Study on Pre-Exposure Prophylaxis Regimens among Men Who Have Sex with Men: A Prospective Cohort Study

Abstract
1. Introduction
2. Subjects and Methods
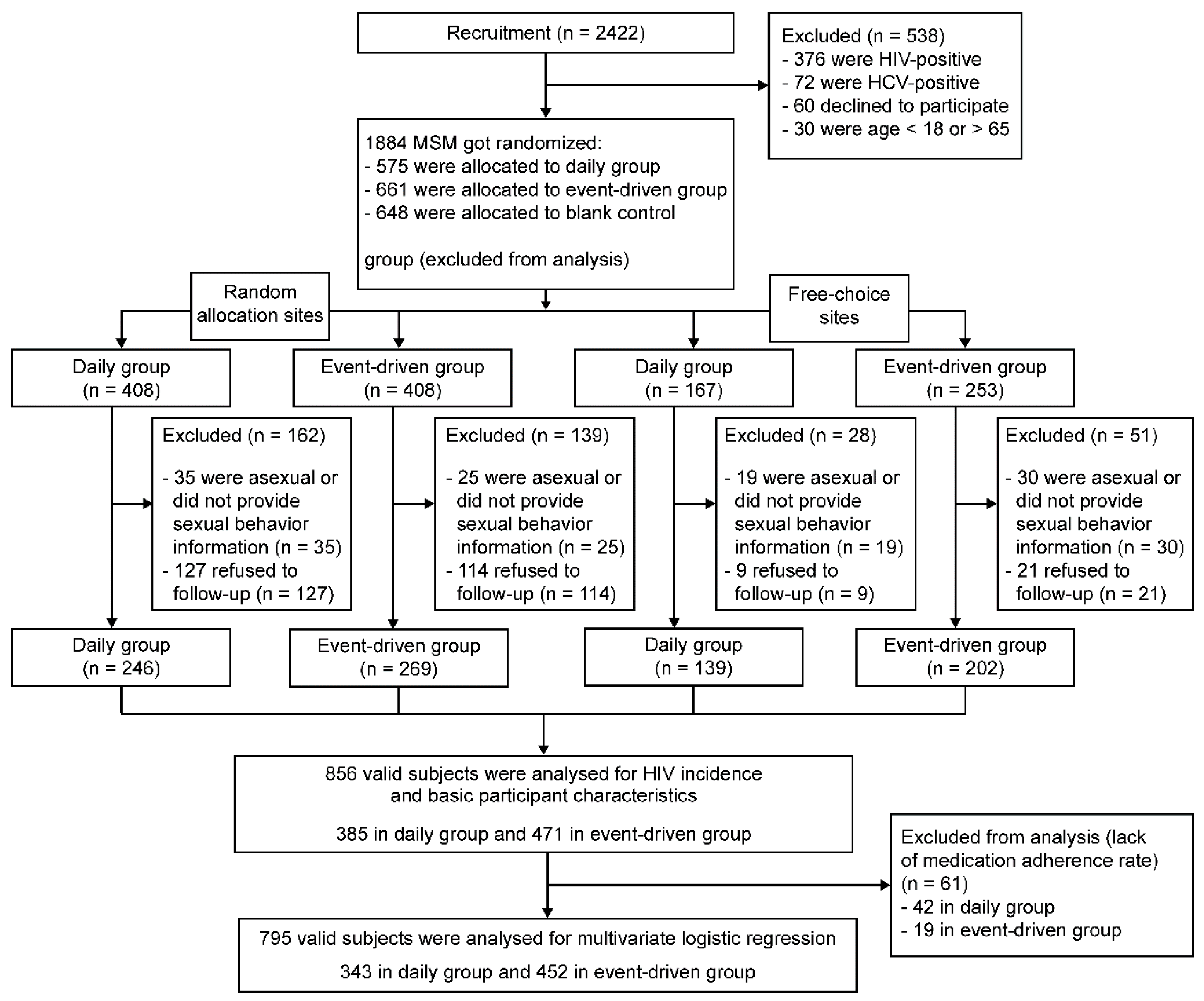
2.1. Research Subjects
2.2. Trial Contents and Methods
2.2.1. Design
2.2.2. Study Procedures
2.2.3. Measures
2.3. Quality Control and Ethics
2.4. Statistical Analysis
3. Results
3.1. Subject Characteristics
