The Mortality Response to Absolute and Relative Temperature Extremes



Abstract
1. Introduction
2. Data and Methods
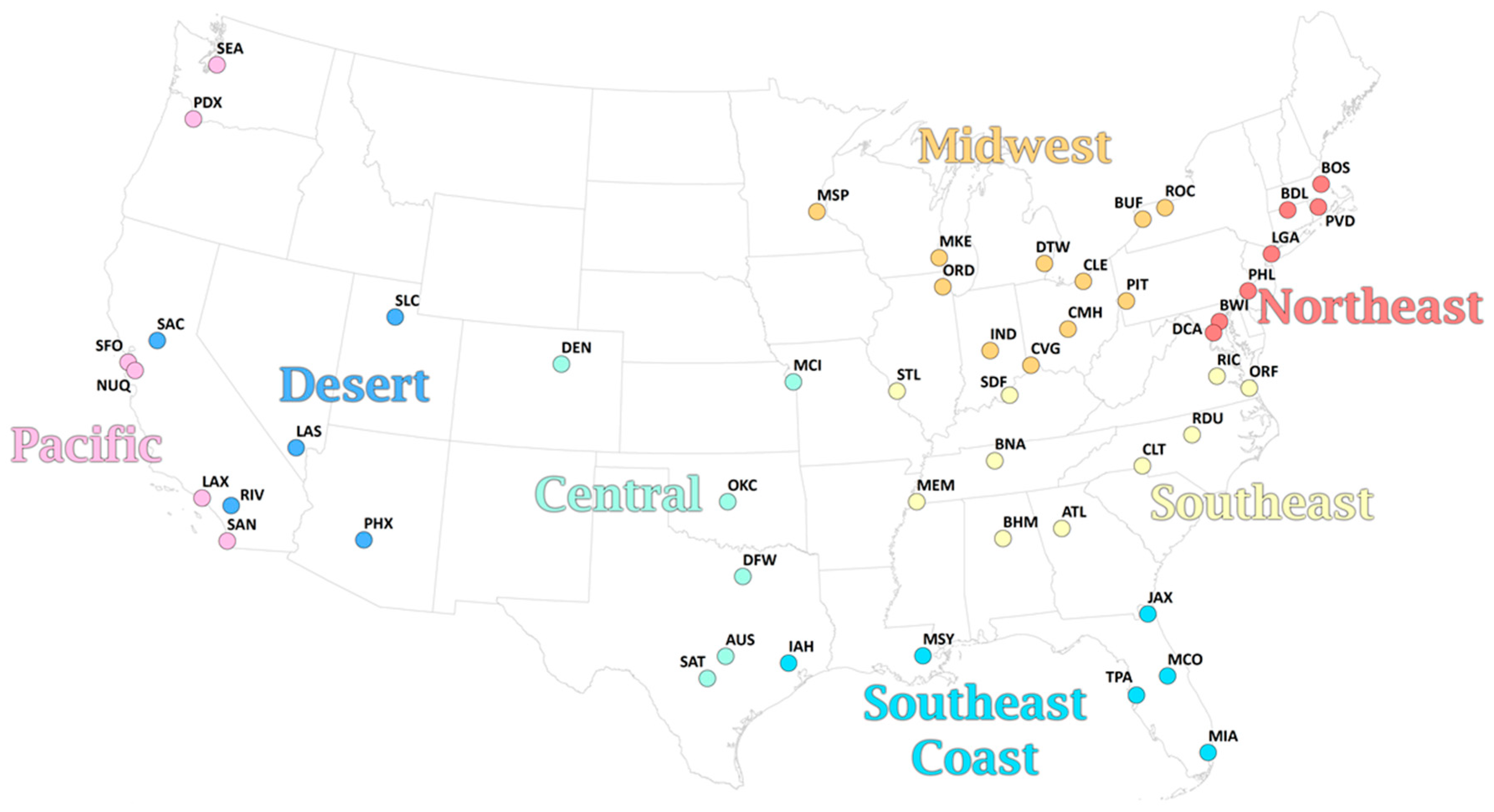
2.1. Data and Calculation of Apparent Temperature
2.2. Calculation of Extreme Events
2.3. Mortality Data
2.4. Calculating Relative Risks of Mortality
- -
- Days that were classified as EHE
- -
- Days that were classified as ECE
- -
- Days that were classified as REHE that were not also EHE, and whose mean daily apparent temperature was at or above the mean annual apparent temperature for the location
- -
- Days that were classified as RECE that were not also ECE, and whose mean daily apparent temperature was at or below the mean annual apparent temperature for the location
- mortality is the daily all-cause mortality total for the metropolitan area, assuming a Poisson distribution of counts;
- ns (time) is a natural spline fit to the full 36-year period with 6 degrees of freedom per year (216 degrees of freedom in total), to account for long-term changes in baseline mortality as well as seasonal variations; and
- ETE occurrence refers to an array of binary variables created for each of the four ETE definitions above, where a day on which an ETE occurred is coded as 1, and a day in which an ETE did not occur is coded as 0.
