Conventional Rehabilitation Therapy Versus Telerehabilitation in Cardiac Patients: A Comparison of Motivation, Psychological Distress, and Quality of Life


 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Participants
2.3. Procedure
2.4. The Intervention
2.4.1. TR Group
2.4.2. The Control Group
2.5. Measures
Psychological Measures
3. Results
3.1. Baseline Characteristics
3.2. Motivation
3.3. Anxiety, Depression, and Quality of Life (QoL)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Data and Statistics. Available online: http://www.euro.who.int/en/health-topics/noncommunicable-diseases/cardiovascular-diseases/data-and-statistics (accessed on 21 November 2018).
- British Heart Foundation. Coronary Heart Disease Statistics, 2010 ed.; British Heart Foundation: Birmingham, England, 2010; Available online: https://www.bhf.org.uk/informationsupport/publications/statistics/coronary-heart-disease-statistics-2010 (accessed on 6 January 2019).
- Yohannes, A.M.; Doherty, P.; Bundy, C.; Yalfani, A. The long-term benefits of cardiac rehabilitation on depression, anxiety, physical activity and quality of life. J. Clin. Nurs. 2010, 19, 2806–2813. [Google Scholar] [CrossRef] [PubMed]
- Choo, C.C.; Chew, P.; Lai, S.M.; Soo, S.C.; Ho, C.S.; Ho, R.C.; Wong, R.C. Effect of cardiac rehabilitation on quality of life, depression, and anxiety in Asian patients. Int. J. Environ. Health Res. 2018, 15, 1095. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, E.; Piepoli, M.F.; Jaarsma, T.; Lambrinou, E.; Coats, A.J.; Schmid, J.P.; Adamopoulos, S. Telerehabilitation in heart failure patients: The evidence and the pitfalls. Int. J. Cardiol. 2016, 220, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, E.; Baranowski, R.; Bilinska, M.; Stepnowska, M.; Piotrowska, M.; Wójcik, A.; Piotrowski, W. A new model of home-based telemonitored cardiac rehabilitation in patients with heart failure: Effectiveness, quality of life, and adherence. Eur. J. Heart Fail. 2010, 12, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Dalleck, L.C.; Schmidt, L.K.; Lueker, R. Cardiac rehabilitation outcomes in a conventional versus telemedicine-based programme. J. Telemed. Telecare 2011, 17, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Cranen, K.; Drossaert, C.H.; Brinkman, E.S.; Braakman-Jansen, A.L.; IJzerman, M.J.; Vollenbroek-Hutten, M.M. An exploration of chronic pain patients’ perceptions of home telerehabilitation services. Health Expect. 2012, 15, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Balady, G.J.; Ades, P.A.; Bittner, V.A.; Franklin, B.B.; Gordon, N.F.; Thomas, R.J.; Tomaselli, G.F.; Yancy, C.W. Referral, enrollment, and delivery of cardiac rehabilitation/secondary prevention programs at clinical centers and beyond. Circulation 2011, 124, 2951–2960. [Google Scholar] [CrossRef]
- Dinesen, B.; Nonnecke, B.; Lindeman, D.; Toft, E.; Kidholm, K.; Jethwani, K.; Young, H.M.; Spindler, H.; Oestergaard, C.U.; Southard, J.A.; et al. Personalized telehealth in the future: A global research agenda. J. Med. Internet Res. 2016, 18, e53. [Google Scholar] [CrossRef]
- Wootton, R. Twenty years of telemedicine in chronic disease management—An evidence synthesis. J. Telemed. Telecare 2012, 18, 211–220. [Google Scholar] [CrossRef]
- Brennan, D.; Tindall, L.; Theodoros, D.; Brown, J.; Campbell, M.; Christiana, D.; Lee, A. A blueprint for telerehabilitation guidelines. Int. J. Telerehab. 2010, 2, 31. [Google Scholar] [CrossRef]
- Cranen, K.; Groothuis-Oudshoorn, C.G.; Vollenbroek-Hutten, M.M.; IJzerman, M.J. Toward patient-centered telerehabilitation design: Understanding chronic pain patients’ preferences for web-based exercise telerehabilitation using a discrete choice experiment. J. Med. Internet Res. 2017, 19, e26. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, M.; Hirani, S.P.; Rixon, L.; Beynon, M.; Doll, H.; Bower, P.; Rogers, A. Effect of telehealth on quality of life and psychological outcomes over 12 months (Whole Systems Demonstrator telehealth questionnaire study): Nested study of patient reported outcomes in a pragmatic, cluster randomised controlled trial. BMJ 2013, 346, f653. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Dalal, H.; Jolly, K.; Moxham, T.; Zawada, A. Home-based versus centre-based cardiac rehabilitation. Cochrane Database Syst. Rev. 2010, CD007130. [Google Scholar] [CrossRef]
