Modeling the Impact of an Indoor Air Filter on Air Pollution Exposure Reduction and Associated Mortality in Urban Delhi Household


Abstract
1. Introduction
2. Materials and Methods
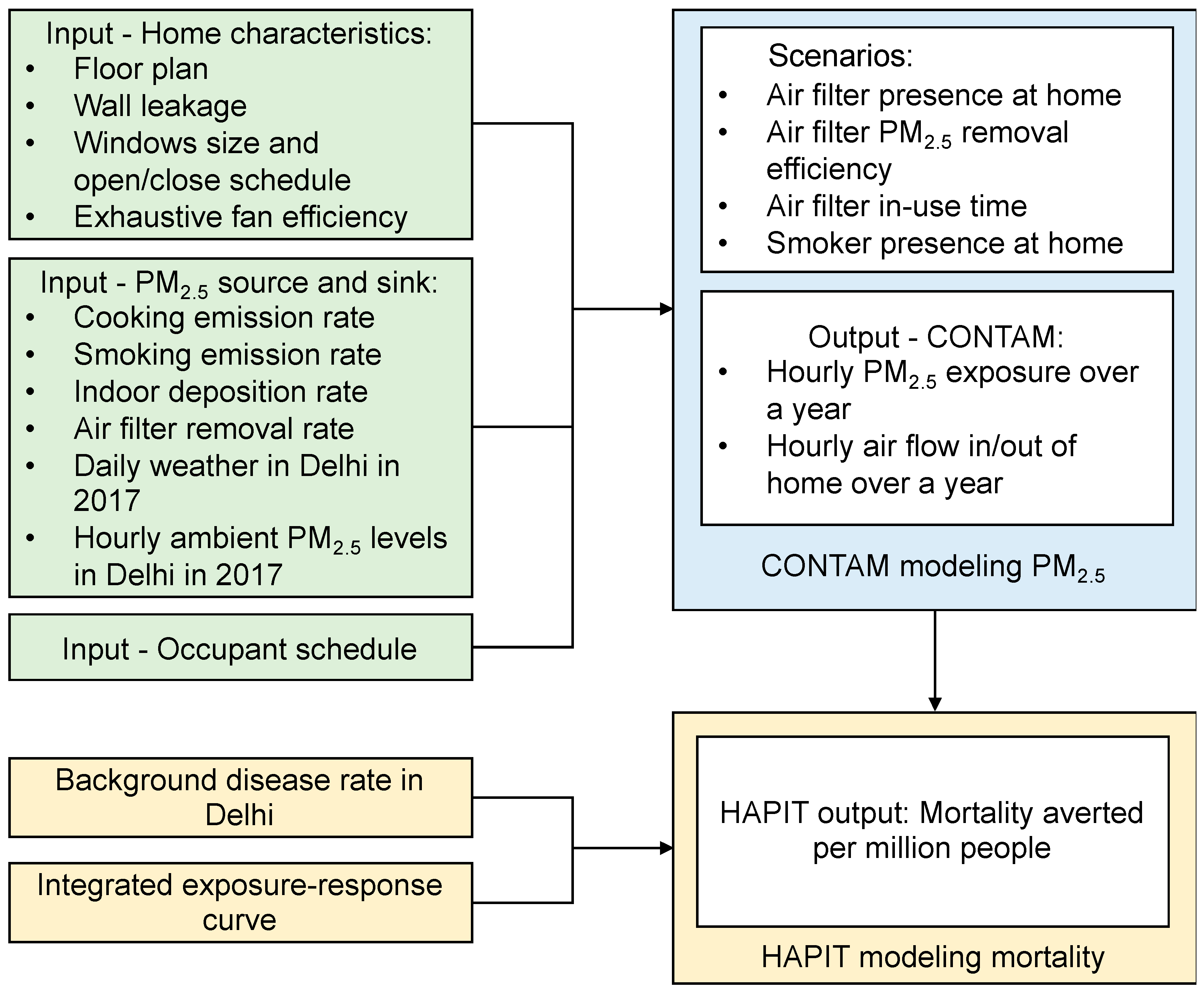
2.1. Study Overview
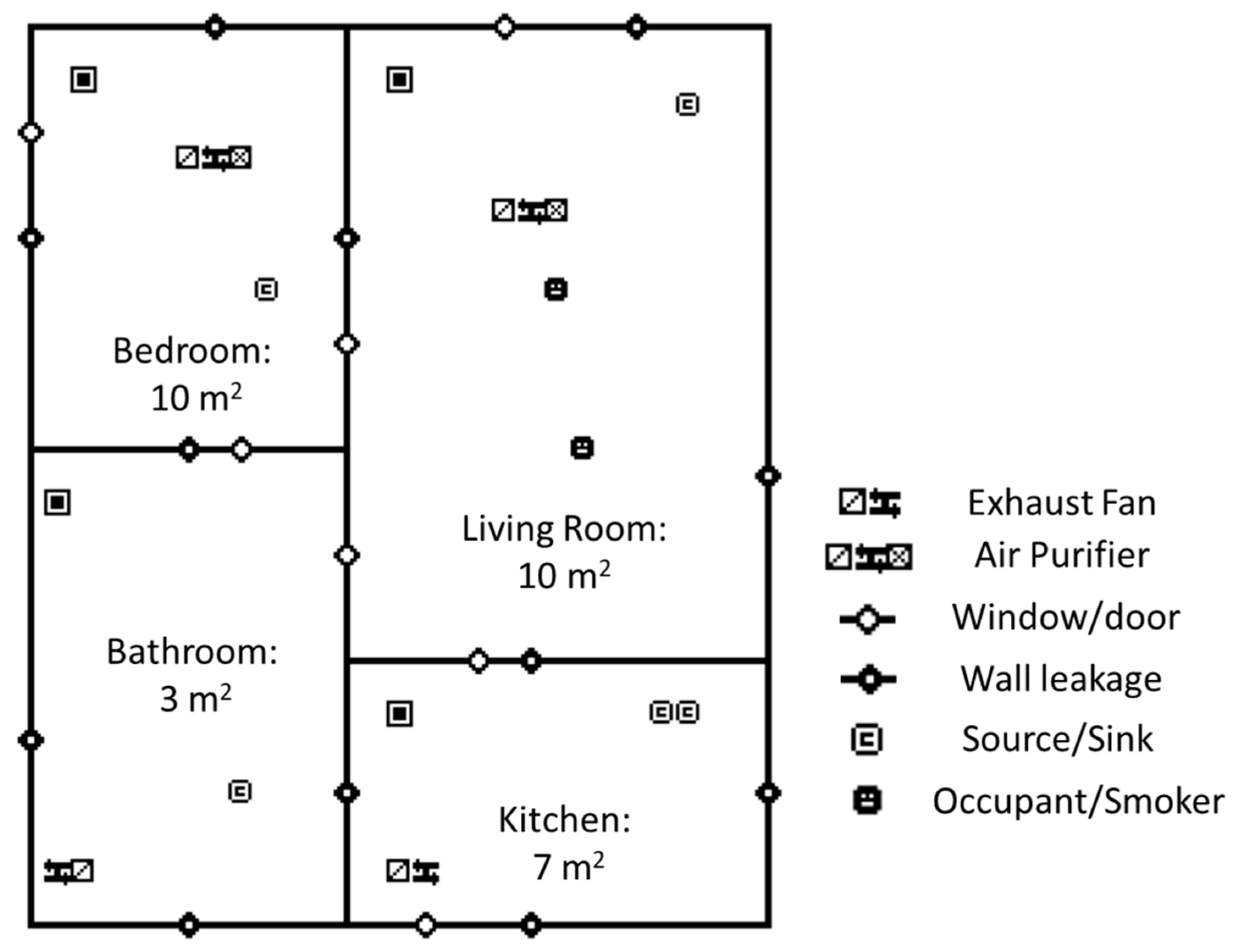
2.2. Simulated Indoor Environment
2.3. Contaminant Sources and Sinks
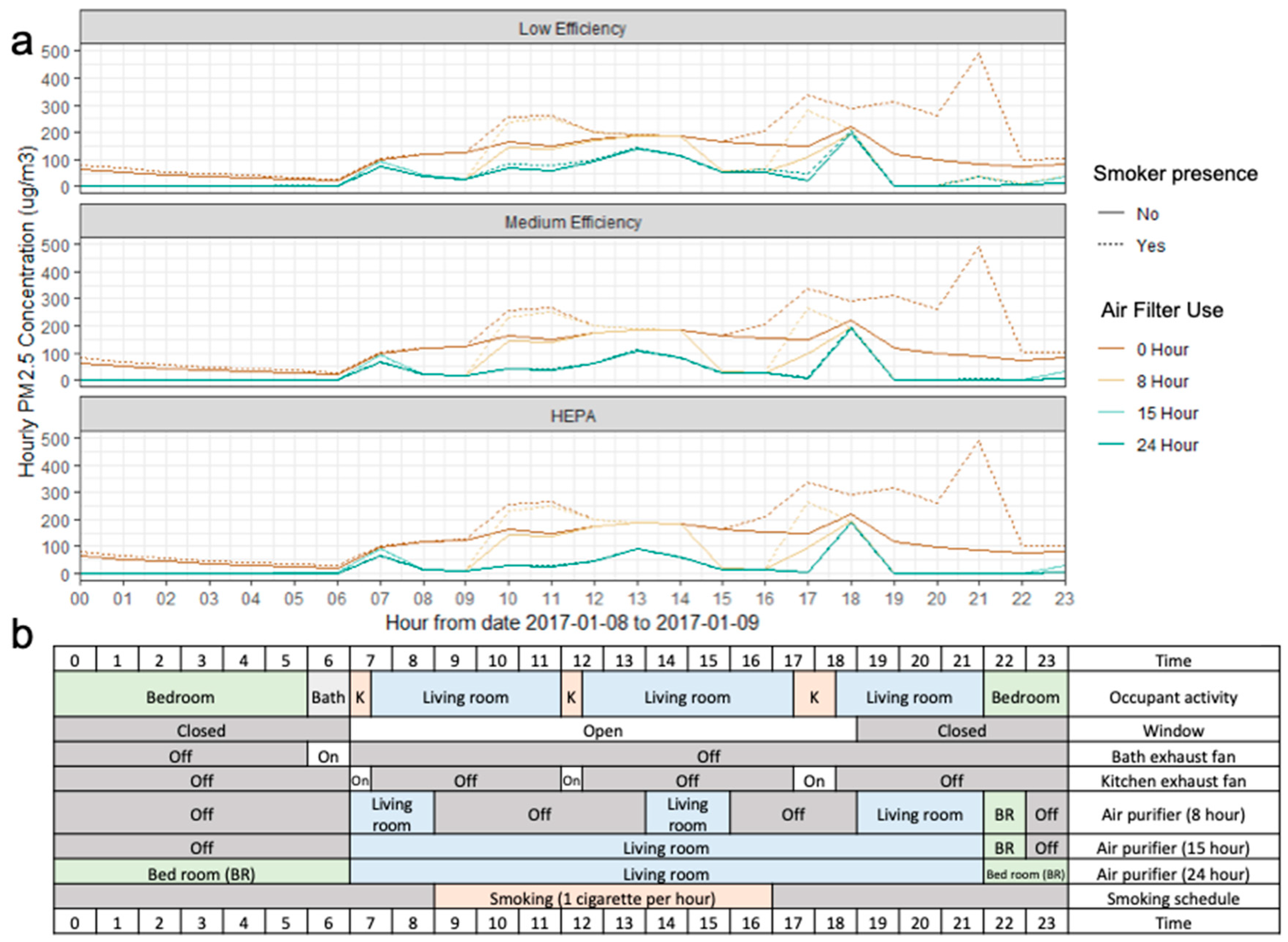
2.4. Simulation Scenarios
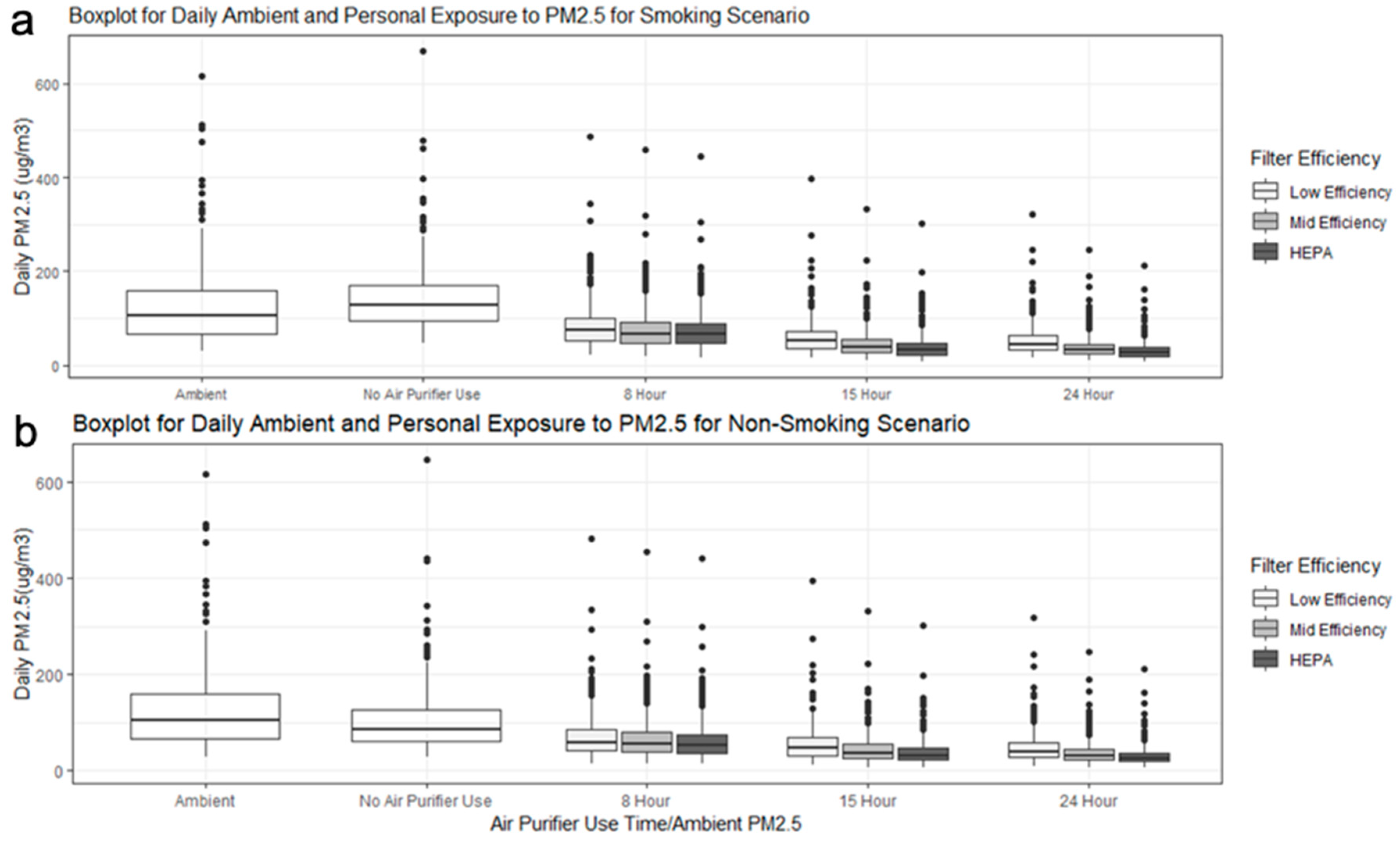
2.5. Statistical Analysis
2.6. Mortality Reduction Associated with Air Filter Use
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Smith, K.R.; McCracken, J.P.; Weber, M.W.; Hubbard, A.; Jenny, A.; Thompson, L.M.; Balmes, J.; Diaz, A.; Arana, B.; Bruce, N. Effect of reduction in household air pollution on childhood pneumonia in Guatemala (RESPIRE): A randomised controlled trial. Lancet 2011, 378, 1717–1726. [Google Scholar] [CrossRef]
- Meng, X.; Wang, C.; Cao, D.; Wong, C.-M.; Kan, H. Short-term effect of ambient air pollution on COPD mortality in four Chinese cities. Atmos. Environ. 2013, 77, 149–154. [Google Scholar] [CrossRef]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine Particulate Air Pollution and Hospital Admission for Cardiovascular and Respiratory Diseases. JAMA 2006, 295, 1127–1134. [Google Scholar] [CrossRef]
- Iii, C.A.P.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung Cancer, Cardiopulmonary Mortality, and Long-term Exposure to Fine Particulate Air Pollution. JAMA 2002, 287, 1132–1141. [Google Scholar]
- Pope, D.P.; Mishra, V.; Thompson, L.; Siddiqui, A.R.; Rehfuess, E.A.; Weber, M.; Bruce, N.G. Risk of Low Birth Weight and Stillbirth Associated with Indoor Air Pollution From Solid Fuel Use in Developing Countries. Epidemiol. Rev. 2010, 32, 70–81. [Google Scholar] [CrossRef]