3. Results
3.1. Climatology of ETEs
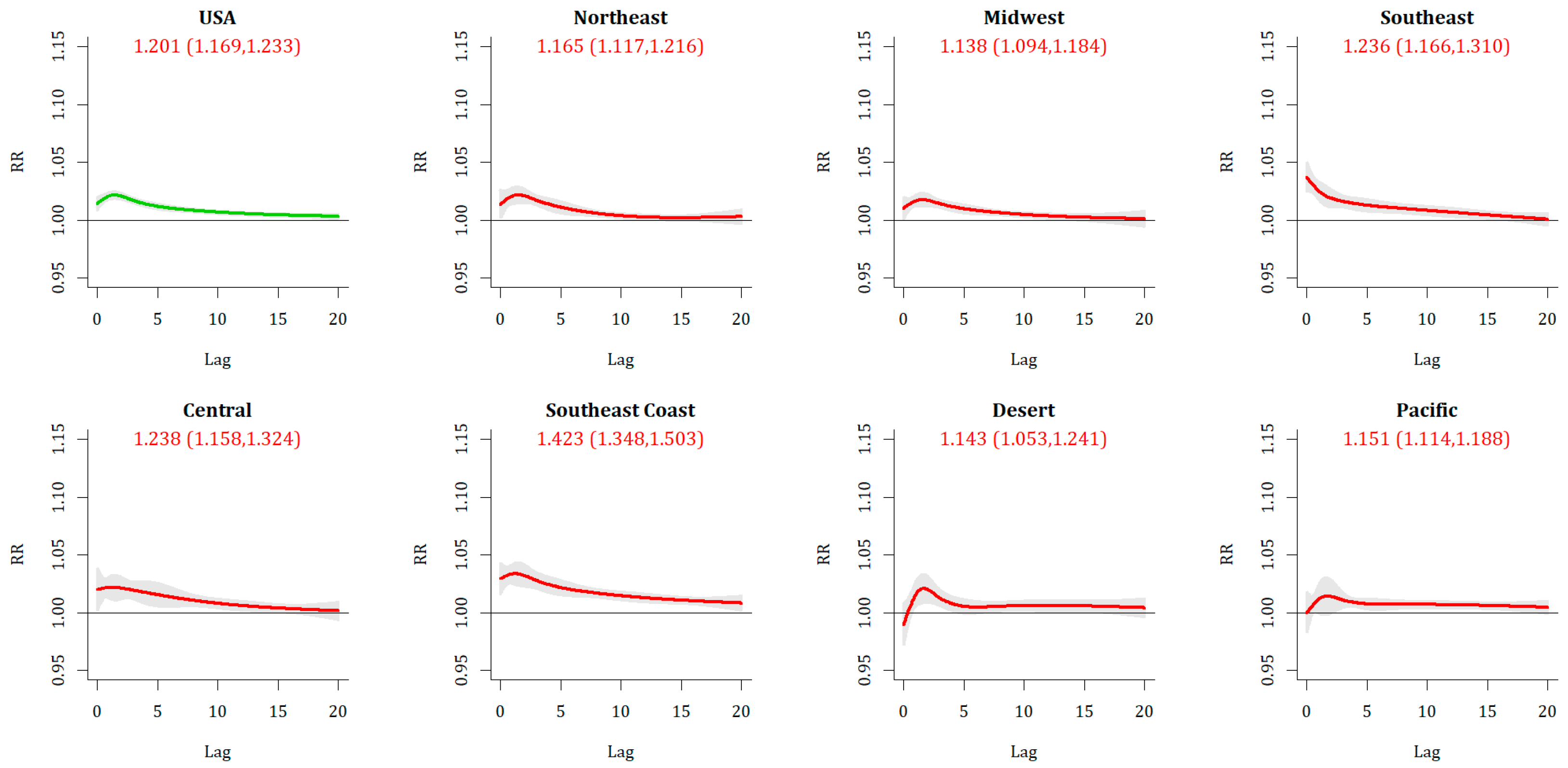
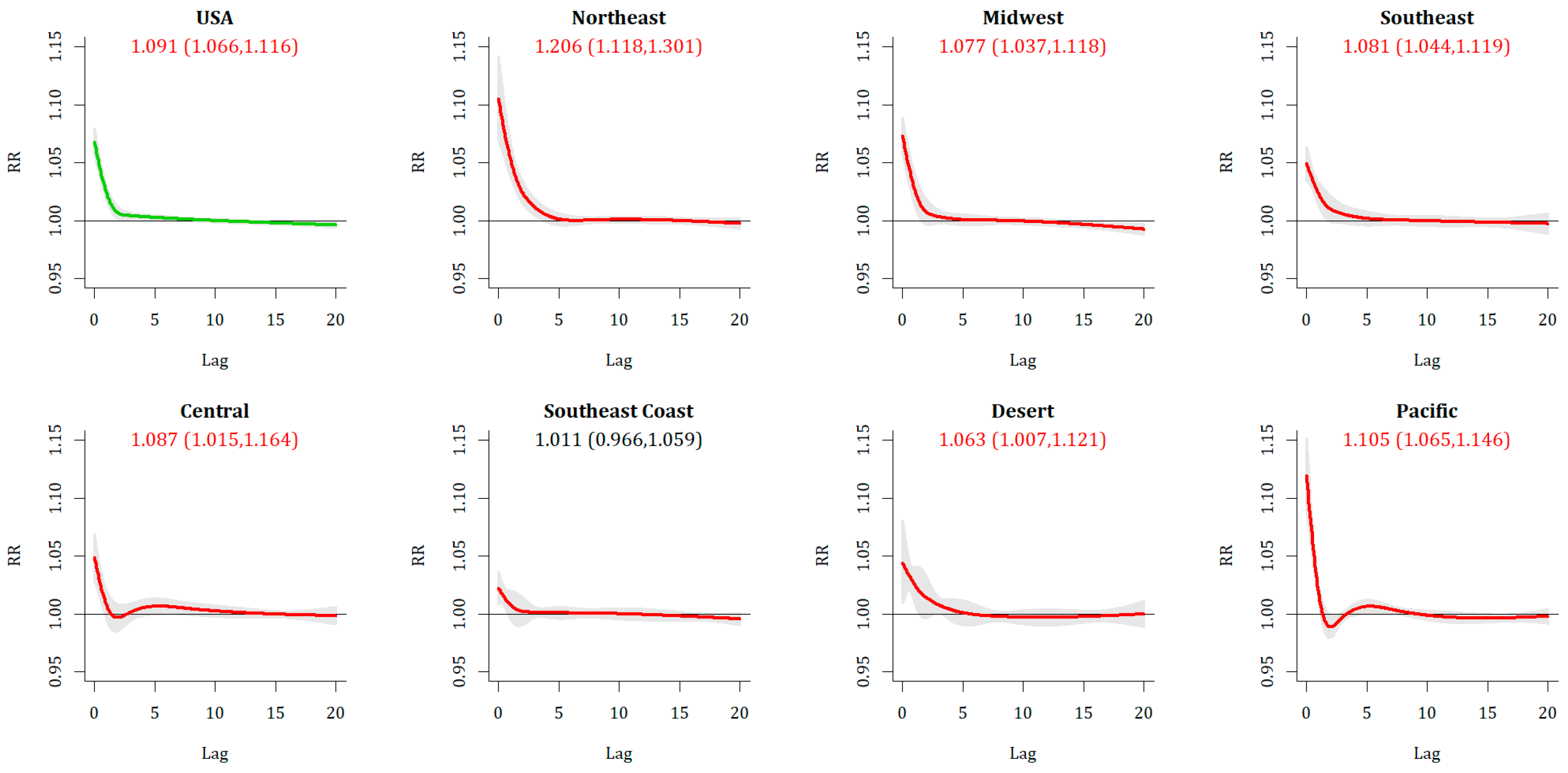
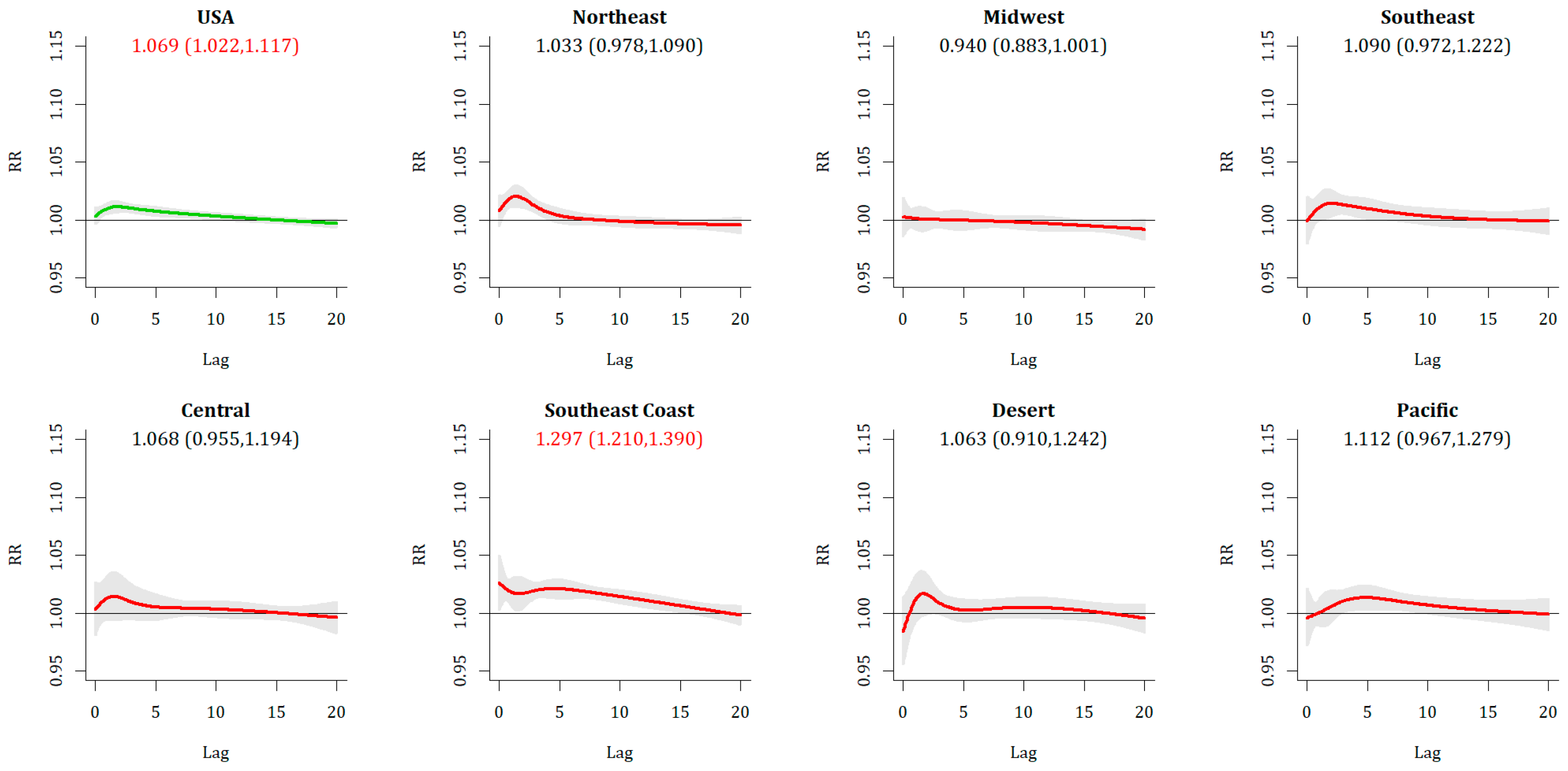
3.2. Associations between ETEs and Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Data
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Df/year; knots | RECE Relative Risk | S.S. Metrosmetros | REHE Relative Risk | S.S. Metrosmetros |
|---|---|---|---|---|
| 6, 2 | 1.070 (1.023, 1.118) | 11 | 0.886 (0.864, 0.909) | 0 |
| 7, 2 | 1.083 (1.037, 1.130) | 13 | 0.893 (0.869, 0.918) | 0 |
| 8, 2 | 1.090 (1.047, 1.135) | 9 | 0.884 (0.860, 0.908) | 0 |
| 6, 3 * | 1.069 (1.022, 1.117) | 12 | 0.890 (0.867, 0.913) | 0 |
| 7, 3 | 1.081 (1.036, 1.129) | 13 | 0.897 (0.872, 0.922) | 0 |
| 8, 3 | 1.089 (1.045, 1.134) | 9 | 0.888 (0.864, 0.912) | 0 |
| 6, 4 | 1.068 (1.022, 1.117) | 12 | 0.890 (0.867, 0.913) | 0 |
| 7, 4 | 1.081 (1.035, 1.129) | 13 | 0.897 (0.872, 0.922) | 0 |
| 8, 4 | 1.088 (1.045, 1.133) | 9 | 0.888 (0.864, 0.912) | 0 |
References
- Anderson, B.G.; Bell, M.L. Heat waves in the United States: Mortality risk during heat waves and effect modification by heat wave characteristics in 43 U.S. communities. Environ. Health Perspect. 2010, 119, 210–218. [Google Scholar] [CrossRef]
- Hajat, S.; Kosatky, T. Heat-related mortality: A review and exploration of heterogeneity. J. Epidemiol. Community Health 2010, 64, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Basu, R. High ambient temperature and mortality: A review of epidemiologic studies from 2001 to 2008. Environ. Health 2009, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Baccini, M.; Kosatsky, T.; Biggeri, A. Impact of summer heat on urban population mortality in Europe during the 1990s: An evaluation of years of life lost adjusted for harvesting. PLoS ONE 2013, 8, e69638. [Google Scholar] [CrossRef] [PubMed]
- Saha, M.V.; Davis, R.E.; Hondula, D.M. Mortality displacement as a function of heat event strength in 7 US cities. Am. J. Epidemiol. 2013, 179, 467–474. [Google Scholar] [CrossRef]
- Arbuthnott, K.; Hajat, S.; Heaviside, C.; Vardoulakis, S. What is cold-related mortality? A multi-disciplinary perspective to inform climate change impact assessments. Environ. Int. 2018, 121, 119–129. [Google Scholar] [CrossRef]
- Kim, Y.M.; Kim, S.; Cheong, H.K.; Kim, E.H. Comparison of temperature indexes for the impact assessment of heat stress on heat-related mortality. Environ. Health Toxicol. 2011, 26, e2011009. [Google Scholar] [CrossRef]