- McLean, S.; Protti, D.; Sheikh, A. Telehealthcare for long term conditions. BMJ 2011, 342, d120. [Google Scholar] [CrossRef] [PubMed]
- Thorup, C.B.; Grønkjær, M.; Spindler, H.; Andreasen, J.J.; Hansen, J.; Dinesen, B.I.; Sørensen, E.E. Pedometer use and self-determined motivation for walking in a cardiac telerehabilitation program: A qualitative study. BMC Sports Sci. Med. Rehab. 2016, 8, 24. [Google Scholar] [CrossRef] [PubMed]
- Fors, A.; Taft, C.; Ulin, K.; Ekman, I. Person-centred care improves self-efficacy to control symptoms after acute coronary syndrome: A randomized controlled trial. Eur. J. Cardiovasc. Nurs. 2016, 15, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Jansson, I.; Fors, A.; Ekman, I.; Ulin, K. Documentation of person-centred health plans for patients with acute coronary syndrome. Eur. J. Cardiovasc. Nurs. 2018, 17, 114–122. [Google Scholar] [CrossRef]
- Ulin, K.; Malm, D.; Nygårdh, A. What is known about the benefits of patient-centered care in patients with heart failure. Curr. Heart Fail. Rep. 2015, 12, 350–359. [Google Scholar] [CrossRef]
- Fletcher, S.M.; Burley, M.B.; Thomas, K.E.; Mitchell, E.K. Feeling supported and abandoned: Mixed messages from attendance at a rural community cardiac rehabilitation program in Australia. J. Cardiopulm. Rehabil. Prev. 2014, 34, 29–33. [Google Scholar] [CrossRef]
- Cho, Y.-M.; Lee, S.; Islam, S.M.S.; Kim, S.Y. Theories applied to m-Health interventions for behavior change in low- and middle-income countries: A systematic review. Telemed. E-Health 2018, 24, 727–741. [Google Scholar] [CrossRef]
- Ryan, R.M.; Patrick, H.; Deci, E.L.; Williams, G.C. Facilitating health behaviour change and its maintenance: Interventions based on self-determination theory. Eur. Health Psychol. 2008, 10, 2–5. [Google Scholar]
- Rahman, R.J.; Hudson, J.; Thøgersen-Ntoumani, C.; Doust, J.H. Motivational processes and well-being in cardiac rehabilitation: A self-determination theory perspective. Psychol. Health Med. 2015, 20, 518–529. [Google Scholar] [CrossRef] [PubMed]
- Lane, D.; Carroll, D.; Ring, C.; Beevers, D.G.; Lip, G.Y. Mortality and quality of life 12 months after myocardial infarction: Effects of depression and anxiety. Psychosom. Med. 2001, 63, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Carels, R.A. The association between disease severity, functional status, depression and daily quality of life in congestive heart failure patients. Qual. Life Res. 2004, 13, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Bekelman, D.B.; Havranek, E.P.; Becker, D.M.; Kutner, J.S.; Peterson, P.N.; Wittstein, I.S.; Gottlieb, S.H.; Yamashita, T.E.; Fairclough, D.L.; Dy, S.M. Symptoms, depression, and quality of life in patients with heart failure. J. Card. Fail. 2007, 13, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Hwang, B.; Moser, D.K.; Dracup, K. Knowledge is insufficient for self-care among heart failure patients with psychological distress. Health Psychol. 2014, 33, 588–596. [Google Scholar] [CrossRef]
- Daly, J.; Sindone, A.P.; Thompson, D.R.; Hancock, K.; Chang, E.; Davidson, P. Barriers to participation in and adherence to cardiac rehabilitation programs: A critical literature review. Prog. Cardiovasc. Nurs. 2002, 17, 8–17. [Google Scholar] [CrossRef]
- Von Hippel, E. Democratizing Innovation; MIT Press: Cambridge, MA, USA, 2005. [Google Scholar]
- Dinesen, B. Teledialog—Tele-Rehabilitation of Heart Patients (Teledialog) (Clinicaltrials.gov Identifier NCT01752192). Available online: https://clinicaltrials.gov/ct2/show/study/NCT01752192 (accessed on 28 November 2018).
