Household Fuel Use for Heating and Cooking and Respiratory Health in a Low-Income, South African Coastal Community

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
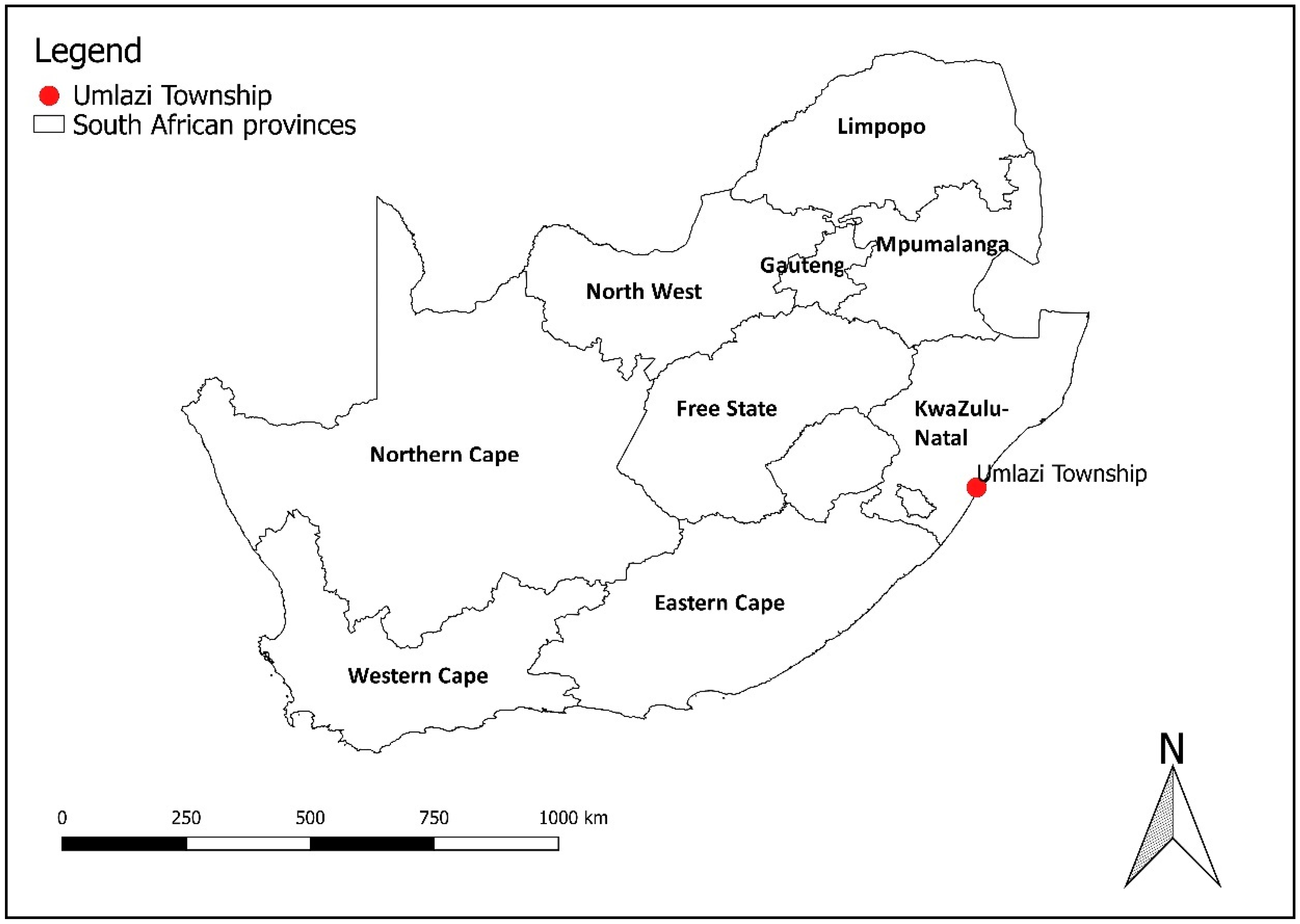
2.1. Study Area
2.2. Survey
2.3. Questionnaire
2.4. Data Management and Statistical Analyses
3. Results
3.1. Sample Description and General Profile of the Study Population
3.2. Prevalence of Respiratory Health Outcomes
3.3. Multiple Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Household air pollution and health. Available online: http://www.who.int/news-room/fact-sheets/detail/household-air-pollution-and-health (accessed on 8 November 2018).
- Ezzati, M. Indoor air pollution and health in developing countries. Lancet 2005, 366, 104–106. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Observatory (GHO) Data. Household Air Pollution. Available online: http://www.who.int/gho/phe/indoor_air_pollution/en/ (accessed on 14 November 2018).