- Gakidou, E.; Afshin, A.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Aboyans, V.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines for Indoor Air Quality: Household Fuel Combustion; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Balakrishnan, K.; Dey, S.; Gupta, T.; Dhaliwal, R.S.; Brauer, M.; Cohen, A.J.; Stanaway, J.D.; Beig, G.; Joshi, T.K.; Aggarwal, A.N.; et al. The impact of air pollution on deaths, disease burden, and life expectancy across the states of India: The Global Burden of Disease Study 2017. Lancet Planet. Health 2019, 3, e26–e39. [Google Scholar] [CrossRef]
- Pant, P.; Guttikunda, S.K.; Peltier, R.E. Exposure to particulate matter in India: A synthesis of findings and future directions. Environ. Res. 2016, 147, 480–496. [Google Scholar] [CrossRef]
- Smith, K.R. National burden of disease in India from indoor air pollution. Proc. Natl. Acad. Sci. USA 2000, 97, 13286–13293. [Google Scholar] [CrossRef]
- Balakrishnan, K.; Ghosh, S.; Ganguli, B.; Sambandam, S.; Bruce, N.; Barnes, D.F.; Smith, K.R. State and national household concentrations of PM2.5 from solid cookfuel use: Results from measurements and modeling in India for estimation of the global burden of disease. Environ. Health 2013, 12, 77. [Google Scholar] [CrossRef]
- Satsangi, P.G.; Yadav, S.; Pipal, A.S.; Kumbhar, N. Characteristics of trace metals in fine (PM2.5) and inhalable (PM10) particles and its health risk assessment along with in-silico approach in indoor environment of India. Atmos. Environ. 2014, 92, 384–393. [Google Scholar] [CrossRef]