- Teledialog UK. Available online: https://www.youtube.com/watch?v=gegto_B0YRA (accessed on 12 February 2019).
- Sundhedsstyrelsen. National Klinisk Retningslinje for Hjerterehabilitering; Sundhedsstyrelsen: Copenhagen, Denmark, 2013; ISBN 9788771045277. Available online: https://www.sst.dk/da/udgivelser/2015/~/media/401919781C684EE9AAE544EB5E76847B.ashx (accessed on 2 October 2018).
- Williams, G.C.; Ryan, R.M.; Deci, E.L. Health-Care, Self-Determination Theory Packet. 2004. Available online: http://selfdeterminationtheory.org/health-care-self-determination-theory/ (accessed on 9 June 2016).
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Herrmann, C. International experiences with the Hospital Anxiety and Depression Scale-a review of validation data and clinical results. J. Psychosom. Res. 1997, 42, 17–41. [Google Scholar] [CrossRef]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Burns, A.; Höfer, S.; Curry, P.; Sexton, E.; Doyle, F. Revisiting the dimensionality of the Hospital Anxiety and Depression Scale in an international sample of patients with ischaemic heart disease. J. Psychosom. Res. 2014, 77, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.R.; Thompson, D.R.; Barth, J. Factor structure of the Hospital Anxiety and Depression Scale in coronary heart disease patients in three countries. J. Eval. Clin. Pract. 2008, 14, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Emons, W.H.; Sijtsma, K.; Pedersen, S.S. Dimensionality of the Hospital Anxiety and Depression Scale (HADS) in cardiac patients: Comparison of Mokken scale analysis and factor analysis. Assessment 2012, 19, 337–353. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. Formatual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Kidholm, K.; Rasmussen, M.K.; Andreasen, J.J.; Hansen, J.; Nielsen, G.; Spindler, H.; Dinesen, B. Cost-utility analysis of a cardiac telerehabilitation program: The Teledialog Project. Telemed. E-Health 2016, 22, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Markland, D.; Ryan, R.M.; Tobin, V.J.; Rollnick, S. Motivational interviewing and self–determination theory. J. Soc. Clin. Psychol. 2005, 24, 811–831. [Google Scholar] [CrossRef]