- World Health Organization. Air Pollution. WHO Guideline for Indoor Air Quality: Household Fuel Combustion. Available online: https://www.who.int/airpollution/guidelines/household-fuel-combustion/en/ (accessed on 14 November 2018).
- Lam, N.L.; Smith, K.R.; Gauthier, A.; Bates, M.N. Kerosene: A review of household uses and their hazards in low- and middle-income countries. J. Toxicol. Environ. Health B. Crit. Rev. 2012, 15, 396–432. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef]
- Norman, R.; Barnes, B.; Mathee, A.; Bradshaw, D.; South African Comparitive Risk Assessment Collaboration. Estimating the burden of disease attributable to indoor air pollution from household use of solid fuels in South Africa in 2000. S. Afr. Med. J. 2007, 97, 764–771. [Google Scholar] [CrossRef] [PubMed]
- Petzer, G. Indoor Air Quality Issues in South Africa. In Proceedings of the 2009 National Association for Clean Air Conference, Vanderbijlpark, South Africa, October 2009. [Google Scholar]
- Bruce, N.; Perez-Padilla, R.; Albalak, R. Indoor air pollution in developing countries: A major environmental and public health challenge. Bull. World Health Organ. 2000, 78, 1078–1092. [Google Scholar] [PubMed]
- Smith, K.R.; Mehta, S. The burden of disease from indoor air pollution in developing countries: Comparison of estimates. Int. J. Hyg. Environ. Health 2003, 206, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Bruce, N.; Pope, D.; Rehfuss, E.; Kalpana, B.; Adair-Rohani, H.; Carlos, D. WHO indoor air quality guidelines on household fuel combustion: Strategy implications of new evidence on interventions and exposure-risk functions. Atmos. Environ. 2015, 106, 451–457. [Google Scholar] [CrossRef]
- Naicker, N.; Teare, J.; Balakrishna, Y.; Wright, C.Y.; Mathee, A. Indoor temperatures in low cost housing in Johannesburg, South Africa. Int. J. Environ. Res. Public Health 2017, 14, 1410. [Google Scholar] [CrossRef]
- Rehfuess, E.A.; Puzzolo, E.; Stanistreet, D.; Pope, D.; Bruce, N.G. Enablers and barriers to large-scale uptake of improved solid fuel stoves: A systematic review. Environ. Health Perspect. 2013, 122, 120–130. [Google Scholar] [CrossRef]
- Muyanja, D.; Allen, J.G.; Vallarinno, J.; Valeri, L.; Kakuhikire, B.; Bangsberg, D.R.; Christiani, D.C.; Tsai, A.C.; Lai, P.S. Kerosene lighting contributes to household air pollution in rural Uganda. Int. J. Indoor Environ. Health 2017, 27, 1022–1029. [Google Scholar] [CrossRef]
- Sidhu, M.K.; Ravindra, K.; Mor, S.; John, S. Household air pollution from various types of rural kitchens and its exposure assessment. Sci. Total Environ. 2017, 586, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Ni, K.; Carter, E.; Schauer, J.J.; Ezzati, M.; Zhang, Y.; Niu, H.; Lai, A.M.; Shan, M.; Wang, Y.; Yang, X.; et al. Seasonal variation in outdoor, indoor and personal air pollution exposures of women using wood stoves in the Tibetan Plateau: Baseline assessment for an energy intervention study. Environ. Int. 2016, 94, 449–457. [Google Scholar] [CrossRef]
- Deng, Q.; Deng, L.; Miao, Y.; Guo, X.; Li, Y. Particle deposition in the human lung: Health implications of particulate matter from different sources. Environ. Res. 2018, 169, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Fazlzadeh, M.; Rostami, R.; Hazrati, S.; Rastgu, A. Concentrations of carbon monoxide in indoor and outdoor air of Ghalyun cafes. Atmos. Pollut. Res. 2015, 6, 550–555. [Google Scholar] [CrossRef]
- Language, B.; Piketh, S.J.; Wernecke, B.; Burger, R. Household air pollution in South African low-income settlements: A case study. In Proceedings of the 24th International Conference on Modelling, Monitoring and Management of Air Pollution (AIR 2016), Crete, Greece, 20–22 June 2016. [Google Scholar]
- Muller, E.; Diab, R.D.; Binedell, M.; Hounsome, R. Health risk assessment of kerosene usage in an informal settlement in Durban, South Africa. Atmos. Environ. 2003, 37, 2015–2022. [Google Scholar] [CrossRef]
- Gordon, S.B.; Bruce, N.G.; Grigg, J.; Hibberd, P.L.; Kurmi, O.P.; Lam, K.B.; Mortimer, K.; Asante, K.P.; Balakrishnan, K.; Balmes, J.; et al. Respiratory risks from household air pollution in low and middle income countries. Lancet Respir. Med. 2014, 10, 823–860. [Google Scholar] [CrossRef]
- Department of Energy. IEP Planning Workshop. Overview of Universal Energy Access Strategy. Available online: http://www.energy.gov.za/files/IEP/Polokwane/Overview-of-Universal-Energy-Access-Strategy.pdf (accessed on 8 November 2018).
