Quality Management Systems in the Ambulant Sector: An Analytical Comparison of Different Quality Management Systems


Abstract
:1. Introduction
1.1. Background to the Study
1.2. The Aims of the Study
2. Methods
2.1. Design
- -
- DIN EN ISO 9001 (specialists/family physicians)
- -
- Quality and Development in Practices (QEP) (specialists/family physicians)
- -
- Quality management in Saxony medical practices (QisA) (specialists/family physicians)
2.2. Study Groups
2.3. Setting
2.4. Data Collection
2.5. Data Analysis
3. Results
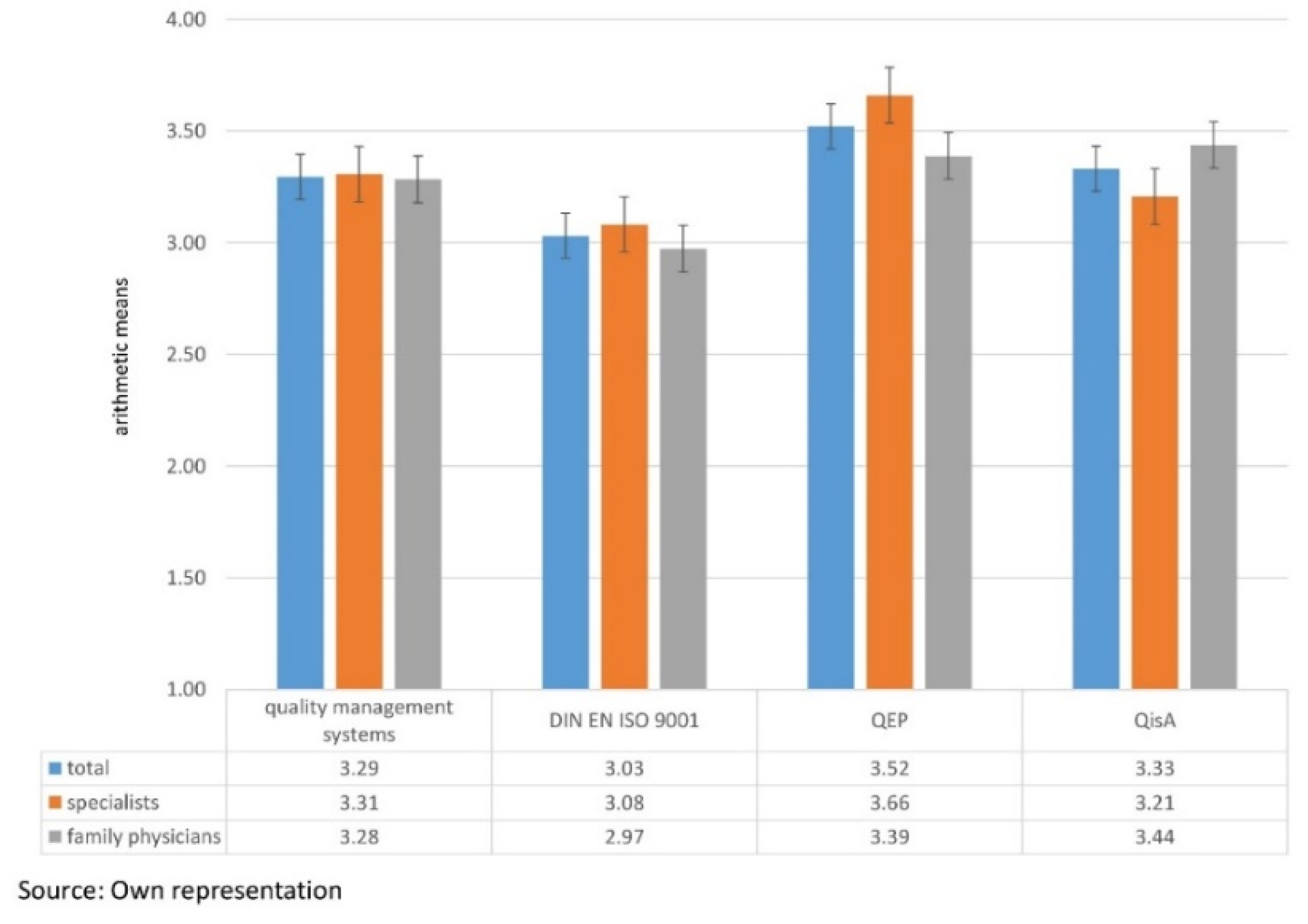
3.1. Differences in the Average Scores of the Quality Management Systems
3.2. Differences in the Average Scores of Quality Management Systems Among Specialists and Family Physicians
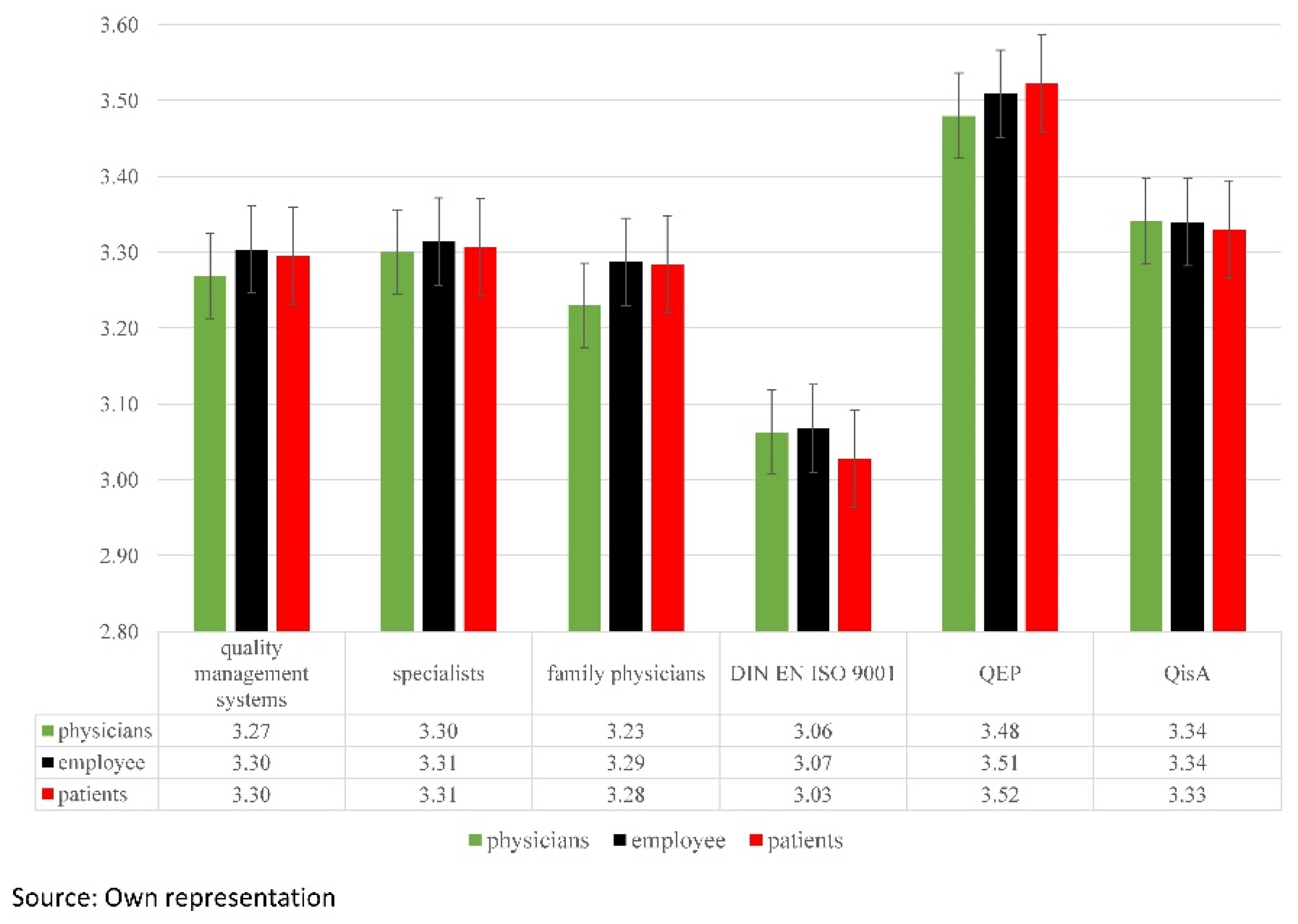
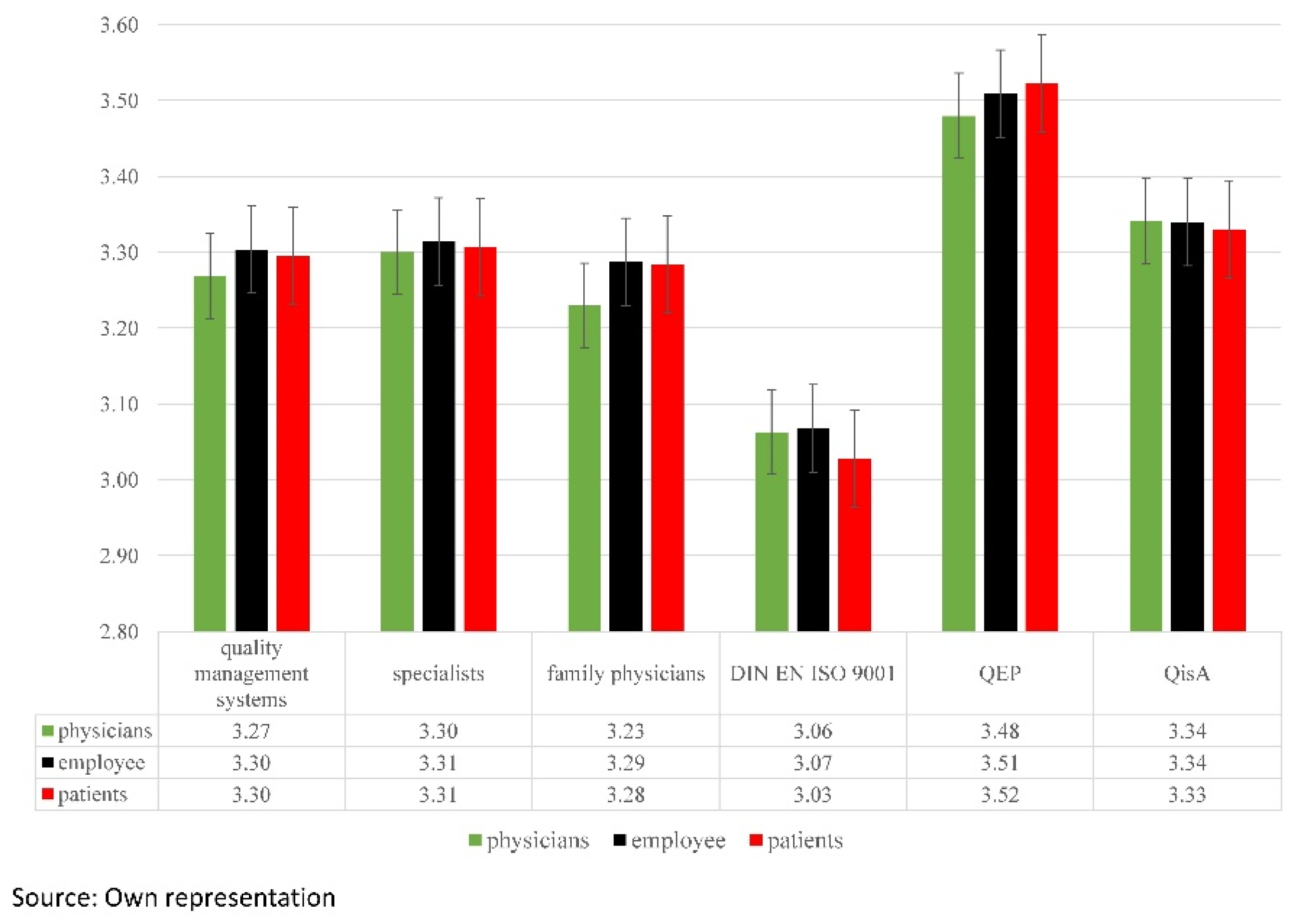
3.3. Evaluation of the Questionnaire Groups
3.4. Kruskal–Wallis Test between the Individual Quality Management Systems and Doctor Groups
