Does Eating-Away-from-Home Increase the Risk of a Metabolic Syndrome Diagnosis?


Abstract
1. Introduction
2. Materials and Methods
2.1. Population and Data Collection
2.2. Dietary Assessment and EAFH
2.3. Biomarker Variables and MetS
2.4. Measurement of Other Covariates
2.5. Statistical Analysis
3. Results
3.1. Summary of Population Characteristics
3.2. Nutrients Intake and MetS
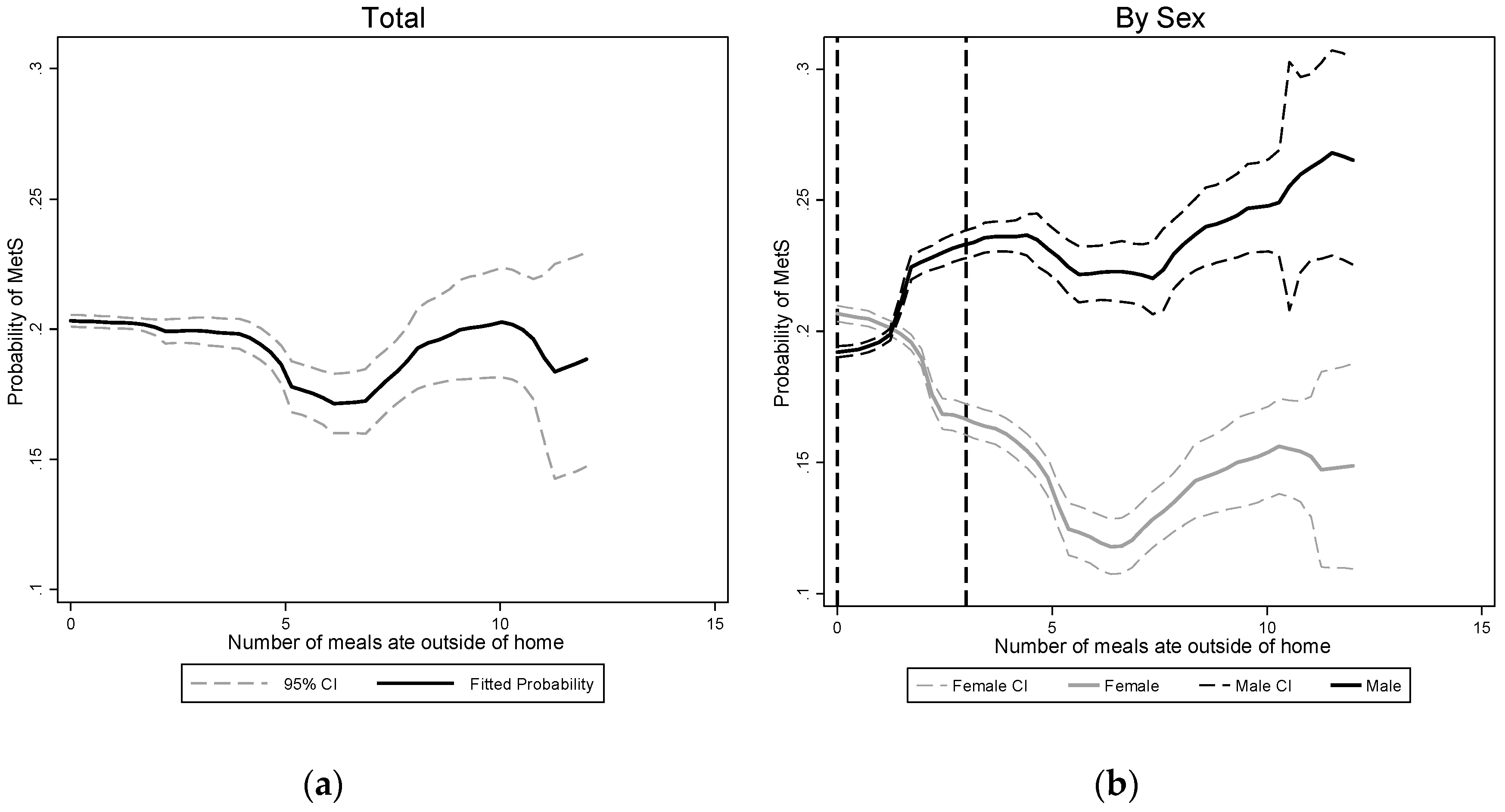
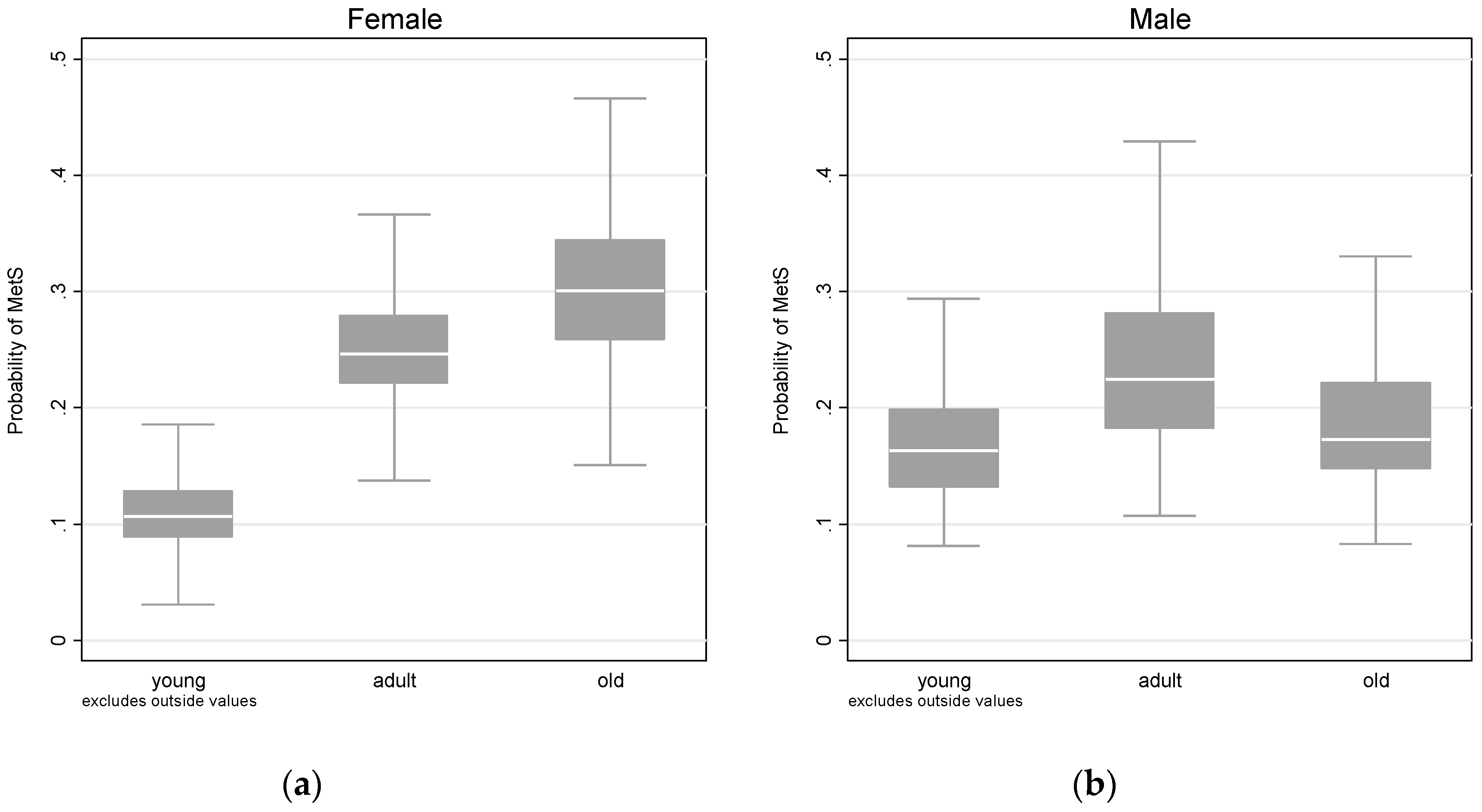
3.3. Association between EAFH and MetS and its Components
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zeng, Q.; Zeng, Y. Eating out and getting fat? A comparative study between urban and rural China. Appetite 2018, 120, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Gao, Y.; Zhao, Y. Impact of income growth on food consumption pattern in urban China. China Econ. Q. 2015, 15, 263–288. (In Chinese) [Google Scholar]
- Xu, X. An analysis of food consumption in rural area of China 2000–2010 (in Chinese). World Surv. Res. 2011, 12, 23–26. [Google Scholar]
- Tian, X.; Zhong, L.; von Cramon-Taubadel, S.; Tu, H.; Wang, H. Restaurants in the Neighborhood, Eating Away from Home and BMI in China. PLoS ONE 2016, 11, e0167721. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Yu, X.H. Using semiparametric models to study nutrition improvement and dietary change with different indices: The case of China. Food Policy 2015, 53, 67–81. [Google Scholar] [CrossRef]
- Popkin, B.M. Dynamics of the nutrition transition and its implications for the developing world. Forum Nutr. 2003, 56, 262–264. [Google Scholar] [PubMed]
- Drewnowski, A.; Popkin, B.M. The nutrition transition: New trends in the global diet. Nutr. Rev. 1997, 55, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Ma, X.; Zhu, S. Metabolic syndrome in the prevention of cardiovascular diseases and diabetes–still a matter of debate? Eur. J. Clin. Nutr. 2013, 67, 518–521. [Google Scholar] [CrossRef]
- Pusztová, L.; Babič, F.; Paralič, J. Data Analytics for Metabolic Syndrome Diagnostics. In World Congress on Medical Physics and Biomedical Engineering 2018; Lhotska, L., Sukupova, L., Lacković, I., Ibbott, G.S., Eds.; Springer: Singapore, 2018; pp. 311–314. [Google Scholar]
- GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef]
- International Diabetes Federation. IDF Diabetes Atlas; International Diabetes Federation: Brussels, Belgium, 2013. [Google Scholar]
