Density of Green Spaces and Cardiovascular Risk Factors in the City of Madrid: The Heart Healthy Hoods Study


 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Population
2.3. Exposure: Density of Green Spaces
2.4. Outcome: Cardiovascular Risk Factors
2.5. Covariates
2.6. Data Analysis
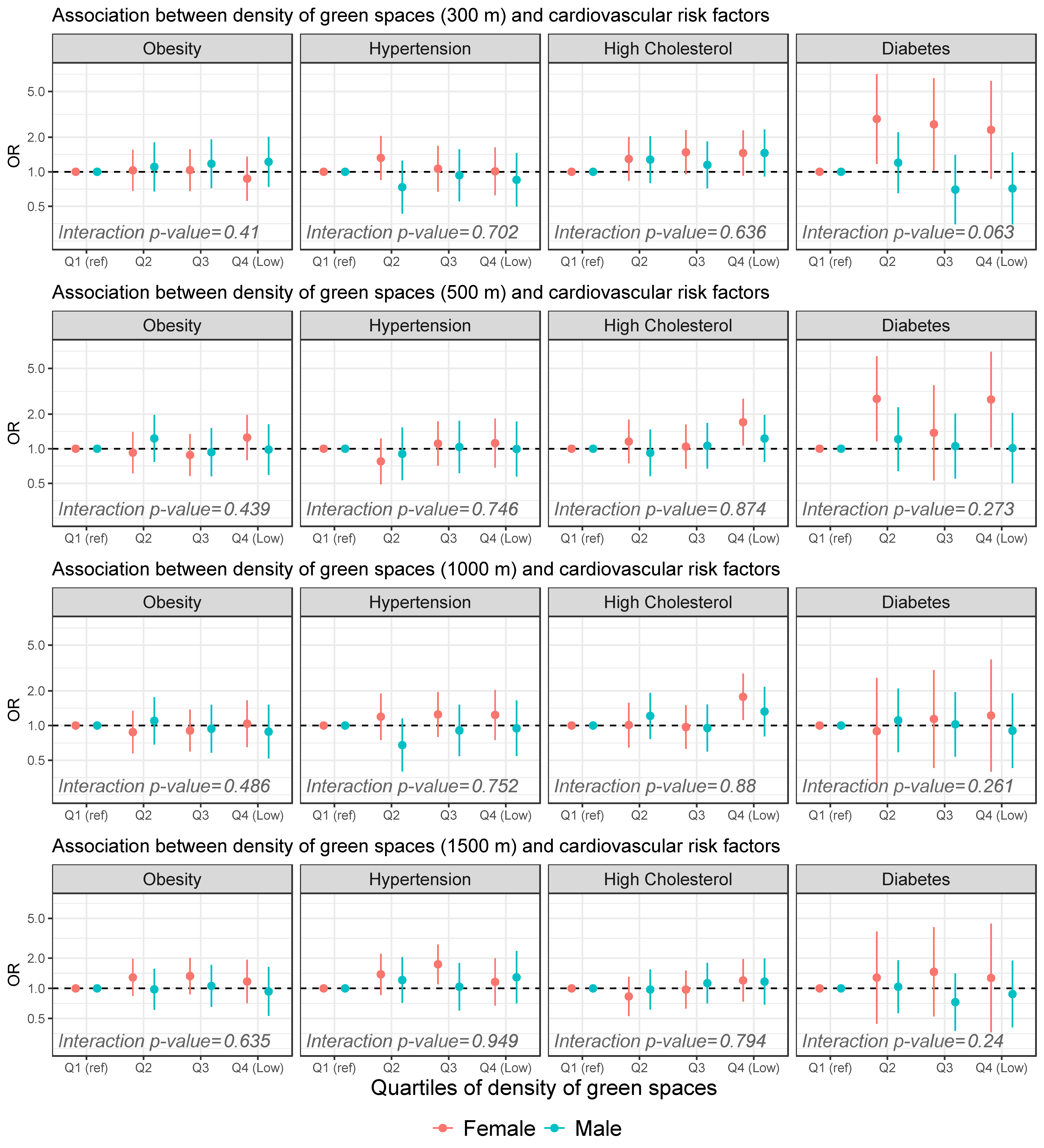
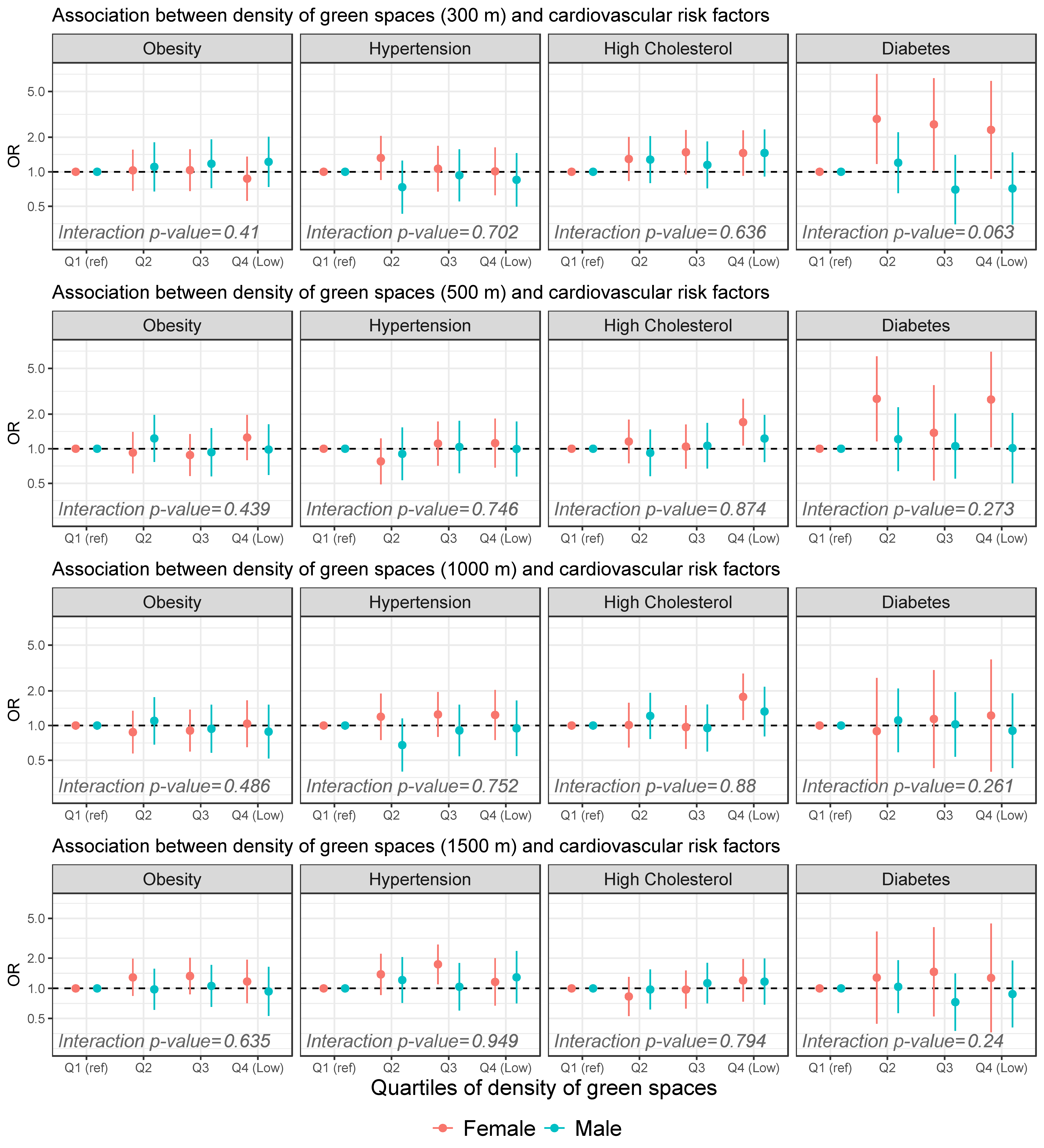
3. Results
4. Discussion
4.1. Key Findings
4.2. Comparison with Previous Studies and Mechanisms
4.3. Effect of Gender and Buffer Size
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Joseph, P.; Leong, D.; McKee, M.; Anand, S.S.; Schwalm, J.-D.; Teo, K.; Mente, A.; Yusuf, S. Reducing the Global Burden of Cardiovascular Disease, Part 1. Circ. Res. 2017, 121, 677–694. [Google Scholar] [CrossRef] [PubMed]
- Townsend, N.; Wilson, L.; Bhatnagar, P.; Wickramasinghe, K.; Rayner, M.; Nichols, M. Cardiovascular disease in Europe: Epidemiological update 2016. Eur. Heart J. 2016, 37, 3232–3245. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Status Report on Noncommunicable Diseases 2014; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Chow, C.K.; Lock, K.; Teo, K.; Subramanian, S.; McKee, M.; Yusuf, S. Environmental and societal influences acting on cardiovascular risk factors and disease at a population level: A review. Int. J. Epidemiol. 2009, 38, 1580–1594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aranceta-Bartrina, J.; Pérez-Rodrigo, C.; Alberdi-Aresti, G.; Ramos-Carrera, N.; Lázaro-Masedo, S. Prevalence of General Obesity and Abdominal Obesity in the Spanish Adult Population (Aged 25–64 Years) 2014–2015: The ENPE Study. Rev. Española Cardiol. 2016, 69, 579–587. [Google Scholar] [CrossRef]