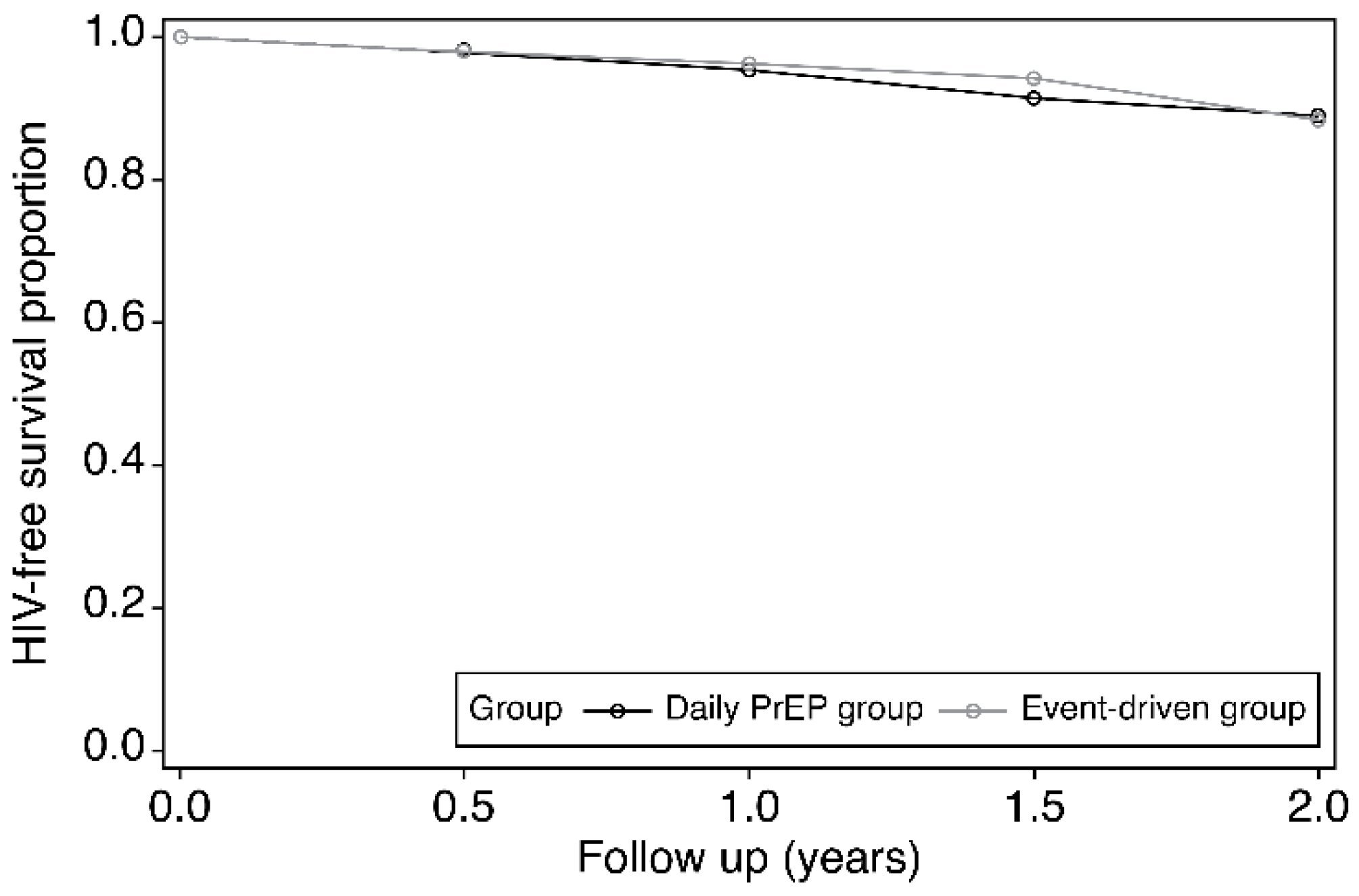
3.2. Sero-Conversion in Subjects
3.3. Serum TDF Concentration
3.4. Factors Influencing Adherence
3.4.1. Univariate Analysis
3.4.2. Multivariate Logistic Regression Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UNAIDS. Available online: http://www.unaids.org/en/resources/documents/2018/unaids-data-2018 (accessed on 5 March 2019).