- Weiwei, C.; Runlin, G.; Lisheng, L.; Manlu, Z.; Wen, W.; Yongjun, W.; Zhaosu, W.; Huijun, L.; Zhe, Z.; Lixin, J.; et al. Outline of the report on cardiovascular diseases in China, 2014. Eur. Heart J. Suppl. J. Eur. Soc. Cardiol. 2016, 18, F2–F11. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, L.; He, J.; Bi, Y.; Li, M.; Wang, T.; Jiang, Y.; Dai, M.; Lu, J.; Xu, M.; et al. Prevalence and control of diabetes in Chinese adults. JAMA 2013, 310, 948–959. [Google Scholar] [CrossRef] [PubMed]
- Waxman, A. WHO global strategy on diet, physical activity and health. Food Nutr. Bull. 2004, 25, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Wu, M.; Zang, J.; Zhu, Y.; Wang, H. Dietary diversity and adiposity in Chinese men and women: An analysis of four waves of cross-sectional survey data. Eur. J. Clin. Nutr. 2017, 71, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Liu, J.; Chen, B.; Jin, D.; Fu, Z.; Liu, H.; Du, S.; Popkin, B.M.; Mendez, M.A. Differences in nutrient and energy contents of commonly consumed dishes prepared in restaurants v. at home in Hunan Province, China. Public Health Nutr. 2018, 21, 1307–1318. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Song, W.O.; Cho, M.S. Dietary quality differs by consumption of meals prepared at home vs. outside in Korean adults. Nutr. Res. Pract. 2016, 10, 294–304. [Google Scholar] [CrossRef] [PubMed]
- Nordstrom, J.; Thunstrom, L. The impact of price reductions on individuals’ choice of healthy meals away from home. Appetite 2015, 89, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Lachat, C.; Nago, E.; Verstraeten, R.; Roberfroid, D.; Van Camp, J.; Kolsteren, P. Eating out of home and its association with dietary intake: A systematic review of the evidence. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2012, 13, 329–346. [Google Scholar] [CrossRef]
- Duffey, K.J.; Gordon-Larsen, P.; Jacobs, D.R., Jr.; Williams, O.D.; Popkin, B.M. Differential associations of fast food and restaurant food consumption with 3-y change in body mass index: The Coronary Artery Risk Development in Young Adults Study. Am. J. Clin. Nutr. 2007, 85, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, C.; Fan, H.; Tian, X. Rising food accessibility contributed to the increasing dietary diversity in rural and urban China. Asia Pac. J. Clin. Nutr. 2017, 26, 738–747. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Xu, X.; Zhang, K.; Wang, H. Gender difference of metabolic syndrome and its association with dietary diversity at different ages. Oncotarget 2017, 8, 73568–73578. [Google Scholar] [CrossRef] [PubMed]
