Dietary Lead Exposure and Associated Health Risks in Guangzhou, China

Abstract
1. Introduction
2. Materials and Methods
2.1. Chemicals and Instruments
2.2. Food Sampling
2.3. Analytical Procedure
2.4. Quality Assurance
2.5. Food Consumption Data
2.6. Intake Calculation
2.7. Risk Assessment
2.8. Statistical Analysis
3. Results
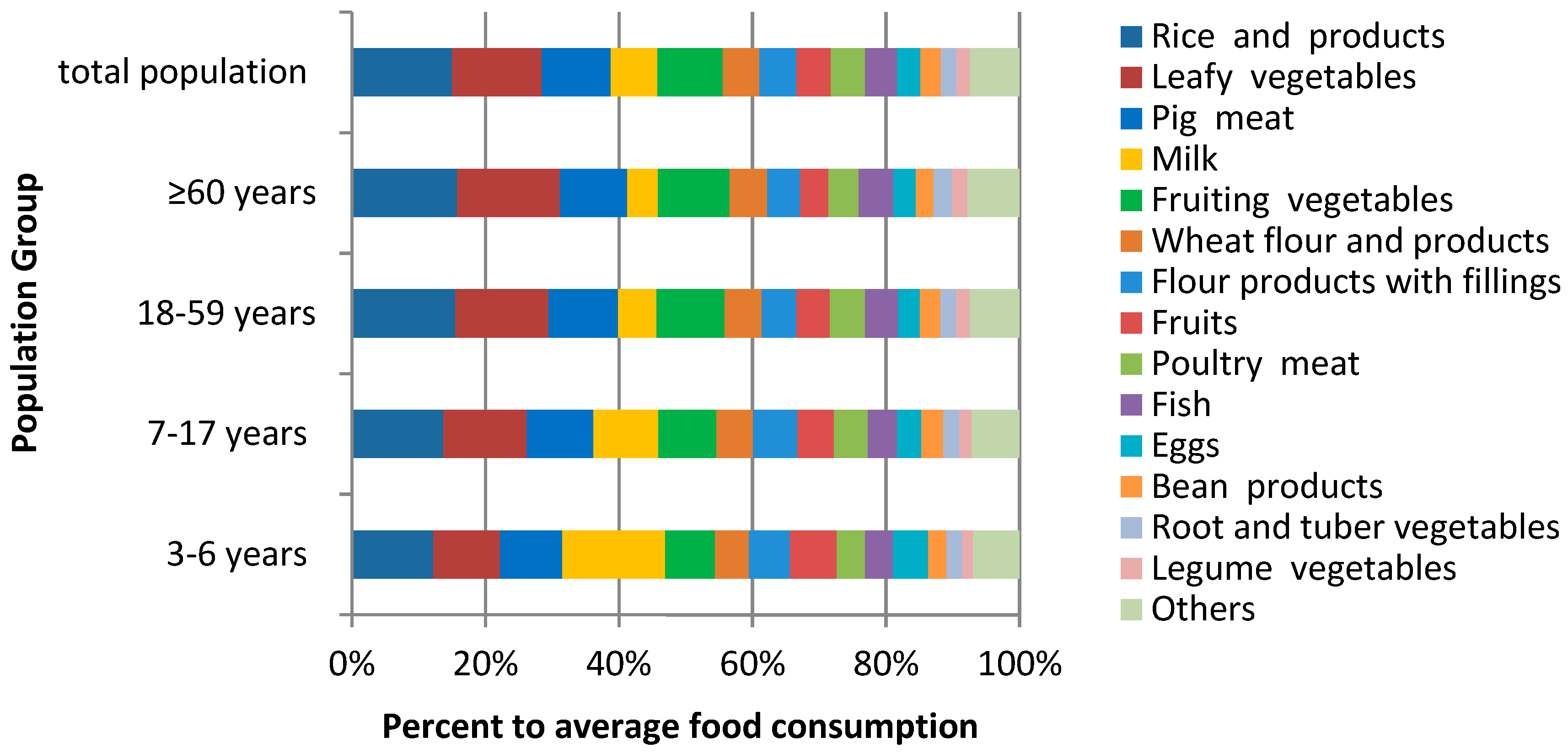
3.1. Contaminant Monitoring and Food Consumption Data
3.2. Dietary Lead Exposure and Risk Assessment
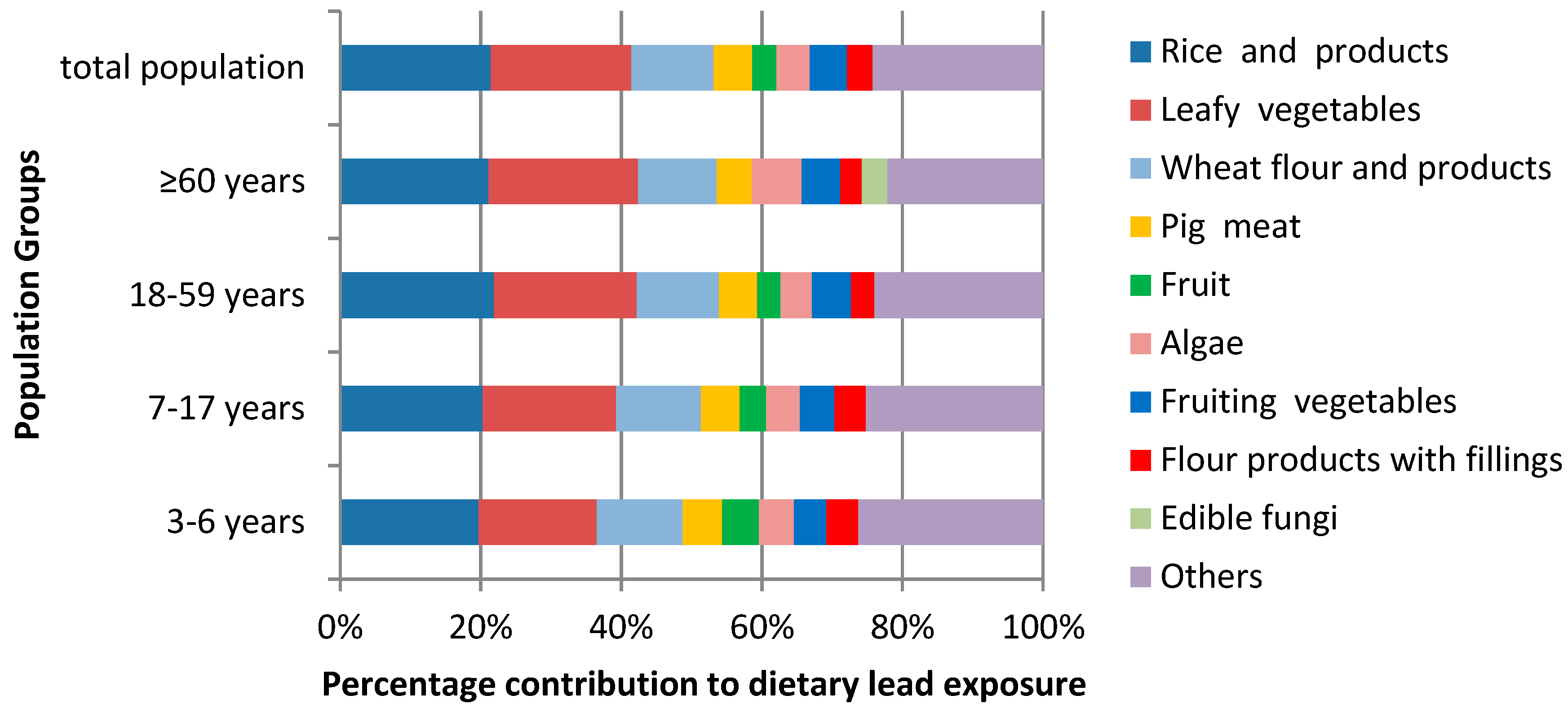
3.3. Contributions of Different Food Groups to the Mean Lead Exposure
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Food Category | 3–6 years | 7–17 years | 18–59 years | ≥60 years | Overall Population | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | P95 | Mean | P95 | Mean | P95 | Mean | P95 | Mean | P95 | |
| Rice and rice products | 78.6 ± 45.5 | 168.8 | 121.3 ± 73.9 | 265.9 | 146.5 ± 90.8 | 309.0 | 148.5 ± 89.6 | 292.6 | 135.8 ± 86.9 | 293.2 |
| Wheat flour and products | 32.6 ± 42.3 | 109.3 | 48.4 ± 58.6 | 166.7 | 52.3 ± 58.8 | 166.7 | 52.6 ± 62.0 | 160.3 | 49.9 ± 57.9 | 160.0 |
| Flour products with fillings | 39.5 ± 42.8 | 125.5 | 58.5 ± 64.5 | 186.0 | 48.9 ± 58.3 | 159.4 | 46.2 ± 53.5 | 170.1 | 49.9 ± 58.4 | 161.6 |
| Other cereals | 6.3 ± 18.8 | 30.2 | 7.0 ± 17.5 | 38.3 | 9.2 ± 27.5 | 46.0 | 14.8 ± 42.3 | 66.7 | 8.8 ± 26.3 | 45.0 |
| Pulses | 1.8 ± 5.4 | 15.5 | 4.1 ± 15.6 | 26.7 | 3.8 ± 14.0 | 24.2 | 2.2 ± 9.0 | 16.7 | 3.6 ± 13.6 | 23.3 |
| Bean products | 17.7 ± 32.7 | 83.3 | 28.8 ± 49.6 | 146.7 | 28.9 ± 50.0 | 133.3 | 25.1 ± 41.6 | 123.3 | 27.7 ± 48.3 | 133.3 |
| Preserved eggs | 0.5 ± 3.3 | 0.0 | 0.7 ± 4.5 | 3.3 | 0.7 ± 3.4 | 3.3 | 0.5 ± 3.0 | 0.2 | 0.6 ± 3.6 | 3.3 |
| Eggs | 33.7 ± 30.1 | 100.8 | 32.5 ± 30.1 | 81.2 | 31.3 ± 29.6 | 82.6 | 31.2 ± 25.9 | 79.5 | 31.7 ± 29.6 | 83.3 |
| Pig meat | 60.0 ± 43.2 | 149.9 | 88.4 ± 64.4 | 211.6 | 98.6 ± 69.9 | 234.4 | 94.5 ± 62.9 | 227.0 | 93.0 ± 67.4 | 228.0 |