- Goldemberg, J.; Martinez-Gomez, J.; Sagar, A.; Smith, K.R. Household air pollution, health, and climate change: Cleaning the air. Environ. Res. Lett. 2018, 13. [Google Scholar] [CrossRef]
- STATS SA. Statistics South Africa. Statistics by Place. Ethekwini. Umlazi. Available online: http://www.statssa.gov.za/?page_id=4286&id=10459 (accessed on 08 November 2018).
- Niranjan, I. A Case Study of Environmental Health in the South Durban Basin. Master’s Thesis, University of KwaZulu Natal, KwaZulu Natal, South Africa, January 2005. [Google Scholar]
- Diab, R.; Prause, A.; Bencherif, H. Analysis of SO2 Pollution in the South Durban Industrial Basin. S. Afr. J. Sci. 2002, 98, 543–546. [Google Scholar]
- Nriagu, J.; Robins, T.; Gary, L.; Liggans, G.; Davila, R.; Supuwood, K.; Harvey, C.C.; Naidoo, R. Prevalence of asthma and respiratory symptoms in south-central Durban, South Africa. Eur. J. Epidemiol. 1999, 15, 747–755. [Google Scholar] [CrossRef]
- Naidoo, R.N.; Robins, T.G.; Batterman, S.; Mentz, G.; Jack, C. Ambient pollution and respiratory outcomes among schoolchildren in Durban, South Africa. S. Afr. J. Child Health 2013, 7, 127–134. [Google Scholar] [CrossRef]
- Frankfort-Nachmias, C.; Nachmias, D. Research Methods in the Social Sciences, 5th ed.; St. Martin’s Press: New York, NY, USA, 1996. [Google Scholar]
- Ferris, B.G. Epidemiology standardization project. Am. Rev. Respir. Dis. 1978, 118, 1–120. [Google Scholar] [PubMed]
- Terblanche, P.; Opperman, L.; Nel, C.M.E.; Reinach, S.G.; Tosen, G.; Cadman, A. Preliminary results of exposure measurements and health effects of the Vaal Triangle Air Pollution Health Study. S. Afr. Med. J. 1992, 81, 550–556. [Google Scholar] [PubMed]
- Albers, P.N.; Wright, C.Y.; Voyi, K.V.V.; Mathee, A. Household fuel use and child respiratory ill health in two towns in Mpumalanga, South Africa. S. Afr. Med. J. 2016, 105, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.Y.; Nkosi, V.; Wichmann, J. Respiratory Health Symptoms among Schoolchildren in Relation to Possible Food-Related Risk and Protective Factors. Int. J. Environ. Res. Public Health 2018, 15, 502. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 14; StataCorp LP: College Station, TX, USA, 2015. [Google Scholar]
- Israel-Akinbo, S.O.; Snowball, J.; Fraser, G. An Investigation of Multidimensional Energy Poverty among South African Low-income Households. South Afr. J. Econ. 2018, (in press).