- Bhupathiraju, S.N.; Wedick, N.M.; Pan, A.; Manson, J.E.; Rexrode, K.M.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Quantity and variety in fruit and vegetable intake and risk of coronary heart disease. Am. J. Clin. Nutr. 2013, 98, 1514–1523. [Google Scholar] [CrossRef]
- Cooper, A.J.; Sharp, S.J.; Lentjes, M.A.; Luben, R.N.; Khaw, K.T.; Wareham, N.J.; Forouhi, N.G. A prospective study of the association between quantity and variety of fruit and vegetable intake and incident type 2 diabetes. Diabetes Care 2012, 35, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- Vadiveloo, M.; Dixon, L.B.; Mijanovich, T.; Elbel, B.; Parekh, N. Dietary variety is inversely associated with body adiposity among US adults using a novel food diversity index. J. Nutr. 2015, 145, 555–563. [Google Scholar] [CrossRef]
- McCrory, M.A.; Burke, A.; Roberts, S.B. Dietary (sensory) variety and energy balance. Physiol. Behav. 2012, 107, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Kwon, A.R.; Yoon, Y.S.; Min, K.P.; Lee, Y.K.; Jeon, J.H. Eating alone and metabolic syndrome: A population-based Korean National Health and Nutrition Examination Survey 2013–2014. Obes. Res. Clin. Pract. 2018, 12, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Zhai, F.Y.; Du, S.F.; Popkin, B.M. The China Health and Nutrition Survey, 1989–2011. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2014, 15, 2–7. [Google Scholar] [CrossRef] [PubMed]
- National Health and Family Planning Commission of the People’s Republic of China. Professional Standard of Health Care of the People’s Republic of China; National Health and Family Planning Commission of the People’s Republic of China: Beijing, China, 2013; Volume WS/T 428-2013. [Google Scholar]
- Du, W.W.; Zhang, B.; Wang, H.J.; Wang, Z.H.; Su, C.; Zhang, J.G.; Zhang, J.; Jia, X.F.; Jiang, H.R. Gender difference in the association between food away-from-home consumption and body weight outcomes among Chinese adults. Public Health Nutr. 2016, 19, 2984–2990. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, I.N.; Junior, E.V.; Pereira, R.A.; Sichieri, R. Away-from-home eating: Nutritional status and dietary intake among Brazilian adults. Public Health Nutr. 2015, 18, 1011–1017. [Google Scholar] [CrossRef]