- Pâquet, M.; Bolduc, N.; Xhignesse, M.; Vanasse, A. Re-engineering cardiac rehabilitation programmes: Considering the patient’s point of view. J. Adv. Nurs. 2005, 51, 567–576. [Google Scholar] [CrossRef]
- Melholt, C.; Joensson, K.; Spindler, H.; Hansen, J.; Andreasen, J.J.; Nielsen, G.; Dinesen, B. Cardiac patients’ experiences with a telerehabilitation web portal: Implications for eHealth literacy. Patient Educ. Couns. 2018, 101, 854–861. [Google Scholar] [CrossRef]
- Söllner, W.; DeVries, A.; Steixner, E.; Lukas, P.; Sprinzl, G.; Rumpold, G.; Maislinger, S. How successful are oncologists in identifying patient distress, perceived social support, and need for psychosocial counselling? Br. J. Cancer 2001, 84, 179. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Tele-rehabilitation (TR) n = 69 | Conventional Rehabilitation (CR) n = 65 | Total Sample | p-Value |
|---|---|---|---|---|
| Sociodemographic variables | ||||
| Age mean (SD) | 61.86 ± 12.46 | 62.68 ± 11.95 | 62.25 ± 12.17 | 0.70 |
| Males n (%) | 54 (50.5) | 53 (49.5) | 107 (79.9) | 0.64 |
| Education | 46 (50) | 46 (50) | 92 (71.3) | 0.49 |
| Work | 28 (53.8) | 24 (46.2) | 52 (44.1) | 0.93 |
| Clinical variables | ||||
| Acute Coronary Syndrome (ACS) n (%) | 42 (50.6) | 41 (49.4) | 83 (61.9) | 0.80 |
| Bypass n (%) | 12 (57.1) | 9 (42.9) | 21 (15.7) | 0.57 |
| Heart Valve n (%) | 12 (66.7) | 6 (33.3) | 18 (13.4) | 0.17 |
| Heart Failure n (%) | 18 (48.6) | 19 (51.4) | 37 (27.6) | 0.68 |
| Hypertension n (%) | 4 (66.7) | 2 (33.3) | 6 (4.5) | 0.45 |
| Diabetes (type 1+2) n (%) | 3 (75.0) | 1 (25.0) | 4 (3.0) | 0.34 |
| Obesity n (%) | 3 (60.0) | 2 (40.0) | 5 (3.7) | 0.70 |
| Motivation | ||||
| Autonomous Motivation | 6.00 ± 0.97 | 6.31 ± 0.84 | 6.15 ± 0.92 | 0.049 |
