Factors Associated with Participation of Community-Dwelling Older Adults in a Home-Based Falls Prevention Program

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Home-Based Exercise Program
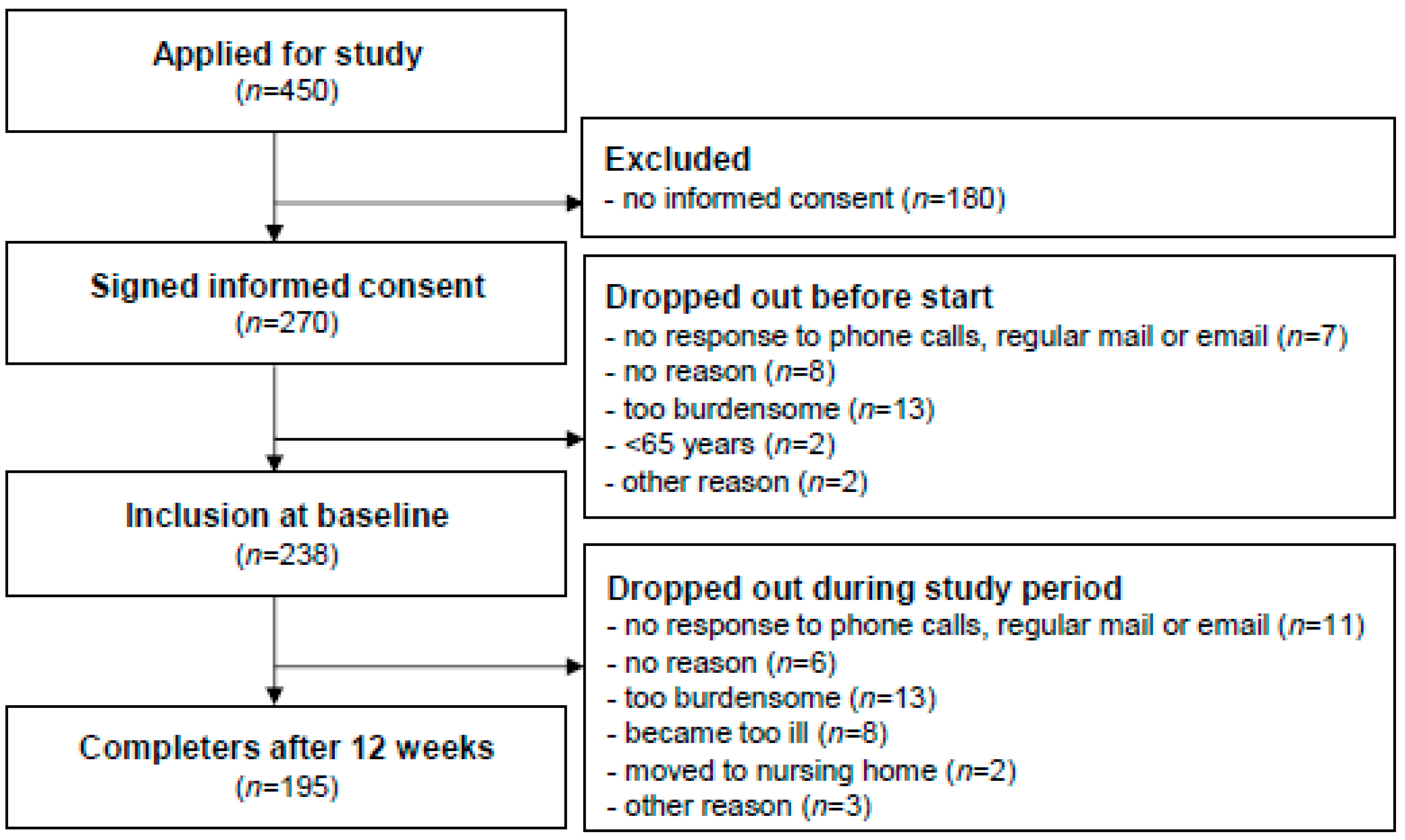
2.3. Recruitment
2.4. Outcome Variables
2.4.1. Participant Characteristics at Baseline and Follow-Up
2.4.2. Level of Participation
2.5. Statistical Analyses
2.5.1. Baseline Characteristics
2.5.2. Association between Factors and Frequent Participation
2.5.3. Effects of Frequent Participation on Health-Related Outcomes
2.5.4. Multicollinearity
3. Results
3.1. Baseline Characteristics
3.2. Association between Factors and Frequent Participation
3.3. Effects of Frequent Participation on Health-Related Outcomes
3.4. Multicollinearity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Haagsma, J.A.; Graetz, N.; Bolliger, I.; Naghavi, M.; Higashi, H.; Mullany, E.C.; Abera, S.F.; Abraham, J.P.; Adofo, K.; Alsharif, U.; et al. The global burden of injury: Incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study 2013. Inj. Prev. 2016, 22, 3–18. [Google Scholar] [CrossRef]
- Davis, J.C.; Robertson, M.C.; Ashe, M.C.; Liu-Ambrose, T.; Khan, K.M.; Marra, C.A. International comparison of cost of falls in older adults living in the community: A systematic review. Osteoporos. Int. 2010, 21, 1295–1306. [Google Scholar] [CrossRef]
- CBS Nederland. Population. Available online: http://www.cbs.nl/en-gb/society/population (accessed on 15 December 2018).