- Wu, Z.Y. Characteristics of HIV sexually transmission and challenges for controlling the epidemic in China. Zhonghua Liu Xing Bing Xue Za Zhi 2018, 39, 707–709. [Google Scholar] [PubMed]
- Wright, E.; Grulich, A.; Roy, K.; Boyd, M.; Cornelisse, V.; Russell, D.; O’Donnell, D.; Whittaker, B.; Crooks, L.; Zablotska, I. Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine HIV pre-exposure prophylaxis: Clinical guidelines. J. Virus Erad. 2018, 4, 143–159. [Google Scholar] [PubMed]
- Baeten, J.M.; Donnell, D.; Mugo, N.R.; Ndase, P.; Thomas, K.K.; Campbell, J.D.; Wangisi, J.; Tappero, J.W.; Bukusi, E.A.; Cohen, C.R.; et al. Single-Agent Tenofovir versus Combination Emtricitabine/Tenofovir for Pre-Exposure Prophylaxis against HIV-1 Acquisition: A Randomized Trial. Lancet Infect. Dis. 2014, 14, 1055–1064. [Google Scholar] [CrossRef]
- Baeten, J.M.; Donnell, D.; Ndase, P.; Mugo, N.R.; Campbell, J.D.; Wangisi, J.; Tappero, J.W.; Bukusi, E.A.; Cohen, C.R.; Katabira, E.; et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N. Engl. J. Med. 2012, 367, 399–410. [Google Scholar] [CrossRef]
- Molina, J.-M.; Capitant, C.; Charreau, I.; Meyer, L.; Spire, B.; Pialoux, G.; Chidiac, C.; Delfraissy, J.-F.; Tremblay, C. On Demand PrEP with Oral TDF-FTC in MSM: Results of the ANRS Ipergay Trial. Available online: https://www.avac.org/sites/default/files/u3/clarity_on_PrEP_SLIDES.pdf (accessed on 9 November 2019).
- Desai, M.; Field, N.; Grant, R.; McCormack, S. Recent advances in PrEP for HIV. BMJ 2017, 359, j5011. [Google Scholar] [CrossRef] [PubMed]
- Grant, R.M.; Lama, J.R.; Anderson, P.L.; McMahan, V.; Liu, A.Y.; Vargas, L.; Goicochea, P.; Casapía, M.; Guanira-Carranza, J.V.; Ramirez-Cardich, M.E.; et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N. Engl. J. Med. 2010, 363, 2587–2599. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhong, X.; Peng, B.; Liang, H.; Peng, H.; Huang, A. Awareness, experience and willingness of using HIV pre-exposure prophylaxis among men who have sex with men. J. Third Mil. Med. Univ. 2013, 35, 2226–2230. [Google Scholar]
- De Baetselier, I.; Reyniers, T.; Nöstlinger, C.; Wouters, K.; Fransen, K.; Crucitti, T.; Kenyon, C.; Buyze, J.; Schurmans, C.; Laga, M.; et al. Pre-Exposure prophylaxis (PrEP) as an additional tool for HIV prevention among men who have sex with men in Belgium: The Be-PrEP-ared Study Protocol. JMIR Res. Protoc. 2017, 6, e11. [Google Scholar] [CrossRef] [PubMed]
- Hoornenborg, E.; Achterbergh, R.C.; van der Loeff, M.F.S.; Davidovich, U.; van der Helm, J.J.; Hogewoning, A.; van Duijnhoven, Y.T.; Sonder, G.J.; de Vries, H.J.; Prins, M.; et al. Men who have sex with men more often chose daily than event-driven use of pre-exposure prophylaxis: Baseline analysis of a demonstration study in Amsterdam. J. Int. AIDS Soc. 2018, 21, e25105. [Google Scholar] [CrossRef] [PubMed]