| Controlled Motivation | 3.51 ± 1.51 | 3.96 ± 1.43 | 3.73 ± 1.50 | 0.08 |
| Amotivation | 2.77 ± 1.54 | 2.61 ± 1.53 | 2.67 ± 1.53 | 0.55 |
| Perceived Competence | 5.22 ± 1.18 | 5.39 ± 1.24 | 5.30 ± 1.21 | 0.41 |
| Healthcare Climate | 5.69 ± 1.15 | 5.50 ± 1.43 | 5.59 ± 1.29 | 0.39 |
| Psychological variables | ||||
| Anxiety | 7.10 ± 4.48 | 5.82 ±3.41 | 6.54 ± 4.04 | 0.07 |
| Depression | 5.58 ± 4.05 | 4.46 ± 2.95 | 5.07 ± 3.57 | 0.07 |
| Physical functioning | 58.99 ± 28.14 | 65.54 ± 26.39 | 62.10 ± 27.40 | 0.17 |
| Social functioning | 73.01 ± 28.57 | 79.04 ± 23.71 | 75.74 ± 26.25 | 0.19 |
| Role physical functioning | 35.87 ± 41.89 | 41.15 ± 42.26 | 38.05 ± 41.83 | 0.47 |
| Role emotional functioning | 56.52 ± 42.90 | 57.95 ± 44.60 | 57.11 ± 43.30 | 0.85 |
| Mental Health | 66.72 ± 22.07 | 71.82 ± 19.47 | 69.09 ± 20.81 | 0.16 |
| Vitality | 46.16 ± 27.64 | 52.15 ± 24.62 | 48.86 ± 26.18 | 0.19 |
| Pain | 58.72 ± 27.55 | 61.14 ± 28.46 | 59.62 ± 27.83 | 0.62 |
| General Health | 59.42 ± 23.56 | 63.60 ± 21.87 | 61.18 ± 22.76 | 0.29 |
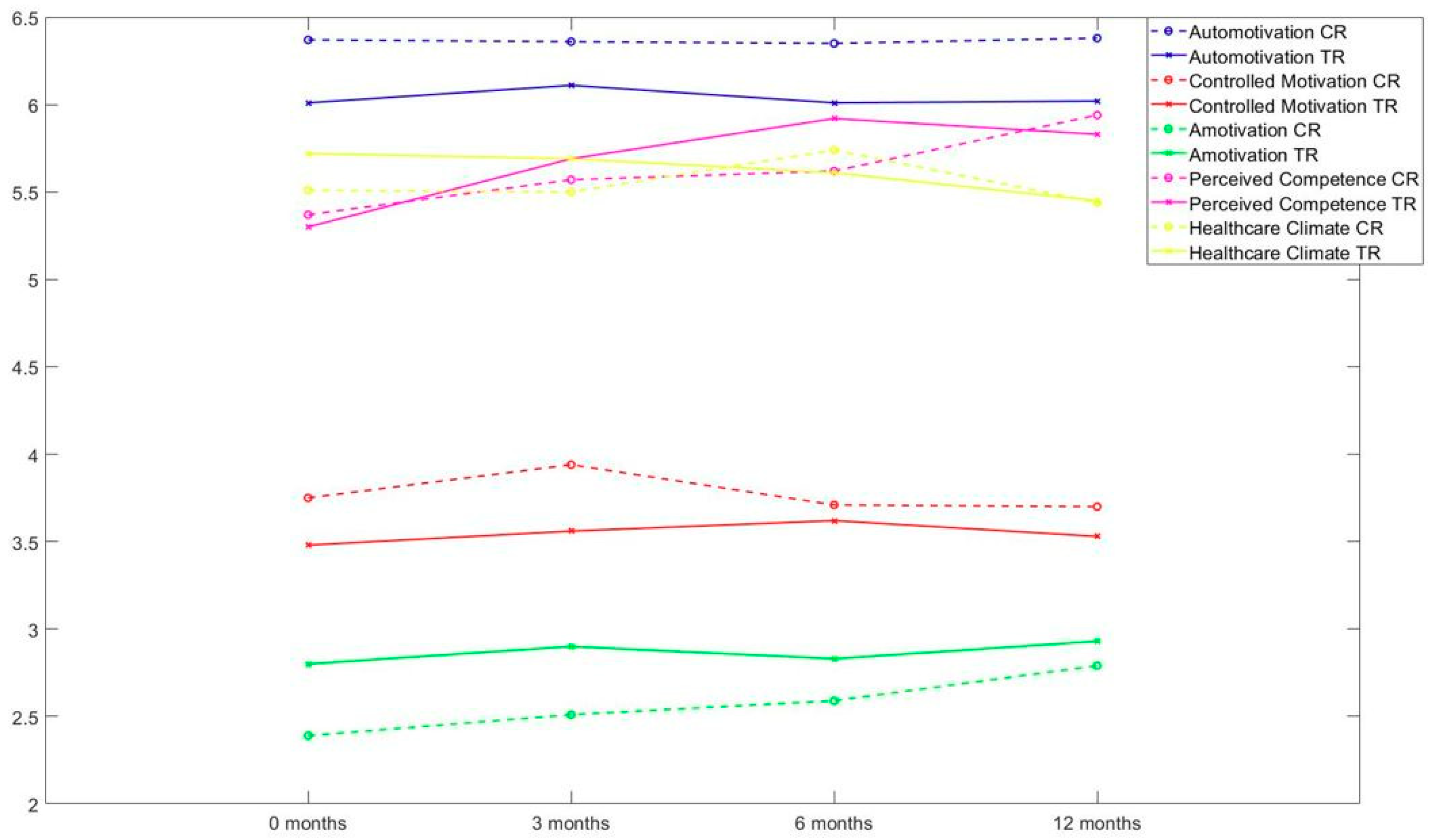
| Time Point | 0 mos. Mean (S.D.) | 3 mos. Mean (S.D.) | 6 mos. Mean (S.D.) | 12 mos. Mean (S.D.) | F Time Group Interaction | p-Value |
|---|---|---|---|---|---|---|
| Motivation | ||||||
| Autonomous Motivation TR (n = 64) CR (n = 55) | 6.01 (0.98) 6.37 (0.85) | 6.11 (0.91) 6.36 (0.86) | 6.01 (1.16) 6.35 (.76) | 6.02 (1.01) 6.38 (0.77) | F2.78 = 0.21 F = 5.09 F2.78 = 0.09 | 0.88 0.03 0.85 |
| Controlled Motivation TR (n = 64) CR (n = 55) | 3.48 (1.53) 3.75 (1.47) | 3.56 (1.41) 3.94 (1.37) | 3.62 (1.55) 3.71 (1.42) | 3.53 (1.54) 3.70 (1.73) | F2.86 = 0.55 F = 0.64 F2.86 = 0.54 | 0.64 0.33 0.65 |
| Amotivation TR (n = 64) CR (n = 55) | 2.80 (1.56) 2.39 (1.47) | 2.90 (1.47) 2.51 (1.23) | 2.83 (1.62) 2.59 (1.37) | 2.93 (1.71) 2.79 (1.54) | F3 = 1.28 F = 1.73 F3 = 0.45 | 0.28 0.19 0.72 |
| Perceived Competence TR (n = 64) CR (n = 55) | 5.30 (1.16) 5.37 (1.29) | 5.69 (1.27) 5.57 (1.27) | 5.92 (1.11) 5.62 (1.23) | 5.83 (1.23) 5.94 (1.14) | F2.85 = 8.68 F = 0.11 F2.85 = 1.31 | 0.00 0.74 0.27 |