4. Discussion
4.1. Representation of the Individual Quality Categories
- -
- treatment pathways and guidelines (Ø = 3.93)
- -
- disease-specific measures (Ø = 3.88)
- -
- maintenance and service (Ø = 3.83)
- -
- services and interventions (Ø = 3.88)
- -
- health promotion and prevention (Ø = 3.88)
- -
- maintaining patient records (Ø = 3.90)
- -
- confidentiality and professional secrecy (Ø = 3.86)
- -
- continuing professional development and qualification (Ø = 3.81)
- -
- infrastructure (Ø = 3.82)
- -
- procurement and storage (Ø = 3.81)
4.2. Evaluation of the Individual Quality Management Systems
4.3. Evaluation of the Individual Quality Categories
- -
- range of services
- -
- allocation of appointments
- -
- treatment pathways and guidelines
- -
- disease-specific measures
- -
- patient education
- -
- patient safety, risk- and error-management
- -
- personnel planning and employee discussions
- -
- service and maintenance
- -
- occupational safety
- -
- hygiene and cleaning
- -
- services and interventions
- -
- health promotion and prevention
- -
- telephone enquiries
- -
- external cooperation and communication
- -
- emergency management
- -
- maintaining patient records
- -
- initial patient information
- -
- confidentiality and professional secrecy
- -
- organizational structure
- -
- quality objectives
- -
- quality management-practice handbook
- -
- prescriptions
4.4. Evaluations of the Questionnaire Groups
4.5. Supporting the Physician in the Selection of a Suitable Quality Management System
4.6. Limitations of the Research
4.7. Practical Implications
4.8. Further Research Questions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Availability of Data and Material
References
- Federal Ministry of Justice and Consumer Protection. Fifth Social Security Statute Book (SGB V); Statutory Health Insurance; Federal Ministry of Justice and Consumer Protection: Berlin, Germany, 1988.