- Ouellet, E.; Durand, M.; Guertin, J.R.; LeLorier, J.; Tremblay, C.L. Cost effectiveness of ‘on demand’ HIV pre-exposure prophylaxis for non-injection drug-using men who have sex with men in Canada. Can. J. Infect. Dis. Med. Microbiol. 2015, 26, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Sagaon-Teyssier, L.; Suzan-Monti, M.; Demoulin, B.; Capitant, C.; Lorente, N.; Préau, M.; Mora, M.; Rojas Castro, D.; Chidiac, C.; Chas, J.; et al. Uptake of PrEP and condom and sexual risk behavior among MSM during the ANRS IPERGAY trial. AIDS Care 2016, 28, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Dimitrov, D.T.; Mâsse, B.R.; Donnell, D. PrEP adherence patterns strongly impact individual HIV risk and observed efficacy in randomized clinical trials. J. Acquir. Immune Defic. Syndr. 2016, 72, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Haberer, J.E.; Kidoguchi, L.; Heffron, R.; Mugo, N.; Bukusi, E.; Katabira, E.; Asiimwe, S.; Thomas, K.K.; Celum, C.; Baeten, J.M. Alignment of adherence and risk for HIV acquisition in a demonstration project of pre-exposure prophylaxis among HIV serodiscordant couples in Kenya and Uganda: A prospective analysis of prevention-effective adherence. J. Int. AIDS Soc. 2017, 20, 21842. [Google Scholar] [CrossRef] [PubMed]
- Haberer, J.E.; Baeten, J.M.; Campbell, J.; Wangisi, J.; Katabira, E.; Ronald, A.; Tumwesigye, E.; Psaros, C.; Safren, S.A.; Ware, N.C.; et al. Adherence to antiretroviral prophylaxis for HIV prevention: A substudy cohort within a clinical trial of serodiscordant couples in East Africa. PLoS Med. 2013, 10, e1001511. [Google Scholar] [CrossRef] [PubMed]
- Burch, L.; Smith, C.; Anderson, J.; Sherr, L.; Rodger, A.; O’Connell, R.; Gilson, R.; Elford, J.; Phillips, A.; Speakman, A.; et al. Socio-economic factors and virological suppression among people diagnosed with HIV in the United Kingdom: Results from the ASTRA study. J. Int. AIDS Soc. 2014, 17, 19533. [Google Scholar] [CrossRef] [PubMed]
- Batchelder, A.W.; Safren, S.; Mitchell, A.D.; Ivardic, I.; O’Cleirigh, C. Mental health in 2020 for men who have sex with men in the United States. Sex. Health 2017, 14, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Zhong, X.; Peng, B.; Zhang, Y.; Liang, H.; Zou, Y.; Dai, J.; Liu, Q.; Song, B.; Huang, W.; et al. Pre-exposure prophylaxis for HIV high-risk groups: An analysis of clinical adherence. Acad. J. Second Mil. Med. Univ. 2012, 32, 1186–1193. [Google Scholar] [CrossRef]
- Storholm, E.D.; Volk, J.E.; Marcus, J.L.; Silverberg, M.J.; Satre, D.D. Risk perception, sexual behaviors, and PrEP adherence among substance-using men who have sex with men: A qualitative study. Prev. Sci. 2017, 18, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Abaasa, A.; Hendrix, C.; Gandhi, M.; Anderson, P.; Kamali, A.; Kibengo, F.; Sanders, E.J.; Mutua, G.; Bumpus, N.N.; Priddy, F.; et al. Utility of different adherence measures for PrEP: Patterns and incremental value. AIDS Behav. 2018, 22, 1165–1173. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Daily PrEP Group (N = 385) | Event-Driven Group (N = 471) | χ2 Value | p Value | Daily PrEP Group in Random Allocation Sites (N = 246) | Event-Driven Group in Random Allocation Sites (N = 269) | χ2 Value | p Value | Daily PrEP Group in Free-Choice Sites (N = 139) | Event-Driven Group in Free-Choice Sites (N = 202) | χ2 Value | p Value |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 2.08 | 0.149 | 1.01 | 0.314 | 1.04 | 0.308 | ||||||