| Healthcare Climate TR (n = 64) CR (n = 55) | 5.72 (1.18) 5.51 (1.52) | 5.69 (1.28) 5.50 (1.47) | 5.61 (1.42) 5.74 (1.32) | 5.45 (1.51) 5.44 (1.57) | F2.71 = 1.24 F = 0.11 F2.71 = 0.81 | 0.30 0.74 0.48 |
| Psychological | ||||||
| Anxiety TR (n = 64) CR (n = 55) | 7.06 (4.49) 5.93 (3.67) | 5.42 (4.33) 5.15 (3.90) | 5.38 (4.18) 5.11 (4.02) | 5.06 (3.92) 4.78 (3.85) | F2.69 = 10.70 F = 0.56 F2.69 = 1.04 | 0.00 0.45 0.37 |
| Depression TR (n = 64) CR (n = 55) | 5.53 (4.01) 4.51 (3.06) | 4.38 (4.16) 4.20 (3.69) | 4.44 (4.52) 4.16 (3.53) | 4.47 (4.78) 3.64 (3.25) | F2.49 = 3.40 F = 0.89 F2.49 = 0.83 | 0.03 0.35 0.46 |
| Quality of Life | ||||||
| Physical functioning TR(n = 64) CR(n = 55) | 60.63 (28.32) 67.09 (25.25) | 73.59 (26.19) 75.82 (21.73) | 74.61 (25.33) 75.45 (24.21) | 74.38 (26.13) 76.36 (23.44) | F1.83 = 18.83 F = 0.50 F1.83 = 0.91 | 0.00 0.48 0.40 |
| Social functioning TR (n = 64) CR (n = 55) | 71.68 (28.97) 78.18 (24.44) | 78.71 (25.26) 86.82 (16.57) | 83.20 (22.63) 85.45 (21.08) | 85.35 (21.31) 85.45 (21.21) | F2.63 = 9.49 F = 1.65 F2.63 = 1.45 | 0.00 0.20 0.23 |
| Rolephysical functioning TR (n = 64) CR (n = 55) | 37.11 (42.95) 40.91 (43.93) | 50.78 (41.54) 55.00 (42.60) | 53.52 (44.96) 54.55 (45.41) | 61.33 (42.71) 65.45 (63.01) | F2.77 = 10.23 F = 0.26 F2.77 = 0.06 | 0.00 0.61 0.98 |
| Roleemotional functioning TR (n = 64) CR (n = 55) | 57.29 (42.61) 56.97 (44.75) | 65.10 (42.59) 70.30 (38.85) | 67.19 (40.93) 72.12 (41.46) | 76.56 (34.47) 78.79 (72.11) | F2.43 = 5.86 F = 0.27 F2.43 = 0.14 | 0.00 0.61 0.91 |
| Mental Health TR (n = 64) CR (n = 55) | 66.88 (22.41) 72.00 (20.22) | 76.63 (18.81) 79.93 (16.93) | 79.69 (20.51) 79.27 (18.43) | 78.38 (19.38) 81.38 (17.23) | F2.57 = 16.83 F = 0.91 F2.57 = 0.92 | 0.00 0.34 0.42 |
| Vitality TR (n = 64) CR (n = 55) | 46.64 (28.27) 52.00 (25.58) | 58.59 (25.55) 60.73 (23.64) | 60.47 (26.20) 59.73 (25.83) | 61.33 (26.71) 65.64 (23.27) | F2.46 = 18.47 F = 0.47 F2.46 = 0.90 | 0.00 0.50 0.43 |