- Federal Ministry of Justice and Consumer Protection. Fifth Social Security Statute Book (SGB V); Statutory Health Insurance; Federal Ministry of Justice and Consumer Protection: Berlin, Germany, 2014.
- Joint Federal Committee. Guideline on the Basic Requirement for an Institution-Internal Quality Management for Physicians, Psychotherapists and Medical Care Centers Participating in the Contract Care. Federal Gazette, 2005. Available online: https://www.g-ba.de/downloads/62-492-864/ÄQM-RL_2014-01-23.pdf (accessed on 20 October 2018).
- Joint Federal Committee. Guideline on a Basic Requirement for the Establishment of an Internal Quality Management System for Contract Physicians, Contract Psychotherapists, Medical Care Centers, Contract Dentists and Licensed Hospitals. Federal Gazette, 2015. Available online: https://www.g-ba.de/downloads/39-261-2434/2015-12-17_2016-09-15_QM-RL_Erst-fassung_konsolidiert_BAnz.pdf (accessed on 20 October 2018).
- Adamus, W. Quality Management in Hospitals and its Role in infections Provision. In Proceedings of the International Symposium on the Analytic Hierarchy Process, Sorrento, Italy, 15–18 June 2011. [Google Scholar]
- Andres, E.; Armbruster, S.; Dannenmaler, G.; Diel, F.; Dierks, M.L.; Geraedts, M.; Gerlach, F.M.; Gibis, B.; Hollstein, D.; Johannes, H.; et al. Compendium Q-M-A—Quality Management in Ambulatory Care; Medical Center of Quality in Medicine: Berlin/Köln, Germany, 2009. [Google Scholar]
- Association of Statutory Health Insurance Physicians in Saxony. QisA—Quality [Management Systems] in Saxony Medical Practices; Quality Management; Association of Statutory Health Insurance Physicians in Saxony: Saxony, Germany, 2009. [Google Scholar]
- DIN e.V. Quality Management: QM-Systems and -Procedures. DIN Paperback; DIN e.V./Beuth Publishing House: Berlin, Germany, 2010. [Google Scholar]
- National Association of Statutory Health Insurance Physicians. QEP-Quality target catalog: Quality and development in practices, for practices, for cooperations, for MVZ. QEP—The quality management system for outpatient healthcare. In Quality and Development in Practices; Diel/Gibis, Ed.; German Medical Publishing House: Berlin, Germany, 2011. [Google Scholar]
- National Association of Statutory Health Insurance Physicians. Legal Requirements for Quality Management. 2014. Available online: http://www.kbv.de/html/7155.php (accessed on 20 October 2018).
- KTQ-GMBH. KTQ Manual including KTQ Catalog Version 2.0; Cooperation for Transparency and Quality in Health Care; Köllen Druck + Verlag GmbH.: Bonn, Germany, 2009. [Google Scholar]
- Association of Statutory Health Insurance Physicians in Westphalia-Lippe. Quality Management. KPQM. 2017. Available online: https://www.kvwl.de/arzt/qsqm/management/ (accessed on 20 October 2018).
- AQUA. EPA—That Is Quality Management in a New Dimension. Institute for Applied Quality Assurance and Research in Health Care GmbH: Göttingen, 2014. Available online: https://www.epa-qm.de//epa/ (accessed on 20 October 2018).
- European Foundation for Quality Management. Total-Quality-Management. 1988. Available online: http://www.efqm.org/efqm-model/ (accessed on 20 October 2018).
- Kiess, W. Quality Management in Outpatient Pediatric Care. Vision and Utopia of Flawless Medicine. Pediatrics 2018. [Google Scholar] [CrossRef]
- Kühlein, T.; Madlo-Thiess, F.; Wambach, V.; Schaffer, S. Ten Years of Quality Management: Perception and Significance from the Point of View of General Practitioners in a Network of Doctors; Health Care Issue 80(03); Georg Thieme Publishing KG: Stuttgart, Germany; New York, NY, USA, 2018. [Google Scholar]
- Sieger, S. First DIN EN Set of Rules for Health Care Services. Risk Management and Error Prevention in Hospitals; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Chiarini, A.; Baccarani, C. TQM and lean strategy deployment in Italian hospitals: Benefits related to patient satisfaction and encountered pitfalls. Leadership Health Serv. 2016, 29, 377–391. [Google Scholar] [CrossRef] [PubMed]
- Manzanera, R.; Moya, D.; Guilabert, M.; Plana, M.; Gálvez, G.; Ortner, J.; Mira, J. Quality Assurance and Patient Safety Measures: A Comparative Longitudinal Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1568. [Google Scholar] [CrossRef] [PubMed]
- Tzelepis, F.; Clinton-McHarg, T.; Paul, C.L.; Sanson-Fisher, R.W.; Joshua, D.; Carey, M.L. Quality of Patient-Centered Care Provided to Patients Attending Hematological Cancer Treatment Centers. Int. J. Environ. Res. Public Health 2018, 15, 549. [Google Scholar] [CrossRef] [PubMed]
- Eichhorn, L.; Murday, A.K.; Kohnen, B.; Guttenthaler, V.; Türler, A.; Baumgarten, G.; Wittmann, M. Patient Satisfaction as a Measure of Quality Management—A Comparison between a University Hospital and a Standard Care Hospital; Gesundheitswesen [Health Care] Issue 79(08/09); Georg Thieme Publishing KG: Stuttgart, Germany; New York, NY, USA, 2017. [Google Scholar]
- Kuntsche, P.; Börchers, K. Integrated Management Systems. Quality and Risk Management in Healthcare; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Xyländer, M.; Meyer, T. Quality development in health organizations using the example of medical rehabilitation with a special focus on the quality of results and the role of the professions. In Professional Quality Development in Interdisciplinary Health Care; Springer: Wiesbaden, Germany, 2017. [Google Scholar]
- Federal Chamber of Physicians. (Pattern-)Guidelines on the Content of Continuing Education. Version: 07.04.1994; Federal Chamber of Physicians: Berlin, Germany, 1994.