| <30 | 139 (36.1%) | 31.4 (51.2%) | 89 (36.2%) | 86 (31.97%) | 50 (36.0%) | 62 (30.7%) | ||||||
| Household registration * | 1.09 | 0.296 | 0.12 | 0.730 | 0.60 | 0.439 | ||||||
| Town | 279 (72.7%) | 357 (75.8%) | 165 (67.4%) | 185 (68.8%) | 114 (82.0%) | 172 (85.2%) | ||||||
| Nationality | 0.18 | 0.674 | 0.31 | 0.580 | 0.16 | 0.690 | ||||||
| Han nationality | 353 (91.7%) | 428 (90.9%) | 239 (97.2%) | 259 (96.3%) | 114 (82.0%) | 169 (83.7%) | ||||||
| Degree of Education * | 1.91 | 0.592 | 3.64 | 0.303 | 1.10 | 0.778 | ||||||
| Junior high school and below | 41 (10.7%) | 55 (11.7%) | 31 (12.6%) | 42 (15.6%) | 10 (7.3%) | 13 (6.4%) | ||||||
| Senior high school/vocational high school/technical secondary school | 109 (28.4%) | 114 (24.3%) | 80 (32.5%) | 70 (26.0%) | 29 (21.0%) | 44 (21.9%) | ||||||
| Junior College | 87 (22.7%) | 111 (23.6%) | 58 (23.6%) | 60 (22.3%) | 29 (21.0%) | 51 (25.4%) | ||||||
| University or above | 147 (38.3%) | 190 (40.4%) | 77 (31.3%) | 97 (36.1%) | 70 (50.7%) | 93 (46.3%) | ||||||
| Employment * | 0.10 | 0.949 | 3.12 | 0.211 | 0.05 | 0.978 | ||||||
| Employed | 293 (76.7%) | 281 (80.9%) | 185 (75.8%) | 221 (82.1%) | 108 (78.3%) | 160 (79.2%) | ||||||
| Students | 54 (14.1%) | 54 (11.4%) | 36 (14.8%) | 29 (10.8%) | 18 (13.0%) | 25 (12.4%) | ||||||
| Unemployed or retired | 35 (9.2%) | 36 (9.7%) | 23 (9.4%) | 19 (7.1%) | 12 (8.7%) | 17 (8.4%) | ||||||
| Marital status | 5.09 | 0.079 | 2.11 | 0.348 | 5.13 | 0.077 | ||||||
| Unmarried | 297 (77.1%) | 336 (71.4%) | 182 (74.0%) | 184 (68.4%) | 115 (82.7%) | 152 (75.2%) | ||||||
| Married | 61 (15.9%) | 83 (17.6%) | 42 (17.1%) | 53 (19.7%) | 19 (13.7%) | 30 (14.9%) | ||||||
| Divorced or widowed | 27 (7.0%) | 52 (11.0%) | 22 (8.9%) | 32 (11.9%) | 5 (3.6%) | 20 (9.9%) | ||||||
| Monthly income * | 1.99 | 0.738 | 7.57 | 0.109 | 6.66 | 0.155 | ||||||
| 1000 yuan or below | 57 (15.1%) | 66 (14.2%) | 43 (17.7%) | 34 (12.7%) | 14 (10.3%) | 32 (16.1%) | ||||||
| 1001~3000 yuan | 138 (36.4%) | 165 (35.4%) | 98 (40.3%) | 113 (42.3%) | 40 (29.4%) | 52 (26.1%) | ||||||
| 3001~5000 yuan | 132 (34.8%) | 180 (38.6%) | 76 (31.3%) | 92 (34.5%) | 56 (41.2%) | 88 (44.2%) | ||||||
| 5001~10,000 yuan | 44 (11.6%) | 44 (9.4%) | 24 (9.9%) | 19 (7.1%) | 20 (14.7%) | 25 (12.6%) | ||||||
| above 10,000 yuan | 8 (2.1%) | 11 (2.4%) | 2 (0.8%) | 9 (3.4%) | 6 (4.4%) | 2 (1.0%) | ||||||
| Have you taken the initiative to conduct HIV free consultation? * | 0.46 | 0.496 | 0.26 | 0.608 | 0.37 | 0.541 | ||||||
| Yes | 243 (63.3%) | 306 (65.5%) | 128 (52.2%) | 145 (54.5%) | 115 (82.7%) | 161 (80.1%) | ||||||
| Have you tested the HIV virus? | 0.01 | 0.959 | 0.04 | 0.848 | 2.20 | 0.138 | ||||||
| Yes | 70 (18.2%) | 85 (18.1%) | 64 (26.0%) | 68 (25.3%) | 6 (4.3%) | 17 (8.4%) | ||||||
| Frequency of sexual partners through the Internet * | 2.50 | 0.476 | 0.54 | 0.911 | 2.93 | 0.402 | ||||||
| Often | 23 (6.3%) | 34 (7.5%) | 16 (7.1%) | 20 (7.9%) | 7 (5.1%) | 14 (7.0%) | ||||||
| Sometimes | 66 (18.1%) | 75 (16.6%) | 39 (17.2%) | 39 (15.5%) | 27 (19.7%) | 36 (17.9%) | ||||||
