Early Discharge for Anterior Cervical Fusion Surgery: Prediction of Readmission and Special Considerations for Older Adults



Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Source and Ethical Concerns
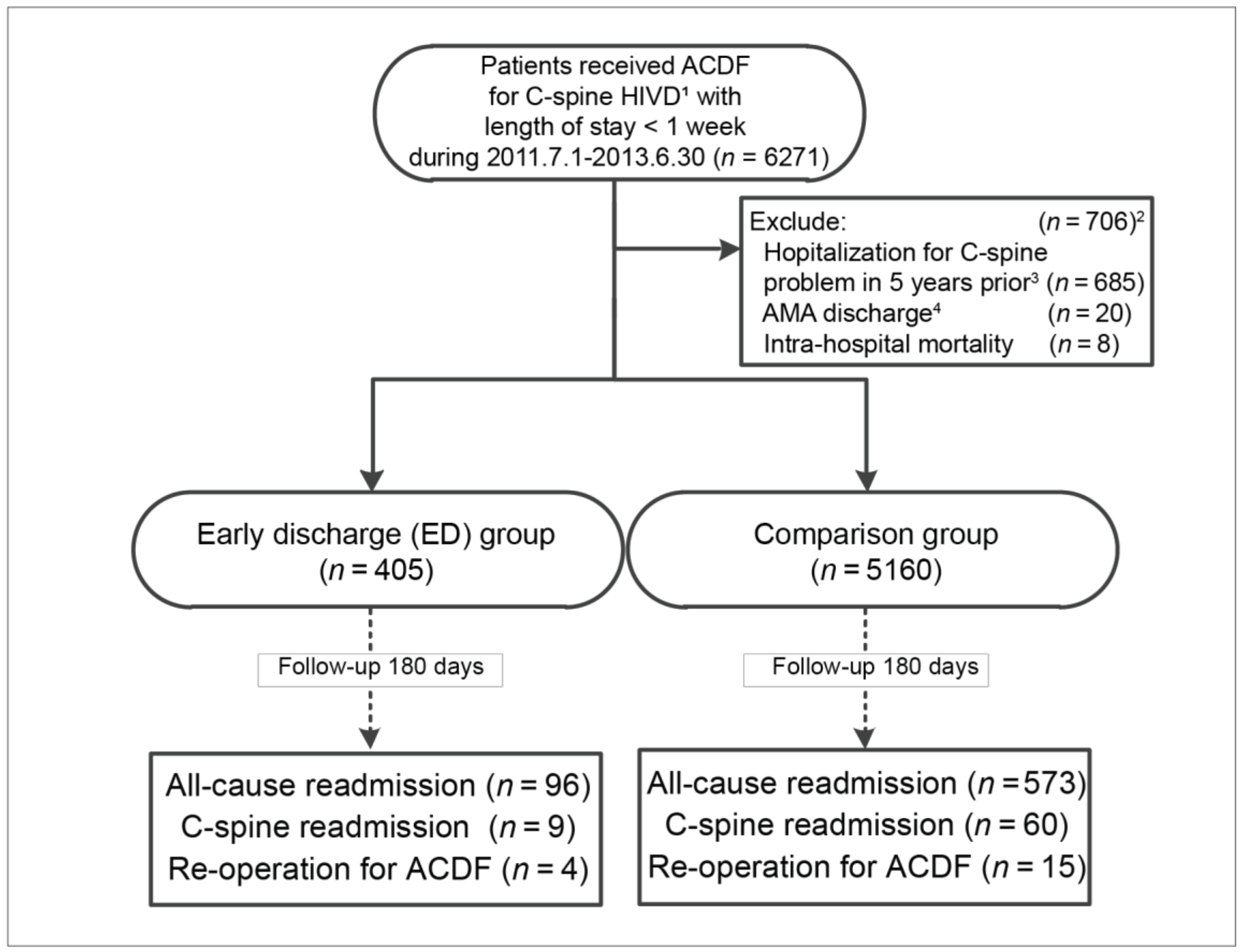
2.2. Identification of Study Cohort, and Hospitalization for ACDF
2.3. ED Group vs. Comparison Group
2.4. Follow-Up Outcomes and Risk Factors
2.5. Outcome Analysis and Sub-Group Analysis for Older Adults
2.6. Statistical Analysis
3. Results
3.1. Preoperative Demographics
3.2. Rates of Re-Admission and Re-Operation
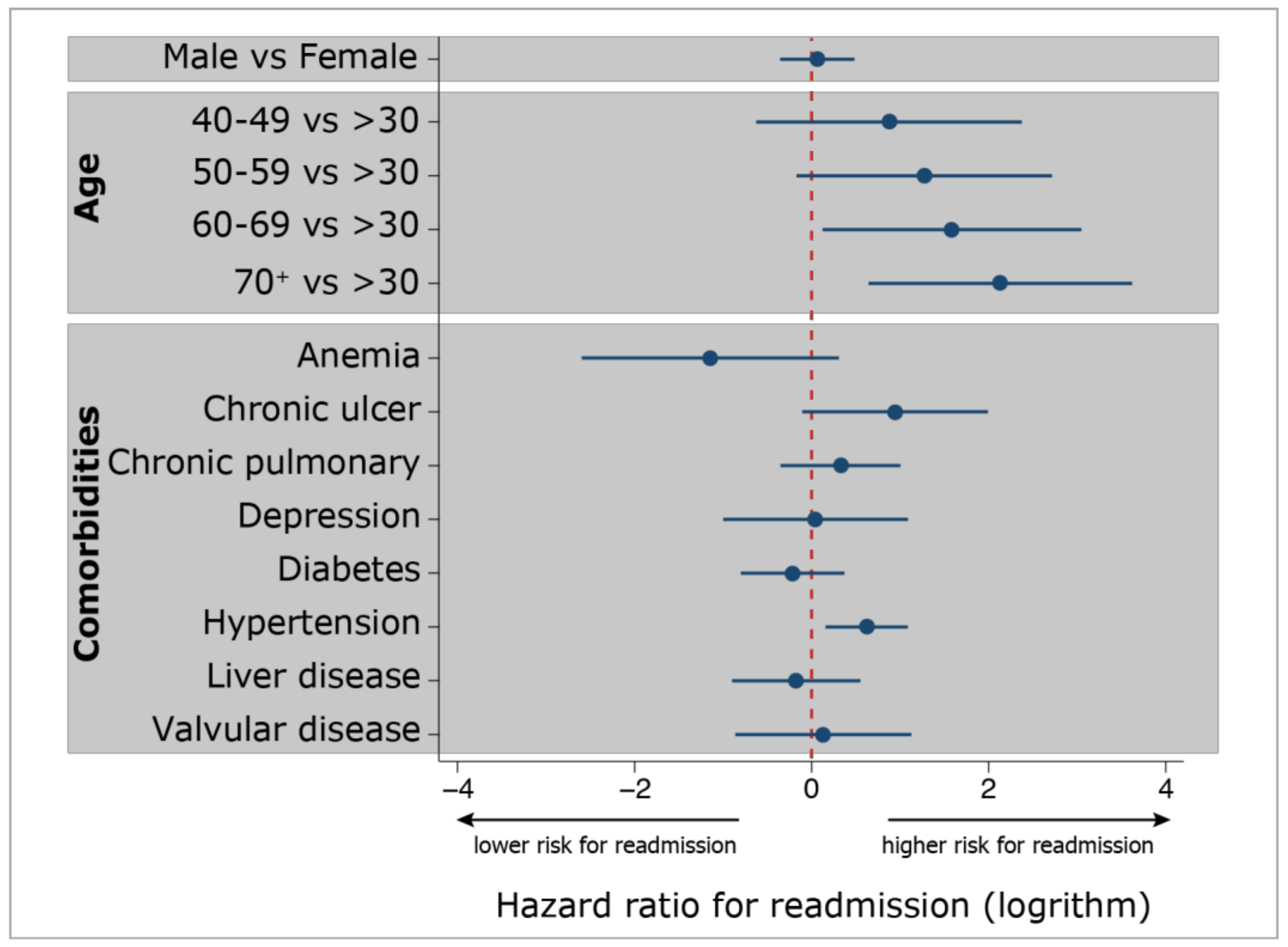
3.3. Risk Analysis
3.4. Outcome Analysis
3.5. Subgroup Analysis for Older Adults
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcomes | Model 1, ED ≤ 48 Hours | Model 2, ED ≤ 72 Hours | ||||
|---|---|---|---|---|---|---|
| aHR 1 | (95% CI) | p-Value | aHR 1 | (95% CI) | p-Value | |
| Any re-admission | 2.39 | (1.92–2.97) | <0.001 | 1.31 | (1.11–1.54) | <0.001 |
| Re-admission for C-spine problem | 1.72 | (SE = 2.13) 2 | 0.660 | 1.51 | (SE = 0.40) 2 | 0.118 |
| Re-admission for second ACDF | 3.27 | (SE = 18.80) 2 | 0.852 | 1.98 | (SE = 1.00) 2 | 0.178 |
References
- Chang, P.Y.; Chang, H.K.; Wu, J.C.; Huang, W.C.; Fay, L.Y.; Tu, T.H.; Wu, C.L.; Cheng, H. Is cervical disc arthroplasty good for congenital cervical stenosis? J. Neurosurg. Spine 2017, 26, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Fay, L.Y.; Huang, W.C.; Tsai, T.Y.; Wu, J.C.; Ko, C.C.; Tu, T.H.; Wu, C.L.; Cheng, H. Differences between arthroplasty and anterior cervical fusion in two-level cervical degenerative disc disease. Eur. Spine J. 2014, 23, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Mummaneni, P.V.; Amin, B.Y.; Wu, J.C.; Brodt, E.D.; Dettori, J.R.; Sasso, R.C. Cervical artificial disc replacement versus fusion in the cervical spine: A systematic review comparing long-term follow-up results from two FDA trials. Evid. Based Spine Care J. 2012, 3, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.C.; Huang, W.C.; Tsai, H.W.; Ko, C.C.; Fay, L.Y.; Tu, T.H.; Wu, C.L.; Cheng, H. Differences