- Federal Chamber of Physicians. (Pattern-)Guidelines. Version: 23.10.2015; Federal Chamber of Physicians: Berlin, Germany, 2015.
- Federal Ministry of Justice. Law on Medical Devices (Medical Devices Act—MPG). Adoption: 02.08.1994; Federal Ministry of Justice: Berlin, Germany, 1994.
- MacCallum, R.C.; Widaman, K.F.; Zhang, S.; Hong, S. Sample size in factor analysis. Psychol. Methods 1999, 4, 84–99. [Google Scholar] [CrossRef]
- Mundform, D.J.; Shaw, D.G.; Ke, T.L. Minimum sample size recommendations for conducting factor analysis. Int. J. Test. 2005, 5, 159–168. [Google Scholar] [CrossRef]
- Weiß, C. Basic Knowledge of Medical Statistics, 6th ed.; Weiß, C., Ed.; Springer: Berlin, Germany, 2013. [Google Scholar]
- Schüller, A.M.; Dumont, M. The Successful Medical Practice; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Beyer, M.; Dovey, S.; Gerlach, F.M. Error in general practice: Results oft he international PCISME-study in Germany. J. Gen. Med. 2003, 79, 327–331. [Google Scholar]
- Schillinger, D.; Piette, J.; Grumbach, K.; Wang, F.; Wilson, C.; Daher, C.; Leong-Grotz, K.; Castro, C.; Bindman, A.B. Closing the loop: Physician communication with diabetic patients who have low healthy literacy. Arch. Intern. Med. 2003, 163, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Szecsenyi, J.; Klingenberg, A.; Magdeburg, K. Evaluation oft he patient book oft he medical quality community Ried by general practitioners. J. Med. Educ. Qual. Health Care 2002, 78, 403–407. [Google Scholar]
- Beske, F.; Ratschko, K.W. The GKV-Modernization Act—GMG and Ist Effects: A Critical Analysis; German Medical Publishing House: Berlin, Germany, 2006. [Google Scholar]
- Kohn, L.T.; Corrigan, J.M.; Donaldson, M.S. To Error is Human: Building a Safer Health System; The National Academies Press: Washington, DC, USA, 1999. [Google Scholar]
- Abdi, H. Bonferroni and Sidak corrections for multiple comparisons. In Encyclopedia of Measurement and Statistics; Salkind, N.J., Ed.; Sage: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Holm, S. A simple sequentially rejective multiple test procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- IBM. PASW Statistics Version 18.0.0; PASW (Predictive Analysis SoftWare); SPSS Inc.: Chicago, IL, USA, 2009; Available online: https://www.ibm.com/analytics/us/en/technology/spss/ (accessed on 2 April 2017).
- Kruskal, W.H.; Wallis, W.A. Use of ranks in one-criterion variance analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]
- Mack, H.B.; Wolfe, D.A. K-sample rank tests for umbrella alternatives. J. Am. Stat. Assoc. 1981, 76, 175–181. [Google Scholar]
- Montgomery, D.C. Design and Analysis of Experiments; John Wiley and Sons: London, UK, 2005. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: New Jersey, NY, USA, 1988. [Google Scholar]
- Cohen, B. Explaining Psychological Statistics, 3rd ed.; John Wiley & Sons: London, UK, 2008. [Google Scholar]
- Fritz, C.O.; Morris, P.E.; Richler, J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Baiker, K.; Chandra, A. Medicare Spending, The Physician Workforce, and Beneficiaries Quality of Care. Health Aff. 2004. [Google Scholar] [CrossRef] [PubMed]
- Editorial Office Health. Regional Homestay Models in Germany—Research of the Editorial Office Health at the Federal Associations of Health Insurances and Associations of Statutory Health Insurances Physicians. 2006. Available online: www.die-gesundheitsreform.de/zukunft_entwickeln/hausarztmodell/beispiele/pdf/uebersicht_hausarztmodelle_deutschland.pdf (accessed on 20 October 2018).

