Can an Exercise-Based Educational and Motivational Intervention be Durably Effective in Changing Compliance to Physical Activity and Anthropometric Risk in People with Type 2 Diabetes? A Follow-Up Study

 ,
, 
 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
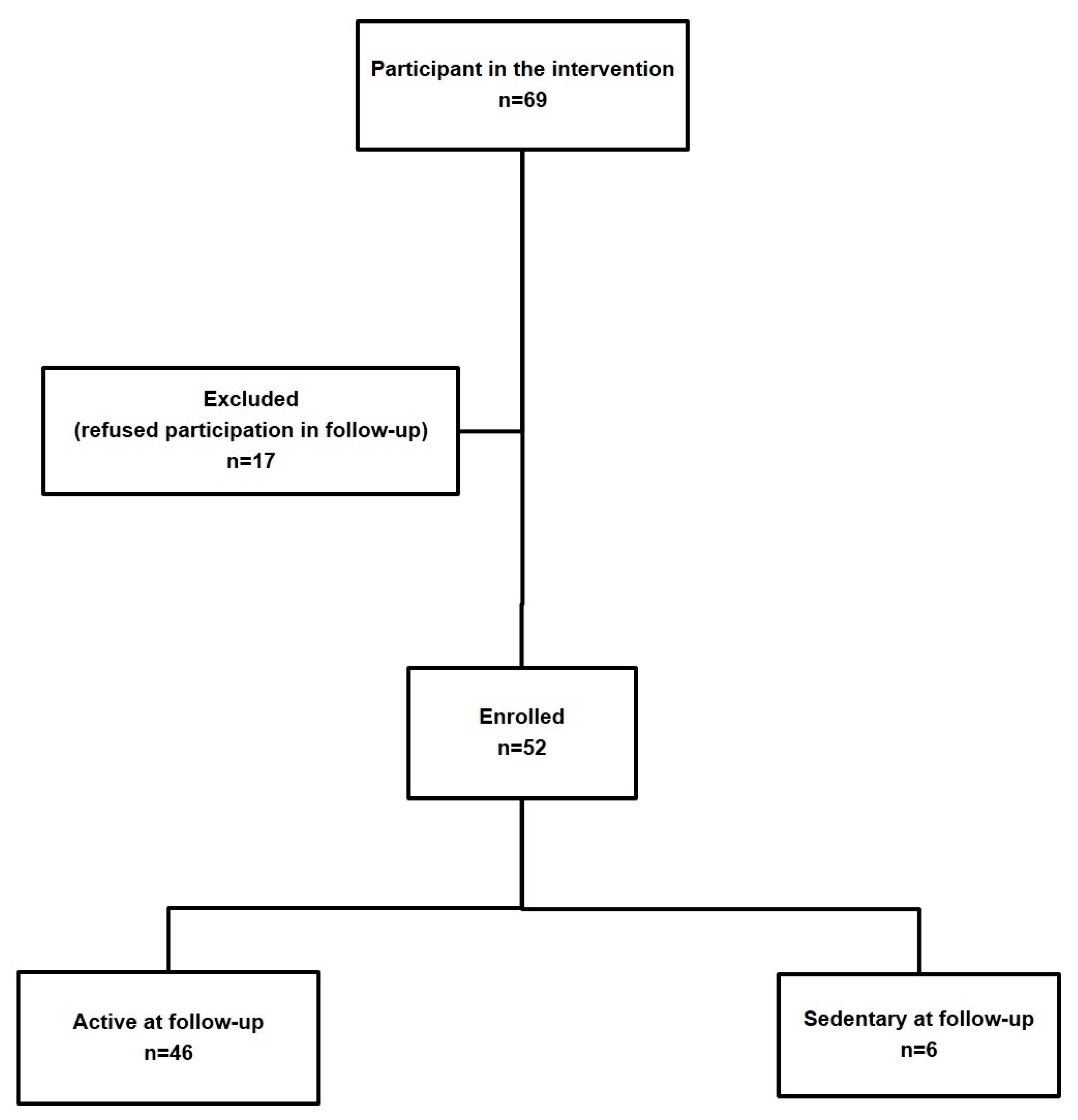
2.1. Participants and Setting
2.2. Intervention
2.3. Outcomes
2.3.1. Behavioral Outcomes
2.3.2. Anthropometric Outcomes
2.3.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Global Report on Diabetes; WHO Press: Geneva, Switzerland, 2016. [Google Scholar]
- Italian Institute of Statistics. Indagine Multiscopo “Aspetti Della Vita Quotidiana”. 2016. Available online: http://dati.istat.it/Index.aspx?DataSetCode=DCCV_INTRAT_MUSEI (accessed on 10 September 2018).
