Long-Term Attitude Change After a Single-Day Manager Training Addressing Mental Health at the Workplace

 ,
,
Abstract
1. Introduction
2. Materials and Methods
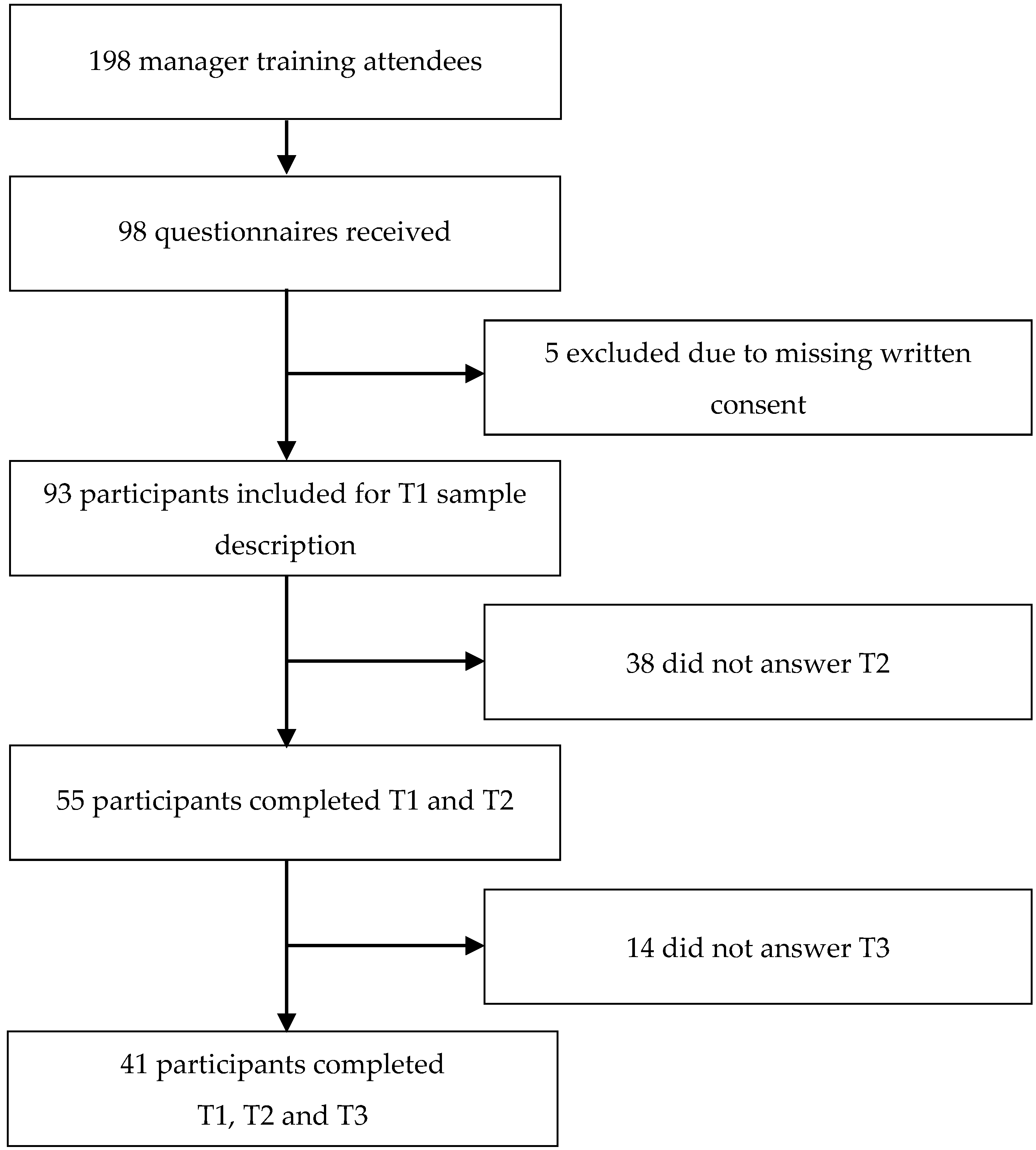
2.1. Sample
2.2. Manager Training
2.3. Quantitative Instruments
2.4. Qualitative Instruments
2.5. Implementation
2.6. Design and Data Analysis
2.7. Ethical Approval and Registration
3. Results
3.1. Descriptives
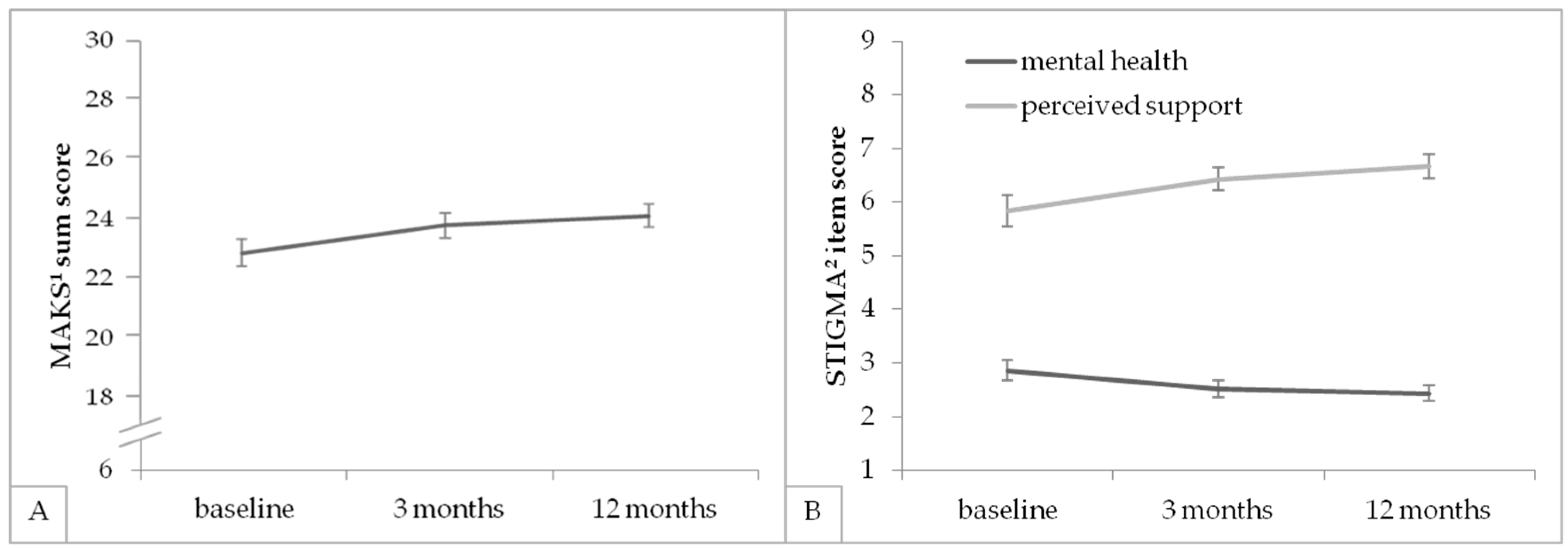
3.2. Knowledge and Attitudes Concerning Mental Health
3.3. Working Situation
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Stigma-Related Single Items (STIGMA)
| How do you think about yourself and your psychological condition? | label |
| 1. From a psychological point, I am entirely healthy. | mh |
| 2. Would you feel embarrassed if being affected by a mental health problem (e.g., depressive disorder, anxiety disorder, alcohol addiction)? | shames |
| 3. Would you feel embarrassed if somebody of your family would be affected by a mental health problem (e.g., depressive disorder, anxiety disorder, alcohol addiction)? | Shameo |
