Factors Associated with Levels of Latrine Completion and Consequent Latrine Use in Northern Ghana

Abstract
1. Introduction
- (1)
- How do the levels of latrine completion relate to latrine use?
- (2)
- How are socio-demographic characteristics of households linked to levels of latrine completion?
- (3)
- What factors may deter households of different latrine completion levels from using their latrines?
- (4)
- How do psychosocial factors differ between households’ latrine completion levels?
- (5)
- How do reported reasons for latrine building differ between households’ latrine completion levels?
2. Methods
2.1. Research Context and Sampling
2.2. Data Collection
2.3. Measures
2.3.1. Latrine Construction
2.3.2. Latrine Usage
2.3.3. Socio-Demographic Factors
2.3.4. Psychosocial Determinants
2.3.5. Level of Latrine Construction
2.4. Data Analysis Procedure
3. Results
3.1. Level 1 (L1): Only Pit Is Dug
3.2. Level 2 (L2): Pit Is Dug and Superstructure Constructed (Pit + Superstructure)
3.3. Level 3 (L3): Pit Is Dug, Superstructure Constructed and Latrine Is Roofed (Pit + Superstructure + Roof)
3.4. Level 4 (L4): Pit Is Dug, Superstructure Constructed, Latrine Is Roofed and Has Door (Pit + Superstructure + Roof + Door)
3.5. Level 5: Pit Is Dug, Superstructure Constructed, Latrines Is Roofed, Latrine Has Door and a Vent Pipe (Pit + Superstructure + Roof +Door + Vent Pipe)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines. 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/258617/9789241512893-eng.pdf?sequence=1 (accessed on 17 August 2018).
- Liu, L.; Oza, S.; Hogan, D.; Perin, J.; Rudan, I.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: An updated systematic analysis. Lancet 2015, 385, 430–440. [Google Scholar] [CrossRef]
- Wolf, J.; Hunter, P.R.; Freeman, M.C.; Cumming, O.; Clasen, T.; Bartram, J.; Higgins, J.P.T.; Johnston, R.; Medlicott, K.; Boisson, S.; et al. Impact of drinking water, sanitation and handwashing with soap on childhood diarrhoeal disease: Updated meta-analysis and meta-regression. Trop. Med. Int. Health 2018, 23, 508–525. [Google Scholar] [CrossRef] [PubMed]
- Wolf, J.; Prüss-Ustün, A.; Cumming, O.; Bartram, J.; Bonjour, S.; Cairncross, S.; Clasen, T.; Colford, J.M., Jr.; Curtis, V.; De France, J.; et al. Systematic review: Assessing the impact of drinking water and sanitation on diarrhoeal disease in low-and middle-income settings: Systematic review and meta-regression. Trop. Med. Int. Health 2014, 19, 928–942. [Google Scholar] [CrossRef]
- Jenkins, M.W.; Sugden, S. Human Development Report 2006; United Nations Development Programme: New York, NY, USA, 2006. [Google Scholar]
- Global Water Initiative—West Africa. From Demonstration Latrines to Community Led Total Sanitation (CLTS). Available online: https://www.gwiwestafrica.org/en/demonstration-latrines-community-led-total-sanitation-clts-1 (accessed on 10 August 2018).
- Mosler, H.J. A systematic approach to behavior change interventions for the water and sanitation sector in developing countries: A conceptual model, a review, and a guideline. Int. J. Environ. Health Res. 2012, 22, 431–449. [Google Scholar] [CrossRef] [PubMed]
- Kar, K.; Chambers, R. Handbook on Community-Led Total Sanitation. 2008. Available online: https://www.communityledtotalsanitation.org/sites/communityledtotalsanitation.org/files/cltshandbook.pdf (accessed on 17 August 2018).