| Occasional | 137 (37.7%) | 190 (41.9%) | 87 (38.3%) | 102 (40.5%) | 50 (36.5%) | 88 (43.8%) | ||||||
| Completely none | 138 (37.9%) | 154 (34.0%) | 85 (37.4%) | 91 (36.1%) | 53 (38.7%) | 63 (31.3%) | ||||||
| Have you been diagnosed with sexually transmitted diseases by doctors? * | 1.71 | 0.191 | 2.95 | 0.086 | 0.16 | 0.685 | ||||||
| Yes | 38 (10.0%) | 35 (7.5%) | 21 (8.6%) | 13 (4.9%) | 17 (12.3%) | 22 (10.9%) | ||||||
| Drinking alcohol frequency in a recent month * | 3.69 | 0.449 | 4.91 | 0.297 | 2.73 | 0.604 | ||||||
| Daily | 13 (3.4%) | 21 (4.5%) | 11 (4.6%) | 16 (6.0%) | 2 (1.5%) | 5 (2.5%) | ||||||
| At least three times/week | 39 (10.2%) | 42 (8.9%) | 30 (12.2%) | 23 (8.6%) | 9 (6.5%) | 19 (9.4%) | ||||||
| At least once/week | 55 (14.4%) | 81 (17.2%) | 30 (12.2%) | 36 (13.4%) | 25 (18.1%) | 45 (22.3%) | ||||||
| Less than once a week | 146 (38.1%) | 189 (40.1%) | 86 (35.1%) | 112 (41.6%) | 60 (43.5%) | 77 (38.1%) | ||||||
| No alcohol | 130 (33.9%) | 138 (29.3%) | 88 (35.9%) | 82 (30.4%) | 42 (30.4%) | 56 (27.7%) | ||||||
| Drug use in the last half a year * | 0.83 | 0.362 | 0.99 | 0.319 | 0.04 | 0.852 | ||||||
| Using | 9 (2.4%) | 16 (3.5%) | 4 (1.7) | 8 (3.0) | 5 (3.7%) | 8 (4.1%) | ||||||
| Commercial sex behavior in recent half a year * | 0.14 | 0.710 | 0.02 | 0.883 | 0.59 | 0.441 | ||||||
| Occurring | 20 (5.2%) | 22 (4.7%) | 12 (4.9%) | 14 (5.2%) | 8 (5.8%) | 8 (4.0%) |
| Stratification Factors | Group | Positive Conversion | The Number of Exposed Subjects | Total Person Years at Risk | Overall Person Years | HIV Incidence (Cases/100 Person-Years) | RR Vale (95% CI) | |
|---|---|---|---|---|---|---|---|---|
| Overall | Daily PrEP group | 30 | 385 | 26.75 | 454.5 | 6.60 | 0.844 (0.492–1.449) | |
| Event-driven group | 32 | 471 | 29.00 | 575.0 | 5.565 | |||
| Medication adherence rate | <80% | Daily PrEP group * | 22 | 243 | 20.00 | 294.75 | 7.464 | 1.216 (0.661–2.236) |
| Event-driven group * | 27 | 252 | 25.50 | 297.5 | 9.076 | |||
| ≥80% | Daily PrEP group * | 4 | 124 | 3.00 | 147.0 | 2.720 | 0.668 (0.141–3.164) | |
| Event-driven group * | 5 | 215 | 3.50 | 275.25 | 1.817 | |||
| Sites | Random allocation sites | Daily PrEP group | 20 | 246 | 20.50 | 297.0 | 6.734 | 0.844 (0.425–1.675) |
| Event-driven group | 19 | 269 | 15.00 | 334.25 | 5.684 | |||
| Free-choice sites | Daily PrEP group | 10 | 139 | 6.25 | 157.50 | 6.349 | 0.851 (0.324–2.233) | |
| Event-driven group | 13 | 202 | 14.00 | 240.75 | 5.400 | |||
| Medication Adherence Rate | Medication Pattern | N | Median(mg/L) | P25–P75(mg/L) | Z | p |
|---|---|---|---|---|---|---|
| <80% | Daily PrEP group * | 67 | 0.404 | 0.237–0.661 | −0.997 | 0.319 |
| Event-driven group * | 71 | 0.472 | 0.255–0.987 | |||
| ≥80% | Daily PrEP group * | 57 | 0.458 | 0.272–0.625 | 0.190 | 0.849 |
| Event-driven group * | 66 | 0.429 | 0.278–0.648 |
| Variable | High Adherence (N = 409) | Low Adherence (N = 386) | χ2 | p |
|---|---|---|---|---|
| Behavioral characteristics of subjects | ||||
| Have you taken the initiative to conduct HIV free consultation? * | 2.22 | 0.136 | ||
| Yes | 274 (67.7%) | 241 (62.6%) | ||