| Livestock meat | 7.6 ± 15.4 | 35.3 | 13.6 ± 23.0 | 66.0 | 16.0 ± 26.7 | 66.7 | 9.9 ± 17.3 | 50.0 | 14.5 ± 24.9 | 66.7 |
| Poultry | 27.6 ± 31.6 | 80.9 | 44.7 ± 40.6 | 114.1 | 49.9 ± 48.0 | 139.1 | 42.3 ± 36.8 | 110.4 | 46.6 ± 45.3 | 133.3 |
| Edible offal | 2.7 ± 9.9 | 17.7 | 4.8 ± 13.8 | 33.3 | 5.7 ± 16.7 | 33.3 | 6.3 ± 17.1 | 50.0 | 5.3 ± 15.7 | 33.3 |
| Meat products | 5.3 ± 12.4 | 33.3 | 10.1 ± 20.3 | 57.5 | 8.8 ± 18.8 | 50.0 | 6.6 ± 15.7 | 40.2 | 8.6 ± 18.5 | 50.0 |
| Milk powder | 6.4 ± 17.1 | 52.0 | 0.5 ± 4.8 | 0.0 | 0.2 ± 2.0 | 0.0 | 0.6 ± 4.8 | 0.0 | 0.8 ± 6.0 | 0.0 |
| Milk | 98.7 ± 111.4 | 309.7 | 85.7 ± 102.0 | 255.3 | 53.8 ± 79.0 | 218.8 | 43.1 ± 64.4 | 173.6 | 63.4 ± 88.1 | 250.0 |
| Leafy vegetables | 64.4 ± 54.4 | 166.7 | 109.8 ± 75.4 | 250.0 | 131.5 ± 93.2 | 300.8 | 144.6 ± 98.4 | 350.0 | 122.2 ± 89.7 | 298.0 |
| Fruiting vegetables | 48.1 ± 41.4 | 127.7 | 76.6 ± 65.1 | 200.3 | 96.6 ± 83.7 | 249.5 | 101.5 ± 101.9 | 284.8 | 88.8 ± 80.0 | 236.7 |
| Root and tuber vegetables | 15.1 ± 25.2 | 60.6 | 21.2 ± 34.9 | 83.3 | 22.1 ± 36.5 | 94.9 | 25.9 ± 36.5 | 105.3 | 21.5 ± 35.4 | 91.6 |
| Legume vegetables | 10.2 ± 17.9 | 50.0 | 16.2 ± 25.9 | 66.7 | 19.0 ± 30.2 | 82.9 | 22.0 ± 39.3 | 83.5 | 17.9 ± 29.2 | 76.0 |
| Bulb vegetables | 3.1 ± 9.5 | 27.3 | 4.5 ± 12.6 | 32.7 | 5.6 ± 14.0 | 33.3 | 6.9 ± 13.9 | 36.5 | 5.2 ± 13.4 | 33.3 |
| Fruit | 44.9 ± 58.8 | 159.6 | 48.3 ± 71.6 | 190.8 | 47.2 ± 69.3 | 194.4 | 40.1 ± 58.4 | 152.8 | 46.9 ± 68.4 | 187.9 |
| Fish | 27.0 ± 29.7 | 83.3 | 38.3 ± 35.9 | 101.6 | 46.1 ± 42.9 | 133.3 | 49.3 ± 46.4 | 122.1 | 43.1 ± 41.2 | 121.0 |
| Crustaceans | 3.0 ± 8.6 | 26.7 | 4.9 ± 13.6 | 33.3 | 6.3 ± 20.4 | 40.0 | 6.7 ± 17.5 | 43.7 | 5.7 ± 18.4 | 36.6 |
| Mollusks | 0.8 ± 4.2 | 6.7 | 1.9 ± 7.8 | 16.7 | 2.2 ± 8.9 | 16.9 | 2.2 ± 7.9 | 26.0 | 2.0 ± 8.4 | 16.7 |
| Dried seafood | 0.3 ± 1.8 | 0.0 | 0.6 ± 4.6 | 0.0 | 0.6 ± 4.6 | 0.0 | 0.0 ± 0.3 | 0.0 | 0.5 ± 4.3 | 0.0 |
| Algae | 1.7 ± 7.4 | 8.8 | 2.5 ± 8.3 | 18.0 | 2.6 ± 9.6 | 16.7 | 4.3 ± 15.4 | 33.3 | 2.6 ± 9.6 | 16.7 |