between 1- and 2-level cervical arthroplasty: More heterotopic ossification in 2-level disc replacement: Clinical article. J. Neurosurg. Spine 2012, 16, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.C.; Huang, W.C.; Tu, T.H.; Tsai, H.W.; Ko, C.C.; Wu, C.L.; Cheng, H. Differences between soft-disc herniation and spondylosis in cervical arthroplasty: CT-documented heterotopic ossification with minimum 2 years of follow-up. J. Neurosurg. Spine 2012, 16, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Khoueir, P.; Oh, B.C.; DiRisio, D.J.; Wang, M.Y. Multilevel anterior cervical fusion using a collagen-hydroxyapatite matrix with iliac crest bone marrow aspirate: An 18-month follow-up study. Neurosurgery 2007, 61, 963–970. [Google Scholar] [CrossRef]
- Wang, M.Y.; Levi, A.D.; Shah, S.; Green, B.A. Polylactic acid mesh reconstruction of the anterior iliac crest after bone harvesting reduces early postoperative pain after anterior cervical fusion surgery. Neurosurgery 2002, 51, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.Y.; Liu, C.Y. Resorbable polylactic acid interbody spacers with vertebral autograft for anterior cervical discectomy and fusion. Neurosurgery 2005, 57, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Boakye, M.; Mummaneni, P.V.; Garrett, M.; Rodts, G.; Haid, R. Anterior cervical discectomy and fusion involving a polyetheretherketone spacer and bone morphogenetic protein. J. Neurosurg. Spine 2005, 2, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Lau, D.; Chou, D.; Mummaneni, P.V. Two-level corpectomy versus three-level discectomy for cervical spondylotic myelopathy: A comparison of perioperative, radiographic, and clinical outcomes. J. Neurosurg. Spine 2015, 23, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Tumialan, L.M.; Pan, J.; Rodts, G.E.; Mummaneni, P.V. The safety and efficacy of anterior cervical discectomy and fusion with polyetheretherketone spacer and recombinant human bone morphogenetic