| Have you tested the HIV virus? | 0.01 | 0.928 | ||
| Yes | 339 (82.9%) | 319 (82.6%) | ||
| Frequency of sexual partners through Internet in recent half a year * | 5.49 | 0.139 | ||
| Often | 31 (7.9%) | 23 (6.3%) | ||
| Sometimes | 66 (16.8%) | 58 (15.9%) | ||
| Occasional | 169 (43.1%) | 137 (37.7%) | ||
| Completely none | 126 (32.2%) | 146 (40.1%) | ||
| Have you been diagnosed with sexually transmitted diseases by doctors in recent half a year? * | 2.73 | 0.099 | ||
| Yes | 29 (7.1%) | 40 (10.4%) | ||
| Drinking alcohol frequency in a recent month * | 6.44 | 0.169 | ||
| Daily | 18 (4.4%) | 15 (3.9%) | ||
| At least three times/week | 41 (10.0%) | 33 (8.6%) | ||
| At least once/week | 56 (13.7%) | 70 (18.2%) | ||
| Less than once a week | 155 (37.9%) | 160 (41.7%) | ||
| No alcohol | 139 (34.0%) | 106 (27.6%) | ||
| Drug use in the last half a year * | 0.03 | 0.873 | ||
| Using | 12 (3.0%) | 12 (3.2%) | ||
| Commercial sex behavior in recent half a year * | 0.35 | 0.552 | ||
| Occurring | 23 (5.6%) | 18 (4.7%) | ||
| Perceptions and AIDS related attitudes of the subjects | ||||
| What do you think of the severity of AIDS? * | 4.89 | 0.299 | ||
| Very high | 266 (65.0%) | 278 (72.2%) | ||
| Relatively high | 118 (28.9%) | 88 (22.9%) | ||
| Average | 20 (4.9%) | 16 (4.2%) | ||
| Relatively low | 3 (0.7%) | 2 (0.5%) | ||
| Very low | 2 (0.5%) | 1 (0.2%) | ||
| Medicine makes me safe, away from AIDS * | 19.93 | 0.001 | ||
| Completely none | 89 (21.9%) | 129 (33.7%) | ||
| A little | 86 (21.2%) | 88 (23.0%) | ||
| Somewhat | 98 (24.2%) | 61 (15.9%) | ||
| Majority | 46 (11.3%) | 44 (11.5%) | ||
| Always | 87 (21.4%) | 61 (15.9%) | ||
| I am worried that the medicine does not work * | 13.03 | 0.011 | ||
| Completely none | 96 (23.7%) | 89 (23.2%) | ||
| A little | 148 (36.5%) | 120 (31.3%) | ||
| Somewhat | 87 (21.4%) | 64 (16.7%) | ||
| Majority | 20 (4.9%) | 34 (8.9%) | ||
| Always | 55 (13.5%) | 76 (19.9%) | ||
| I’m worried about the side effects of medicine * | 17.74 | 0.001 | ||
| Completely none | 92 (22.6%) | 58 (15.1%) | ||
| A little | 121 (29.8%) | 93 (24.3%) | ||
| Somewhat | 99 (24.4%) | 98 (25.6%) | ||
| Majority | 34 (8.4%) | 48 (12.5%) | ||
| Always | 60 (14.8%) | 86 (22.5%) | ||
| I am worried that others know that I am taking medicine * | 15.58 | 0.004 | ||
| Completely none | 136 (33.4%) | 102 (26.6%) | ||
| A little | 120 (29.5%) | 92 (24.0%) | ||
| Somewhat | 74 (18.2%) | 74 (19.3%) | ||
| Majority | 21 (5.2%) | 35 (9.2%) | ||
| Always | 56 (13.7%) | 80 (20.9%) | ||
| I felt the side effects of medicine * | 5.97 | 0.201 | ||
| Completely none | 238 (58.6%) | 241 (62.9%) | ||
| A little | 115 (28.3%) | 92 (24.0%) | ||
| Somewhat | 38 (9.4%) | 27 (7.1%) | ||
| Majority | 9 (2.2%) | 11 (2.9%) | ||
| Always | 6 (1.5%) | 12 (3.1%) | ||
| I am more afraid of AIDS * | 12.05 | 0.017 | ||
| Completely none | 218 (53.6%) | 200 (52.2%) | ||
| A little | 117 (28.8%) | 113 (29.5%) | ||
| Somewhat | 40 (9.8%) | 35 (9.2%) | ||
| Majority | 4 (1.0%) | 18 (4.7%) | ||
| Always | 28 (6.8%) | 17 (4.4%) | ||
| I feel that the doctors have discriminated against me * | 0.35 | 0.987 | ||