- Balakrishnan, K.; Sambandam, S.; Ramaswamy, P.; Mehta, S.; Smith, K.R. Exposure assessment for respirable particulates associated with household fuel use in rural districts of Andhra Pradesh, India. J. Expo. Sci. Environ. Epidemiol. 2004, 14, S14–S25. [Google Scholar] [CrossRef] [PubMed]
- Pant, P.; Habib, G.; Marshall, J.D.; Peltier, R.E. PM2.5 exposure in highly polluted cities: A case study from New Delhi, India. Environ. Res. 2017, 156, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Conibear, L.; Butt, E.W.; Knote, C.; Arnold, S.R.; Spracklen, D.V. Residential energy use emissions dominate health impacts from exposure to ambient particulate matter in India. Nat. Commun. 2018, 9, 617. [Google Scholar] [CrossRef]
- WHO Global Ambient Air Quality Database. Available online: http://www.who.int/airpollution/data/cities/en/ (accessed on 14 August 2018).
- Rajivan, A.K. Policy Implications for Gender Equity: The India Time Use Survey, 1998–1999. In Proceedings of the International Seminar on Time Use Surveys, Ahmedabad, Indian, 7–10 December 1999; p. 31. [Google Scholar]
- Shimada, Y.; Matsuoka, Y. Analysis of indoor PM2.5 exposure in Asian countries using time use survey. Sci. Total Environ. 2011, 409, 5243–5252. [Google Scholar] [CrossRef]
- Nazaroff, W.W. Indoor particle dynamics. Indoor Air 2004, 14, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Batterman, S.; Du, L.; Mentz, G.; Mukherjee, B.; Parker, E.; Godwin, C.; Chin, J.-Y.; O’Toole, A.; Robins, T.; Rowe, Z.; et al. Particulate matter concentrations in residences: An intervention study evaluating stand-alone filters and air conditioners. Indoor Air 2012, 22, 235–252. [Google Scholar] [CrossRef]