| How are employees with mental health problems treated at your company? | |
| 4. Colleagues with mental health problems are supported by colleagues and supervisors and treated fairly. | support |
| 5. Personally, I avoid dealing with colleagues with mental health problems, if possible. | sd |
| 6. If I would have mental health problems, I would tell colleagues and supervisors at the workplace. | inf |
References
- Boysen, E.; Schiller, B.; Mörtl, K.; Gündel, H.; Hölzer, M. Preliminary Analyses Showed Short-Term Mental Health Improvements after a Single-Day Manager Training. Int. J. Environ. Res. Public 2018, 15, 108. [Google Scholar] [CrossRef] [PubMed]
- Wittchen, H.-U.; Jacobi, F.; Rehm, J.; Gustavsson, A.; Svensson, M.; Jönsson, B.; Olesen, J.; Allgulander, C.; Alonso, J.; Faravelli, C. The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 2011, 21, 655–679. [Google Scholar] [CrossRef] [PubMed]
- Marschall, J.; Hildebrandt, S.; Nolting, H.-D.; Burgart, E.; Heil, K.L.; Tisch, T.; Woköck, T. Gesundheitsreport 2019. Available online: https://www.dak.de/dak/bundesthemen/gesundheitsreport-2019-2099306.html (accessed on 20 October 2019).