protein-2: A review of 200 patients. J. Neurosurg. Spine 2008, 8, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Fearon, K.C.; Ljungqvist, O.; Von Meyenfeldt, M.; Revhaug, A.; Dejong, C.H.; Lassen, K.; Nygren, J.; Hausel, J.; Soop, M.; Andersen, J.; et al. Enhanced recovery after surgery: A consensus review of clinical care for patients undergoing colonic resection. Clin. Nutr. 2005, 24, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Lassen, K.; Soop, M.; Nygren, J.; Cox, P.B.; Hendry, P.O.; Spies, C.; von Meyenfeldt, M.F.; Fearon, K.C.; Revhaug, A.; Norderval, S.; et al. Consensus review of optimal perioperative care in colorectal surgery: Enhanced Recovery After Surgery (ERAS) Group recommendations. Arch. Surg. 2009, 144, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Varadhan, K.K.; Neal, K.R.; Dejong, C.H.; Fearon, K.C.; Ljungqvist, O.; Lobo, D.N. The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: A meta-analysis of randomized controlled trials. Clin. Nutr. 2010, 29, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Adamson, T.; Godil, S.S.; Mehrlich, M.; Mendenhall, S.; Asher, A.L.; McGirt, M.J. Anterior cervical discectomy and fusion in the outpatient ambulatory surgery setting compared with the inpatient hospital setting: Analysis of 1000 consecutive cases. J. Neurosurg. Spine 2016, 24, 878–884. [Google Scholar] [CrossRef] [PubMed]
- McClelland, S.; Passias, P.G.; Errico, T.J.; Bess, R.S.; Protopsaltis, T.S. Outpatient Anterior Cervical Discectomy and Fusion: An Analysis of Readmissions from the New Jersey State Ambulatory Services Database. Int. J. Spine Surg. 2017, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Garringer, S.M.; Sasso, R.C. Safety of anterior cervical discectomy and fusion performed as outpatient surgery. J. Spinal Disord. Tech. 2010, 23, 439–443. [Google Scholar] [CrossRef]
- Villavicencio, A.T.; Pushchak, E.; Burneikiene, S.; Thramann, J.J. The safety of instrumented outpatient anterior cervical discectomy and fusion. Spine J. 2007, 7, 148–153. [Google Scholar] [CrossRef]