- VeiligheidNL. Privé-Valongevallen bij Ouderen—Ongevalscijfers 2017 (Private Fall-Related Accidents among Older Adults—Accident figures 2017. In Dutch). Available online: https://www.veiligheid.nl/valpreventie/kennis-en-cijfers/cijfers (accessed on 15 December 2018).
- Karlsson, M.K.; Magnusson, H.; von Schewelov, T.; Rosengren, B.E. Prevention of falls in the elderly—A review. Osteoporos. Int. 2013, 24, 747–762. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Michaleff, Z.A.; Fairhall, N.; Paul, S.S.; Tiedemann, A.; Whitney, J.; Cumming, R.G.; Herbert, R.D.; Close, J.C.; Lord, S.R. Exercise to prevent falls in older adults: An updated systematic review and meta-analysis. Br. J. Sports Med. 2016, 51, 1750–1758. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Brefka, S.; Denkinger, M. What works to prevent falls in community-dwelling older adults? An umbrella review of meta-analyses of randomized controlled trials. J. Am. Phys. Ther. Assoc. 2015, 95, 1095–1110. [Google Scholar] [CrossRef]
- Tricco, A.C.; Thomas, S.M.; Veroniki, A.A.; Hamid, J.S.; Cogo, E.; Strifler, L.; Khan, P.A.; Robson, R.; Sibley, K.M.; MacDonald, H.; et al. Comparisons of Interventions for Preventing Falls in Older Adults: A Systematic Review and Meta-analysis. JAMA 2017, 318, 1687–1699. [Google Scholar] [CrossRef] [PubMed]
- Yardley, L.; Kirby, S.; Ben-Shlomo, Y.; Gilbert, R.; Whitehead, S.; Todd, C. How likely are older people to take up different falls prevention activities? Prev. Med. 2008, 47, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Simek, E.M.; McPhate, L.; Haines, T.P. Adherence to and efficacy of home exercise programs to prevent falls: A systematic review and meta-analysis of the impact of exercise program characteristics. Prev. Med. 2012, 55, 262–275. [Google Scholar] [CrossRef] [PubMed]
- Osho, O.; Owoeye, O.; Armijo-Olivo, S. Adherence and Attrition in Fall Prevention Exercise Programs for Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. J. Aging Phys. Act. 2018, 26, 304–326. [Google Scholar] [CrossRef]
- Bongers, K.; Schoon, Y.; Graauwmans, M.; Hoogsteen-Ossewaarde, M.; Olde Rikkert, M. Safety, feasibility and reliability of the maximal step length, gait speed and chair test measured by seniors themselves: The Senior Step Study. J. Aging Phys. Act. 2015, 23, 438–443. [Google Scholar] [CrossRef]
- Campbell, A.J.; Robertson, M.C.; Gardner, M.M.; Norton, R.N.; Buchner, D.M. Falls prevention over 2 years: A randomized controlled trial in women 80 years and older. Age Ageing 1999, 28, 513–518. [Google Scholar] [CrossRef]
- Hoeymans, N.; van Lindert, H.; Westert, G.P. The health status of the Dutch population as assessed by the EQ-6D. Qual. Life Res. 2005, 14, 655–663. [Google Scholar] [CrossRef] [PubMed]
- VeiligheidNL. Valanalyse Inventarisatie Valrisico 65+ Door de Eerstelijnszorg (Fall Analysis Assessment Fall Risk 65+ by Primary Care. In Dutch). Available online: https://www.veiligheid.nl/valpreventie/interventies/screening/valanalyse (accessed on 15 December 2018).