- Reusch, J.E.; Bridenstine, M.; Regensteiner, J.G. Type 2 diabetes mellitus and exercise impairment. Rev. Endocr. Metab. Disord. 2013, 14, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Villafaina, S.; Collado-Mateo, D.; Fuentes, J.P.; Merellano-Navarro, E.; Gusi, N. Physical Exercise Improves Heart Rate Variability in Patients with Type 2 Diabetes: A Systematic Review. Curr. Diabetes Rep. 2017, 17, 110. [Google Scholar] [CrossRef] [PubMed]
- Santos, D.A.; Silva, A.M.; Baptista, F.; Santos, R.; Gobbo, L.A.; Mota, J.; Sardinha, L.B. Are cardiorespiratory fitness and moderate-to-vigorous physical activity independently associated to overweight, obesity, and abdominal obesity in elderly? Am. J. Hum. Biol. 2012, 24, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.D. The impact of a supervised strength and aerobic training program on muscular strength and aerobic capacity in individuals with type 2 diabetes. J. Strength Cond. Res. 2007, 21, 824–830. [Google Scholar] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010, 33, e147–e167. [Google Scholar] [CrossRef] [PubMed]
- Morrato, E.H.; Hill, J.O.; Wyatt, H.R.; Ghushchyan, V.; Sullivan, P.W. Physical activity in U.S. adults with diabetes and at risk for developing diabetes, 2003. Diabetes Care 2007, 30, 203–209. [Google Scholar] [CrossRef] [PubMed]
- De Greef, K.; Deforche, B.; Tudor-Locke, C.; De Bourdeaudhuij, I. A cognitive-behavioural pedometer-based group intervention on physical activity and sedentary behaviour in individuals with type 2 diabetes. Health Educ. Res. 2010, 25, 724–736. [Google Scholar] [CrossRef] [PubMed]
- De Greef, K.; Deforche, B.; Tudor-Locke, C.; De Bourdeaudhuij, I. Increasing physical activity in Belgian type 2 diabetes patients: A three-arm randomized controlled trial. Int. J. Behav. Med. 2011, 18, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Lambers, S.; Van Laethem, C.; Van Acker, K.; Calders, P. Influence of combined exercise training on indices of obesity, diabetes and cardiovascular risk in type 2 diabetes patients. Clin. Rehabil. 2008, 22, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Grelier, S.; Serresse, O.; Boudreau-Lariviere, C.; Zory, R. Effects of a three-month combined training program on the cardiopulmonary and muscle strength capacities of type 2 diabetic subjects. J. Sports Med. Phys. Fitness 2013, 53, 56–64. [Google Scholar] [PubMed]
- Greaves, C.J.; Sheppard, K.E.; Abraham, C.; Hardeman, W.; Roden, M.; Evans, P.H.; Schwarz, P. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Pub. Health 2011, 11, 119. [Google Scholar] [CrossRef] [PubMed]
- Rossen, J.; Yngve, A.; Hagströmer, M.; Brismar, K.; Ainsworth, B.E.; Iskull, C.; Möller, P.; Johansson, U.-B. Physical activity promotion in the primary care setting in pre- and type 2 diabetes—The Sophia step study, an RCT. BMC Pub. Health 2015, 15, 647. [Google Scholar] [CrossRef] [PubMed]