{kind=link}
{kind=link}
| Quality Categories | Content of the Questionnaires |
|---|---|
| range of services | The practises detail their specific “range of services”. This is determined by their specialist status, their focus and special features of their practise [30]. |
| allocation of appointments | According to § 17 Section 1 Federal Master Treaty, the physicians must offer sufficient working hours for appointments (at least 20 hours per week) [9]. |
| telephone enquiries | The employees must know which patient enquiries may be answered by the physician or the personnel. |
| treatment pathways and guidelines | The “treatment pathways and guidelines” should be tools to support decisions that objectify and systematize the diagnostic and therapeutic questions [31]. |
| disease-specific measures | In complex medical discussions, it is useful to support the patient with written documents. Information may be offered during the treatment or in the waiting room for this purpose [32,33]. |
| external cooperation and communication | The family physician plays a coordinating role between the specialists in the treatment of the patient [9]. |
| emergency management | Patients with health-related disorders must be identified and treated quickly [9]. |
| maintaining patient records | Each patient record must have a clear structure. It must reveal the most important data about the patient [9]. |
| patient education | This category investigates how the patient is educated about medical measures [9]. |
| initial patient information | The patient record must not contain any discriminatory remarks about the “initial patient information” [34]. |
| patient safety, risk- and error-management | Drugs are prescribed in medical practises, diagnostic investigations are performed and basic medical tasks are delegated [9,35]. |
| confidentiality and professional secrecy | Due to the sensitive situation of the patient, their privacy must be maintained at all times. |
| personnel planning and employee discussions | Practice employees should be assigned clearly defined tasks. |
| continuous professional development and qualification | Targeted continuous professional development and training for the practise employees promotes improvement to procedures and processes. |
| organizational structure | The quality management guideline describes the “organizational structure” [9]. |
| infrastructure | It is mandatory that medical practises are accessible to patients with walking aids or wheelchairs. On the other hand, access options for buggies are recommended for paediatric practises [9]. |
| service and maintenance | It should be ensured that technical equipment is used by qualified personnel. Physicians and employees are supported in the handling of the equipment by operating instructions [9,26]. |
| occupational safety | The practise management must create a safe working environment for patients and employees [9]. |
| hygiene and cleaning | The guidelines must be used for the implementation of the hygiene specifications [9]. |
| quality management system | A systematic system is important for the many different procedures and processes in a practise [9]. |
| quality objectives | “Quality objectives” can be classified into primary, qualitative and quantitative objectives. |
| quality management-practise handbook | The practise handbook should define in writing the rules of the practise and quality-relevant aspects, such as treatment paths. The handbook should be published so that the patient can submit an assessment for the practise. |
| prescriptions | “Prescriptions” must always be filled correctly [31]. |
| services and interventions | Certain services require that the physicians and employees fulfil certain quality requirements. |
| health promotion and prevention | Preventive measures promote the early detection and treatment of diseases. |