- Mgwambani, S.L.; Kasangana, K.K.; Makonene, T.; Masekameni, D.; Gulumian, M.; Mbonane, T.P. Assessment of Household Energy Poverty levels in Louiville, Mpumalanga, South Africa. In Proceedings of the Domestic Use of Energy Conference, Cape Peninsula University of Technology, Cape Town, South Africa, 3–5 April 2018. [Google Scholar]
- Lloyd, P. The Energy Profile of a low-income urban community. In Proceedings of the Domestic Use of Energy Conference, Cape Peninsula University of Technology, Cape Town, South Africa, 29 March–2 April 2014. [Google Scholar]
- Ismail, Z.; Khembo, P. Determinants of energy poverty in South Africa. J. Energy South Afr. 2015, 26, 66–78. [Google Scholar]
- Krieger, J.; Higgins, D.L. Housing and Health: Time Again for Public Health Action. Am. J. Public Health 2002, 92, 758–768. [Google Scholar] [CrossRef]
- Weinmayr, G.; Gehring, U.; Genuneit, J.; Buchele, G.; Kleiner, A.; Siebers, R.; Wickens, K.; Crane, J.; Brunekreef, B.; Strachan, D.P.; et al. Dampness and moulds in relation to respiratory and allergic symptoms in children: Results from Phase Two of the International Study of Asthma and Allergies in Childhood (ISAAC Phase Two). Clin. Exp. Allergy 2013, 43, 762–774. [Google Scholar] [CrossRef]
- Fell, A.K.M.; Svendsen, M.V.; Kim, J.L.; Abrahamsen, R.; Henneberger, P.K.; Toren, K.; Blanc, P.D.; Kongerud, J. Exposure to second-hand tobacco smoke and respiratory symptoms in non-smoking adults: Cross-sectional data from the general population of Telemark, Norway. BMC Public Health 2018, 18, 843–851. [Google Scholar] [CrossRef]
- Vanker, A.; Gie, R.P.; Zar, H.J. Early-life exposures to environmental tobacco smoke and indoor air pollution in the Drakenstein Child Health Study: Impact on child health. S. Afr. Med. J. 2018, 108, 71–72. [Google Scholar] [CrossRef]
- Ezzati, M.; Kammen, D.M. Indoor air pollution from biomass combustion and acute respiratory infections in Kenya: An exposure-response study. Lancet 2001, 358, 619–624. [Google Scholar] [CrossRef]
- Tunno, B.J.; Naumoff Schields, K.; Cambal, L.; Tripathy, S.; Holguin, F.; Lioy, P.; Clougherty, J.E. Indoor air sampling for fine particulate matter and black carbon in industrial communities in Pittsburgh. Sci. Total Environ. 2015, 536, 108–115. [Google Scholar] [CrossRef]
- Wernecke, B. Ambient and Indoor Particulate Matter Concentrations on the Mpumalanga Highveld. Master’s Thesis, North West University, Potchefstroom, South Africa, May 2018. [Google Scholar]
- Guastella, L.; Knudsen, S. South Durban Basin Multi-Point Plan: Case Study Report. Air Quality Act Implementation: Air Quality Management Planning; Department of Environmental Affairs and Tourism: Pretoria, South Africa, 2007.
- Kistnasamy, J. The Relationship between Asthma and Outdoor Air Pollutant Concentrations of Sulphur Dioxide, Oxides of Nitrogen, Ozone, Total Reduced Sulphates, Carbon Monoxide and Respirable Particulate Matter Less than 10 Microns in Learners and Teachers at Settlers Primary School in Merebank, South Durban. Master’s Thesis, Environmental Health, Durban Institute of Technology, Durban, South Africa, 2005. [Google Scholar]
- Vissers, A. Perceptions of Air Pollution and its Impact on Human Health in the South Durban Basin: A Community Perspective. Master’s Thesis, University of South Africa, Pretoria, South Africa, 2010. [Google Scholar]
- Wittwer, R.; Hubrivh, S. Nonresponse in Household Surveys: A Survey of Non-respondents from Repeated Cross-sectional Study “Mobility in Cities—SrV” in Germany. Transp. Res. Procedia. 2015, 11, 66–84. [Google Scholar] [CrossRef]
- Barnes, B.; Mathee, A.; Thomas, E.; Bruce, N. Household energy, indoor air pollution and child respiratory health in South Africa. J. Energy South Afr. 2009, 20, 1–13. [Google Scholar] [CrossRef]
- Shezi, B.; Wright, C.Y. Household air pollution exposure and respiratory health outcomes: A narrative review update of the South African epidemiological evidence. Clean Air J. 2018, 28, 43–56. [Google Scholar] [CrossRef]
- World Health Organisation. Fuel for Life. Household Energy and Health. Available online: http://www.who.int/airpollution/publications/fuelforlife.pdf. (accessed on 14 November 2018).