- Wu, J.C.; Liu, L.; Wen-Cheng, H.; Chen, Y.C.; Ko, C.C.; Wu, C.L.; Chen, T.J.; Cheng, H.; Su, T.P. The incidence of adjacent segment disease requiring surgery after anterior cervical diskectomy and fusion: Estimation using an 11-year comprehensive nationwide database in Taiwan. Neurosurgery 2012, 70, 594–601. [Google Scholar] [CrossRef]
- Moore, B.J.; White, S.; Washington, R.; Coenen, N.; Elixhauser, A. Identifying Increased Risk of Readmission and In-hospital Mortality Using Hospital Administrative Data: The AHRQ Elixhauser Comorbidity Index. Med. Care 2017, 55, 698–705. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Aasvang, E.K.; Luna, I.E.; Kehlet, H. Challenges in postdischarge function and recovery: The case of fast-track hip and knee arthroplasty. Br. J. Anaesth. 2015, 115, 861–866. [Google Scholar] [CrossRef]
- Venkata, H.K.; van Dellen, J.R. A perspective on the use of an enhanced recovery program in open, non-instrumented day surgery for degenerative lumbar and cervical spinal conditions. J. Neurosurg. Sci. 2018, 62, 245–254. [Google Scholar] [CrossRef]
- Fu, M.C.; Gruskay, J.A.; Samuel, A.M.; Sheha, E.D.; Derman, P.B.; Iyer, S.; Grauer, J.N.; Albert, T.J. Outpatient Anterior Cervical Discectomy and Fusion is Associated With Fewer Short-term Complications in One- and Two-level Cases: A Propensity-adjusted Analysis. Spine 2017, 42, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- McGirt, M.J.; Godil, S.S.; Asher, A.L.; Parker, S.L.; Devin, C.J. Quality analysis of anterior cervical discectomy and fusion in the outpatient versus inpatient setting: Analysis of 7288 patients from the NSQIP database. Neurosurg. Focus 2015, 39, E9. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.T.; Pugely, A.J.; Gao, Y.; Mendoza-Lattes, S. Thirty-Day Morbidity After Single-Level Anterior Cervical Discectomy and Fusion: Identification of Risk Factors and Emphasis on the Safety of Outpatient Procedures. J. Bone Joint Surg. 2014, 96, 1288–1294. [Google Scholar] [CrossRef] [PubMed]