- Urban, A.; Kyselý, J. Comparison of UTCI with other thermal indices in the assessment of heat and cold effects on cardiovascular mortality in the Czech Republic. Int. J. Environ. Res. Public Health 2014, 11, 952–967. [Google Scholar] [CrossRef]
- Steadman, R.G. A universal scale of apparent temperature. J. Clim. Appl. Meteorol. 1984, 23, 1674–1687. [Google Scholar] [CrossRef]
- Sheridan, S.C.; Allen, M.J. Changes in the frequency and intensity of extreme temperature events and human health concerns. Curr. Clim. Chang. Rep. 2015, 1, 155–162. [Google Scholar] [CrossRef]
- Sheridan, S.C.; Dixon, P.G. Spatiotemporal trends in human vulnerability and adaptation to heat across the United States. Anthropocene 2017, 20, 61–73. [Google Scholar] [CrossRef]
- Ng, C.F.S.; Ueda, K.; Ono, M.; Nitta, H.; Takami, A. Characterizing the effect of summer temperature on heatstroke-related emergency ambulance dispatches in the Kanto area of Japan. Int. J. Biometeorol. 2014, 58, 941–948. [Google Scholar] [CrossRef]
- Allen, M.J.; Sheridan, S.C. Mortality risks during extreme temperature events (ETEs) using a distributed lag non-linear model. Int. J. Biometeorol. 2018, 62, 57–67. [Google Scholar] [CrossRef]
- Smith, E.T.; Sheridan, S.C. The influence of extreme cold events on mortality in the United States. Sci. Total Environ. 2019, 647, 342–351. [Google Scholar] [CrossRef]
- Nairn, J.R.; Fawcett, R.J. The excess heat factor: A metric for heatwave intensity and its use in classifying heatwave severity. Int. J. Environ. Res. Public Health 2014, 12, 227–253. [Google Scholar] [CrossRef]
- Wilson, L.A.; Morgan, G.G.; Hanigan, I.C.; Johnston, F.H.; Abu-Rayya, H.; Broome, R.; Gaskin, C.; Jalaludin, B. The impact of heat on mortality and morbidity in the Greater Metropolitan Sydney Region: A case crossover analysis. Environ. Health 2013, 12, 98. [Google Scholar] [CrossRef]
- Hatvani-Kovacs, G.; Belusko, M.; Pockett, J.; Boland, J. Can the Excess Heat Factor indicate heatwave-related morbidity? A case study in Adelaide, South Australia. EcoHealth 2016, 13, 100–110. [Google Scholar] [CrossRef]
- Grumm, R.; Arnott, J.M.; Halblaub, J. The Epic Eastern North American Warm Episode of March 2012. J. Oper. Meteorol. 2014, 2, 36–50. [Google Scholar] [CrossRef]
- Kalkstein, A.J.; Kalkstein, L.S.; Vanos, J.K.; Eisenman, D.P.; Dixon, P.G. Heat/mortality sensitivities in Los Angeles during winter: A unique phenomenon in the United States. Environ. Health 2018, 17, 45. [Google Scholar] [CrossRef]