- Noonan, C.W.; Semmens, E.O.; Smith, P.; Harrar, S.W.; Montrose, L.; Weiler, E.; McNamara, M.; Ward, T.J. Randomized Trial of Interventions to Improve Childhood Asthma in Homes with Wood-burning Stoves. Environ. Health Perspect. 2017, 125, 097010. [Google Scholar] [CrossRef]
- Chen, R.; Zhao, A.; Chen, H.; Zhao, Z.; Cai, J.; Wang, C.; Yang, C.; Li, H.; Xu, X.; Ha, S.; et al. Cardiopulmonary benefits of reducing indoor particles of outdoor origin: A randomized, double-blind crossover trial of air purifiers. J. Am. Coll. Cardiol. 2015, 65, 2279–2287. [Google Scholar] [CrossRef]
- Vyas, S.; Srivastav, N.; Spears, D. An Experiment with Air Purifiers in Delhi during Winter 2015–2016. PLoS ONE 2016, 11, e0167999. [Google Scholar] [CrossRef]
- Cui, X.; Li, F.; Xiang, J.; Fang, L.; Chung, M.K.; Day, D.B.; Mo, J.; Weschler, C.J.; Gong, J.; He, L.; et al. Cardiopulmonary effects of overnight indoor air filtration in healthy non-smoking adults: A double-blind randomized crossover study. Environ. Int. 2018, 114, 27–36. [Google Scholar] [CrossRef]
- Xu, Y.; Raja, S.; Ferro, A.R.; Jaques, P.A.; Hopke, P.K.; Gressani, C.; Wetzel, L.E. Effectiveness of heating, ventilation and air conditioning system with HEPA filter unit on indoor air quality and asthmatic children’s health. Build. Environ. 2010, 45, 330–337. [Google Scholar] [CrossRef]
- Dutta, K.; Shields, K.N.; Edwards, R.; Smith, K.R. Impact of improved biomass cookstoves on indoor air quality near Pune, India. Energy Sustain. Dev. 2007, 11, 19–32. [Google Scholar] [CrossRef]