- Richtlijnen Database. Preventie van Valincidenten bij Ouderen (Falls Prevention among Older Adults. In Dutch); Nederlandse Vereniging voor Klinische Geriatrie: Utrecht, The Netherlands, 2017. [Google Scholar]
- Podsiadlo, D.; Richardson, S. The timed “Up & GO”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Kempen, G.I.; Yardley, L.; van Haastregt, J.C.; Zijlstra, G.A.; Beyer, N.; Hauer, K.; Todd, C. The Short FES-I: A shortened version of the falls efficacy scale-international to assess fear of falling. Age Ageing 2008, 37, 45–50. [Google Scholar] [CrossRef]
- Cramm, J.M.; Strating, M.M.H.; de Vreede, P.L.; Steverink, N.; Nieboer, A.P. Validation of the self-management ability scale (SMAS) and development and validation of a shorter scale (SMAS-S) among older patients shortly after hospitalisation. Health Qual. Life Outcomes 2012, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Kempen, G.I. The MOS Short-Form General Health Survey: Single item vs. multiple measures of health-related quality of life: Some nuances. Psychol. Rep. 1992, 70, 608–610. [Google Scholar] [CrossRef]
- Thompson, F.T.; Levine, D.U. Examples of Easily Explainable Suppressor Variables in Multiple Regression Research. Mult. Linear Regres. Viewp. 1997, 24, 11–13. [Google Scholar]
- Hinkle, D.E.; Wiersma, W.; Jurs, S.G. Applied Statistics for the Behavioral Sciences, 5th ed.; Houghton Mifflin: Boston, MA, USA, 2003. [Google Scholar]
- Kutner, M.; Nachtsheim, C.; Neter, J. Applied Linear Statistical Models, 4th ed.; McGraw-Hill: Irwin, CA, USA, 2004. [Google Scholar]
- Curi, V.S.; Vilaca, J.; Haas, A.N.; Fernandes, H.M. Effects of 16-weeks of Pilates on health perception and sleep quality among elderly women. Arch. Gerontol. Geriatr. 2018, 74, 118–122. [Google Scholar] [CrossRef]
- De Lira, C.A.B.; Taveira, H.V.; Rufo-Tavares, W.; Amorim, A.D.S.; Ferreira, L.M.C.; Andrade, M.S.; Vancini, R.L. Engagement in a Community Physical Activity Program and Its Effects Upon the Health-Related Quality of Life of Elderly People: A Cross-Sectional Study. Value Health Reg. Issues 2018, 17, 183–188. [Google Scholar] [CrossRef]
- Nguyen, M.H.; Kruse, A. The effects of Tai Chi training on physical fitness, perceived health, and blood pressure in elderly Vietnamese. Open Access J. Sports Med. 2012, 3, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Robertson, M.C.; Campbell, A.J.; Gardner, M.M.; Devlin, N. Preventing injuries in older people by preventing falls: A meta-analysis of individual-level data. JAGS 2002, 50, 905–911. [Google Scholar] [CrossRef]
- Doubova, S.V.; Sanchez-Garcia, S.; Infante-Castaneda, C.; Perez-Cuevas, R. Factors associated with regular physical exercise and consumption of fruits and vegetables among Mexican older adults. BMC Public Health 2016, 16, 952. [Google Scholar] [CrossRef] [PubMed]
- Yamakita, M.; Kanamori, S.; Kondo, N.; Kondo, K. Correlates of Regular Participation in Sports Groups among Japanese Older Adults: JAGES Cross-Sectional Study. PLoS ONE 2015, 10, e0141638. [Google Scholar] [CrossRef]
- Walsh, J.M.E.; Pressman, A.R.; Cauley, J.A.; Browner, W.S. Predictors of Physical Activity in Community-dwelling Elderly White Women. J. Gen. Intern. Med. 2001, 16, 721–727. [Google Scholar] [CrossRef]