- Regitz-Zagrosek, V.; Lehmkuhl, E.; Weickert, M.O. Gender differences in the metabolic syndrome and their role for cardiovascular disease. Clin. Res. Cardiol. Off. J. Ger. Cardiac Soc. 2006, 95, 136–147. [Google Scholar] [CrossRef]
- Huang, K.C.; Lin, R.C.; Kormas, N.; Lee, L.T.; Chen, C.Y.; Gill, T.P.; Caterson, I.D. Plasma leptin is associated with insulin resistance independent of age, body mass index, fat mass, lipids, and pubertal development in nondiabetic adolescents. Int. J. Obes. Relat. Metabol. Disord. J. Int. Assoc. Study Obes. 2004, 28, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Min, J.; Yan, A.F.; Wang, V.H.C.; Wang, Y. Obesity, body image, and its impact on children’s eating and exercise behaviors in China: A nationwide longitudinal study. Prev. Med. 2018, 106, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Azadbakht, L.; Hajishafiee, M.; Golshahi, J.; Esmaillzadeh, A. Snacking Behavior and Obesity among Female Adolescents in Isfahan, Iran. J. Am. Coll. Nutr. 2016, 35, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Azadbakht, L.; Esmaillzadeh, A. Dietary energy density is favorably associated with dietary diversity score among female university students in Isfahan. Nutrition 2012, 28, 991–995. [Google Scholar] [CrossRef]
- Robinson, E.; Jones, A.; Whitelock, V.; Mead, B.R.; Haynes, A. (Over)eating out at major UK restaurant chains: Observational study of energy content of main meals. BMJ 2018, 363, k4982. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Females | Males | |||||||
|---|---|---|---|---|---|---|---|---|
| Never | Sometimes | Often | p Trend 2 | Never | Sometimes | Often | p Trends | |
| Observations | 1798 | 476 | 167 | 1449 | 431 | 197 | ||
| Age(y) | 50.2 ±14.2 | 46.7 ± 14.3 | 40.4 ± 13.3 | <0.001 | 50.9 ± 15.1 | 47.2 ± 14.4 | 42.9 ± 13.2 | <0.001 |
| ln(income) 3 | 10.0 ±1.4 | 10.2 ± 1.3 | 10.3 ± 1.0 | <0.001 | 10.0 ± 1.4 | 10.2 ± 1.4 | 10.3 ± 1.4 | <0.001 |
| Educational level(%) 4 | ||||||||
| primary | 52.1 | 34.9 | 22.8 | <0.001 | 35.7 | 24.6 | 18.3 | <0.001 |
| middle | 44.5 | 58.2 | 62.9 | <0.001 | 59.1 | 67.3 | 68.5 | <0.001 |