- Lee, C.C.; Sheridan, S.C. A new approach to modeling temperature-related mortality: Non-linear autoregressive models with exogenous input. Environ. Res. 2018, 164, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.C. A systematic evaluation of the lagged effects of spatiotemporally relative surface weather types on wintertime cardiovascular-related mortality across 19 US cities. Int. J. Biometeorol. 2015, 59, 1633–1645. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, S.C.; Lee, C.C. Temporal trends in absolute and relative extreme temperature events across North America. J. Geophys. Res. Atmos. 2018, 123, 11–889. [Google Scholar] [CrossRef]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [PubMed]
- Rocklöv, J.; Ebi, K.; Forsberg, B. Mortality related to temperature and persistent extreme temperatures: A study of cause-specific and age-stratified mortality. Occup. Environ. Med. 2011, 68, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Fuhrmann, C.M.; Sugg, M.M.; Konrad, C.E.; Waller, A. Impact of extreme heat events on emergency department visits in North Carolina (2007–2011). J. Community Health 2016, 41, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Zaninović, K.; Matzarakis, A. Impact of heat waves on mortality in Croatia. Int. J. Biometeorol. 2014, 58, 1135–1145. [Google Scholar] [CrossRef]
- Allen, M.J.; Lee, C.C. Investigating high mortality during the cold season: Mapping mean weather patterns of temperature and pressure. Theor. Appl. Climatol. 2014, 118, 419–428. [Google Scholar] [CrossRef]
- Lee, W.; Choi, H.M.; Lee, J.Y.; Kim, D.H.; Honda, Y.; Kim, H. Temporal changes in mortality impacts of heat wave and cold spell in Korea and Japan. Environ. Int. 2018, 116, 136–146. [Google Scholar] [CrossRef]
- Guirguis, K.; Gershunov, A.; Tardy, A.; Basu, R. The impact of recent heat waves on human health in California. J. Appl. Meteorol. Climatol. 2014, 53, 3–19. [Google Scholar] [CrossRef]
- Hajat, S.; Armstrong, B.G.; Gouveia, N.; Wilkinson, P. Mortality displacement of heat-related deaths: A comparison of Delhi, Sao Paulo, and London. Epidemiology 2005, 16, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Office of National Statistics. Quarterly Mortality Report, England: April to June 2018. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/quarterlymortalityreports/apriltojune2018 (accessed on 22 March 2019).