- Harvey, P. Community-led total sanitation, Zambia: Stick, carrot or balloon? Waterlines 2011, 30, 95–105. [Google Scholar] [CrossRef]
- Crocker, J.; Abodoo, E.; Asamani, D.; Domapielle, W.; Gyapong, B.; Bartram, J. Impact Evaluation of Training Natural Leaders during a Community-Led Total Sanitation Intervention: A Cluster-Randomized Field Trial in Ghana. Environ. Sci. Technol. 2016, 50, 8867–8875. [Google Scholar] [CrossRef]
- Garn, J.V.; Sclar, G.D.; Freeman, M.C.; Penakalapati, G.; Alexander, K.T.; Brooks, P.; Rehfuess, E.A.; Boisson, S.; Medlicott, K.O.; Clasen, T.F. The impact of sanitation interventions on latrine coverage and latrine use: A systematic review and meta-analysis. Int. J. Hyg. Environ. Health 2017, 220 2 Pt B, 329–340. [Google Scholar] [CrossRef]
- Venkataramanan, V.; Crocker, J.; Karon, A.; Bartram, J. Community-Led Total Sanitation: A Mixed-Methods Systematic Review of Evidence and Its Quality. Environ. Health Perspect. 2018, 126, 026001. [Google Scholar] [CrossRef]
- Mosler, H.J.; Mosch, S.; Harter, M. Is Community-Led Total Sanitation connected to the rebuilding of latrines? Quantitative evidence from Mozambique. PLoS ONE 2018, 13, e0197483. [Google Scholar] [CrossRef]
- Cameron, L.A.; Olivia, S.; Shah, M. Initial Conditions Matter: Social Capital and Participatory Development. 2015. Available online: http://dx.doi.org/10.2139/ssrn.2704614 (accessed on 20 August 2018).
- Dickin, S.; Bisung, E.; Savadogo, K. Sanitation and the commons: The role of collective action in sanitation use. Geoforum 2017, 86, 118–126. [Google Scholar] [CrossRef]
- Slekiene, J.; Mosler, H.J. Characterizing the Last Latrine Nonowners in Rural Malawi. Am. J. Trop. Med. Hyg. 2018, 98, 295–299. [Google Scholar] [CrossRef]
- Nielsen, L.; Riddle, M.; King, J.W.; Aklin, W.M.; Chen, W.; Clark, D.; Collier, E.; Czajkowski, S.; Esposito, L.; Ferrer, R.; et al. The NIH Science of Behavior Change Program: Transforming the science through a focus on mechanisms of change. Behav. Res. Ther. 2018, 101, 3–11. [Google Scholar] [CrossRef]
- Mosler, H.J.; Contzen, N. Systematic Behavior Change in Water, Sanitation and Hygiene. A Practical Guide Using the RANAS Approach. Version, 1.0. 2016. Available online: http://www.toiletboard.org/media/29-Guideline_V1.0_final_25_08_2016_druck_3.pdf (accessed on 14 July 2018).
- Alemu, F.; Kumie, A.; Medhin, G.; Gasana, J. The role of psychological factors in predicting latrine ownership and consistent latrine use in rural Ethiopia: A cross-sectional study. BMC Public Health 2018, 18, 229. [Google Scholar] [CrossRef]
- Harter, M.; Mosch, S.; Mosler, H.J. How does Community-Led Total Sanitation (CLTS) affect latrine ownership? A quantitative case study from Mozambique. BMC Public Health 2018, 18, 387. [Google Scholar] [CrossRef]
- Mosler, H.J.; Sonego, I.L. Improved latrine cleanliness through behaviour change and changes in quality of latrine construction: A longitudinal intervention study in rural Burundi. Int. J. Environ. Health Res. 2017, 27, 355–367. [Google Scholar] [CrossRef]
- Tumwebaze, I.K.; Mosler, H.J. Effectiveness of group discussions and commitment in improving cleaning behaviour of shared sanitation users in Kampala, Uganda slums. Soc. Sci. Med. 2015, 147, 72–79. [Google Scholar] [CrossRef]
- Jenkins, M.W.; Scott, B. Behavioral indicators of household decision-making and demand for sanitation and potential gains from social marketing in Ghana. Soc. Sci. Med. 2007, 64, 2427–2442. [Google Scholar] [CrossRef]