- Gallé, F.; Di Onofrio, V.; Cirella, A.; Di Dio, M.; Miele, A.; Spinosa, T.; Liguori, G. Improving self-management of type 2 diabetes in overweight and inactive patients through an educational and motivational intervention addressing diet and physical activity: A prospective study in Naples, South Italy. Diabetes Ther. 2017, 8, 875–886. [Google Scholar] [CrossRef] [PubMed]
- Gallè, F.; Di Onofrio, V.; Miele, A.; Belfiore, P.; Liguori, G. Effects of a community-based exercise and motivational intervention on physical fitness of subjects with type 2 diabetes. Eur. J. Pub. Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Di Onofrio, V.; Gallé, F.; Di Dio, M.; Belfiore, P.; Liguori, G. Effects of nutrition motivational intervention in patients affected by type 2 diabetes mellitus: A longitudinal study in Naples, South Italy. BMC Public Health 2018, 18, 1181. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, N.Y.; Krakauer, J.C. A new body shape index predicts mortality hazard independently of body mass index. PLoS ONE 2012, 7, e39504. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, N.Y.; Krakauer, J.C. Dynamic association of mortality hazard with body shape. PLoS ONE 2014, 9, e88793. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, N.Y.; Krakauer, J.C. An Anthropometric Risk Index based on combining height, weight, waist, and hip measurements. J. Obes. 2016, 2016, 8094275. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry; Technical Report Series; WHO: Geneva, Switzerland, 1995; p. 854. [Google Scholar]
- Petursson, H.; Sigurdsson, J.A.; Bengtsson, C.; Nilsen, T.I.L.; Getz, L. Body configuration as a predictor of mortality: Comparison of five anthropometric measures in a 12 year follow up of the Norwegian HUNT 2 study. PLoS ONE 2011, 6, e26621. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Jousilahti, P.; Stehouwer, C.D.; Söderberg, S.; Onat, A.; Laatikainen, T.; Yudkin, J.S.; Dankner, R.; Morris, R.; Tuomilehto, J.; et al. Cardiovascular and all-cause mortality in relation to various anthropometric measures of obesity in Europeans. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Dhana, K.; Ikram, M.A.; Hofman, A.; Franco, O.H.; Kavousi, M. Anthropometric measures in cardiovascular disease prediction: Comparison of laboratory-based versus non-laboratory-based model. Heart 2015, 101, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Sözmen, K.; Ünal, B.; Sakarya, S.; Dinç, G.; Yardim, N.; Keskinkılıç, B.; Ergör, G. Association of anthropometric measurement methods with cardiovascular disease risk in Turkey. Dicle Med. J. 2016, 43, 99–106. [Google Scholar] [CrossRef]
- Savva, S.C.; Lamnisos, D.; Kafatos, A.G. Predicting cardiometabolic risk: Waist-to-height ratio or BMI. A meta-analysis. Diabetes Metab. Syndr. Obes. Targets Ther. 2013, 6, 403–419. [Google Scholar] [CrossRef] [PubMed]