- Monier, E.; Gao, X. Climate change impacts on extreme events in the United States: An uncertainty analysis. Clim. Chang. 2015, 131, 67–81. [Google Scholar] [CrossRef]
- Oudin Åström, D.; Ebi, K.L.; Vicedo-Cabrera, A.M.; Gasparrini, A. Investigating changes in mortality attributable to heat and cold in Stockholm, Sweden. Int. J. Biometeorol. 2018, 62, 1777–1780. [Google Scholar] [CrossRef] [PubMed]





| Metropolitan Area | Airport | Pop. | Sample Sizes | AT Percentiles | ||||
|---|---|---|---|---|---|---|---|---|
| Code | (mln) | ECE | EHE | RECE | REHE | 5th | 95th | |
| Atlanta | ATL | 5.3 | 77 | 88 | 39 | 54 | −2.8 | 28.9 |
| Austin | AUS | 1.7 | 78 | 87 | 84 | 44 | 1.9 | 31.5 |
| Baltimore | BWI | 2.7 | 81 | 81 | 29 | 67 | −7.5 | 27.9 |
| Birmingham | BHM | 1.1 | 76 | 90 | 36 | 66 | −1.7 | 29.8 |
| Boston | BOS | 4.5 | 77 | 76 | 36 | 56 | −11.2 | 24.5 |
| Buffalo | BUF | 1.1 | 91 | 85 | 33 | 64 | −14.5 | 23.3 |
| Charlotte | CLT | 2.2 | 85 | 81 | 39 | 66 | −2.5 | 28.8 |
| Chicago | ORD | 9.5 | 97 | 78 | 30 | 70 | −14.6 | 25.9 |
| Cincinnati | CVG | 2.1 | 100 | 87 | 33 | 65 | −10.3 | 26.8 |
| Cleveland | CLE | 2.1 | 96 | 75 | 26 | 67 | −12.9 | 24.9 |
| Columbus | CMH | 1.9 | 99 | 75 | 26 | 69 | −11.2 | 26.5 |
| Dallas | DFW | 6.4 | 73 | 118 | 39 | 45 | −1.6 | 31.6 |
| Denver | DEN | 2.5 | 51 | 86 | 55 | 54 | −10.7 | 22.6 |
| Detroit | DTW | 4.3 | 87 | 78 | 34 | 66 | −13.6 | 25.1 |
| Hartford | BDL | 1.2 | 83 | 72 | 38 | 63 | −11.7 | 25.4 |
| Houston | IAH | 5.9 | 71 | 83 | 58 | 56 | 3.4 | 31.8 |
| Indianapolis | IND | 1.9 | 94 | 97 | 32 | 69 | −12.0 | 26.8 |
| Jacksonville | JAX | 1.3 | 71 | 103 | 50 | 56 | 3.9 | 30.2 |
| Kansas City | MCI | 2.0 | 93 | 94 | 38 | 54 | −12.2 | 28.1 |
| Las Vegas | LAS | 2.0 | 98 | 74 | 47 | 59 | 2.2 | 33.0 |
| Los Angeles | LAX | 12.8 | 96 | 98 | 42 | 78 | 9.0 | 21.8 |
| Louisville | SDF | 1.2 | 99 | 93 | 35 | 62 | −7.9 | 29.0 |
| Memphis | MEM | 1.3 | 76 | 122 | 38 | 49 | −3.6 | 31.4 |
| Miami | MIA | 5.6 | 86 | 141 | 43 | 95 | 14.6 | 31.4 |
| Milwaukee | MKE | 1.6 | 97 | 73 | 34 | 59 | −15.5 | 24.3 |
| Minneapolis | MSP | 3.3 | 92 | 85 | 35 | 69 | −20.1 | 24.9 |
| Nashville | BNA | 1.7 | 79 | 104 | 35 | 62 | −5.2 | 29.3 |
| New Orleans | MSY | 1.2 | 71 | 113 | 48 | 71 | 3.7 | 31.5 |
| New York | LGA | 19.6 | 86 | 75 | 34 | 53 | −9.4 | 26.9 |
| Oklahoma City | OKC | 1.3 | 79 | 104 | 31 | 46 | −6.7 | 29.4 |
| Orlando | MCO | 2.1 | 73 | 82 | 49 | 66 | 8.4 | 30.3 |
| Philadelphia | PHL | 6.0 | 85 | 76 | 34 | 66 | −8.6 | 27.6 |
| Phoenix | PHX | 4.2 | 105 | 82 | 61 | 58 | 8.0 | 36.1 |
| Pittsburgh | PIT | 2.4 | 84 | 85 | 32 | 69 | −11.7 | 25.0 |
| Portland | PDX | 2.2 | 94 | 78 | 26 | 51 | −1.8 | 21.2 |
| Providence | PVD | 1.6 | 84 | 79 | 37 | 51 | −10.5 | 24.8 |
| Raleigh | RDU | 1.1 | 96 | 76 | 42 | 61 | −3.3 | 28.8 |
| Richmond | RIC | 1.2 | 88 | 87 | 31 | 72 | −4.9 | 28.8 |
| Riverside | RIV | 4.2 | 95 | 87 | 55 | 81 | 5.9 | 27.2 |