| procurement and storage | There are many suppliers where practises can purchase consumables and drugs. Selection criteria may be the price or the reliability [9]. |
| Fragenkomplex | DIN EN ISO 9001 | QEP | QisA | DIN EN ISO 9001 | QEP | QisA | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Specialists | Family Physicians | Specialists | Family Physicians | Specialists | Family Physicians | |||||
| range of services | 2.90 | 3.43 | 3.07 | 3.08 | 2.69 | 3.79 | 3.08 | 3.09 | 3.06 | |
| allocation of appointments | 2.73 | 3.39 | 3.03 | 2.80 | 2.65 | 3.69 | 3.11 | 3.07 | 3.00 | |
| telephone enquiries | 2.64 | 3.54 | 3.40 | 2.59 | 2.70 | 3.52 | 3.56 | 2.94 | 3.80 | |
| treatment pathways and guidelines | 3.07 | 3.61 | 3.20 | 3.09 | 3.04 | 3.93 | 3.30 | 3.31 | 3.10 | |
| disease-specific measures | 2.87 | 3.49 | 3.13 | 3.01 | 2.70 | 3.88 | 3.11 | 3.28 | 3.00 | |
| external cooperation and communication | 3.29 | 3.68 | 3.63 | 3.25 | 3.33 | 3.62 | 3.73 | 3.42 | 3.80 | |
| emergency management | 3.15 | 3.54 | 3.50 | 3.05 | 3.26 | 3.52 | 3.57 | 3.14 | 3.80 | |
| maintaining patient records | 3.26 | 3.76 | 3.68 | 3.22 | 3.32 | 3.72 | 3.79 | 3.42 | 3.90 | |
| patient education | 2.86 | 3.37 | 3.07 | 2.97 | 2.73 | 3.68 | 3.08 | 3.13 | 3.02 | |
| initial patient information | 2.97 | 3.56 | 3.45 | 2.94 | 3.00 | 3.51 | 3.61 | 3.06 | 3.77 | |
| patient safety, risk- and error-management | 3.15 | 3.47 | 3.27 | 3.25 | 3.05 | 3.65 | 3.29 | 3.34 | 3.22 | |
| confidentialy and professional secrecy | 3.30 | 3.74 | 3.72 | 3.29 | 3.30 | 3.71 | 3.77 | 3.55 | 3.86 | |
| personnel planning and employee discussions | 2.81 | 3.32 | 3.12 | 2.89 | 2.60 | 3.56 | 3.06 | 3.23 | 3.00 | |
| continuous professional development and qualification | 3.46 | 3.49 | 3.47 | 3.81 | 2.50 | 3.64 | 3.31 | 3.47 | 3.47 | |
| organizational structure | 3.24 | 3.61 | 3.55 | 3.22 | 3.26 | 3.59 | 3.63 | 3.25 | 3.80 | |
| infrastructure | 3.43 | 3.60 | 3.47 | 3.82 | 2.99 | 3.71 | 3.49 | 3.50 | 3.43 | |
| service and maintenance | 3.04 | 3.43 | 3.26 | 3.09 | 2.99 | 3.83 | 3.06 | 3.27 | 3.25 | |
| occupational safety | 2.89 | 3.48 | 3.21 | 2.94 | 2.83 | 3.78 | 3.20 | 3.22 | 3.20 | |
| hygiene and cleaning | 3.18 | 3.56 | 3.48 | 3.24 | 3.00 | 3.78 | 3.31 | 3.50 | 3.47 | |
| quality management system | 2.68 | 3.18 | 3.17 | 2.56 | 3.00 | 3.06 | 3.31 | 3.07 | 3.27 | |
| quality objectives | 2.86 | 3.32 | 3.30 | 2.81 | 3.00 | 3.22 | 3.44 | 2.80 | 3.80 | |
| quality management-practise handbook | 2.75 | 3.30 | 3.27 | 2.68 | 2.83 | 3.10 | 3.49 | 2.70 | 3.75 | |
| prescriptions | 3.07 | 3.39 | 3.37 | 3.03 | 3.12 | 3.25 | 3.53 | 2.97 | 3.71 | |
| services and interventions | 2.98 | 3.55 | 3.23 | 3.11 | 2.84 | 3.88 | 3.24 | 3.24 | 3.21 | |
| health promotion and prevention | 3.01 | 3.52 | 3.14 | 3.10 | 2.90 | 3.88 | 3.17 | 3.19 | 3.10 | |
| procurement and storage | 3.38 | 3.50 | 3.42 | 3.81 | 2.20 | 3.67 | 3.31 | 3.43 | 3.40 | |
| Questions | Mean Rank Sum | Chi-Squared | [Df] | Asymptotic Significance | Effect Size According to H2 | Effect Size According to Cohen’s d | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| DIN Specialists | DIN Family Physicians | QEP Specialists | QEP Family Physicians | QisA Specialists | QisA Family Physicians | ||||||
| range of service | 783.99 | 444.61 | 1389.70 | 753.70 | 834.54 | 744.49 | 595.7080 | 5.00 | <0.000001 | 0.390 | 1.492 |
| allocation of appointments | 654.13 | 589.99 | 1222.88 | 846.82 | 863.99 | 778.58 | 348.5896 | 5.00 | <0.000001 | 0.208 | 1.025 |
| telephone enquiries | 461.32 | 525.03 | 1,011.20 | 1033.89 | 657.91 | 1191.81 | 665.7452 | 5.00 | <0.000001 | 0.400 | 1.633 |
| treatment pathways and guidelines | 669.65 | 620.41 | 1347.59 | 839.18 | 844.61 | 661.58 | 458.6346 | 5.00 | <0.000001 | 0.290 | 1.231 |
| disease-specific measures | 685.19 | 459.40 | 1424.28 | 786.37 | 932.90 | 682.40 | 653.1031 | 5.00 | <0.000001 | 0.446 | 1.607 |
| external cooperation and communication | 535.66 | 595.27 | 907.76 | 1029.09 | 719.64 | 1105.46 | 379.3159 | 5.00 | <0.000001 | 0.227 | 1.083 |