- Hanna, R.; Duflo, E.; Greenstone, M. Up in Smoke: The Influence of Household Behavior on the Long-Run Impact of Improved Cooking Stoves. Am. Econ. J.: Econ. Policy, Am. Econ. Assoc. 2012, 8, 80–114. [Google Scholar]
- Mukhopadhyay, R.; Sambandam, S.; Pillarisetti, A.; Jack, D.; Mukhopadhyay, K.; Balakrishnan, K.; Vaswani, M.; Bates, M.N.; Kinney, P.; Arora, N.; et al. Cooking practices, air quality, and the acceptability of advanced cookstoves in Haryana, India: An exploratory study to inform large-scale interventions. Glob. Health Act. 2012, 5, 19016. [Google Scholar] [CrossRef]
- Johnson, M.; Lam, N.; Brant, S.; Gray, C.; Pennise, D. Modeling indoor air pollution from cookstove emissions in developing countries using a Monte Carlo single-box model. Atmos. Environ. 2011, 45, 3237–3243. [Google Scholar] [CrossRef]
- Shao, D.; Du, Y.; Liu, S.; Brunekreef, B.; Meliefste, K.; Zhao, Q.; Chen, J.; Song, X.; Wang, M.; Wang, J.; et al. Cardiorespiratory responses of air filtration: A randomized crossover intervention trial in seniors living in Beijing: Beijing Indoor Air Purifier StudY, BIAPSY. Sci. Total Environ. 2017, 603–604, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Fabian, M.P.; Stout, N.K.; Adamkiewicz, G.; Geggel, A.; Ren, C.; Sandel, M.; Levy, J.I. The effects of indoor environmental exposures on pediatric asthma: A discrete event simulation model. Environ. Health Glob. Access Sci. Source 2012, 11, 66. [Google Scholar] [CrossRef] [PubMed]
- Fabian, P.; Adamkiewicz, G.; Levy, J.I. Simulating indoor concentrations of NO2 and PM2.5 in multi-family housing for use in health-based intervention modeling. Indoor Air 2012, 22, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.A.; Chiang, R.A. Quantitative Guidance for Stove Usage and Performance to Achieve Health and Environmental Targets. Environ. Health Perspect. 