- Hawley-Hague, H.; Horne, M.; Skelton, D.A.; Todd, C. Review of how we should define (and measure) adherence in studies examining older adults’ participation in exercise classes. BMJ Open 2016, 6, e011560. [Google Scholar] [CrossRef] [PubMed]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older people’s perspectives on participation in physical activity: A systematic review and thematic synthesis of qualitative literature. Br. J. Sports Med. 2015, 49, 1268–1276. [Google Scholar] [CrossRef] [PubMed]
- Elskamp, A.B.; Hartholt, K.A.; Patka, P.; van Beeck, E.F.; van der Cammen, T.J. Why older people refuse to participate in falls prevention trials: A qualitative study. Exp. Gerontol. 2012, 47, 342–345. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| All Participants (n = 238) | Total Frequent and Infrequent or Nonparticipation (n = 195) | Frequent Participation (n = 102) | Infrequent or Nonparticipation (n = 93) | Difference between Frequent and Infrequent or Nonparticipation * | |
|---|---|---|---|---|---|
| Demographic characteristics | n (%) | n (%) | n (%) | n (%) | p-value |
| Female | 169 (71) | 140 (72) | 76 (75) | 64 (69) | 0.38 |
| Age—mean ± SD | 81.1 ± 6.7 | 80.9 ± 6.6 | 80.6 ± 6.4 | 81.3 ± 6.8 | 0.46 |
| Living alone | 151 (63) | 124 (64) | 66 (65) | 58 (62) | 0.73 |
| Education | |||||
| low | 70 (29) | 53 (27) | 24 (24) | 29 (31) | 0.23 |
| middle | 130 (55) | 108 (55) | 56 (55) | 52 (56) | 0.89 |
| high | 38 (16) | 34 (17) | 22 (22) | 12 (13) | 0.11 |
| Health-related outcomes | mean ± SD | mean ± SD | mean ± SD | mean ± SD | p-value |
| Quality of life (EQ-5D + cognition) 1 | 0.64 ± 0.24 | 0.65 ± 0.24 | 0.70 ± 0.23 | 0.60 ± 0.24 | 0.00 |
| Elevated fall risk—n (%) | 161 (69) a | 133 (69) d | 65 (64) g | 68 (75) i | 0.12 |
| Mobility (TUG) in seconds | 17.0 ± 9.1 b | 16.9 ± 8.9 e | 16.2 ± 7.9 h | 17.6 ± 10.0 j | 0.29 |
| Concern about falling (Short FES-I) | 9.8 ± 4.0 | 9.8 ± 3.9 | 9.9 ± 3.6 | 9.7 ± 4.1 | 0.77 |
| Self-management (SMAS-S) 2 | 59.3 ± 16.2 c | 60.1 ± 16.0 f | 63.8 ± 14.9 | 56.1 ± 16.3 k | 0.00 |
| General health (SF-20) 3 | |||||
| physical functioning | 45.1 ± 31.7 c | 45.1 ± 31.6 f | 50.2 ± 32.0 | 39.5 ± 30.2 k | 0.02 |
| role functioning | 28.8 ± 41.4 | 29.2 ± 41.1 | 34.3 ± 43.9 | 23.7 ± 37.3 | 0.07 |
| social functioning | 72.5 ± 34.0 | 74.5 ± 32.7 | 76.3 ± 32.5 | 72.5 ± 33.0 | 0.42 |
| mental health | 73.0 ± 20.7 c | 73.2 ± 20.8 f | 74.1 ± 20.8 g | 72.3 ± 20.7 | 0.55 |
| current health perceptions | 46.4 ± 21.1 c | 46.9 ± 21.1 f | 47.1 ± 20.5 | 46.7 ± 21.9 k | 0.89 |
| pain | 33.0 ± 27.6 | 31.9 ± 27.8 | 35.8 ± 27.1 | 27.7 ± 27.9 | 0.04 |
| Univariate | Multivariable Model 1 † | Multivariable Model 2 ‡ | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | OR (95% CI) | p-value | |
| Female | 1.33 (0.71–2.48) | 0.38 | 1.40 (0.66–2.98) | 0.38 | 1.12 (0.50–2.47) | 0.79 |
| Age | 0.98 (0.94–1.03) | 0.46 | 1.01 (0.96–1.06) | 0.78 | 1.01 (0.95–1.06) | 0.82 |
| Living alone | 1.11 (0.62–1.98) | 0.73 | 0.88 (0.45–1.74) | 0.72 | 0.82 (0.40–1.68) | 0.59 |
| Education | ||||||
| low | 0.68 (0.36–1.28) | 0.23 | 1.14 (0.55–2.37) | 0.72 | 1.51 (0.68–3.36) | 0.32 |
| middle | 0.96 (0.55–1.69) | 0.89 | 0.88 (0.42–1.82) | 0.72 | 0.66 (0.30–1.48) | 0.32 |
| high | 1.86 (0.86–4.00) | 0.12 | 1.93 (0.83–4.46) | 0.13 | 1.47 (0.60–3.62) | 0.40 |
| Quality of life (EQ-5D + cognition) | 3.52 (1.16–10.71) | 0.03 | 1.39 (0.21–9.31) | 0.73 | 0.63 (0.07–6.12) | 0.63 |
| Elevated fall risk | 0.72 (0.41–1.27) | 0.25 | 1.00 (0.49–2.03) | 1.00 | 0.96 (0.43–2.18) | 0.93 |