- Sivaganesan, A.; Hirsch, B.; Phillips, F.M.; McGirt, M.J. Spine Surgery in the Ambulatory Surgery Center Setting: Value-Based Advancement or Safety Liability? Neurosurgery 2018, 83, 159–165. [Google Scholar] [CrossRef]
| Characteristics and Outcomes | Comparison Group | ED Group | p-Value | ||
|---|---|---|---|---|---|
| n = 5160 | (%) | n = 405 | (%) | ||
| Gender | 0.443 | ||||
| Female Male | 2459 | (47.7) | 185 | (45.7) | |
| 2701 | (52.3) | 220 | (54.3) | ||
| Age, mean (SD) | 55.1 | (11.37) | 54.5 | (11.29) | 0.327 |
| Co-morbidities | |||||
| Anemia | 217 | (4.2) | 14 | (3.5) | 0.467 |
| Chronic peptic ulcer disease | 186 | (3.6) | 10 | (2.5) | 0.233 |
| Chronic pulmonary disease | 602 | (11.7) | 46 | (11.4) | 0.852 |
| Depression | 268 | (5.2) | 16 | (4.0) | 0.274 |
| Diabetes | 996 | (19.3) | 74 | (18.3) | 0.612 |
| Hypertension | 1749 | (33.9) | 130 | (32.1) | 0.462 |
| Liver disease | 530 | (10.3) | 38 | (9.4) | 0.569 |
| Valvular disease | 20 | (4.0) | 13 | (3.2) | 0.436 |
| Outcomes | |||||
| All-cause re-admission | |||||
| 30-day re-admission | 113 | (2.2) | 20 | (4.9) | <0.001 |
| 60-day re-admission | 214 | (4.1) | 49 | (12.1) | <0.001 |
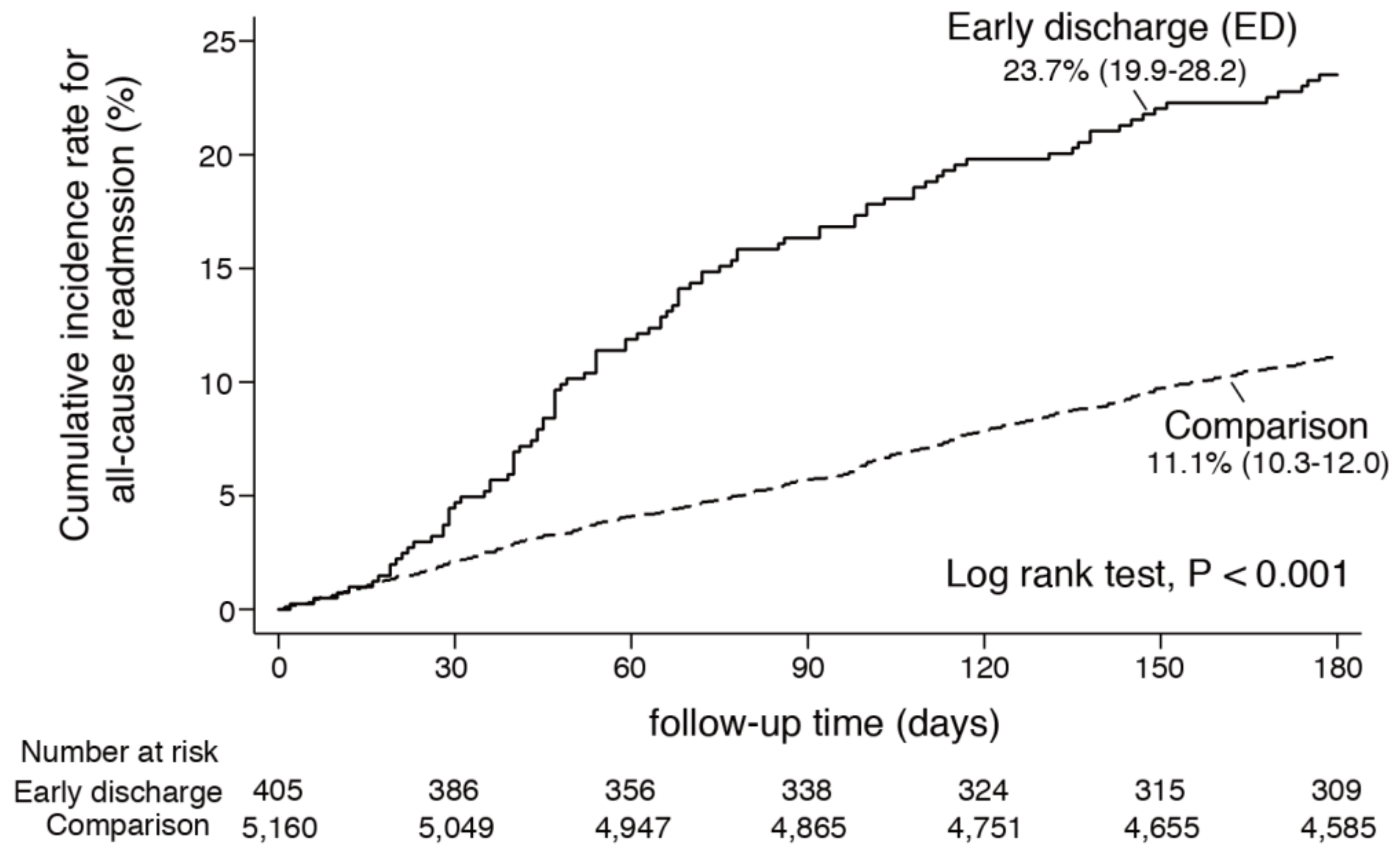
| 180-day re-admission | 573 | (11.1) | 96 | (23.7) | <0.001 |
| Cervical spine-related re-admission | |||||
| 30-day re-admission | 12 | (0.2) | 6 | (1.5) | <0.001 |
| 60-day re-admission | 25 | (0.5) | 6 | (1.5) | 0.009 |
| 180-day re-admission | 60 | (1.2) | 9 | (2.2) | <0.001 |
| Re-operations | |||||
| 30-day re-operation | 2 | (0.0) | 3 | (0.7) | <0.001 |
| 60-day re-operation | 6 | (0.1) | 3 | (0.7) | 0.003 |
| 180-day re-operation | 15 | (0.3) | 4 | (1.0) | 0.021 |
| Re-Admission during 180-Day Follow-Up | Comparison Group | ED Group |
|---|---|---|
| All-cause re-admissions Incidence of all-cause re-admissions | ||
| (per 1000 person-years) | 235.1 | 548.5 |
| Number of occurrences | 572 | 95 |
| Observed person-years | 2428.4 | 173.2 |
| Crude hazard ratio (95% CI) | 1.00 | 2.33 (1.86–2.90) ***2 |