| emergency management | 510.12 | 692.06 | 929.11 | 974.22 | 607.90 | 1177.00 | 439.7436 | 5.00 | <0.000001 | 0.263 | 1.195 |
| maintaining patient records | 557.46 | 666.21 | 912.89 | 994.31 | 722.56 | 1052.85 | 338.7056 | 5.00 | <0.000001 | 0.202 | 1.006 |
| patient education | 682.71 | 598.29 | 1300.85 | 814.24 | 845.78 | 726.17 | 365.5875 | 5.00 | <0.000001 | 0.218 | 1.057 |
| initial patient information | 487.72 | 511.60 | 996.02 | 1077.24 | 591.19 | 1211.16 | 690.1791 | 5.00 | <0.000001 | 0.415 | 1.684 |
| patient safety, risk- and error-management | 775.39 | 646.65 | 1,130.37 | 792.82 | 847.23 | 761.64 | 163.2550 | 5.00 | <0.000001 | 0.180 | 0.651 |
| confidentialy and professional secrecy | 634.01 | 645.21 | 894.53 | 937.65 | 790.22 | 1006.79 | 211.1905 | 5.00 | <0.000001 | 0.140 | 0.755 |
| personnel planning and employee discussions | 44.15 | 36.20 | 68.67 | 49.94 | 56.07 | 48.07 | 12.9925 | 5.00 | <0.000001 | 0.136 | 0.568 |
| continuous professional development and qualification | 64,07 | 20.35 | 57.72 | 44.22 | 49.83 | 48.23 | 23.5778 | 5.00 | <0.000001 | 0.272 | 0.917 |
| organizational structure | 656.20 | 692.80 | 901.90 | 930.22 | 665.62 | 1056.30 | 226.2623 | 5.00 | <0.000001 | 0.140 | 0.787 |
| infrastructure | 1028.68 | 551.02 | 954.15 | 827.57 | 829.84 | 740.13 | 214.7406 | 5.00 | <0.000001 | 0.150 | 0.763 |
| service and maintenance | 712.82 | 650.59 | 1228.99 | 711.75 | 829.42 | 816.99 | 292.7535 | 5.00 | <0.000001 | 0.180 | 0.919 |
| occupational safety | 663.90 | 634.26 | 1186.41 | 793.56 | 845.51 | 826.22 | 261.3655 | 5.00 | <0.000001 | 0.155 | 0.857 |
| hygiene and cleaning | 42.67 | 38.90 | 67.67 | 47.19 | 54.70 | 54.43 | 12.9622 | 5.00 | <0.000001 | 0.138 | 0.567 |
| quality management system | 34.13 | 51.20 | 53.17 | 64.75 | 53.70 | 61.27 | 17.5136 | 5.00 | 0.003622 | 0.158 | 0.788 |
| quality objectives | 38.94 | 46.00 | 50.33 | 63.03 | 39.57 | 75.43 | 23.9098 | 5.00 | <0.000001 | 0.192 | 0.927 |
| quality management-practice handbook | 535.23 | 617.64 | 765.84 | 979.35 | 537.39 | 1,129.99 | 484.3620 | 5.00 | <0.000001 | 0.309 | 1.338 |
| prescriptions | 623.86 | 690.57 | 773.08 | 996.01 | 648.26 | 1,150.81 | 312.9589 | 5.00 | <0.000001 | 0.186 | 0.957 |
| services and interventions | 709.44 | 581.24 | 1276.66 | 824.84 | 795.30 | 769.74 | 349.3415 | 5.00 | <0.000001 | 0.208 | 1.026 |
| health promotion and prevention | 721.03 | 625.53 | 1338.52 | 814.92 | 787.17 | 689.05 | 402.2985 | 5.00 | <0.000001 | 0.240 | 1.125 |
| procurement and storage | 64.57 | 22.50 | 57.83 | 43.28 | 47.57 | 49.03 | 22.5309 | 5.00 | <0.000001 | 0.336 | 0.885 |
| total | 13,441.82 | 12,450.07 | 22,192.06 | 18,011.62 | 15,382.59 | 18,563.25 | 4130.8390 | 5.00 | <0.000001 | 0.125 | 0.750 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gumpert, M.; Reese, J.-P. Quality Management Systems in the Ambulant Sector: An Analytical Comparison of Different Quality Management Systems. Int. J. Environ. Res. Public Health 2019, 16, 444. https://doi.org/10.3390/ijerph16030444
Gumpert M, Reese J-P. Quality Management Systems in the Ambulant Sector: An Analytical Comparison of Different Quality Management Systems. International Journal of Environmental Research and Public Health. 2019; 16(3):444. https://doi.org/10.3390/ijerph16030444
Chicago/Turabian StyleGumpert, Marcus, and Jens-Peter Reese. 2019. "Quality Management Systems in the Ambulant Sector: An Analytical Comparison of Different Quality Management Systems" International Journal of Environmental Research and Public Health 16, no. 3: 444. https://doi.org/10.3390/ijerph16030444
APA StyleGumpert, M., & Reese, J.-P. (2019). Quality Management Systems in the Ambulant Sector: An Analytical Comparison of Different Quality Management Systems. International Journal of Environmental Research and Public Health, 16(3), 444. https://doi.org/10.3390/ijerph16030444