- Andrade, L.H.; Alonso, J.; Mneimneh, Z.; Wells, J.; Al-Hamzawi, A.; Borges, G.; Bromet, E.; Bruffaerts, R.; De Girolamo, G.; De Graaf, R. Barriers to mental health treatment: Results from the WHO World Mental Health surveys. Psychol. Med. 2014, 44, 1303–1317. [Google Scholar] [CrossRef] [PubMed]
- Haugen, P.T.; McCrillis, A.M.; Smid, G.E.; Nijdam, M.J. Mental health stigma and barriers to mental health care for first responders: A systematic review and meta-analysis. J. Psychiatr. Res. 2017, 94, 218–229. [Google Scholar] [CrossRef]
- Wu, I.H.; Bathje, G.J.; Kalibatseva, Z.; Sung, D.; Leong, F.T.; Collins-Eaglin, J. Stigma, mental health, and counseling service use: A person-centered approach to mental health stigma profiles. Psychol. Serv. 2017, 14, 490. [Google Scholar] [CrossRef]
- Schütte, M.; Windel, A. Psychische Gesundheit in der Arbeitswelt-Wissenschaftliche Standortbestimmung. Z. Arb. 2017, 71, 1–5. [Google Scholar] [CrossRef][Green Version]
- Cottini, E.; Lucifora, C. Mental health and working conditions in Europe. Ind. Labor Relat. Rev. 2013, 66, 958–988. [Google Scholar] [CrossRef]
- Harvey, S.B.; Modini, M.; Joyce, S.; Milligan-Saville, J.S.; Tan, L.; Mykletun, A.; Bryant, R.A.; Christensen, H.; Mitchell, P.B. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup. Environ. Med. 2017, 74, 301–310. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, K.; Bruinvels, D.; Frings-Dresen, M. Psychosocial work environment and stress-related disorders, a systematic review. Occup. Med. 2010, 60, 277–286. [Google Scholar] [CrossRef]
- Stansfeld, S.; Candy, B. Psychosocial work environment and mental health—A meta-analytic review. Scand. J. Work Environ. Health 2006, 32, 443–462. [Google Scholar] [CrossRef]
- Theorell, T.; Hammarström, A.; Aronsson, G.; Bendz, L.T.; Grape, T.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Hall, C. A systematic review including meta-analysis of work environment and depressive symptoms. BMC Public Health 2015, 15, 738. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.; Roesler, U.; Kusserow, T.; Rau, R. Uncertainty in the workplace: Examining role ambiguity and role conflict, and their link to depression—A meta-analysis. Eur. J. Work Organ. Psychol. 2014, 23, 91–106. [Google Scholar] [CrossRef]
- Virtanen, M.; Kivimäki, M.; Joensuu, M.; Virtanen, P.; Elovainio, M.; Vahtera, J. Temporary employment and health: A review. Int. J. Epidemiol. 2005, 34, 610–622. [Google Scholar] [CrossRef] [PubMed]
- Netterstrøm, B.; Conrad, N.; Bech, P.; Fink, P.; Olsen, O.; Rugulies, R.; Stansfeld, S. The relation between work-related psychosocial factors and the development of depression. Epidemiol. Rev. 2008, 30, 118–132. [Google Scholar] [CrossRef] [PubMed]
- Verkuil, B.; Atasayi, S.; Molendijk, M.L. Workplace bullying and mental health: A meta-analysis on cross-sectional and longitudinal data. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Modini, M.; Joyce, S.; Mykletun, A.; Christensen, H.; Bryant, R.A.; Mitchell, P.B.; Harvey, S.B. The mental health benefits of employment: Results of a systematic meta-review. Australas. Psychiatry 2016, 24, 331–336. [Google Scholar] [CrossRef]