- Abete, I.; Arriola, L.; Etxezarreta, N.; Mozo, I.; Moreno-Iribas, C.; Amiano, P.; Egüés, N.; Goyenechea, E.; de Munain, A.L.; Martinez, M.; et al. Association between different obesity measures and the risk of stroke in the EPIC Spanish cohort. Eur. J. Nutr. 2015, 54, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Bozorgmanesh, M.; Sardarinia, M.; Hajsheikholeslami, F.; Azizi, F.; Hadaegh, F. CVD-predictive performances of ‘a body shape index’ versus simple anthropometric measures: Tehran Lipid and Glucose Study. Eur. J. Nutr. 2016, 55, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Bertoli, S.; Leone, A.; Krakauer, N.Y.; Bedogni, G.; Vanzulli, A.; Redaelli, V.I.; De Amicis, I.; Vignati, L.; Krakauer, J.C.; Battezzati, A. Association of Body Shape Index (ABSI) with cardio-metabolic risk factors: A cross-sectional study of 6081 Caucasian adults. PLoS ONE 2017, 12, e0185013. [Google Scholar] [CrossRef] [PubMed]
- Consalvo, V.; Krakauer, J.C.; Krakauer, N.Y.; Canero, A.; Romano, M.; Salsano, V. ABSI (A Body Shape Index) and ARI (Anthropometric Risk Indicator) in bariatric surgery. First application on a bariatric cohort and possible clinical use. Obes. Surg. 2018, 28, 1966–1973. [Google Scholar] [CrossRef] [PubMed]
- Mameli, C.; Krakauer, J.C.; Krakauer, N.Y.; Bosetti, A.; Ferrari, C.M.; Schneider, L.; Borsani, B.; Arrigoni, S.; Pendezza, E.; Zuccotti, G.V. Effects of a multidisciplinary weight loss intervention in overweight and obese children and adolescents: 11 years of experience. PLoS ONE 2017, 12, e0181095. [Google Scholar] [CrossRef] [PubMed]
- Mameli, C.; Krakauer, N.Y.; Krakauer, J.C.; Bosetti, A.; Ferrari, C.M.; Moiana, N.; Schneider, L.; Borsani, B.; Genoni, T.; Zuccotti, G. The association between a body shape index and cardiovascular risk in overweight and obese children and adolescents. PLoS ONE 2018, 13, e0190426. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, J.C.; Krakauer, N.Y. Combining Body Mass and Shape Indices in Clinical Practice. Case Rep. Med. 2016, 2016, 1526175. [Google Scholar] [CrossRef] [PubMed]
- Krakauer, N.Y.; Krakauer, J.C. Untangling Waist Circumference and Hip Circumference from Body Mass Index with A Body Shape Index, Hip Index, and Anthropometric Risk Indicator. Metab. Syndr. Relat. Disord. 2018, 16, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Ji, M.; Zhang, S.; An, R. Effectiveness of A Body Shape Index (ABSI) in predicting chronic diseases and mortality: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 737–759. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Outcome | T0 | T1 | T2 | T0–T1 p | T1–T2 p | T0–T2 p | ANOVA p |
|---|---|---|---|---|---|---|---|
| Habitual PA MET-min/week | 474.8 ± 90.3 | 641 ± 53.5 | 663.4 ± 57.0 | <0.01 | 1 | <0.01 | <0.01 |
| minutes/week spent in PA | 122 ± 35.2 | 153 ± 10.7 | 168 ± 25.3 | <0.01 | <0.01 | <0.01 | <0.01 |
| vigorous PA | 10 ± 5.5 | 20 ± 5.2 | 15 ± 5.6 | <0.01 | 0.06 | <0.01 | <0.01 |
| moderate PA | 36 ± 6.3 | 60 ± 4.5 | 55 ± 10.5 | <0.01 | 0.13 | <0.01 | <0.01 |
| Weight Kg | 83.7 ± 8.8 | 79.1 ± 8.5 | 76.4 ± 9.2 | 0.03 | 0.38 | <0.01 | <0.01 |
| Waist circumference cm | 99.5 ± 6.3 | 93.9 ± 7.9 | 91.3 ± 9.2 | <0.01 | 0.32 | <0.01 | <0.01 |
| Hip circumference cm | 97.8 ± 6.8 | 96.5 ± 7.2 | 95.5 ± 8.5 | 1 | 1 | 0.41 | 0.32 |