| high | 3.3 | 6.9 | 14.4 | <0.001 | 5.2 | 8.1 | 13.2 | <0.001 |
| Physical activity(%) 5 | ||||||||
| light | 27.7 | 35.1 | 34.1 | 0.002 | 23.2 | 28.1 | 22.8 | 0.364 |
| middle | 24.9 | 28.4 | 37.7 | <0.001 | 16.9 | 22.5 | 22.8 | 0.004 |
| heavy | 47.4 | 36.6 | 28.1 | <0.001 | 59.9 | 49.4 | 54.3 | 0.002 |
| Smoking(%) | 3.9 | 2.3 | 0.0 | 0.003 | 54.7 | 60.1 | 64 | 0.004 |
| Drinking(%) | 7.6 | 12.4 | 7.8 | 0.059 | 59.1 | 68.9 | 70.1 | <0.001 |
| Rural (%) | 75.3 | 49.4 | 47.9 | <0.001 | 76.9 | 54.8 | 50.8 | <0.001 |
| North(%) | 49.2 | 22.1 | 29.9 | <0.001 | 48.6 | 26.2 | 21.8 | <0.001 |
| BMI | 23.3 ± 3.5 | 23.0 ± 3.3 | 22.5 ± 3.2 | 0.004 | 23.1 ± 3.3 | 22.9 ± 3.1 | 23.4 ± 3.8 | 0.486 |
| BMI ≥ 28(%) | 10.0 | 8.0 | 7.2 | 0.098 | 7.1 | 4.9 | 12.2 | 0.184 |
| Females | Males | |||||||
|---|---|---|---|---|---|---|---|---|
| Never | Sometimes | Often | p Trend 2 | Never | Sometimes | Often | p Trends | |
| Observations | 1798 | 476 | 167 | 1449 | 431 | 197 | ||
| Nutrients | ||||||||
| Total energy(kcal/day) | 1992 ± 585 | 1971 ± 562 | 1852 ± 588 | 0.008 | 2339 ± 663 | 2402 ± 666 | 2254 ± 715 | 0.611 |
| Carbohydrate(g/day) | 281 ± 96 | 260 ± 89 | 245 ± 83 | <0.001 | 329 ± 106 | 313 ± 106 | 291 ± 99 | <0.001 |
| Fat(g/day) | 68 ± 32 | 75 ± 33 | 68 ± 40 | 0.052 | 79 ± 38 | 88 ± 39 | 80 ± 51 | 0.020 |
| Protein(g/day) | 61 ± 21 | 63 ± 21 | 64 ± 22 | 0.024 | 70 ± 23 | 77 ± 26 | 77 ± 25 | <0.001 |
| Energy share (%) | ||||||||
| Carbohydrate | 56.6 | 52.9 | 54.0 | <0.001 | 56.5 | 52.5 | 52.8 | <0.001 |
| Fat | 30.9 | 34.1 | 31.7 | <0.001 | 30.2 | 32.3 | 30.8 | 0.007 |
| Protein | 12.3 | 12.8 | 14.1 | <0.001 | 12.1 | 12.9 | 13.9 | <0.001 |
| Mets Markers | ||||||||
| Waist circumference (cm) | 80 ± 10 | 80 ± 10 | 78 ± 9 | 0.006 | 83 ± 10 | 83 ± 9 | 85 ± 10 | 0.137 |
| Serum triglycerides (mg/dL) | 133 ± 101 | 125 ± 104 | 119 ± 96 | 0.043 | 147 ± 149 | 162 ± 142 | 162 ± 125 | 0.054 |
| HDL-C (mg/dL) | 57 ± 15 | 57 ± 14 | 59 ± 18 | 0.377 | 55 ± 17 | 53 ± 16 | 53 ± 17 | 0.054 |
| Fasting blood glucose (mg/dL) | 95 ± 21 | 93 ± 12 | 90 ± 11 | 0.001 | 95 ± 23 | 95 ± 25 | 94 ± 20 | 0.368 |
| Systolic blood pressure (mmHg) | 121 ± 17 | 117 ± 17 | 115 ± 15 | <0.001 | 125 ± 16 | 122 ± 16 | 122 ± 15 | 0.002 |
| Diastolic blood pressure (mmHg) | 78 ± 10 | 76 ± 10 | 76 ± 10 | <0.001 | 81 ± 10 | 80 ± 10 | 81 ± 11 | 0.205 |