- McKee-Ryan, F.; Song, Z.; Wanberg, C.R.; Kinicki, A.J. Psychological and physical well-being during unemployment: A meta-analytic study. J. Appl. Psychol. 2005, 90, 53. [Google Scholar] [CrossRef]
- Jin, R.L.; Shah, C.P.; Svoboda, T.J. The impact of unemployment on health: A review of the evidence. Can. Med. Assoc. J. 1997, 18, 275–301. [Google Scholar] [CrossRef]
- Fossey, E.M.; Harvey, C.A. Finding and sustaining employment: A qualitative meta-synthesis of mental health consumer views. Can. J. Occup. Ther. 2010, 77, 303–314. [Google Scholar] [CrossRef]
- Mor Barak, M.E.; Travis, D.J.; Pyun, H.; Xie, B. The impact of supervision on worker outcomes: A meta-analysis. Soc. Serv. Rev. 2009, 83, 3–32. [Google Scholar] [CrossRef]
- Kuehnl, A.; Seubert, C.; Rehfuess, E.; von Elm, E.; Nowak, D.; Glaser, J. Human resource management training of supervisors for improving health and well-being of employees. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef] [PubMed]
- McGorry, P.D.; Ratheesh, A.; O’Donoghue, B. Early Intervention—An implementation challenge for 21st century mental health care. JAMA Psychiatry 2018, 75, 545–546. [Google Scholar] [CrossRef] [PubMed]
- Furlan, A.D.; Gnam, W.H.; Carnide, N.; Irvin, E.; Amick, B.C.; DeRango, K.; McMaster, R.; Cullen, K.; Slack, T.; Brouwer, S. Systematic review of intervention practices for depression in the workplace. J. Occup. Rehabil. 2012, 22, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Joyce, S.; Modini, M.; Christensen, H.; Mykletun, A.; Bryant, R.; Mitchell, P.B.; Harvey, S.B. Workplace interventions for common mental disorders: A systematic meta-review. Psychol. Med. 2016, 46, 683–697. [Google Scholar] [CrossRef]
- Pomaki, G.; Franche, R.-L.; Murray, E.; Khushrushahi, N.; Lampinen, T.M. Workplace-based work disability prevention interventions for workers with common mental health conditions: A review of the literature. J. Occup. Rehabil. 2012, 22, 182–195. [Google Scholar] [CrossRef]
- Yunus, W.M.A.W.M.; Musiat, P.; Brown, J.S. Systematic review of universal and targeted workplace interventions for depression. Occup. Environ. Med. 2018, 75, 66–75. [Google Scholar] [CrossRef]
- Holman, D.; Johnson, S.; O’Connor, E. Stress management interventions: Improving subjective psychological well-being in the workplace. In Handbook of Well-Being; Diener, E., Oishi, S., Tay, L., Eds.; DEF Publishers: Salt Lake City, UT, USA, 2018. [Google Scholar]
- Richardson, K.M.; Rothstein, H.R. Effects of occupational stress management intervention programs: A meta-analysis. J. Occup. Health Psychol. 2008, 13, 69. [Google Scholar] [CrossRef]
- Dobson, K.S.; Szeto, A.; Knaak, S. The Working Mind: A meta-analysis of a workplace mental health and stigma reduction program. Can. J. Psychiatry 2019. [Google Scholar] [CrossRef]
- Dobson, K.S.; Szeto, A.; Knaak, S.; Krupa, T.; Kirsh, B.; Luong, D.; McLean, R.; Pietrus, M. Mental health initiatives in the workplace: Models, methods and results from the Mental Health Commission of Canada. World Psychiatry 2018, 17, 370. [Google Scholar] [CrossRef]
- Montano, D.; Reeske, A.; Franke, F.; Hüffmeier, J. Leadership, followers’ mental health and job performance in organizations: A comprehensive meta-analysis from an occupational health perspective. J. Organ. Behav. 2017, 38, 327–350. [Google Scholar] [CrossRef]