| Rochester | ROC | 1.1 | 89 | 89 | 35 | 71 | −13.9 | 23.9 |
| Sacramento | SAC | 2.1 | 87 | 64 | 53 | 53 | 3.2 | 25.1 |
| Saint Louis | STL | 2.8 | 92 | 94 | 33 | 58 | −10.2 | 29.7 |
| Salt Lake City | SLC | 1.1 | 95 | 75 | 26 | 54 | −8.4 | 25.1 |
| San Antonio | SAT | 2.1 | 71 | 124 | 50 | 42 | 3.0 | 30.9 |
| San Diego | SAN | 3.1 | 92 | 113 | 51 | 74 | 10.3 | 23.3 |
| San Francisco | SFO | 4.3 | 88 | 75 | 51 | 40 | 5.1 | 16.7 |
| San Jose | NUQ | 1.8 | 57 | 66 | 60 | 35 | 6.3 | 21.1 |
| Seattle | SEA | 3.4 | 88 | 79 | 19 | 50 | −1.3 | 19.0 |
| Tampa | TPA | 2.8 | 83 | 91 | 55 | 55 | 8.9 | 31.2 |
| Virginia Beach | ORF | 1.7 | 89 | 71 | 38 | 56 | −3.9 | 28.8 |
| Washington | DCA | 5.6 | 82 | 88 | 37 | 63 | −6.2 | 29.0 |
| ETE Type | JAN | FEB | MAR | APR | MAY | JUN | JUL | AUG | SEP | OCT | NOV | DEC | ANN |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ECE | 1.17 | 0.38 | 0.05 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.05 | 0.72 | 2.37 |
| EHE | 0.00 | 0.00 | 0.00 | 0.01 | 0.02 | 0.42 | 1.23 | 0.62 | 0.12 | 0.02 | 0.00 | 0.00 | 2.44 |
| RECE | 0.01 | 0.07 | 0.17 | 0.13 | 0.05 | 0.02 | 0.00 | 0.00 | 0.06 | 0.22 | 0.30 | 0.09 | 1.12 |
| REHE | 0.15 | 0.14 | 0.41 | 0.41 | 0.23 | 0.04 | 0.00 | 0.00 | 0.00 | 0.05 | 0.08 | 0.16 | 1.68 |
| ECE | Overall | Dec | Jan | Feb |
| NATIONAL | 1.201 (1.169,1.233) | 1.351 (1.285,1.419) | 1.157 (1.124,1.190) | 1.114 (1.064,1.167) |
| Northeast | 1.165 (1.117,1.216) | 1.455 (1.339,1.580) | 1.129 (1.042,1.222) | 1.096 (1.036,1.159) |
| Midwest | 1.138 (1.094,1.184) | 1.290 (1.187,1.402) | 1.092 (1.057,1.127) | 1.056 (0.965,1.156) |
| Southeast | 1.236 (1.166,1.310) | 1.513 (1.298,1.764) | 1.176 (1.117,1.238) | 1.027 (0.911,1.158) |
| Central | 1.238 (1.158,1.324) | 1.313 (1.202,1.434) | 1.172 (1.076,1.275) | 1.095 (0.973,1.232) |
| Southeast Coast | 1.423 (1.348,1.503) | 1.724 (1.494,1.990) | 1.320 (1.253,1.390) | 1.250 (0.971,1.609) |
| Desert | 1.143 (1.053,1.241) | 1.181 (1.102,1.265) | 1.083 (0.955,1.228) | 1.155 (0.853,1.565) |
| Pacific | 1.151 (1.114,1.188) | 1.162 (1.073,1.259) | 1.207 (1.131,1.288) | 1.184 (1.099,1.275) |
| S.S. Metros | 42 | 37 | 25 | 6 |
| EHE | Overall | JUN | JUL | AUG |
| NATIONAL | 1.091 (1.066,1.116) | 1.071 (1.027,1.117) | 1.111 (1.077,1.147) | 1.037 (1.005,1.071) |
| Northeast | 1.206 (1.118,1.301) | 1.234 (1.072,1.421) | 1.231 (1.128,1.345) | 1.076 (0.992,1.167) |
| Midwest | 1.077 (1.037,1.118) | 1.001 (0.937,1.069) | 1.108 (1.052,1.168) | 1.032 (0.956,1.115) |
| Southeast | 1.081 (1.044,1.119) | 1.053 (0.948,1.170) | 1.124 (1.060,1.193) | 0.991 (0.926,1.061) |
| Central | 1.087 (1.015,1.164) | 1.196 (1.023,1.398) | 1.093 (1.013,1.179) | 1.020 (0.947,1.098) |
| Southeast Coast | 1.011 (0.966,1.059) | 1.042 (0.975,1.113) | 1.025 (0.898,1.171) | 0.968 (0.865,1.083) |
| Desert | 1.063 (1.007,1.121) | 0.999 (0.751,1.331) | 1.060 (0.994,1.130) | 1.156 (0.998,1.338) |
| Pacific | 1.105 (1.065,1.146) | 1.103 (0.998,1.218) | 1.116 (1.038,1.199) | 1.141 (1.051,1.238) |