| Edible fungi | 5.4 ± 9.8 | 26.7 | 7.8 ± 17.5 | 36.0 | 8.8 ± 18.8 | 46.7 | 12.1 ± 20.4 | 57.2 | 8.5 ± 18.1 | 43.3 |
References
- Xiao, C.K. Analysis of Present Situation about Lead Pollution in China. Environ. Sustain. Dev. 2017, 42, 91–92. [Google Scholar] [CrossRef]
- European Food Safety Authority. Lead dietary exposure in the European population. EFSA J. 2012, 10, 2831–2889. [Google Scholar] [CrossRef]
- Abadin, H.; Ashizawa, A.; Stevens, Y.W.; Llados, F.; Diamond, G.; Sage, G.; Citra, M.; Quinones, A.; Bosch, S.J.; Swarts, S.G. Toxicological Profile for Lead; Agency for Toxic Substances and Disease Registry (US): Atlanta, GA, USA, 2007; pp. 1–31. [Google Scholar]
- Ye, X.; Wong, O. Lead exposure, lead poisoning, and lead regulatory standards in China, 1990–2005. Regul. Toxicol. Pharm. 2006, 46, 157–162. [Google Scholar] [CrossRef]
- He, K.; Wang, S.; Zhang, J. Blood lead levels of children and its trend in China. Sci. Total Environ. 2009, 407, 3986–3993. [Google Scholar] [CrossRef]
- Growing up in a Leaded Environment: Lead Pollution and Children in China. Available online: https://www.wilsoncenter.org/publication/growing-leaded-environment-lead-pollution-and-children-china (accessed on 22 March 2019).
- Access Condition of Lead and Zinc Industry. Available online: http://www.ndrc.gov.cn/zcfb/zcfbgg/200703/t20070316_121733.html (accessed on 22 March 2019).
- Ji, A.; Wang, F.; Luo, W.; Yang, R.; Chen, J.; Cai, T. Lead poisoning in China: A nightmare from industrialisation. Lancet 2011, 377, 1474–1476. [Google Scholar] [CrossRef]
- Liu, P.; Wang, C.N.; Song, X.Y.; Wu, Y.N. Dietary intake of lead and cadmium by children and adults—Result calculated from dietary recall and available lead/cadmium level in food in comparison to result from food duplicate diet method. Int. J. Hyg. Environ. Health 2010, 213, 450–457. [Google Scholar] [CrossRef]
- Exposure to Lead: A Major Public Health Concern. Available online: http://www.who.int/ipcs/features/lead.pdf (accessed on 22 March 2019).