- Gayed, A.; Milligan-Saville, J.S.; Nicholas, J.; Bryan, B.T.; LaMontagne, A.D.; Milner, A.; Madan, I.; Calvo, R.A.; Christensen, H.; Mykletun, A. Effectiveness of training workplace managers to understand and support the mental health needs of employees: A systematic review and meta-analysis. Occup. Environ. Med. 2018, 75, 462–470. [Google Scholar] [CrossRef]
- Milligan-Saville, J.S.; Tan, L.; Gayed, A.; Barnes, C.; Madan, I.; Dobson, M.; Bryant, R.A.; Christensen, H.; Mykletun, A.; Harvey, S.B. Workplace mental health training for managers and its effect on sick leave in employees: A cluster randomised controlled trial. Lancet 2017, 4, 850–858. [Google Scholar] [CrossRef]
- Britt, T.W.; Wright, K.M.; Moore, D. Leadership as a predictor of stigma and practical barriers toward receiving mental health treatment: A multilevel approach. Psychol. Serv. 2012, 9, 26. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumi, A. Development of an evidence-based guideline for supervisor training in promoting mental health: Literature review. J. Occup. Health 2011, 53, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Angerer, P.; Rothermund, E.; Limm, H.; Heinmüller, M.; Marten-Mittag, B.; Nater, U.M.; Gündel, H. Stressbewältigungsintervention am Arbeitsplatz. Psychotherapeut 2011, 56, 34–39. [Google Scholar] [CrossRef]
- Siegrist, K.; Silberhorn, T. Stressabbau in Organisationen-Ein Manual Zum Stressmanagement; LIT Verlag Münster: Berlin, Germany, 1998. [Google Scholar]
- Evans-Lacko, S.; Little, K.; Meltzer, H.; Rose, D.; Rhydderch, D.; Henderson, C.; Thornicroft, G. Development and psychometric properties of the mental health knowledge schedule. Can. J. Psychiatry 2010, 55, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Link, B.G.; Phelan, J.C.; Bresnahan, M.; Stueve, A.; Pescosolido, B.A. Public conceptions of mental illness: Labels, causes, dangerousness, and social distance. AJPH 1999, 89, 1328–1333. [Google Scholar] [CrossRef]
- Bogardus, E.S. Social distance and its origins. J. Appl. Sociol. 1925, 9, 216–226. [Google Scholar]
- Marie, D.; Miles, B. Social distance and perceived dangerousness across four diagnostic categories of mental disorder. Aust. N. Z. J. Psychiatry 2008, 42, 126–133. [Google Scholar] [CrossRef]
- Morfeld, M.; Stritter, W.; Bullinger, M. Der SF-36 Health Survey. In Gesundheitsökonomische Evaluationen; Springer: Berlin/Heidelberg, Germany, 2012; pp. 393–410. [Google Scholar]
- Löwe, B.; Spitzer, R.L.; Zipfel, S.; Herzog, W. Gesundheitsfragebogen für Patienten (PHQ-D). Manual und Testunterlagen (2. Auflage); Pfizer: Karlsruhe, Germany, 2002. [Google Scholar]
- Löwe, B.; Spitzer, R.; Zipfel, S.; Herzog, W. Manual (Komplettversion und Kurzform): Autorisierte Deutsche Version des Prime MD Patient Health Questionnaire (PHQ); Pfizer: Karlsruhe, Germany, 2002. [Google Scholar]
- Rödel, A.; Siegrist, J.; Hessel, A.; Brähler, E. Fragebogen zur Messung beruflicher Gratifikationskrisen. Z. Diff. Diag. Psych. 2004, 25, 227–238. [Google Scholar] [CrossRef]