2015, 123, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Myatt, T.A.; Minegishi, T.; Allen, J.G.; MacIntosh, D.L. Control of asthma triggers in indoor air with air cleaners: A modeling analysis. Environ. Health 2008, 7, 43. [Google Scholar] [CrossRef] [PubMed]
- Polidoro, B. CONTAM. Available online: https://www.nist.gov/services-resources/software/contam (accessed on 13 August 2018).
- Dols, W.S.; Polidoro, B.J. CONTAM User Guide and Program Documentation Version 3.2; Technical Note. NIST TN-1887; National Institute of Standards and Technology: Gaithersburg, MD, USA, 2015.
- Pillarisetti, A.; Mehta, S.; Smith, K.R. HAPIT, the Household Air Pollution Intervention Tool, to Evaluate the Health Benefits and Cost-Effectiveness of Clean Cooking Interventions. In Broken Pumps and Promises; Springer: Cham, Switzerland, 2016; pp. 147–169. ISBN 978-3-319-28641-9. [Google Scholar]
- Rawal, R.; Shukla, Y. Residential Buildings in India: Energy Use Projections and Savings Potentials; Global Buildings Performance Network (GBPN): Paris, France, 2014. [Google Scholar]
- Shen, G.; Yang, Y.; Wang, W.; Tao, S.; Zhu, C.; Min, Y.; Xue, M.; Ding, J.; Wang, B.; Wang, R.; et al. Emission Factors of Particulate Matter and Elemental Carbon for Crop Residues and Coals Burned in Typical Household Stoves in China. Environ. Sci. Technol. 2010, 44, 7157–7162. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Petroleum and Natural Gas, Government of India. LPG Profile - data on LPG Marketing; Ministry of Petroleum & Natural Gas: New Delhi, India, 2017.