- Martorell, I.; Perelló, G.; Martí-Cid, R.; Llobet, J.M.; Castell, V.; Domingo, J.L. Human exposure to arsenic, cadmium, mercury, and lead from foods in Catalonia, Spain: Temporal trend. Biol. Trace Elem. Res. 2011, 142, 309–322. [Google Scholar] [CrossRef]
- Yusa, V.; Pardo, O. Human risk assessment and regulatory framework for minerals in food. In Handbook of Mineral Elements in Food; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2015; pp. 261–283. [Google Scholar]
- Galal-Gorchev, H. Dietary intake, levels in food and estimated intake of lead, cadmium, and mercury. Food Addit. Contam. 1993, 10, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Rabinowitz, M.B. Toxicokinetics of bone lead. Environ. Health Perspect. 1991, 91, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Gidlow, D.A. Lead toxicity. Occup. Med. (Lond.) 2015, 65, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Rosin, A. The long-term consequences of exposure to lead. Isr. Med. Assoc. J. 2009, 11, 689–694. [Google Scholar] [PubMed]
- Rehman, K.; Fatima, F.; Waheed, I.; Akash, M. Prevalence of exposure of heavy metals and their impact on health consequences. J. Cell. Biochem. 2018, 119, 157–184. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.C.; Su, P.H.; Chen, H.Y.; Huang, H.B.; Tsai, J.L.; Huang, H.I.; Wang, S.L. Childhood blood lead levels and intellectual development after ban of leaded gasoline in Taiwan: A 9-year prospective study. Environ. Int. 2012, 40, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, A.R. Redefining toxic lead levels among adults. Ann. Intern. Med. 2012, 157, 292–293. [Google Scholar] [CrossRef]
- Shen, X.; Wu, S.; Yan, C. Impacts of low-level lead exposure on development of children: Recent studies in China. Clin. Chim. Acta 2001, 313, 217–220. [Google Scholar] [CrossRef]
- Canfield, R.L.; Henderson, C.J.; Cory-Slechta, D.A.; Cox, C.; Jusko, T.A.; Lanphear, B.P. Intellectual impairment in children with blood lead concentrations below 10 microg per deciliter. N. Engl. J. Med. 2003, 348, 1517–1526. [Google Scholar] [CrossRef] [PubMed]
- Lanphear, B.P.; Hornung, R.; Khoury, J.; Yolton, K.; Baghurst, P.; Bellinger, D.C.; Canfield, R.L.; Dietrich, K.N.; Bornschein, R.; Greene, T.; et al. Low-level environmental lead exposure and children’s intellectual function: An international pooled analysis. Environ. Health Perspect. 2005, 113, 894–899. [Google Scholar] [CrossRef] [PubMed]
- IARC. Inorganic and organic lead compounds. IARC. Monogr. Eval. Carcinog. Risks Hum. 2006, 87, 1–471. [Google Scholar]
- Ten Chemicals of Major Public Health Concern. Available online: https://www.who.int/ipcs/assessment/public_health/chemicals_phc/en/ (accessed on 22 March 2019).
- Lead Poisoning and Health. Available online: http://www.who.int/news-room/fact-sheets/detail/lead-poisoning-and-health (accessed on 22 March 2019).
- FAO/WHO. Principles and Methods for the Risk Assessment of Chemicals in Food; World Health Organization: Geneva, Switzerland, 2009; pp. 1–752. [Google Scholar]
- Lambe, J. The use of food consumption data in assessments of exposure to food chemicals including the application of probabilistic modelling. Proc. Nutr. Soc. 2002, 61, 11–18. [Google Scholar] [CrossRef]
- Renwick, A.G.; Barlow, S.M.; Hertz-Picciotto, I.; Boobis, A.R.; Dybing, E.; Edler, L.; Eisenbrand, G.; Greig, J.B.; Kleiner, J.; Lambe, J.; et al. Risk characterisation of chemicals in food and diet. Food Chem. Toxicol. 2003, 41, 1211–1271. [Google Scholar] [CrossRef]
- WHO. Guidelines for the Study of Dietary Intakes of Chemical Contaminants; WHO Offset Publication: Geneva, Switzerland, 1985; pp. 1–102. [Google Scholar]
- WHO. Evaluation of Certain Food Additives and Contaminants. Seventy-third Meeting of the Joint FAO/WHO Expert Committee on Food Additives; WHO Technical Report Series; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- EFSA. Opinion of the Scientific Committee on a request from EFSA related to A Harmonised Approach for Risk Assessment of Substances Which are both Genotoxic and Carcinogenic. EFSA J. 2005, 282, 1–31. [Google Scholar]
- EFSA. Scientific opinion on lead in food—EFSA panel on contaminants in the food chain. EFSA J. 2010, 8, 1–151. [Google Scholar] [CrossRef]
- The 23rd Australian Total Diet Study. Available online: http://www.foodstandards.gov.au (accessed on 22 March 2019).