- Mohr, G.; Rigotti, T.; Müller, A. Irritation-ein instrument zur Erfassung psychischer Beanspruchung im arbeitskontext. Skalen-und itemparameter aus 15 Studien. Z. Arb. Org. Psych. 2005, 49, 44–48. [Google Scholar] [CrossRef]
- Siegrist, J.; Starke, D.; Chandola, T.; Godin, I.; Marmot, M.; Niedhammer, I.; Peter, R. The measurement of effort-reward imbalance at work: European comparisons. Soc. Sci. Med. 2004, 58, 1483–1499. [Google Scholar] [CrossRef]
- Wark, C.; Galliher, J.F. Emory Bogardus and the origins of the social distance scale. Am. Sociol. 2007, 38, 383–395. [Google Scholar] [CrossRef]
- Moxham, L.; Taylor, E.; Patterson, C.; Perlman, D.; Brighton, R.; Sumskis, S.; Keough, E.; Heffernan, T. Can a clinical placement influence stigma? An analysis of measures of social distance. Nurse Educ. Today 2016, 44, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Limm, H.; Gündel, H.; Heinmüller, M.; Marten-Mittag, B.; Nater, U.M.; Siegrist, J.; Angerer, P. Stress management interventions in the workplace improve stress reactivity: A randomised controlled trial. Occup. Environ. Med. 2011, 68, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Herr, R.; Barrech, A.; Riedel, N.; Gündel, H.; Angerer, P.; Li, J. Long-term effectiveness of stress management at work: Effects of the changes in perceived stress reactivity on mental health and sleep problems seven years later. Int. J. Environ. Res. Public 2018, 15, 255. [Google Scholar] [CrossRef]
- Li, J.; Riedel, N.; Barrech, A.; Herr, R.M.; Aust, B.; Mörtl, K.; Siegrist, J.; Gündel, H.; Angerer, P. Long-Term Effectiveness of a Stress Management Intervention at Work: A 9-Year Follow-Up Study Based on a Randomized Wait-List Controlled Trial in Male Managers. BioMed Res. Int. 2017, 2017. [Google Scholar] [CrossRef]
- Szeto, A.C.; Luong, D.; Dobson, K.S. Does labeling matter? An examination of attitudes and perceptions of labels for mental disorders. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 659–671. [Google Scholar] [CrossRef]
- Griffiths, K.M.; Christensen, H.; Jorm, A.F.; Evans, K.; Groves, C. Effect of web-based depression literacy and cognitive–behavioural therapy interventions on stigmatising attitudes to depression: Randomised controlled trial. Br. J. Psychiatry 2004, 185, 342–349. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline, 3- and 12-Month Follow-Up (n = 41) | Baseline and No Follow-Up (n = 26) | All Included Participants at Baseline (n = 67) | |
|---|---|---|---|
| Male gender n (%) | 35 (85.4) | 21 (80.8) | 56 (83.6) |
| Age at baseline M (SD) | 47.8 (8.4) | 45.6 (8.4) | 47.0 (8.4) |
| Abitur or comparable n (%) | 35 (87.5) | 23 (88.5) | 58 (89.3) |
| Position 1 | |||
| Stage A n (%) | 4 (9.8) | 1 (3.8) | 5 (7.6) |
| Stage B n (%) | 16 (39.0) | 11 (42.3) | 27 (40.9) |
| Stage C n (%) | 8 (19.5) | 7 (26.9) | 15 (22.4) |
| Stage D n (%) | 3 (7.3) | 2 (7.7) | 5 (7.5) |
| Others 2 n (%) | 10 (24.4) | 4 (15.4) | 14 (20.9) |
| Personnel responsibility M (SD) | 21.3 (36.1) | 42.4 (98.3) | 29.3 (67.2) |
| Working hours/week M (SD) | 44.2 (8.6) | 42.4 (9.8) | 43.6 (9.0) |
| SF-12 3 physical health | 53.1 (6.8) | 51.3 (6.4) | 52.5 (6.7) |
| SF-12 3 mental health | 48.8 (9.0) | 49.8 (9.6) | 49.2 (9.2) |
| PHQ-D 4 | 4.1 (2.8) | 3.8 (3.3) | 4.0 (3.0) |