| Completely none | 372 (91.4%) | 346 (90.3%) | ||
| A little | 20 (4.9%) | 21 (5.5%) | ||
| Somewhat | 6 (1.5%) | 6 (1.6%) | ||
| Majority | 4 (1.0%) | 5 (1.3%) | ||
| Always | 5 (1.2%) | 5 (1.3%) |
| Variable (Controlled Group) | β | p Value | OR (95% CI) |
|---|---|---|---|
| Overall analysis | |||
| Age * | 0.0221 | 0.0290 | 1.022 (1.002–1.043) |
| Number of sexual partners in the last two weeks * | −0.3783 | 0.0002 | 0.685 (0.563–0.834) |
| Medication regimen (daily PrEP group) * | |||
| event-driven group | 0.7662 | <0.0001 | 2.152 (1.566–2.957) |
| Medicine makes me safe, away from AIDS (Completely none) * | |||
| A little | 0.5462 | 0.0163 | 1.727 (1.106–2.696) |
| Somewhat | 1.1155 | <0.0001 | 3.051 (1.921–4.847) |
| Majority | 0.5973 | 0.0325 | 1.817 (1.051–3.141) |
| Always | 0.8935 | 0.0002 | 2.444 (1.522–3.924) |
| I am worried that others know I am taking medicine * | |||
| A little | 0.1412 | 0.5064 | 1.152 (0.759–1.746) |
| Somewhat | −0.0651 | 0.7780 | 0.937 (0.596–1.473) |
| Majority | −0.6967 | 0.0396 | 0.498 (0.257–0.967) |
| Always | −0.4864 | 0.0434 | 0.615 (0.383–0.986) |
| Sub-analysis of subjects in the random allocation sites | |||
| Age * | 0.0426 | 0.0009 | 1.044 (1.018–1.070) |
| Number of sexual partners in the last two weeks * | −0.4152 | 0.0005 | 0.660 (0.522–0.835) |
| Sub-analysis of subjects in the free-choice sites | |||
| Medication regimen (daily PrEP group) * | |||
| event-driven group | 2.5891 | <0.0001 | 13.317 (6.664–26.614) |
| Medicine makes me safe, away from AIDS (Completely none) * | |||
| A little | 0.3956 | 0.2731 | 1.485 (0.732–3.013) |
| Somewhat | 1.7924 | <0.0001 | 6.004 (2.725–13.231) |
| Majority | 1.4685 | 0.0224 | 4.343 (1.231–15.313) |
| Always | 2.2687 | 0.0582 | 9.667 (0.925–101.068) |
| I am worried that others know I am taking medicine * | |||
| A little | 1.1294 | 0.0045 | 3.094 (1.420–6.741) |
| Somewhat | 1.3899 | 0.0053 | 4.014 (1.510–10.672) |
| Majority | −0.1518 | 0.7839 | 0.859 (0.290–2.543) |
| Always | 0.2005 | 0.5757 | 1.222 (0.606–2.466) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, D.; Tao, H.; Dai, J.; Liang, H.; Huang, A.; Zhong, X. Study on Pre-Exposure Prophylaxis Regimens among Men Who Have Sex with Men: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 4996. https://doi.org/10.3390/ijerph16244996
Wu D, Tao H, Dai J, Liang H, Huang A, Zhong X. Study on Pre-Exposure Prophylaxis Regimens among Men Who Have Sex with Men: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2019; 16(24):4996. https://doi.org/10.3390/ijerph16244996
Chicago/Turabian StyleWu, Dan, Hao Tao, Jianghong Dai, Hao Liang, Ailong Huang, and Xiaoni Zhong. 2019. "Study on Pre-Exposure Prophylaxis Regimens among Men Who Have Sex with Men: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 16, no. 24: 4996. https://doi.org/10.3390/ijerph16244996
APA StyleWu, D., Tao, H., Dai, J., Liang, H., Huang, A., & Zhong, X. (2019). Study on Pre-Exposure Prophylaxis Regimens among Men Who Have Sex with Men: A Prospective Cohort Study. International Journal of Environmental Research and Public Health, 16(24), 4996. https://doi.org/10.3390/ijerph16244996