- Li, X.; Liu, Q.; Liu, L.; Wu, Y. Application of the data from China Total Diet Study to assess the distribution of lead exposure in different age-gender population groups. J. Hyg. Res. 2012, 41, 379–384. [Google Scholar]
- Zhang, W.; Liu, Y.; Liu, Y.; Liang, B.; Zhou, H.; Li, Y.; Zhang, Y.; Huang, J.; Yu, C.; Chen, K. An Assessment of Dietary Exposure to Cadmium in Residents of Guangzhou, China. Int. J. Environ. Res. Public Health 2018, 15, 556. [Google Scholar] [CrossRef]
- Yu, C.; He, J.Y.; Li, Y.Y.; Lin, X.H.; Xie, C.J.; Zhou, Q.; Chen, K.C. Analysis on the Lead-Contamination of Foods in Guangzhou City in 2008. Chin. J. Food Hyg. 2009, 21, 460–463. [Google Scholar]
- Zhang, Y.; Liu, P.; Wang, C.; Wu, Y. Human health risk assessment of cadmium via dietary intake by children in Jiangsu Province, China. Environ. Geochem. Health 2017, 39, 29–41. [Google Scholar] [CrossRef]
- Rose, M.; Baxter, M.; Brereton, N.; Baskaran, C. Dietary exposure to metals and other elements in the 2006 UK Total Diet Study and some trends over the last 30 years. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2010, 27, 1380–1404. [Google Scholar] [CrossRef]
- Liang, C.S.; Luo, J.B. Food Safety Risk Monitoring Manual; Standards Press of China: Beijing, China, 2012; p. 351. [Google Scholar]
- Zhang, Y.H.; Li, Y.Y.; He, J.Y.; Liang, B.H.; Yu, C.; Zhang, W.W.; Huang, J. Food consumption and nutrients intake among residents in Guangzhou city. Chin. J. Public Health 2017, 33, 969–972. [Google Scholar] [CrossRef]
- FAO/WHO. Dietary Exposure Assessment of Chemicals in Food: Report of a Joint FAO/ WHO Consultation; WHO Library: Annapolis, MD, USA, 2005. [Google Scholar]
- WHO. GEMS/Food-EURO Second Workshop on Reliable Evaluation of Low-Level Contamination of Food: Report on a Workshop in the Frame of GEMS Food-EURO, Kulmbach, Germany, 26–27 May 1995; WHO: Geneva, Switzerland, 1995. [Google Scholar]
- EFSA. Guidance of the Scientific Committee on a request from EFSA on the use of the benchmark dose approach in risk assessment. EFSA J. 2009, 1150. [Google Scholar] [CrossRef]
- Jin, Y.; Liu, P.; Sun, J.; Wang, C.; Min, J.; Zhang, Y.; Wang, S.; Wu, Y. Dietary exposure and risk assessment to lead of the population of Jiangsu province, China. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2014, 31, 1187–1195. [Google Scholar] [CrossRef]
- Juric, A.K.; Batal, M.; David, W.; Sharp, D.; Schwartz, H.; Ing, A.; Fediuk, K.; Black, A.; Tikhonov, C.; Chan, H.M.; et al. Risk assessment of dietary lead exposure among First Nations people living on-reserve in Ontario, Canada using a total diet study and a probabilistic approach. J. Hazard. Mater. 2018, 344, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Cai, W.; Su, Z.; Hu, S.; Huang, W. Assessment of the content and exposure of lead and cadmium in the major food of Guangdong residents. Chin. J. Health Lab. Technol. 2015, 25, 2388–2392. [Google Scholar]
- Pan, L.; Wang, Z.; Peng, Z.; Liu, G.; Zhang, H.; Zhang, J.; Jiang, J.; Pathiraja, N.; Xiao, Y.; Jiao, R.; Huang, W. Dietary exposure to lead of adults in Shenzhen city, China. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2016, 33, 1200–1206. [Google Scholar] [CrossRef]
- Liu, H.; Wu, C.; Lu, Y.; Fang, Y.; Gao, W.; Xing, Z.; Lu, D. Assessment on the dietary exposure of lead and cadmium in Shanghai residents. Chin. J. Food. Hyg. 2011, 23, 218–223. [Google Scholar] [CrossRef]
- Luo, X.; Huang, W.; Zhang, J.; Yang, L.; Wang, Z.; Pan, L.; Zhang, L. Assessment on dietary exposure of lead and cadmium of residents in Shenzhen City. China Trop. Med. 2016. [Google Scholar] [CrossRef]
- Sun, J.F.; Wang, C.N.; Wu, Y.N.; Yuan, B.J.; Tian, Z.H.; Song, X.Y.; Li, C.Y.; Liu, P. Long-term dietary exposure to lead of the population of Jiangsu Province, China. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2011, 28, 107–114. [Google Scholar] [CrossRef]