- Jones, P.S. Mind the gap: Access to ARV medication, rights and the politics of scale in South Africa. Soc. Sci. Med. 2012, 74, 28–35. [Google Scholar] [CrossRef]
- King, B. Political ecologies of health. Prog. Hum. Geogr. 2010, 34, 38–55. [Google Scholar] [CrossRef]
- Asfaw, B.; Azage, M.; Gebregergs, G.B. Latrine access and utilization among people with limited mobility: A cross sectional study. Arch. Public Health 2016, 74, 9. [Google Scholar] [CrossRef]
- Leshargie, C.T.; Alebel, A.; Negesse, A.; Mengistu, G.; Wondemagegn, A.T.; Mulugeta, H.; Tesfaye, B.; Alamirew, N.M.; Wagnew, F.; Belay, Y.A.; et al. Household latrine utilization and its association with educational status of household heads in Ethiopia: A systematic review and meta-analysis. BMC Public Health 2018, 18, 901. [Google Scholar] [CrossRef]
- Yimam, Y.T.; Gelaye, K.A.; Chercos, D.H. Latrine utilization and associated factors among people living in rural areas of Denbia district, Northwest Ethiopia, 2013, a cross-sectional study. Pan Afr. Med J. 2014, 18, 334. [Google Scholar] [CrossRef]
- Oljira, D.; Berkessa, T.S. Latrine Use and Determinant Factors in Southwest Ethiopia. J. Epidemiol. Public Health Rev. 2016, 1. [Google Scholar] [CrossRef]
- Barnard, S.; Routray, P.; Majorin, F.; Peletz, R.; Boisson, S.; Sinha, A.; Clasen, T. Impact of Indian Total Sanitation Campaign on latrine coverage and use: A cross-sectional study in Orissa three years following programme implementation. PLoS ONE 2013, 8, e71438. [Google Scholar] [CrossRef]
- Coffey, D.; Gupta, A.; Hathi, P.; Khurana, N.; Spears, D.; Srivastav, N.; Vyas, S. Revealed preference for open defecation. Econ. Polit. Wkly. 2014, 49, 43–55. [Google Scholar]
- Ghana Statistical Service. Ghana Multiple Indicator Cluster Survey with an Enhanced Malaria Module and Biomarker. Final Report. Available online: https://dhsprogram.com/publications/publication-fr262-other-final-reports.cfm (accessed on 20 July 2018).
- Ghana Statistical Service. 2010 Population & Housing Census: Regional Analytical Report, Northern Region. Available online: http://www.statsghana.gov.gh/docfiles/2010phc/2010_PHC_Regional_Analytical_Reports_Northern_Region.pdf (accessed on 20 July 2018).
- Hoffmeyer-Zlotnik, J.H. New sampling designs and the quality of data. Dev. Appl. Stat. 2003, 19, 205–217. [Google Scholar]
- O’Reilly, K.; Dhanju, R.; Goel, A. Exploring “The Remote” and “The Rural”: Open Defecation and Latrine Use in Uttarakhand, India. World Dev. 2017, 93, 193–205. [Google Scholar] [CrossRef]
- Shakya, H.B.; Christakis, N.A.; Fowler, J.H. Social network predictors of latrine ownership. Soc. Sci. Med. 2015, 125, 129–138. [Google Scholar] [CrossRef]
- Alemu, F.; Kumie, A.; Medhin, G.; Gebre, T.; Godfrey, P. A socio-ecological analysis of barriers to the adoption, sustainablity and consistent use of sanitation facilities in rural Ethiopia. BMC Public Health 2017, 17, 706. [Google Scholar] [CrossRef]
- Coffey, D.; Spears, D.; Vyas, S. Switching to sanitation: Understanding latrine adoption in a representative panel of rural Indian households. Soc. Sci. Med. 2017, 188, 41–50. [Google Scholar] [CrossRef]
- Dickinson, K.; Pattanayak, S. Open Sky Latrines: Do Social Effects Influence Technology Adoption in the Case of a (Very) Impure Public Good. Duke University, 2012. Available online: https://pdfs.semanticscholar.org/d478/f70cc4a5ff401b4e6a4ea826495336821e9b.pdf (accessed on 16 July 2018).