| Adjusted hazard ratio (95% CI) 1 | 1.00 | 2.39 (1.92–2.97) ***2 |
| Cervical spine-related re-admissions Incidence of cervical-spine-related re-admissions (per 1000 person-years) | 23.0 | 40.2 |
| Number of occurrences | 59 | 8 |
| Observed person-years | 2561.4 | 198.8 |
| Crude hazard ratio (95% CI) | 1.00 | 1.75 (0.72–3.67) |
| Adjusted hazard ratio (SE, p-value) 3 | 1.00 | 1.72 (SE = 2.13, p-value = 0.660) |
| Re-operations Incidence of re-operations | ||
| (per 1000 person-years) | 5.8 | 19.9 |
| Number of occurrences | 15 | 4 |
| Observed person-years | 2573.9 | 200.8 |
| Crude hazard ratio (95% CI) | 1.00 | 3.42 (0.83-10.73) |
| The adjusted hazard ratio (SE, p-value) 3 | 1.00 | 3.27 (SE = 18.80, p-value = 0.852) |
| Reasons for Re-Admission | Comparison Group n = 5160 | ED Group n = 405 | Incidence Rate Ratio (IRR) 2 | |||||
|---|---|---|---|---|---|---|---|---|
| n | IR 1 | n | IR 1 | IRR | (95% CI) | p-value | Sig. 3 | |
| Musculoskeletal system & connective tissue | 204 | 79.1 | 50 | 246.9 | 3.12 | (2.24–4.27) | <0.001 | *** |
| Injuries | 74 | 28.7 | 14 | 69.1 | 2.41 | (1.26–4.30) | 0.006 | ** |
| Diseases of the circulatory system | 55 | 21.3 | 5 | 24.7 | 1.16 | 0.36–2.87) | 0.715 | |
| Diseases of the respiratory system | 38 | 14.7 | 1 | 4.9 | 0.34 | (0.01–1.98) | 0.266 | |
| Neoplasms | 38 | 14.7 | 3 | 14.8 | 1.01 | (0.20–3.17) | 0.931 | |
| Diseases of the nervous system | 36 | 14.0 | −6.98 | (−9.26–4.70) 4 | 0.033 | * | ||
| Diseases of the digestive system | 33 | 12.8 | 6 | 29.6 | 2.32 | (0.79–5.60) | 0.082 | |
| Diseases of the genitourinary system | 31 | 12.0 | 4 | 19.8 | 1.64 | (0.42–4.65) | 0.356 | |
| Endocrine, metabolic, and immunity disorders | 15 | 5.8 | 2 | 9.9 | 1.70 | (0.19–7.30) | 0.476 | |
| Congenital anomalies | 13 | 5.0 | 10 | 49.4 | 9.80 | (3.85–24.19) | <0.001 | *** |
| Others | 36 | 14.0 | 1 | 4.9 | 0.35 | (0.01–2.10) | 0.300 | |
| Outcomes in Older Adults (n = 1827) | n | Median Time to Re-Admission (days) | Incidence Rate (IR) (per 1000 Person-Years) | p-Value | ||