- Fan, W.; Wang, J.; Chen, L. Assessment on the dietary exposure of lead, cadmium and total mercury in different populations in Shaoxing. Chin. J. Food Hyg. 2016, 28, 535–540. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, P.; Jin, Y.; Wang, C.; Min, J.; Wu, Y. Dietary exposure and risk assessment to cadmium of the adult population of Jiangsu province, China: Comparing between semi-probabilistic and fully probabilistic approaches. Hum. Ecol. Risk Assess. Int. J. 2016, 22, 226–240. [Google Scholar] [CrossRef]
- Chen, M.Y.; Chan, B.T.; Lam, C.H.; Chung, S.W.; Ho, Y.Y.; Xiao, Y. Dietary exposures to eight metallic contaminants of the Hong Kong adult population from a total diet study. Food Addit. Contam. Part A Chem. Anal. Control Expo. Risk Assess. 2014, 31, 1539–1549. [Google Scholar] [CrossRef]
- Koh, E.; Shin, H.; Yon, M.; Nam, J.W.; Lee, Y.; Kim, D.; Lee, J.; Kim, M.; Park, S.K.; Choi, H.; et al. Measures for a closer-to-real estimate of dietary exposure to total mercury and lead in total diet study for Koreans. Nutr. Res. Pract. 2012, 6, 436–443. [Google Scholar] [CrossRef]
- Arnich, N.; Sirot, V.; Riviere, G.; Jean, J.; Noel, L.; Guerin, T.; Leblanc, J.C. Dietary exposure to trace elements and health risk assessment in the 2nd French Total Diet Study. Food Chem. Toxicol. 2012, 50, 2432–2449. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, L.; Nashalian, O.; Naja, F.; Itani, L.; Parent-Massin, D.; Nabhani-Zeidan, M.; Hwalla, N. Dietary exposure to essential and toxic trace elements from a Total diet study in an adult Lebanese urban population. Food Chem. Toxicol. 2010, 48, 1262–1269. [Google Scholar] [CrossRef] [PubMed]
- Koch, W.; Karim, M.R.; Marzec, Z.; Miyataka, H.; Himeno, S.; Asakawa, Y. Dietary intake of metals by the young adult population of Eastern Poland: Results from a market basket study. J. Trace Elem. Med. Biol. 2016, 35, 36–42. [Google Scholar] [CrossRef]
- Skrbic, B.; Zivancev, J.; Mrmos, N. Concentrations of arsenic, cadmium and lead in selected foodstuffs from Serbian market basket: Estimated intake by the population from the Serbia. Food Chem. Toxicol. 2013, 58, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Turconi, G.; Minoia, C.; Ronchi, A.; Roggi, C. Dietary exposure estimates of twenty-one trace elements from a Total Diet Study carried out in Pavia, Northern Italy. Br. J. Nutr. 2009, 101, 1200–1208. [Google Scholar] [CrossRef] [PubMed]


| Parameters | Operating Conditions |
|---|---|
| RF Power (KW) | 1550 |
| Sample Depth (mm) | 8.0 |
| Carrier Gas (L/min) | 0.7 |
| Makeup Gas (L/min) | 0.5 |
| Argon Flow (mL/min) | 4.3 |
| Extraction 1 (V) | 0.0 |
| Extraction 2 (V) | −130 |
| Omega Bias (V) | −90 |
| Omega Lens (V) | 7.0 |
| Deflect (V) | 1.4 |
| Octopole Bias (V) | −18 |
| Octopole RF (V) | 140 |
| KED (V) | 3.0 |
| Food Category | Samples | Mean | SD a | P50 | P95 | >LOD (%) |
|---|---|---|---|---|---|---|
| Rice and rice products | 990 | 0.0341 | 0.0430 | 0.0151 | 0.1341 | 73.2 |
| Wheat flour and products | 1165 | 0.0509 | 0.0634 | 0.0260 | 0.1707 | 81.7 |
| Flour products with fillings | 26 | 0.0158 | 0.0118 | 0.0130 | 0.0427 | 88.5 |
| Other cereals | 479 | 0.0206 | 0.0264 | 0.0090 | 0.0820 | 57.6 |
| Pulses | 110 | 0.0272 | 0.0262 | 0.0200 | 0.0700 | 80.0 |
| Bean products | 110 | 0.0151 | 0.0245 | 0.0089 | 0.0645 | 74.5 |
| Preserved eggs | 34 | 0.0341 | 0.1646 | 0.0040 | 0.2660 | 64.7 |
| Eggs | 306 | 0.0099 | 0.0115 | 0.0060 | 0.0307 | 68.6 |
| Pig meat | 221 | 0.0127 | 0.0122 | 0.0100 | 0.0300 | 69.7 |
| Livestock meat b | 86 | 0.0083 | 0.0113 | 0.0045 | 0.0356 | 62.8 |
| Poultry | 99 | 0.0115 | 0.0162 | 0.0090 | 0.0280 | 83.8 |
| Edible offal | 140 | 0.0240 | 0.0319 | 0.0190 | 0.0700 | 89.3 |
| Meat products | 72 | 0.0394 | 0.0262 | 0.0345 | 0.0837 | 100.0 |
| Milk powder | 145 | 0.0071 | 0.0081 | 0.0050 | 0.0200 | 22.8 |
| Milk | 208 | 0.0036 | 0.0023 | 0.0500 | 0.0050 | 3.4 |
| Leafy vegetables c | 356 | 0.0354 | 0.0464 | 0.0170 | 0.1432 | 77.2 |