- O’Connell, K.A. What influence open defecaton and latrine ownership in rural households?: Findings from a Global Review. Retrieved from Washington, DC. Available online: https://www.issuelab.org/resources/19200/19200.pdf (accessed on 30 September 2018).
- Anthonj, C.; Diekkruger, B.; Borgemeister, C.; Thomas, K. Health risk perceptions and local knowledge of water-related infectious disease exposure among Kenyan wetland communities. Int. J. Hyg. Environ. Health 2019, 222, 34–48. [Google Scholar] [CrossRef]
- Anthonj, C.; Fleming, L.; Godfrey, S.; Ambelu, A.; Bevan, J.; Cronk, R.; Bartram, J. Health Risk Perceptions Are Associated with Domestic Use of Basic Water and Sanitation Services-Evidence from Rural Ethiopia. Int. J. Environ. Res. Public Health 2018, 15, 2112. [Google Scholar] [CrossRef]
- Anthonj, C.; Githinji, S.; Kistemann, T. The impact of water on health and ill-health in a sub-Saharan African wetland: Exploring both sides of the coin. Sci. Total Environ. 2018, 624, 1411–1420. [Google Scholar] [CrossRef]
- Wiedemann, P.M.; Schutz, H. The precautionary principle and risk perception: Experimental studies in the EMF area. Environ. Health Perspect. 2005, 113, 402–405. [Google Scholar] [CrossRef]
- Renner, B.; Schupp, H.; Vollmann, M.; Hartung, F.M.; Schmälzle, R.; Panzer, M. Risk perception, risk communication and health behavior change: Health psychology at the University of Konstanz. Z. Gesundh. 2008, 16, 150–153. [Google Scholar] [CrossRef]
- Jenkins, M.W.; Curtis, V. Achieving the ‘good life’: Why some people want latrines in rural Benin. Soc. Sci. Med. 2005, 61, 2446–2459. [Google Scholar] [CrossRef]
- Kar, K. Subsidy or Self-Respect? Participatory Total Community Sanitation in Bangladesh; Working paper series, 184; IDS: Brighton, UK, 2003. [Google Scholar]
- Kar, K.; Pasteur, K. Subsidy or Self-Respect? Community Led Total Sanitation. An Update on Recent Developments; Working paper series, 257; IDS: Brighton, UK, 2005. [Google Scholar]
- Guiteras, R.; Levinsohn, J.; Mobarak, A.M. Encouraging sanitation investment in the developing world: A cluster-randomized trial. Science 2015, 348, 903–906. [Google Scholar] [CrossRef]
- Crocker, J.; Saywell, D.; Bartram, J. Sustainability of community-led total sanitation outcomes: Evidence from Ethiopia and Ghana. Int. J. Hyg. Environ. Health 2017, 220, 551–557. [Google Scholar] [CrossRef]
- Biran, A.; Danquah, L.; Chunga, J.; Schmidt, W.P.; Holm, R.; Itimu-Phiri, A.; Singini, W.; Jones, H.; Kuper, H.; White, S. A Cluster-Randomized Trial to Evaluate the Impact of an Inclusive, Community-Led Total Sanitation Intervention on Sanitation Access for People with Disabilities in Malawi. Am. J. Trop. Med. Hyg. 2018, 98, 984–994. [Google Scholar] [CrossRef]
- Movik, S.; Mehta, L. The Dynamics and Sustainability of Community-Led Total Sanitation (CLTS): Mapping Challenges and Pathways. Available online: https://opendocs.ids.ac.uk/opendocs/bitstream/handle/123456789/7972/CLTS_web.pdf?sequence=1 (accessed on 27 February 2019).