| Pain TR (n = 64) CR (n = 55) | 59.00 (27.47) 61.84 (28.63) | 72.11 (28.79) 73.20 (26.86) | 71.08 (29.04) 77.84 (26.35) | 76.33 (27.31) 74.76 (25.21) | F2.61 = 13.90 F = 0.35 F2.61 = 0.86 | 0.00 0.56 0.45 |
| General Health TR (n = 64) CR (n = 55) | 60.75 (23.81) 65.13 (21.28) | 63.20 (25.27) 65.80 (20.50) | 64.16 (25.24) 63.95 (21.13) | 62.02 (25.24) 64.98 (22.56) | F2.80 = 0.35 F = 0.41 F2.80 = 0.71 | 0.77 0.53 0.54 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spindler, H.; Leerskov, K.; Joensson, K.; Nielsen, G.; Andreasen, J.J.; Dinesen, B. Conventional Rehabilitation Therapy Versus Telerehabilitation in Cardiac Patients: A Comparison of Motivation, Psychological Distress, and Quality of Life. Int. J. Environ. Res. Public Health 2019, 16, 512. https://doi.org/10.3390/ijerph16030512
Spindler H, Leerskov K, Joensson K, Nielsen G, Andreasen JJ, Dinesen B. Conventional Rehabilitation Therapy Versus Telerehabilitation in Cardiac Patients: A Comparison of Motivation, Psychological Distress, and Quality of Life. International Journal of Environmental Research and Public Health. 2019; 16(3):512. https://doi.org/10.3390/ijerph16030512
Chicago/Turabian StyleSpindler, Helle, Kasper Leerskov, Katrine Joensson, Gitte Nielsen, Jan Jesper Andreasen, and Birthe Dinesen. 2019. "Conventional Rehabilitation Therapy Versus Telerehabilitation in Cardiac Patients: A Comparison of Motivation, Psychological Distress, and Quality of Life" International Journal of Environmental Research and Public Health 16, no. 3: 512. https://doi.org/10.3390/ijerph16030512
APA StyleSpindler, H., Leerskov, K., Joensson, K., Nielsen, G., Andreasen, J. J., & Dinesen, B. (2019). Conventional Rehabilitation Therapy Versus Telerehabilitation in Cardiac Patients: A Comparison of Motivation, Psychological Distress, and Quality of Life. International Journal of Environmental Research and Public Health, 16(3), 512. https://doi.org/10.3390/ijerph16030512