability Pension, RTW-Intentions, and RTW-Behavior: Expectations and Experiences of Disability Pensioners over 17 Months. International Journal of Environmental Research and Public Health. 2020; 17(1):238. https://doi.org/10.3390/ijerph17010238
Chicago/Turabian StyleLippke, Sonia, Natalie Schüz, and Elisabeth Zschucke. 2020. "Temporary Disability Pension, RTW-Intentions, and RTW-Behavior: Expectations and Experiences of Disability Pensioners over 17 Months" International Journal of Environmental Research and Public Health 17, no. 1: 238. https://doi.org/10.3390/ijerph17010238
APA StyleLippke, S., Schüz, N., & Zschucke, E. (2020). Temporary Disability Pension, RTW-Intentions, and RTW-Behavior: Expectations and Experiences of Disability Pensioners over 17 Months. International Journal of Environmental Research and Public Health, 17(1), 238. https://doi.org/10.3390/ijerph17010238