|---|---|---|---|---|---|---|
| Days | (95% CI) | IR | (95% CI) | |||
| Any re-admission | ||||||
| Overall | 318 | 80.0 | (9.0–95.0) | 376.30 | (343.60–410.00) | |
| ED group | 50 | 54.0 | (19.0–151.0) | 724.64 | (603.85–825.37) | <0.001 |
| Comparison group | 268 | 87.5 | (7.0–168.0) | 317.16 | (285.87–349.73) | |
| Re-admission for C-spine problem | ||||||
| Overall | 30 | 38.5 | (1.0–148.0) | 32.82 | (22.25–46.53) | |
| ED group | 5 | 26.0 | (6.0–70.0) | 72.46 | (23.95–16.11) | 0.082 |
| Comparison group | 25 | 40.0 | (1.0–148.0) | 29.59 | (19.24–43.37) | |
| Re-admission for second ACDF | ||||||
| Overall | 6 | 46.5 | (6.0–155.0) | 6.56 | (3.53–14.23) | |
| ED group | 2 | 16.0 | (6.0–26.0) | 28.99 | (3.53–100.82) | 0.049 |
| Comparison group | 4 | 54.5 | (40.0–155.0) | 4.73 | (1.29–12.08) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-C.; Wu, J.-C.; Chang, H.-K.; Huang, W.-C. Early Discharge for Anterior Cervical Fusion Surgery: Prediction of Readmission and Special Considerations for Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 641. https://doi.org/10.3390/ijerph16040641
Chen Y-C, Wu J-C, Chang H-K, Huang W-C. Early Discharge for Anterior Cervical Fusion Surgery: Prediction of Readmission and Special Considerations for Older Adults. International Journal of Environmental Research and Public Health. 2019; 16(4):641. https://doi.org/10.3390/ijerph16040641
Chicago/Turabian StyleChen, Yu-Chun, Jau-Ching Wu, Hsuan-Kan Chang, and Wen-Cheng Huang. 2019. "Early Discharge for Anterior Cervical Fusion Surgery: Prediction of Readmission and Special Considerations for Older Adults" International Journal of Environmental Research and Public Health 16, no. 4: 641. https://doi.org/10.3390/ijerph16040641
APA StyleChen, Y.-C., Wu, J.-C., Chang, H.-K., & Huang, W.-C. (2019). Early Discharge for Anterior Cervical Fusion Surgery: Prediction of Readmission and Special Considerations for Older Adults. International Journal of Environmental Research and Public Health, 16(4), 641. https://doi.org/10.3390/ijerph16040641