| Fruiting vegetables d | 163 | 0.0130 | 0.0167 | 0.0060 | 0.0468 | 62.0 |
| Root and tuber vegetables | 5 | 0.0230 | 0.0124 | 0.0220 | 0.3500 | 100.0 |
| Legume vegetables | 115 | 0.0209 | 0.0360 | 0.0050 | 0.1096 | 62.6 |
| Bulb vegetables | 42 | 0.0505 | 0.0616 | 0.0270 | 0.2140 | 64.3 |
| Fruit | 223 | 0.0160 | 0.0181 | 0.0090 | 0.0594 | 67.3 |
| Fish | 536 | 0.0134 | 0.0178 | 0.0068 | 0.0483 | 70.9 |
| Crustaceans | 143 | 0.0109 | 0.0101 | 0.0074 | 0.0322 | 68.5 |
| Mollusks | 318 | 0.1384 | 0.1117 | 0.1200 | 0.3351 | 99.7 |
| Dried seafood | 24 | 0.3219 | 0.2603 | 0.2365 | 0.9000 | 100.0 |
| Algae | 175 | 0.3947 | 0.4349 | 0.3400 | 0.8938 | 78.9 |
| Edible fungi | 48 | 0.0729 | 0.0147 | 0.0750 | 0.0900 | 100.0 |
| Total | 6339 | 0.0433 | 0.1104 | 0.0130 | 0.1710 | 71.6 |
| Food Category | 3–6 Years | 7–17 Years | 18–59 Years | ≥60 Years | Total Population | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | P95 | Contrib. | Mean | P95 | Contrib. | Mean | P95 | Contrib. | Mean | P95 | Contrib. | Mean | P95 | Contrib. | |
| Rice and rice products | 0.1473 | 0.3163 | 19.73% | 0.0960 | 0.2104 | 20.26% | 0.0822 | 0.1733 | 21.87% | 0.0851 | 0.1677 | 21.11% | 0.0864 | 0.1865 | 21.42% |
| Wheat flour and products | 0.0912 | 0.3057 | 12.22% | 0.0572 | 0.1969 | 12.07% | 0.0438 | 0.1396 | 11.65% | 0.0450 | 0.1371 | 11.16% | 0.0474 | 0.1519 | 11.75% |
| Flour products with fillings | 0.0343 | 0.1090 | 4.59% | 0.0214 | 0.0682 | 4.52% | 0.0127 | 0.0414 | 3.38% | 0.0123 | 0.0452 | 3.05% | 0.0147 | 0.0476 | 3.64% |
| Other cereals | 0.0071 | 0.0342 | 0.95% | 0.0033 | 0.0183 | 0.70% | 0.0031 | 0.0156 | 0.82% | 0.0051 | 0.0231 | 1.27% | 0.0034 | 0.0173 | 0.84% |
| Pulses | 0.0027 | 0.0232 | 0.36% | 0.0026 | 0.0169 | 0.55% | 0.0017 | 0.0108 | 0.45% | 0.0010 | 0.0076 | 0.25% | 0.0018 | 0.0118 | 0.45% |
| Bean products | 0.0147 | 0.0691 | 1.97% | 0.0101 | 0.0514 | 2.13% | 0.0072 | 0.0331 | 1.92% | 0.0064 | 0.0313 | 1.59% | 0.0078 | 0.0376 | 1.93% |
| Preserved eggs | 0.0009 | 0 | 0.12% | 0.0006 | 0.0026 | 0.13% | 0.0004 | 0.0019 | 0.11% | 0.0003 | 0.0001 | 0.07% | 0.0004 | 0.0021 | 0.10% |
| Eggs | 0.0183 | 0.0548 | 2.45% | 0.0075 | 0.0187 | 1.58% | 0.0051 | 0.0134 | 1.36% | 0.0052 | 0.0132 | 1.29% | 0.0059 | 0.0154 | 1.46% |
| Pig meat | 0.0419 | 0.1046 | 5.61% | 0.0260 | 0.0624 | 5.49% | 0.0206 | 0.0490 | 5.48% | 0.0202 | 0.0485 | 5.01% | 0.0220 | 0.0540 | 5.45% |
| Livestock meat | 0.0035 | 0.0161 | 0.47% | 0.0026 | 0.0127 | 0.55% | 0.0022 | 0.0091 | 0.59% | 0.0014 | 0.0070 | 0.35% | 0.0022 | 0.0103 | 0.55% |
| Poultry | 0.0174 | 0.0511 | 2.33% | 0.0119 | 0.0304 | 2.51% | 0.0094 | 0.0263 | 2.50% | 0.0082 | 0.0213 | 2.03% | 0.0100 | 0.0286 | 2.48% |
| Edible offal | 0.0036 | 0.0233 | 0.48% | 0.0027 | 0.0185 | 0.57% | 0.0023 | 0.0131 | 0.61% | 0.0025 | 0.0202 | 0.62% | 0.0024 | 0.0149 | 0.60% |
| Meat products | 0.0115 | 0.0721 | 1.54% | 0.0092 | 0.0526 | 1.94% | 0.0057 | 0.0324 | 1.52% | 0.0044 | 0.0266 | 1.09% | 0.0063 | 0.0368 | 1.56% |
| Milk powder | 0.0025 | 0.0203 | 0.33% | 0.0001 | 0 | 0.02% | 0 | 0 | 0.00% | 0.0001 | 0 | 0.02% | 0.0001 | 0 | 0.02% |
| Milk | 0.0195 | 0.0613 | 2.61% | 0.0072 | 0.0213 | 1.52% | 0.0032 | 0.0130 | 0.85% | 0.0026 | 0.0105 | 0.65% | 0.0043 | 0.0168 | 1.07% |
| Leafy vegetables | 0.1253 | 0.3242 | 16.78% | 0.0902 | 0.2053 | 19.03% | 0.0766 | 0.1751 | 20.38% | 0.0860 | 0.2082 | 21.33% | 0.0807 | 0.1968 | 20.01% |
| Fruiting vegetables | 0.0344 | 0.0912 | 4.61% | 0.0231 | 0.0604 | 4.87% | 0.0207 | 0.0533 | 5.51% | 0.0222 | 0.0622 | 5.51% | 0.0215 | 0.0574 | 5.33% |
| Root and tuber vegetables | 0.0191 | 0.0766 | 2.56% | 0.0113 | 0.0445 | 2.38% | 0.0084 | 0.0359 | 2.23% | 0.0100 | 0.0407 | 2.48% | 0.0092 | 0.0393 | 2.28% |
| Legume vegetables | 0.0117 | 0.0574 | 1.57% | 0.0079 | 0.0323 | 1.67% | 0.0065 | 0.0285 | 1.73% | 0.0077 | 0.0293 | 1.91% | 0.0070 | 0.0296 | 1.74% |
| Bulb vegetables | 0.0086 | 0.0758 | 1.15% | 0.0053 | 0.0383 | 1.12% | 0.0047 | 0.0277 | 1.25% | 0.0059 | 0.0310 | 1.46% | 0.0049 | 0.0314 | 1.21% |