- Bureau of Energy Efficiency (BEE). User Guide for India’s 2047 Energy Calculator—Cooking Sector; Ministry of Power: New Delhi, India, 2015.
- International Institute for Population Sciences. Global Adult Tobacco Survey—India 2009–2010; International Institute for Population Sciences: Mumbai, India, 2010. [Google Scholar]
- Method of Testing General Ventilation Air-Cleaning Devices for Removal Efficiency by Particle Size: ANSI/ASHRAE Standard 52.2-2017; ASHRAE: Atlanta, GA, USA, 2017.
- Azimi, P.; Zhao, D.; Stephens, B. Estimates of HVAC filtration efficiency for fine and ultrafine particles of outdoor origin. Atmos. Environ. 2014, 98, 337–346. [Google Scholar] [CrossRef]
- EnergyPlus. Available online: https://energyplus.net/weather (accessed on 14 April 2018).
- Ministry of Environment & Forests of Government of India Central Pollution Control Board (CPCB). Available online: http://www.cpcb.gov.in/CAAQM/frmUserAvgReportCriteria.aspx (accessed on 15 April 2019).
- Gordon, T.; Balakrishnan, K.; Dey, S.; Rajagopalan, S.; Thornburg, J.; Thurston, G.; Agrawal, A.; Collman, G.; Guleria, R.; Limaye, S.; et al. Air pollution health research priorities for India: Perspectives of the Indo-U.S. Communities of Researchers. Environ. Int. 2018, 119, 100–108. [Google Scholar] [CrossRef] [PubMed]
- American National Standards Institute Method for Measuring Performance of Portable Household Electric Room Air Cleaners: ANSI/AHAM AC-1-2015; Association of Home Appliance Manufacturers: Washington, DC, USA, 2015.
- CONTAM Results Export Tool. Available online: https://pages.nist.gov/CONTAM-apps/webapps/contam_results_exporter/index.htm (accessed on 20 June 2018).
- ICMR; PHFI; IHME Indian Council of Medical Research, Public Health Foundation of India, and Institute for Health Metrics and Evaluation. Available online: http://vizhub.healthdata.org/gbd-compare/india (accessed on 6 December 2018).
- Haghighat, F.; Megri, A.C. A Comprehensive Validation of Two Airflow Models—COMIS and CONTAM. Indoor Air 1996, 6, 278–288. [Google Scholar] [CrossRef]
- Emmerich, S.J.; Nabinger, S.J. Measurement and Simulation of the IAQ Impact of Particle Cleaners in a Single-Zone Building; NIST InteragencyInternal Rep. NISTIR-6461; National Institute of Standards and Technology: Gaithersburg, MD, USA, 2000.
- Massey, D.; Kulshrestha, A.; Masih, J.; Taneja, A. Seasonal trends of PM10, PM5.0, PM2.5 & PM1.0 in indoor and outdoor environments of residential homes located in North-Central India. Build. Environ. 2012, 47, 223–231. [Google Scholar]
- Barn, P.; Gombojav, E.; Ochir, C.; Boldbaatar, B.; Beejin, B.; Naidan, G.; Galsuren, J.; Legtseg, B.; Byambaa, T.; Hutcheon, J.A.; et al. The effect of portable HEPA filter air cleaner use during pregnancy on fetal growth: The UGAAR randomized controlled trial. Environ. Int. 2018, 121, 981–989. [Google Scholar] [CrossRef]
- Barn, P.; Gombojav, E.; Ochir, C.; Laagan, B.; Beejin, B.; Naidan, G.; Boldbaatar, B.; Galsuren, J.; Byambaa, T.; Janes, C.; et al. The effect of portable HEPA filter air cleaners on indoor PM2.5 concentrations and second hand tobacco smoke exposure among pregnant women in Ulaanbaatar, Mongolia: The UGAAR randomized controlled trial. Sci. Total Environ. 2018, 615, 1379–1389. [Google Scholar] [CrossRef]
- Yuchi, W.; Gombojav, E.; Boldbaatar, B.; Galsuren, J.; Enkhmaa, S.; Beejin, B.; Naidan, G.; Ochir, C.; Legtseg, B.; Byambaa, T.; et al. Evaluation of random forest regression and multiple linear regression for predicting indoor fine particulate matter concentrations in a highly polluted city. Environ. Pollut. 2019, 245, 746–753. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model Input Parameter | Parameter Description | Schedule | Reference |