| S.S. Metros | 21 | 5 | 20 | 5 |
| RECE | Overall | FALL | SPRING | |
| NATIONAL | 1.069 (1.022,1.117) | 1.027 (0.972,1.085) | 1.199 (1.130,1.272) | |
| Northeast | 1.033 (0.978,1.090) | 0.958 (0.880,1.044) | 1.170 (1.061,1.290) | |
| Midwest | 0.940 (0.883,1.001) | 0.873 (0.809,0.942) | 1.155 (1.012,1.319) | |
| Southeast | 1.090 (0.972,1.222) | 1.003 (0.893,1.126) | 1.258 (1.062,1.489) | |
| Central | 1.068 (0.955,1.194) | 1.048 (0.913,1.201) | 1.087 (0.892,1.325) | |
| Southeast Coast | 1.297 (1.210,1.390) | 1.309 (1.202,1.425) | 1.315 (1.170,1.477) | |
| Desert | 1.063 (0.910,1.242) | 1.015 (0.883,1.167) | 1.255 (0.801,1.964) | |
| Pacific | 1.112 (0.967,1.279) | 1.090 (0.948,1.253) | 1.246 (0.986,1.573) | |
| S.S. Metros | 12 | 7 | 13 | |
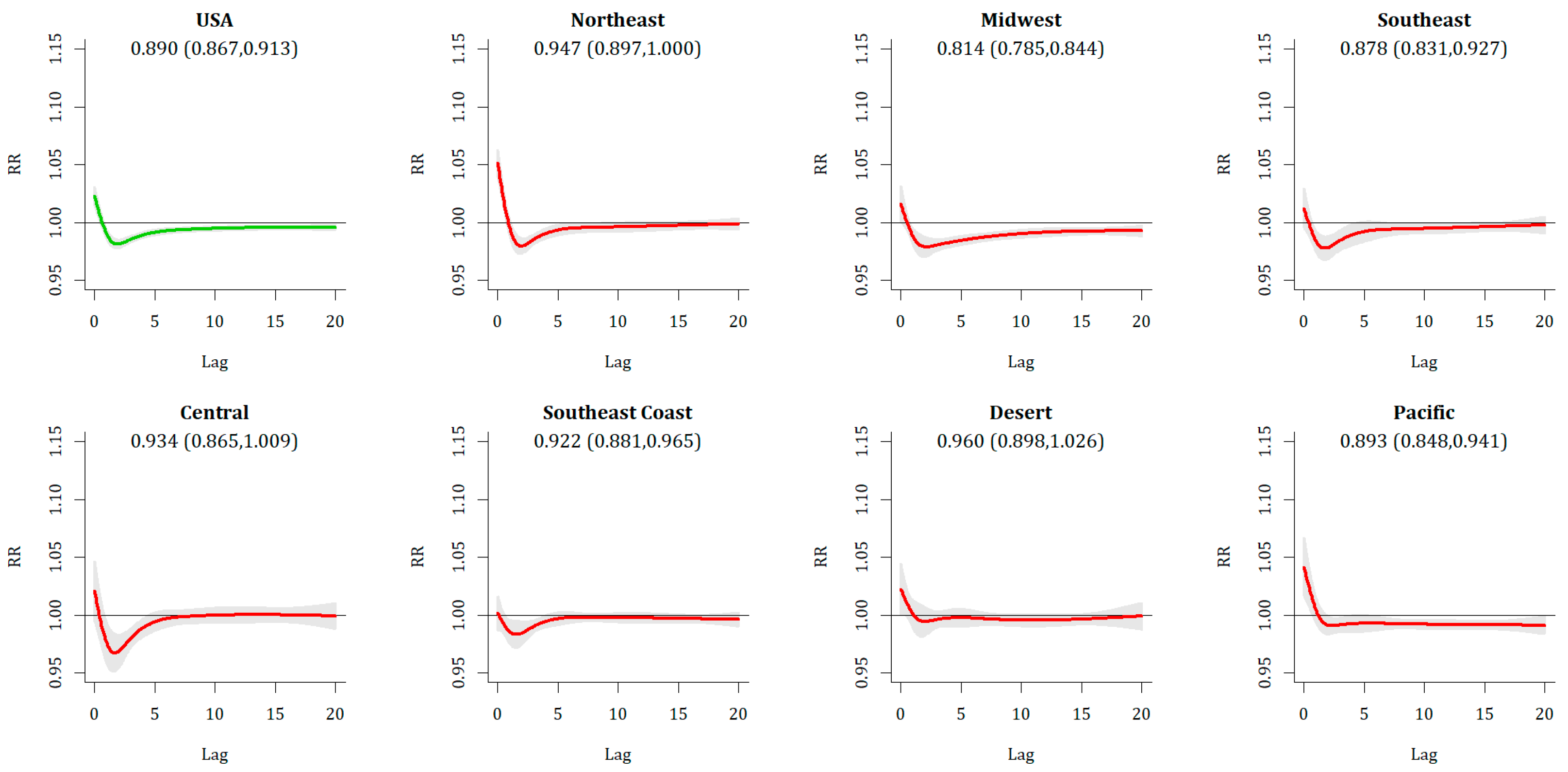
| REHE | Overall | SPRING | ||
| NATIONAL | 0.890 (0.867,0.913) | 0.910 (0.886,0.934) | ||
| Northeast | 0.947 (0.897,1.000) | 0.980 (0.942,1.020) | ||
| Midwest | 0.814 (0.785,0.844) | 0.830 (0.798,0.864) | ||
| Southeast | 0.878 (0.831,0.927) | 0.913 (0.864,0.966) | ||
| Central | 0.934 (0.865,1.009) | 0.992 (0.913,1.079) | ||
| Southeast Coast | 0.922 (0.881,0.965) | 0.948 (0.908,0.991) | ||
| Desert | 0.960 (0.898,1.026) | 0.931 (0.866,1.000) | ||
| Pacific | 0.893 (0.848,0.941) | 0.881 (0.800,0.970) | ||
| S.S. Metros | 0 | 0 |
| ECE | Overall | Dec | Jan | Feb |
| NATIONAL | 1.029 (1.023,1.035) | 1.025 (1.015,1.035) | 1.035 (1.029,1.041) | 1.023 (1.013,1.033) |
| Northeast | 1.031 (1.017,1.044) | 1.038 (1.016,1.061) | 1.029 (1.014,1.044) | 1.029 (1.009,1.048) |
| Midwest | 1.025 (1.016,1.034) | 1.013 (0.993,1.034) | 1.033 (1.022,1.044) | 1.002 (0.981,1.024) |
| Southeast | 1.051 (1.039,1.064) | 1.044 (1.020,1.069) | 1.055 (1.039,1.071) | 1.032 (0.999,1.067) |
| Central | 1.036 (1.020,1.053) | 1.036 (1.009,1.064) | 1.031 (1.005,1.058) | 1.047 (1.011,1.084) |
| Southeast Coast | 1.045 (1.032,1.058) | 1.054 (1.032,1.076) | 1.041 (1.023,1.059) | 1.031 (0.986,1.078) |
| Desert | 1.002 (0.984,1.021) | 0.996 (0.974,1.019) | 1.013 (0.972,1.056) | 1.006 (0.967,1.046) |
| Pacific | 1.010 (0.996,1.024) | 1.002 (0.981,1.024) | 1.021 (0.993,1.050) | 1.023 (1.000,1.047) |
| S.S. Metros | 23 | 9 | 14 | 4 |
| EHE | Overall | JUN | JUL | AUG |
| NATIONAL | 1.084 (1.071,1.097) | 1.077 (1.057,1.097) | 1.098 (1.084,1.113) | 1.068 (1.048,1.088) |
| Northeast | 1.142 (1.101,1.184) | 1.130 (1.075,1.189) | 1.147 (1.108,1.187) | 1.132 (1.083,1.182) |
| Midwest | 1.090 (1.067,1.112) | 1.061 (1.032,1.090) | 1.110 (1.083,1.139) | 1.072 (1.037,1.108) |
| Southeast | 1.073 (1.059,1.086) | 1.021 (0.989,1.055) | 1.108 (1.084,1.133) | 1.025 (1.001,1.050) |
| Central | 1.055 (1.032,1.079) | 1.078 (1.027,1.132) | 1.067 (1.040,1.095) | 1.019 (0.994,1.045) |
| Southeast Coast | 1.029 (1.017,1.040) | 1.028 (1.004,1.053) | 1.038 (1.014,1.062) | 1.022 (0.997,1.048) |