{kind=link}
| Questionnaire Variable | Response Item | Percentage of Participants n = 245 (%) |
|---|---|---|
| Gender of the respondent | Male | 38.9 |
| Female | 60.7 | |
| Missing | 0.4 | |
| Type of home | Single unattached dwelling | 44.9 |
| Single attached dwelling | 39.4 | |
| Hostel | 14.5 | |
| Missing | 2.0 | |
| Main fuel used mostly for cooking | Electricity | 61.6 |
| Paraffin | 17.7 | |
| Gas | 13.9 | |
| Electricity and Gas | 5.5 | |
| Wood/coal | 1.2 | |
| Missing | 3.2 | |
| All heating methods used in the household | Portable electric heater | 17.6 |
| Gas heater | 4.1 | |
| Paraffin | 27.3 | |
| Wood/coal | 11.8 | |
| Missing | 38.8 | |
| Open doors and windows in winter | No | 19.7 |
| Yes | 80.3 | |
| Missing | 0.4 | |
| Mould or mildew in the home | No | 50.2 |
| Yes | 49.8 | |
| Missing | 0.0 | |
| Pets allowed in the home | No | 92.2 |
| Yes | 7.8 | |
| Missing | 0.0 | |
| A household member smokes inside the dwelling on a daily basis | No | 77.5 |
| Yes | 21.6 | |
| Missing | 0.82 | |
| Does the respondent currently smoke? | No | 78.8 |
| Yes | 21.2 | |
| Health status—URTI (past month) | Hay fever | 7.8 |
| Runny nose | 3.7 | |
| Ear ache | 2.5 | |
| Health status—LRTI (past year) | Wheezing | 15.9 |
| Bronchitis | 6.9 | |
| Asthma | 3.7 |
| Energy Source | URTI n = 27 n (%) | LRTI n = 44 n (%) | |
|---|---|---|---|
| Used for cooking | Electricity | 15 (57.7) | 25 (62.5) |
| Paraffin | 4 (15.4) | 9 (22.50) | |
| Gas | 6 (23.1) | 2 (5.0) | |
| Wood/coal | 0 (0.0) | 0 (0.0) | |
| Missing | 2 | 8 | |
| Used for heating | Portable electric heater | 6 (22.2) | 13 (29.6) |
| Gas heater | 2 (7.4) | 4 (9.1) | |
| Paraffin | 13 (48.2) | 12 (27.3) | |
| Wood/coal | 0 (0.0) | 1 (2.3) | |
| Missing | 6 | 14 |
| Energy Source | Prevalence (%) | p-Value | OR (95% CI) | Adjusted p-Value | Adjusted OR (95% CI) a |
|---|---|---|---|---|---|
| Any URTI (n = 27 **) | |||||
| Heating | |||||
| Non-electric a | 33.3 | <0.05 | 3.0 (1.3–6.7) | <0.05 | 3.6 (1.2–10.1) |
| Electric b | 22.2 | 0.50 | 1.4 (0.5–3.7) | 0.90 | 1.1 (0.3–4.4) |
| Cooking | |||||
| Non-electric c | 37.0 | 0.08 | 2.1 (0.9–4.9) | <0.05 | 2.9 (1.1–7.9) |
| Electric d | 18.5 | 0.65 | 0.8 (0.3–1.8) | 0.37 | 0.6 (0.2–1.7) |
| Any LRTI (n = 44 **) | |||||
| Heating | |||||
| Non-electric e | 43.2 | 0.32 | 1.4 (0.2–2.7) | 0.28 | 1.5 (0.7–3.3) |
| Electric f | 29.5 | <0.05 | 2.3 (1.1–5.0) | <0.05 | 2.7 (1.1–6.4) |
| Cooking | |||||
| Non-electric g | 25.0 | 0.76 | 1.1 (0.5–2.4) | 0.95 | 1.0 (0.3–3.0) |
| Electric h | 56.8 | 0.68 | 0.8 (0.4–1.6) | 0.72 | 0.8 (0.3–2.0) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buthelezi, S.A.; Kapwata, T.; Wernecke, B.; Webster, C.; Mathee, A.; Wright, C.Y. Household Fuel Use for Heating and Cooking and Respiratory Health in a Low-Income, South African Coastal Community. Int. J. Environ. Res. Public Health 2019, 16, 550. https://doi.org/10.3390/ijerph16040550
Buthelezi SA, Kapwata T, Wernecke B, Webster C, Mathee A, Wright CY. Household Fuel Use for Heating and Cooking and Respiratory Health in a Low-Income, South African Coastal Community. International Journal of Environmental Research and Public Health. 2019; 16(4):550. https://doi.org/10.3390/ijerph16040550
Chicago/Turabian StyleButhelezi, Sikhumbuzo Archibald, Thandi Kapwata, Bianca Wernecke, Candice Webster, Angela Mathee, and Caradee Yael Wright. 2019. "Household Fuel Use for Heating and Cooking and Respiratory Health in a Low-Income, South African Coastal Community" International Journal of Environmental Research and Public Health 16, no. 4: 550. https://doi.org/10.3390/ijerph16040550
APA StyleButhelezi, S. A., Kapwata, T., Wernecke, B., Webster, C., Mathee, A., & Wright, C. Y. (2019). Household Fuel Use for Heating and Cooking and Respiratory Health in a Low-Income, South African Coastal Community. International Journal of Environmental Research and Public Health, 16(4), 550. https://doi.org/10.3390/ijerph16040550