|---|---|---|---|
| Floor plan | Apartment containing 1 living room, kitchen, bathroom, and bedroom, 30 m2 | Residential buildings in India: energy use and saving potentials, Global building performance network, 2014 [38] | |
| Wall leakage | Wall leakage area 5 cm2/m2 | Residential buildings in India: energy use and saving potentials, Global building performance network, 2014 [38] | |
| Window | 0.8 m2 open area in total | Open: 7:00–18:00 | |
| Bath exhaust fan | 120 m3/h (70 cfm †) | On: 6:00–7:00 | Fabian et al., 2011, Indoor Air [31] |
| Kitchen exhaust fan | 170 m3/h (100 cfm) | On when cooking (7:00–7:30; 12:00–12:30; 17:00–18:00) | Fabian et al., 2011, Indoor Air [31] |
| Source/Sink and Parameter | Emission/Removal Rate | Schedule | Source |
|---|---|---|---|
| Cooking | +0.14 mg/min | 2 h a day | |
| 7:00–7:30; 12:00–12:30; 17:00–18:00 | Shen et al., 2018, Environmental Science and Technology [39] | ||
| Smoking | +0.33 mg/min | 8 cigarettes per day, one per hour from 9:00–14:00 in the day time | Fabian et al., 2011, Indoor Air [31] |
| PM2.5 deposition | −0.19/h | Fabian et al., 2011, Indoor Air [31] | |
| Air Filter at 200 Clean Air Delivery Rate (CADR), PM2.5 removal efficiency | HEPA filter: 0.99 | Either 8 h, 15 h, or 24 h a day | Azimi et al., 2014, Atmospheric Environment [44] |
| Medium efficiency filter: 0.65 | |||
| Low efficiency filter: 0.3 | |||
| Weather | Typical meteorological year (TMY) hourly weather data from Energy Plus [45] |
| Annual Mean PM2.5 Exposure (μg/m3) | Mortality (% of Avoidable †) Averted per Million People | ||||
|---|---|---|---|---|---|
| Smoker Absent | Smoker Present | Smoker Absent | Smoker Present | ||
| 8-hour Air Filter use | No Air Filter | 103 | 137 | NA | NA |
| Low efficiency filter | 71 | 84 | 61 (8.3) | 75 (10.2) | |
| Mid efficiency filter | 65 | 77 | 77 (10.3) | 90 (12.1) | |
| HEPA filter | 62 | 78 | 85 (11.5) | 88 (11.9) | |
| 15-hour Air filter use | Low efficiency filter | 56 | 60 | 104 (14) | 134 (18.1) |
| Mid efficiency filter | 44 | 46 | 150 (20.2) | 184 (24.8) | |
| HEPA filter | 39 | 40 | 174 (23.5) | 212 (28.6) | |
| All day air filter use | Low efficiency filter | 50 | 56 | 125 (16.9) | 146 (19.8) |
| Mid efficiency filter | 35 | 38 | 196 (26.5) | 222 (30) | |
| HEPA filter | 29 | 30 | 235 (31.8) | 271 (36.6) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, J.; Ye, W.; Pillarisetti, A.; Clasen, T.F. Modeling the Impact of an Indoor Air Filter on Air Pollution Exposure Reduction and Associated Mortality in Urban Delhi Household. Int. J. Environ. Res. Public Health 2019, 16, 1391. https://doi.org/10.3390/ijerph16081391
Liao J, Ye W, Pillarisetti A, Clasen TF. Modeling the Impact of an Indoor Air Filter on Air Pollution Exposure Reduction and Associated Mortality in Urban Delhi Household. International Journal of Environmental Research and Public Health. 2019; 16(8):1391. https://doi.org/10.3390/ijerph16081391
Chicago/Turabian StyleLiao, Jiawen, Wenlu Ye, Ajay Pillarisetti, and Thomas F. Clasen. 2019. "Modeling the Impact of an Indoor Air Filter on Air Pollution Exposure Reduction and Associated Mortality in Urban Delhi Household" International Journal of Environmental Research and Public Health 16, no. 8: 1391. https://doi.org/10.3390/ijerph16081391
APA StyleLiao, J., Ye, W., Pillarisetti, A., & Clasen, T. F. (2019). Modeling the Impact of an Indoor Air Filter on Air Pollution Exposure Reduction and Associated Mortality in Urban Delhi Household. International Journal of Environmental Research and Public Health, 16(8), 1391. https://doi.org/10.3390/ijerph16081391