- Menéndez, E.; Delgado, E.; Fernández-Vega, F.; Prieto, M.A.; Bordiú, E.; Calle, A.; Carmena, R.; Castaño, L.; Catalá, M.; Franch, J.; et al. Prevalencia, diagnóstico, tratamiento y control de la hipertensión arterial en España. Resultados del estudio Di@bet.es. Rev. Esp. Cardiol. 2016, 69, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Guallar-Castillón, P.; Gil-Montero, M.; León-Muñoz, L.M.; Graciani, A.; Bayán-Bravo, A.; Taboada, J.M.; Banegas, J.R.; Rodríguez-Artalejo, F. Magnitude and management of hypercholesterolemia in the adult population of Spain, 2008–2010: The ENRICA study. Rev. Esp. Cardiol. 2012, 65, 551–558. [Google Scholar] [CrossRef]
- Soriguer, F.; Goday, A.; Bosch-Comas, A.; Bordiú, E.; Calle-Pascual, A.; Carmena, R.; Casamitjana, R.; Castaño, L.; Castell, C.; Catalá, M.; et al. Prevalence of diabetes mellitus and impaired glucose regulation in Spain: The Di@bet.es Study. Diabetologia 2012, 55, 88–93. [Google Scholar] [CrossRef] [Green Version]
- De Smedt, D.; De Bacquer, D.; De Sutter, J.; Dallongeville, J.; Gevaert, S.; De Backer, G.; Bruthans, J.; Kotseva, K.; Reiner, Ž.; Tokgözoğlu, L.; et al. The gender gap in risk factor control: Effects of age and education on the control of cardiovascular risk factors in male and female coronary patients. the EUROASPIRE IV study by the European Society of Cardiology. Int. J. Cardiol. 2016, 209, 284–290. [Google Scholar] [CrossRef]
- ROSE, G. Sick Individuals and Sick Populations. Int. J. Epidemiol. 1985, 14, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Franco, M.; Bilal, U.; Diez-Roux, A.V. Preventing non-communicable diseases through structural changes in urban environments. J. Epidemiol. Community Health 2015, 69, 509–511. [Google Scholar] [CrossRef] [Green Version]
- Fong, K.C.; Hart, J.E.; James, P. A Review of Epidemiologic Studies on Greenness and Health: Updated Literature Through 2017. Curr. Environ. Health Rep. 2018, 39, 11–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A Review of the Health Benefits of Greenness. Curr. Epidemiol. Rep. 2015, 2, 218. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, M.J.; Khreis, H.; Triguero-Mas, M.; Gascon, M.; Dadvand, P. Fifty shades of green. Epidemiology 2017, 28, 63–71. [Google Scholar] [CrossRef]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef]