| Share of patients | ||||||||
| MetS 3 (%) | 21.9 | 17.6 | 13.8 | 0.002 | 18.4 | 22.5 | 22.3 | 0.053 |
| Abdominal adiposity (%) | 32.4 | 30.9 | 25.8 | 0.092 | 26.3 | 26.0 | 30.5 | 0.350 |
| High serum triglyceride level (%) | 27.6 | 23.1 | 19.2 | 0.003 | 30.0 | 36.4 | 37.1 | 0.005 |
| Low HDL-C (%) | 31.4 | 31.3 | 33.5 | 0.690 | 13.9 | 18.1 | 17.3 | 0.047 |
| Abnormal glucose homeostasis (%) | 23.1 | 20.0 | 15.6 | 0.012 | 25.9 | 23.0 | 24.4 | 0.326 |
| Elevated blood pressure (%) | 32.6 | 24.4 | 15.0 | <0.001 | 41.8 | 35.7 | 39.6 | 0.119 |
| Total Population (n = 4518) | Females (n = 2441) | Males (n = 2077) | |
|---|---|---|---|
| Never(referent) | 1 | 1 | 1 |
| Sometimes | 1.475(1.121, 1.942) 2 | 0.962(0.727, 1.274) | 1.383(1.043, 1.834) |
| Often | 1.678(1.149, 2.451) | 0.861(0.535, 1.385) | 1.500(1.023, 2.199) |
| Females | 1.172(0.933, 1.472) | ||
| Females*sometimes | 0.622(0.428, 0.904) | ||
| Females*often | 0.443(0.247, 0.795) | ||
| Middle aged | 1.942(1.616, 2.332) | 2.524(1.952, 3.263) | 1.476(1.140, 1.910) |
| Elderly adults | 1.861(1.469, 2.358) | 2.968(2.153, 4.091) | 1.085(0.768, 1.534) |
| Indices | Females | Male ORs | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Never | Sometimes | Often | p Trend | Never | Sometimes | Often | p Trends | ||
| MetS 2 | Young 3 | 1 | 0.567(0.364, 0.884) 4 | 0.315(0.143, 0.697) | 0.000 | 1 | 0.877(0.569, 1.350) | 0.802(0.448, 1.436) | 0.367 |
| Middle aged | 1 | 1.060(0.704, 1.596) | 1.514(0.766, 2.991) | 0.308 | 1 | 1.826(1.252, 2.664) | 2.725(1.632, 4.550) | 0.000 | |
| Elderly | 1 | 1.336 (0.790, 2.260) | 1.233(0.384, 3.958) | 0.298 | 1 | 1.896(1.117, 3.216) | 1.561 (0.478, 5.095) | 0.031 | |
| Component of metabolic syndrome | |||||||||
| High serum TGs | Young | 1 | 0.615(0.423, 0.894) | 0.439(0.244, 0.788) | 0.000 | 1 | 1.183(0.843, 1.660) | 1.134(0.739, 1.740) | 0.356 |
| Middle aged | 1 | 1.130(0.789, 1.618) | 1.293(0.685, 2.444) | 0.320 | 1 | 1.414(1.014, 1.972) | 1.610(0.993, 2.610) | 0.009 | |
| Elderly | 1 | 0.893(0.535, 1.492) | 0.991 (0.306, 3.205) | 0.737 | 1 | 0.958(0.558, 1.645) | 0.557(0.163, 1.900) | 0.446 | |
| Low HDL | Young | 1 | 1.191(0.875, 1.620) | 1.301(0.860, 1.967) | 0.124 | 1 | 1.551(1.031, 2.334) | 1.435(0.841, 2.448) | 0.036 |
| Middle aged | 1 | 1.087(0.764, 1.547) | 1.045(0.553, 1.975) | 0.689 | 1 | 1.468(0.958, 2.248) | 1.609(0.894, 2.895) | 0.027 | |