- White, S.; Kuper, H.; Itimu-Phiri, A.; Holm, R.; Biran, A. A qualitative study of barriers to accessing water, sanitation and hygiene for disabled people in Malawi. PLoS ONE 2016, 11, e0155043. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Defecation Habits | L1 | L2 | L3 | L4 | L5 |
|---|---|---|---|---|---|
| Description of levels | only pit | pit + superstructure | pit + superstructure + roof | pit + superstructure + roof + door | pit + superstructure + roof + door + vent pipe |
| n | 362 | 108 | 96 | 270 | 687 |
| Use latrine exclusively | 5.2% | 13.0% | 53.1% | 95.6% | 94.3% |
| Defecate in the open exclusively | 94.8% A,*** | 87.0% B,*** | 46.9% C,*** | 4.4% | 5.7% |
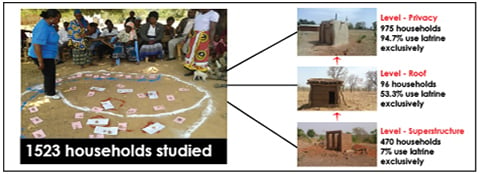
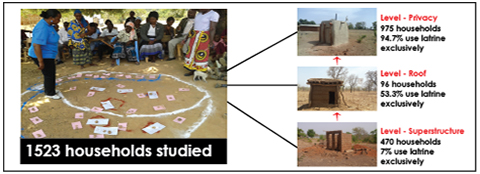
| Defecation Habits | Level-Superstructure | Level-Roof | Level-Privacy |
|---|---|---|---|
| Description of Level | (pit + superstructure) | (pit + superstructure + roof) | (pit + superstructure + roof + door + vent pipe) |
| n | 470 | 96 | 957 |
| Use latrine exclusively | 7.0% | 53.10% | 94.70% |
| Defecate in the open | 93.0% A,*** | 46.9% B,*** | 5.3% |
| Characteristics of Respondents and Households | Level-Superstructure | Level-Roof | Level-Privacy |
|---|---|---|---|
| n | 470 | 96 | 957 |
| Gender | |||
| Males | 62.80% | 67.70% | 66.60% |
| Age | 43.79 (16.17) | 44.10 (16.25) | 45.89 (15.96) |
| Household size | 9.20 (5.22) | 9.93 (4.85) | 10.26 (6.41) |
| Men | 3.37 (2.40) | 3.74 (2.27) | 3.54 (2.22) |
| Women | 3.71 (2.58) | 4.41 (3.21) | 3.89 (2.80) |
| children under age 5 years | 2.39 (2.13) | 2.69 (2.32) | 2.54 (2.80) |
| Income (Ghana Cedis) | 164.65 (259.109) A,* | 102.37 (125.36) B,* | 157.35 (263.92) |
| Are you able to read and write | 17.00% | 13.50% | 14.40% |
| Marital Status | |||
| Single married | 55.70% | 50.00% | 51.80% |
| Single | 9.80% | 8.30% | 6.10% |
| Widowed | 6.60% | 8.30% | 6.40% |
| Cohabiting | 0.00% | 0.00% | 0.40% |
| Divorced/separated | 1.10% | 0.00% | 0.50% |
| Polygamy married | 26.80% | 33.30% | 34.80% |
| Factors that may Deter Latrine Use | Level-Superstructure | Level-Roof | Level-Privacy |
|---|---|---|---|
| n | 470 | 96 | 957 |
| What are the reasons against the use of your own latrine? C | |||
| Smell | 22.20% | 19.50% | 18.20% |
| Too dirty/no hygiene | 25.40% | 12.40% | 18.30% |
| Fear of animals | 1.70% | 0.00% | 0.00% |
| Fear of falling inside | 0.40% | 0.00% | 0.30% |
| Queue of people | 0.20% | 1.00% | 0.70% |
| Latrine is damaged | 30.20% | 33.30% | 32.00% |
| Full pit | 7.60% | 7.30% | 7.40% |
| Other reasons | 4.00% | 9.40% | 5.20% |
| No reason | 17.90% | 16.70% | 16.40% |
| How clean is your own latrine? D | 3.89 (1.13) | 4.25 (1.06) B,** | 4.56 (0.74) |
| Cleanliness of latrine (Field observation) C | |||
| Seems unused | 14.80% | 14.60% | 2.60% |
| Clean: no dirt, no faeces | 2.80% | 18.80% | 55.30% |
| Somewhat clean. Some dirt but no faeces | 1.90% | 20.80% | 35.70% |
| Dirty: faeces on slab | 0.90% | 6.30% | 4.70% |
| Still under construction | 79.60% | 39.60% | 1.70% |
| RANAS Psychosocial Determinants | Level-Superstructure | Level-Roof | Level-Privacy |
|---|---|---|---|
| n | 470 | 96 | 957 |