- Gascon, M.; Triguero-Mas, M.; Martínez, D.; Dadvand, P.; Rojas-Rueda, D.; Plasència, A.; Nieuwenhuijsen, M.J. Residential green spaces and mortality: A systematic review. Environ. Int. 2016, 86, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Tamosiunas, A.; Grazuleviciene, R.; Luksiene, D.; Dedele, A.; Reklaitiene, R.; Baceviciene, M.; Vencloviene, J.; Bernotiene, G.; Radisauskas, R.; Malinauskiene, V.; et al. Accessibility and use of urban green spaces, and cardiovascular health: Findings from a Kaunas cohort study. Environ. Health A Glob. Access Sci. Source 2014, 13, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Yeager, R.; Riggs, D.W.; DeJarnett, N.; Tollerud, D.J.; Wilson, J.; Conklin, D.J.; O’Toole, T.E.; McCracken, J.; Lorkiewicz, P.; Xie, Z.; et al. Association between residential greenness and cardiovascular disease risk. J. Am. Heart Assoc. 2018, 7, e009117. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Greener neighborhoods, slimmer people evidence from 246 920 Australians. Int. J. Obes. 2014, 38, 156–159. [Google Scholar] [CrossRef]
- Bijnens, E.M.; Nawrot, T.S.; Loos, R.J.; Gielen, M.; Vlietinck, R.; Derom, C.; Zeegers, M.P. Blood pressure in young adulthood and residential greenness in the early-life environment of twins. Environ. Health 2017, 16, 53. [Google Scholar] [CrossRef] [Green Version]
- Cebrecos, A.; Escobar, F.; Borrell, L.N.; Díez, J.; Gullón, P.; Sureda, X.; Klein, O.; Franco, M. A multicomponent method assessing healthy cardiovascular urban environments: The Heart Healthy Hoods Index. Health Place 2019, 55, 111–119. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight Fact Sheet. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 20 October 2019).