| Mobility (TUG) in seconds | 0.99 (0.96–1.03) | 0.72 | 1.02 (0.97–1.07) | 0.47 | 1.01 (0.95–1.06) | 0.84 |
| Concern about falling (Short FES-I) | 1.02 (0.96–1.09) | 0.50 | 1.07 (0.98–1.17) | 0.12 | 1.08 (0.98–1.18) | 0.14 |
| Self-management (SMAS-S) | 1.03 (1.01–1.05) | 0.00 | 1.02 (1.00–1.05) | 0.09 | 1.01 (0.98–1.04) | 0.64 |
| General health (SF-20) | ||||||
| physical functioning | 1.01 (1.00–1.02) | 0.07 | 1.00 (0.99–1.02) | 0.67 | 1.00 (0.99–1.02) | 0.69 |
| role functioning | 1.01 (1.00–1.01) | 0.09 | 1.00 (0.99–1.01) | 0.50 | 1.01 (0.99–1.02) | 0.41 |
| social functioning | 1.01 (1.00–1.01) | 0.27 | 1.00 (0.99–1.01) | 0.89 | 1.00 (0.99–1.01) | 0.91 |
| mental health | 1.00 (0.99–1.02) | 0.70 | 0.99 (0.97–1.01) | 0.20 | 0.98 (0.96–1.00) | 0.98 |
| current health perceptions | 1.01 (1.00–1.02) | 0.14 | 1.01 (0.99–1.03) | 0.27 | 1.01 (0.99–1.04) | 0.19 |
| pain | 1.01 (1.00–1.02) | 0.10 | 1.02 (1.01–1.04) | 0.00 | 1.02 (1.00–1.04) | 0.02 |
| Multivariable Model 1 † | Multivariable Model 2 ‡ | |||
|---|---|---|---|---|
| Logistic Regression | OR (95% CI) | p-value | OR (95% CI) | p-value |
| Elevated fall risk | 0.85 (0.43–1.71) | 0.65 | 0.90 (0.42–1.94) | 0.79 |
| Linear regression | B (SE) | p-value | B (SE) | p-value |
| Quality of life (EQ-6D) | 0.01 (0.03) | 0.78 | 0.01 (0.03) | 0.82 |
| Mobility (TUG) in seconds | −0.10 (0.94) | 0.92 | −0.57 (0.91) | 0.53 |
| Concern about falling (Short FES-I) | 0.30 (0.50) | 0.55 | 0.56 (0.51) | 0.27 |
| Self-management (SMAS-S) | 1.79 (1.55) | 0.25 | 1.20 (1.58) | 0.45 |
| General health (SF-20) | ||||
| physical functioning | 0.59 (3.49) | 0.87 | 1.38 (3.53) | 0.70 |
| role functioning | 2.91 (4.23) | 0.49 | 2.43 (4.08) | 0.55 |
| social functioning | 3.51 (4.32) | 0.42 | 1.97 (4.37) | 0.65 |
| mental health | −0.29 (2.01) | 0.89 | −0.49 (2.06) | 0.81 |
| current health perceptions | 4.49 (2.01) | 0.03 | 4.46 (1.99) | 0.03 |
| pain | 3.04 (3.59) | 0.40 | 6.62 (3.60) | 0.07 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olij, B.F.; Barmentloo, L.M.; Smilde, D.; van der Velde, N.; Polinder, S.; Schoon, Y.; Erasmus, V. Factors Associated with Participation of Community-Dwelling Older Adults in a Home-Based Falls Prevention Program. Int. J. Environ. Res. Public Health 2019, 16, 1087. https://doi.org/10.3390/ijerph16061087
Olij BF, Barmentloo LM, Smilde D, van der Velde N, Polinder S, Schoon Y, Erasmus V. Factors Associated with Participation of Community-Dwelling Older Adults in a Home-Based Falls Prevention Program. International Journal of Environmental Research and Public Health. 2019; 16(6):1087. https://doi.org/10.3390/ijerph16061087
Chicago/Turabian StyleOlij, Branko F., Lotte M. Barmentloo, Dini Smilde, Nathalie van der Velde, Suzanne Polinder, Yvonne Schoon, and Vicki Erasmus. 2019. "Factors Associated with Participation of Community-Dwelling Older Adults in a Home-Based Falls Prevention Program" International Journal of Environmental Research and Public Health 16, no. 6: 1087. https://doi.org/10.3390/ijerph16061087
APA StyleOlij, B. F., Barmentloo, L. M., Smilde, D., van der Velde, N., Polinder, S., Schoon, Y., & Erasmus, V. (2019). Factors Associated with Participation of Community-Dwelling Older Adults in a Home-Based Falls Prevention Program. International Journal of Environmental Research and Public Health, 16(6), 1087. https://doi.org/10.3390/ijerph16061087