| n = 41 | MT1 (SD) | MT2 (SD) | MT3 (SD) | df | F | p | η2p |
|---|---|---|---|---|---|---|---|
| SoDi 1 | 0.96 (0.63) | 0.85 (0.66) | 0.84 (0.65) | 2, 82 | 1.84 | 0.165 | 0.04 |
| MAKS 2 | 22.88 (2.89) | 23.79 (2.75) | 24.12 (2.53) | 2, 82 | 5.77 | 0.005 * | 0.12 |
| STIGMA mh 3 | 2.86 (1.28) | 2.52 (1.02) | 2.43 (0.94) | 1.52, 62.12 a | 5.61 | 0.011* | 0.12 |
| STIGMA shames 4 | 4.79 (2.41) | 4.90 (2.10) | 4.40 (1.98) | 2, 82 | 2.14 | 0.124 | 0.05 |
| STIGMA shameo 5 | 2.81 (1.63) | 2.81 (1.71) | 2.69 (1.66) | 2, 82 | 0.22 | 0.801 | 0.01 |
| STIGMA support 6 | 5.83 (1.91) | 6.43 (1.43) | 6.67 (1.43) | 2, 82 | 4.42 | 0.012 * | 0.10 |
| STIGMA sd 7 | 2.40 (1.74) | 2.57 (1.80) | 2.45 (1.73) | 2, 82 | 0.24 | 0.790 | 0.01 |
| STIGMA inf8 | 4.40 (2.39) | 4.60 (2.39) | 4.86 (2.50) | 2, 82 | 1.26 | 0.289 | 0.03 |
| ERI 9 Effort | 17.29 (4.09) | 16.15 (4.89) | 16.10 (4.66) | 2, 80 | 2.83 | 0.065 | 0.07 |
| ERI 9 Reward | 47.88 (7.20) | 48.66 (7.07) | 48.07 (7.56) | 2, 80 | 0.27 | 0.765 | 0.01 |
| ERI 9 Overcommitment | 2.37 (0.61) | 2.32 (0.58) | 2.31 (0.59) | 2, 82 | 0.41 | 0.666 | 0.01 |
| IS 10 general score | 19.80 (9.20) | 20.45 (9.54) | 19.71 (9.88) | 2, 82 | 0.35 | 0.705 | 0.01 |
| Time | Time | Mean Difference | SE | p | Cohen’s d | |
|---|---|---|---|---|---|---|
| MAKS 1 | 1 | 2 | −0.90 | 0.38 | 0.062 | −0.32 |
| 2 | 3 | −0.33 | 0.36 | 1.000 | −0.13 | |
| 1 | 3 | −1.24 * | 0.40 | 0.010 | −0.46 | |
| STIGMA mh 2 | 1 | 2 | 0.33 * | 0.11 | 0.009 | 0.29 |
| 2 | 3 | 0.10 | 0.12 | 1.000 | 0.09 | |
| 1 | 3 | 0.43 * | 0.17 | 0.043 | 0.38 | |
| STIGMA support 3 | 1 | 2 | −0.60 * | 0.24 | 0.047 | −0.36 |
| 2 | 3 | −0.24 | 0.27 | 1.000 | −0.17 | |
| 1 | 3 | −0.83 * | 0.32 | 0.041 | −0.50 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwarz, E.; Schiller, B.; Moertl, K.; Weimer, K.; Eisele, M.; Kauderer, J.; Papenfuss, F.; Guendel, H.; Hoelzer, M. Long-Term Attitude Change After a Single-Day Manager Training Addressing Mental Health at the Workplace. Int. J. Environ. Res. Public Health 2019, 16, 5105. https://doi.org/10.3390/ijerph16245105
Schwarz E, Schiller B, Moertl K, Weimer K, Eisele M, Kauderer J, Papenfuss F, Guendel H, Hoelzer M. Long-Term Attitude Change After a Single-Day Manager Training Addressing Mental Health at the Workplace. International Journal of Environmental Research and Public Health. 2019; 16(24):5105. https://doi.org/10.3390/ijerph16245105
Chicago/Turabian StyleSchwarz, Elena, Birgitta Schiller, Kathrin Moertl, Katja Weimer, Marlene Eisele, Johanna Kauderer, Falko Papenfuss, Harald Guendel, and Michael Hoelzer. 2019. "Long-Term Attitude Change After a Single-Day Manager Training Addressing Mental Health at the Workplace" International Journal of Environmental Research and Public Health 16, no. 24: 5105. https://doi.org/10.3390/ijerph16245105
APA StyleSchwarz, E., Schiller, B., Moertl, K., Weimer, K., Eisele, M., Kauderer, J., Papenfuss, F., Guendel, H., & Hoelzer, M. (2019). Long-Term Attitude Change After a Single-Day Manager Training Addressing Mental Health at the Workplace. International Journal of Environmental Research and Public Health, 16(24), 5105. https://doi.org/10.3390/ijerph16245105