| Elderly | 1 | 0.753(0.441, 1.287) | 0.665 (0.187, 2.372) | 0.239 | 1 | 0.949(0.476, 1.890) | 0.000(0.000, 0.000) | 0.174 | |
| Abdominal adiposity | Young | 1 | 0.745(0.520, 1.066) | 0.569(0.330, 0.981) | 0.014 | 1 | 0.853(0.573, 1.271) | 1.260(0.769, 2.063) | 0.711 |
| Middle aged | 1 | 1.685(1.192, 2.383) | 2.216(1.223, 4.016) | 0.000 | 1 | 1.494(0.990, 2.106) | 2.591(1.576, 4.257) | 0.000 | |
| Elderly | 1 | 1.755(1.086, 2.837) | 1.676(0.538, 5.226) | 0.024 | 1 | 1.695(0.997, 2.884) | 1.644(0.517, 5.234) | 0.056 | |
| Elevated blood pressure | Young | 1 | 0.386(0.253, 0.590) | 0.292(0.145, 0.588) | 0.000 | 1 | 0.522(0.364, 0.748) | 0.718(0.456, 1.129) | 0.005 |
| Middle aged | 1 | 0.825(0.559, 1.218) | 0.450(0.193, 1.051) | 0.044 | 1 | 1.008(0.719, 1.412) | 1.771(1.084, 2.894) | 0.064 | |
| Elderly | 1 | 2.462(1.505, 4.026) | 2.675(0.812, 8.806) | 0.000 | 1 | 2.045(1.241, 3.370) | 4.504(1.416, 14.324) | 0.000 | |
| Impaired fasting glucose | Young | 1 | 0.534(0.351, 0.812) | 0.374(0.190, 0.735) | 0.000 | 1 | 0.577(0.378, 0.880) | 0.396(0.207, 0.760) | 0.000 |
| Middle aged | 1 | 1.114(0.756, 1.643) | 1.336(0.674, 2.648) | 0.344 | 1 | 1.087(0.750, 1.577) | 2.257(1.371, 3.715) | 0.005 | |
| Elderly | 1 | 1.299(0.780, 2.164) | 0.902(0.257, 3.171) | 0.524 | 1 | 1.380(0.822, 2.317) | 1.668(0.600, 4.636) | 0.126 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.; Yu, Y.; Tian, X. Does Eating-Away-from-Home Increase the Risk of a Metabolic Syndrome Diagnosis? Int. J. Environ. Res. Public Health 2019, 16, 575. https://doi.org/10.3390/ijerph16040575
Wang H, Yu Y, Tian X. Does Eating-Away-from-Home Increase the Risk of a Metabolic Syndrome Diagnosis? International Journal of Environmental Research and Public Health. 2019; 16(4):575. https://doi.org/10.3390/ijerph16040575
Chicago/Turabian StyleWang, Hui, Yingjie Yu, and Xu Tian. 2019. "Does Eating-Away-from-Home Increase the Risk of a Metabolic Syndrome Diagnosis?" International Journal of Environmental Research and Public Health 16, no. 4: 575. https://doi.org/10.3390/ijerph16040575
APA StyleWang, H., Yu, Y., & Tian, X. (2019). Does Eating-Away-from-Home Increase the Risk of a Metabolic Syndrome Diagnosis? International Journal of Environmental Research and Public Health, 16(4), 575. https://doi.org/10.3390/ijerph16040575