| RANAS | Mean (SD) | Mean (SD) | Mean (SD) |
| Risk | |||
| Generally, how high do you think is the chance/risk that you get diarrhoea? | 3.29 (1.41) A,* | 2.92 (1.46) | 2.89 (1.52) |
| Imagine that you have diarrhoea, how severe would be the impact on your life? | 4.56 (0.83) | 4.59 (0.80) | 4.57 (0.78) |
| Latrine construction attitudes | |||
| How proud are you of your own latrine? | 4.78 (0.59) | 4.80 (0.49) | 4.79 (0.56) |
| Do you think you are more respected by your community because you have an own latrine? | 4.71 (0.65) | 4.56 (0.80) | 4.68 (0.69) |
| If you construct a latrine, do you think you are more vulnerable for envy? | 2.55 (1.60) | 2.32 (1.45) | 2.31 (1.58) |
| Do you think that constructing your own latrine is expensive? | 3.86 (1.23) A,* | 3.54 (1.39) | 3.58 (1.35) |
| How difficult is it to find the money to construct your own latrine? | 3.99 (1.21) | 3.63 (1.28) | 3.66 (1.38) |
| How difficult is it to find the time and effort to construct your own latrine? | 2.52 (1.61) | 2.84 (1.59) | 2.68 (1.58) |
| Latrine construction norms | |||
| When you constructed your latrine, how many members of your community already had one? | 2.22 (1.24) | 2.30 (1.15) | 2.02 (1.20) |
| How many of your relatives within your community constructed an own latrine? | 3.18 (1.57) A,*** | 4.24 (1.17) | 4.35 (1.19) |
| How many members of your community constructed an own latrine? | 3.42 (1.40) A,*** | 4.25 (1.07) B,* | 4.47 (0.92) |
| How much do people who are important to you (e.g., family, parents, friends) approve that you construct a latrine? | 4.43 (0.97) | 4.30 (1.13) B,* | 4.45 (0.96) |
| People who are leaders in the community (e.g., opinion leader, Chief of village, etc.) how much do they promote that you construct an own latrine? | 4.23 (1.28) | 4.22 (1.32) B,** | 4.48 (1.00) |
| How much do you feel a personal obligation to construct an own latrine? | 4.52 (0.93) | 4.56 (0.87) | 4.51 (0.96) |
| Abilities | |||
| Latrine construction | |||
| How confident are you that you can construct a latrine even if this is difficult (e.g., gathering the materials)? | 4.30 (1.02) | 4.50 (0.75) | 4.52 (0.77) |
| How confident are you that you could finish the construction of a latrine even if problems arise (e.g., you run out of money)? | 4.12 (1.21) | 4.24 (1.16) B,** | 4.48 (0.83) |
| Imagine that the latrine got damaged. How confident are you that you will be able to repair the latrine again? | 4.54 (0.84) | 4.55 (0.77) | 4.66 (0.72) |
| Self-Regulation | |||
| How committed are you to construct your own latrine? | 4.65 (0.69) | 4.76 (0.45) | 4.77 (0.51) |
| Reasons for Latrine Construction | Level-Superstructure | Level-Roof | Level-Privacy |
|---|---|---|---|
| n | 470 | 96 | 957 |
| Why did you construct a latrine? C | |||
| Privacy | 0.60% | 10.20% | 23.70% |
| Security | 0.40% | 2.10% | 5.50% |
| Health | 3.60% | 16.30% | 31.60% |
| Hygiene | 0.20% | 6.20% | 15.10% |
| Comfort | 0.20% | 1.00% | 4.20% |
| Because of the community meeting done here | 0% | 0.00% | 1.70% |
| Because some people came and told us to do so | 0.40% | 6.20% | 7.30% |
| Open defecation is harmful | 0.20% | 4.20% | 8.70% |
| How did you know how to construct a latrine? C | |||