| BMI Kg/m2 | 30.0 ± 2.6 | 28.3 ± 2.4 | 27.4 ± 2.7 | <0.01 | 0.17 | <0.01 | <0.01 |
| BMI z-score | 0.50 ± 0.51 | 0.17 ± 0.46 | −0.01 ± 0.51 | <0.01 | 0.16 | <0.01 | <0.01 |
| ABSI (m11/6 Kg−2/3) | 0.08 ± 0.004 | 0.07 ± 0.005 | 0.07 ± 0.005 | 0.29 | 1 | 0.14 | 0.10 |
| ABSI z-score | −0.83 ± 0.99 | −1.2 ± 1.2 | −1.3 ± 1.4 | 0.27 | 0.24 | 0.14 | 1 |
| HI cm | 91.8 ± 5.1 | 93.1 ± 5.7 | 93.7 ± 6.6 | 0.73 | 1 | 0.27 | 0.21 |
| HI z-score | −1.8 ± 1.3 | −1.4 ± 1.5 | −1.3 ± 1.7 | 0.68 | 1 | 0.23 | 0.19 |
| Outcome | Mean Hazard Ratios | T0–T1 p | T1–T2 p | T0–T2 p | ANOVA | ||
|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | p | ||||
| BMI risk | 1.00 ± 0.09 | 0.94 ± 0.08 | 0.92 ± 0.08 | <0.01 | 0.43 | <0.01 | <0.01 |
| ABSI risk | 0.90 ± 0.09 | 0.88 ± 0.07 | 0.87 ± 0.09 | 0.89 | 1 | 1 | 0.58 |
| HI risk | 1.16 ± 0.16 | 1.12 ± 0.16 | 1.11 ± 0.16 | 0.66 | 1 | 0.39 | 0.27 |
| ARI risk | 1.04 ± 0.14 | 0.93 ± 0.13 | 0.91 ± 0.13 | <0.01 | 1 | <0.01 | <0.01 |
| T1–T2 Changes | Δ BMI z-Score p | Δ ABSI z-Score p | Δ HI z-Score p | Δ PA p |
|---|---|---|---|---|
| Δ BMI z-score p | 1 | −0.20 0.15 | −0.07 0.61 | −0.29 0.04 |
| Δ ABSI z-score p | −0.20 0.15 | 1 | −0.74 <0.01 | 0.15 0.27 |
| Δ HI z-score p | −0.07 0.61 | −0.74 <0.01 | 1 | 0.08 0.56 |
| Δ PA p | −0.29 0.04 | −0.15 0.27 | 0.08 0.56 | 1 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallè, F.; Krakauer, J.C.; Krakauer, N.Y.; Valerio, G.; Liguori, G. Can an Exercise-Based Educational and Motivational Intervention be Durably Effective in Changing Compliance to Physical Activity and Anthropometric Risk in People with Type 2 Diabetes? A Follow-Up Study. Int. J. Environ. Res. Public Health 2019, 16, 701. https://doi.org/10.3390/ijerph16050701
Gallè F, Krakauer JC, Krakauer NY, Valerio G, Liguori G. Can an Exercise-Based Educational and Motivational Intervention be Durably Effective in Changing Compliance to Physical Activity and Anthropometric Risk in People with Type 2 Diabetes? A Follow-Up Study. International Journal of Environmental Research and Public Health. 2019; 16(5):701. https://doi.org/10.3390/ijerph16050701
Chicago/Turabian StyleGallè, Francesca, Jesse C. Krakauer, Nir Y. Krakauer, Giuliana Valerio, and Giorgio Liguori. 2019. "Can an Exercise-Based Educational and Motivational Intervention be Durably Effective in Changing Compliance to Physical Activity and Anthropometric Risk in People with Type 2 Diabetes? A Follow-Up Study" International Journal of Environmental Research and Public Health 16, no. 5: 701. https://doi.org/10.3390/ijerph16050701
APA StyleGallè, F., Krakauer, J. C., Krakauer, N. Y., Valerio, G., & Liguori, G. (2019). Can an Exercise-Based Educational and Motivational Intervention be Durably Effective in Changing Compliance to Physical Activity and Anthropometric Risk in People with Type 2 Diabetes? A Follow-Up Study. International Journal of Environmental Research and Public Health, 16(5), 701. https://doi.org/10.3390/ijerph16050701