| Desert | 1.065 (1.040,1.091) | 1.099 (1.040,1.160) | 1.069 (1.047,1.093) | 1.076 (1.019,1.136) |
| Pacific | 1.123 (1.095,1.152) | 1.161 (1.122,1.202) | 1.113 (1.087,1.139) | 1.142 (1.067,1.223) |
| S.S. Metros | 43 | 19 | 42 | 21 |
| RECE | Overall | FALL | SPRING | |
| NATIONAL | 1.009 (1.002,1.015) | 1.006 (0.998,1.014) | 1.012 (0.998,1.026) | |
| Northeast | 1.015 (1.002,1.029) | 0.993 (0.975,1.011) | 1.043 (1.023,1.064) | |
| Midwest | 1.007 (0.992,1.021) | 1.006 (0.989,1.024) | 1.006 (0.973,1.040) | |
| Southeast | 1.002 (0.983,1.021) | 0.988 (0.956,1.021) | 1.022 (0.981,1.064) | |
| Central | 1.011 (0.989,1.034) | 1.022 (0.994,1.050) | 0.992 (0.950,1.035) | |
| Southeast Coast | 1.026 (1.010,1.043) | 1.035 (1.013,1.057) | 1.016 (0.991,1.042) | |
| Desert | 0.990 (0.960,1.020) | 1.000 (0.967,1.035) | 0.961 (0.926,0.998) | |
| Pacific | 0.998 (0.980,1.017) | 0.998 (0.978,1.019) | 0.998 (0.962,1.035) | |
| S.S. Metros | 3 | 3 | 6 | |
| REHE | Overall | SPRING | ||
| NATIONAL | 1.018 (1.010,1.025) | 1.020 (1.011,1.030) | ||
| Northeast | 1.046 (1.035,1.057) | 1.050 (1.038,1.063) | ||
| Midwest | 1.015 (1.003,1.026) | 1.018 (1.001,1.035) | ||
| Southeast | 1.003 (0.989,1.017) | 1.002 (0.985,1.020) | ||
| Central | 1.009 (0.985,1.034) | 0.999 (0.973,1.026) | ||
| Southeast Coast | 0.992 (0.979,1.005) | 0.995 (0.979,1.010) | ||
| Desert | 1.019 (1.000,1.038) | 1.023 (1.002,1.045) | ||
| Pacific | 1.045 (1.020,1.070) | 1.052 (1.019,1.085) | ||
| S.S. Metros | 10 | 10 |
| Metro | Relative Risk (95% CI) |
|---|---|
| Atlanta | 1.239 (1.028, 1.494) |
| Cleveland | 1.233 (1.005, 1.513) |
| Dallas | 1.213 (1.026, 1.435) |
| Jacksonville | 1.505 (1.157, 1.958) |
| Los Angeles | 1.399 (1.268, 1.543) |
| Memphis | 1.313 (1.042, 1.653) |
| Miami | 1.367 (1.207, 1.548) |
| Nashville | 1.347 (1.036, 1.752) |
| New Orleans | 1.352 (1.103, 1.658) |
| Orlando | 1.307 (1.050, 1.628) |
| Sacramento | 1.226 (1.040, 1.445) |
| Tampa | 1.274 (1.115, 1.455) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sheridan, S.C.; Lee, C.C.; Allen, M.J. The Mortality Response to Absolute and Relative Temperature Extremes. Int. J. Environ. Res. Public Health 2019, 16, 1493. https://doi.org/10.3390/ijerph16091493
Sheridan SC, Lee CC, Allen MJ. The Mortality Response to Absolute and Relative Temperature Extremes. International Journal of Environmental Research and Public Health. 2019; 16(9):1493. https://doi.org/10.3390/ijerph16091493
Chicago/Turabian StyleSheridan, Scott C., Cameron C. Lee, and Michael J. Allen. 2019. "The Mortality Response to Absolute and Relative Temperature Extremes" International Journal of Environmental Research and Public Health 16, no. 9: 1493. https://doi.org/10.3390/ijerph16091493
APA StyleSheridan, S. C., Lee, C. C., & Allen, M. J. (2019). The Mortality Response to Absolute and Relative Temperature Extremes. International Journal of Environmental Research and Public Health, 16(9), 1493. https://doi.org/10.3390/ijerph16091493