| Watched other members of the community | 0.60% | 9.30% | 24.60% |
| Saw it in another community | 0.40% | 2.00% | 12.20% |
| Someone came from outside and told me | 1.90% | 21.90% | 35% |
| I just tried without knowledge | 0.40% | 4.20% | 8.80% |
| Someone else did it for me | 1.10% | 3.10% | 9.60% |
| My father/husband did the construction | 0.40% | 7.30% | 9.60% |
| Who in your household made the final decision to construct a toilet? C | |||
| Head of Household | 77.40% | 79.20% | 80.30% |
| Family all together | 13.20% | 8.30% | 9.30% |
| Wife | 0.60% | 2.10% | 3.40% |
| Children | 3.60% | 1.00% | 3.40% |
| Land lord | 1.90% | 1.00% | 1.00% |
| Other | 3.20% | 8.30% | 4.80% |
| Do you have a plan how you can construct a latrine if you are running out of materials? C | |||
| Collect local materials | 30.90% | 41.40% | 32.80% |
| Buy materials somewhere | 30.20% | 15.50% | 27.00% |
| Go for local dealers | 0.20% | 1% | 0.60% |
| Borrow material from others | 7.80% | 11.50% | 11.90% |
| Ask relatives for help | 3.80% | 8.30% | 5.50% |
| Sell animals/farm products to buy more materials | 12.00% | 11.50% | 15.20% |
| Produce the materials by myself | 2.30% | 1.00% | 1.70% |
| No plan | 12.80% | 9.40% | 4.60% |
| How much did the construction of your latrine cost in Cedi (GHS)? | 338.0 (278.65) | 250.18 (277.80) | 363.45 (560.36) |
| Did you receive any subsidy for the construction of your own latrine within the last year? | |||
| Yes | 2.80% | 6.30% | 14.80% |
| No | 97.20% | 93.80% | 85.20% |
| What kind of subsidy did you receive? C | |||
| Materials | 2.30% | 6.30% | 12.00% |
| Labour | 0.40% | 0.00% | 0.90% |
| Other | 0.00% | 0.00% | 1.80% |
| Who provided you with this subsidy? | |||
| Government | 0.00% | 0.00% | 0.00% |
| NGO | 2.30% | 6.30% | 13.70% |
| People from other communities | 0.20% | 0.00% | 0.50% |
| Family | 0.00% | 0.00% | 40.00% |
| Other | 0.20% | 0.00% | 0.10% |
| How many times did the facilitator follow up in your community | 3.02 (1.22) | 3.20 (1.02) B,* | 3.53 (1.20) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nunbogu, A.M.; Harter, M.; Mosler, H.-J. Factors Associated with Levels of Latrine Completion and Consequent Latrine Use in Northern Ghana. Int. J. Environ. Res. Public Health 2019, 16, 920. https://doi.org/10.3390/ijerph16060920
Nunbogu AM, Harter M, Mosler H-J. Factors Associated with Levels of Latrine Completion and Consequent Latrine Use in Northern Ghana. International Journal of Environmental Research and Public Health. 2019; 16(6):920. https://doi.org/10.3390/ijerph16060920
Chicago/Turabian StyleNunbogu, Abraham Marshall, Miriam Harter, and Hans-Joachim Mosler. 2019. "Factors Associated with Levels of Latrine Completion and Consequent Latrine Use in Northern Ghana" International Journal of Environmental Research and Public Health 16, no. 6: 920. https://doi.org/10.3390/ijerph16060920
APA StyleNunbogu, A. M., Harter, M., & Mosler, H.-J. (2019). Factors Associated with Levels of Latrine Completion and Consequent Latrine Use in Northern Ghana. International Journal of Environmental Research and Public Health, 16(6), 920. https://doi.org/10.3390/ijerph16060920