| Fruit | 0.0395 | 0.1403 | 5.29% | 0.0179 | 0.0708 | 3.78% | 0.0124 | 0.0512 | 3.30% | 0.0108 | 0.0411 | 2.68% | 0.0140 | 0.0561 | 3.47% |
| Fish | 0.0199 | 0.0613 | 2.67% | 0.0119 | 0.0316 | 2.51% | 0.0102 | 0.0294 | 2.71% | 0.0111 | 0.0275 | 2.75% | 0.0108 | 0.0303 | 2.68% |
| Crustaceans | 0.0018 | 0.0160 | 0.24% | 0.0012 | 0.0084 | 0.25% | 0.0011 | 0.0072 | 0.29% | 0.0012 | 0.0080 | 0.30% | 0.0012 | 0.0074 | 0.30% |
| Mollusks | 0.0061 | 0.0509 | 0.82% | 0.0061 | 0.0536 | 1.29% | 0.0050 | 0.0385 | 1.33% | 0.0051 | 0.0605 | 1.27% | 0.0052 | 0.0431 | 1.29% |
| Dried seafood | 0.0053 | 0 | 0.71% | 0.0045 | 0 | 0.95% | 0.0032 | 0 | 0.85% | 0 | 0 | 0.00% | 0.0030 | 0 | 0.74% |
| Algae | 0.0369 | 0.1908 | 4.94% | 0.0229 | 0.1648 | 4.83% | 0.0169 | 0.1084 | 4.50% | 0.0285 | 0.2209 | 7.07% | 0.0191 | 0.1230 | 4.74% |
| Edible fungi | 0.0216 | 0.1069 | 2.89% | 0.0132 | 0.0609 | 2.79% | 0.0106 | 0.0560 | 2.82% | 0.0148 | 0.0701 | 3.67% | 0.0116 | 0.0589 | 2.88% |
| Total | 0.7466 | 2.4525 | 100.00% | 0.4739 | 1.5522 | 100.00% | 0.3759 | 1.1832 | 100.00% | 0.4031 | 1.3589 | 100.00% | 0.4033 | 1.3049 | 100.00% |
| Age Groups | MOE (Mean Exposure) | MOE (P95 Exposure) |
|---|---|---|
| 3–6 years a | 0.8 | 0.2 |
| 7–17 years a | 1.3 | 0.4 |
| 18–59 years b | 3.2 | 1.0 |
| ≥60 years b | 3.0 | 0.9 |
| Country | Population Group | Mean Exposure (μg/kg bw/day) | Reference |
|---|---|---|---|
| China (Guangzhou) | 3–6 years | 0.7466 | Present study |
| 7–17 years | 0.4739 | ||
| 18–59 years | 0.3759 | ||
| ≥60 years | 0.4031 | ||
| Overall population | 0.4033 | ||
| Canada (Ontario) | Adult | 0.21 | Juric et al. (2018) |
| China (Shenzhen) | Adult | 0.59–0.73 a | Pan et al. (2016) |
| Eastern Poland | Young adult | 0.79 | Koch et al. (2016) |
| China (Hong Kong) | Adult | 0.21 | Chen et al. (2014) |
| Serbia | Adult | 1.03 | Skrbic et al. (2013) |
| Korea | Overall population | 0.183 | Koh et al. (2012) |
| China | 2–7 years | 2.54 | Li et al. (2012) |
| 8–12 years | 2.50 | ||
| 13–19 years | 1.75 | ||
| 20–50 years | 1.73 | ||
| 51–65 years | 1.54 | ||
| >65 years | 1.52 | ||
| European countries | Children | 0.96 b | EFSA (2012) |
| Adolescent | 0.55 | ||
| Adult | 0.50 | ||
| Elderly | 0.49 | ||
| Overall population | 0.68 | ||
| France | Children | 0.27 | Arnich et al. (2012) |
| Adult | 0.2 | ||
| Australian | 2–5 years | 0.27 c | FSANZ (2011) |
| 6–12 years | 0.18 | ||
| 13–16 years | 0.12 | ||
| ≥17 years | 0.13 | ||
| United Kingdom | Adult | 0.09–0.10 a | Rose et al. (2010) |
| Lebanon | Adult | 0.11 | Nasreddine et al. (2010) |
| Italy (Pavia) | Adult | 0.85 | Turconi et al. (2009) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, M.; Liang, B.; Zhang, W.; Chen, K.; Zhang, Y.; Zhou, H.; Cheng, Y.; Liu, H.; Zhong, X.; Li, Y.; et al. Dietary Lead Exposure and Associated Health Risks in Guangzhou, China. Int. J. Environ. Res. Public Health 2019, 16, 1417. https://doi.org/10.3390/ijerph16081417
Wang M, Liang B, Zhang W, Chen K, Zhang Y, Zhou H, Cheng Y, Liu H, Zhong X, Li Y, et al. Dietary Lead Exposure and Associated Health Risks in Guangzhou, China. International Journal of Environmental Research and Public Health. 2019; 16(8):1417. https://doi.org/10.3390/ijerph16081417
Chicago/Turabian StyleWang, Man, Boheng Liang, Weiwei Zhang, Kuncai Chen, Yuhua Zhang, Hongwei Zhou, Yanfang Cheng, Huachun Liu, Xianwu Zhong, Yingyue Li, and et al. 2019. "Dietary Lead Exposure and Associated Health Risks in Guangzhou, China" International Journal of Environmental Research and Public Health 16, no. 8: 1417. https://doi.org/10.3390/ijerph16081417
APA StyleWang, M., Liang, B., Zhang, W., Chen, K., Zhang, Y., Zhou, H., Cheng, Y., Liu, H., Zhong, X., Li, Y., & Liu, Y. (2019). Dietary Lead Exposure and Associated Health Risks in Guangzhou, China. International Journal of Environmental Research and Public Health, 16(8), 1417. https://doi.org/10.3390/ijerph16081417