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Grant, P.J.; Chairperson, E.; Germany, S.D.A.; France, N.D.; Uk, C.D.; Germany, H.H.; France, M.M.; Germany, N.M.; Poland, M.T.; France, P.V.; et al. ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD the European Society of Cardiology (ESC) and developed in collaboration. Eur. Heart J. 2013, 34, 3035–3087. [Google Scholar]
- Gullón, P.; Bilal, U.; Cebrecos, A.; Badland, H.M.; Galán, I.; Franco, M. Intersection of neighborhood dynamics and socioeconomic status in small-area walkability: The Heart Healthy Hoods project. Int. J. Health Geogr. 2017, 16, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Instituto Nacional de Estadística Estadística del Padrón Continuo. Available online: www.ine.es (accessed on 29 August 2019).
- Mena, C.; Fuentes, E.; Ormazábal, Y.; Palomo-Vélez, G.; Palomo, I. Role of access to parks and markets with anthropometric measurements, biological markers, and a healthy lifestyle. Int. J. Environ. Health Res. 2015, 25, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Kaczynski, A.T.; Potwarka, L.R.; Saelens, P.B.E. Association of park size, distance, and features with physical activity in neighborhood parks. Am. J. Public Health 2008, 98, 1451–1456. [Google Scholar] [CrossRef]
- Bancroft, C.; Joshi, S.; Rundle, A.; Hutson, M.; Chong, C.; Weiss, C.C.; Genkinger, J.; Neckerman, K.; Lovasi, G. Association of proximity and density of parks and objectively measured physical activity in the United States: A systematic review. Soc. Sci. Med. 2015, 138, 22–30. [Google Scholar] [CrossRef]
- Hosking, J.; Woodward, A.; MacMillan, A.; Smith, M.; Witten, K.; Baas, P.; Mackie, H.; Field, A. Systematic literature review of built environment effects on physical activity and active transport—An update and new findings on health equity. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–27. [Google Scholar]
- Brown, S.C.; Lombard, J.; Wang, K.; Byrne, M.M.; Toro, M.; Plater-Zyberk, E.; Feaster, D.J.; Kardys, J.; Nardi, M.I.; Perez-Gomez, G.; et al. Neighborhood greenness and chronic health conditions in medicare beneficiaries. Am. J. Prev. Med. 2016, 51, 78–89. [Google Scholar] [CrossRef]
- Yang, B.Y.; Markevych, I.; Bloom, M.S.; Heinrich, J.; Guo, Y.; Morawska, L.; Dharmage, S.C.; Knibbs, L.D.; Jalaludin, B.; Jalava, P.; et al. Community greenness, blood pressure, and hypertension in urban dwellers: The 33 Communities Chinese Health Study. Environ. Int. 2019, 126, 727–734. [Google Scholar] [CrossRef]
- Hirabayashi, S.; Nowak, D.J. Comprehensive national database of tree effects on air quality and human health in the United States. Environ. Pollut. 2016, 215, 48–57. [Google Scholar] [CrossRef]
- Kim, H.-J.; Min, J.-Y.; Kim, H.-J.; Min, K.-B. Parks and Green Areas Are Associated with Decreased Risk for Hyperlipidemia. Int. J. Environ. Res. Public Health 2016, 13, 1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalton, A.M.; Jones, A.P.; Sharp, S.J.; Cooper, A.J.M.; Griffin, S.; Wareham, N.J. Residential neighbourhood greenspace is associated with reduced risk of incident diabetes in older people: A prospective cohort study. BMC Public Health 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodicoat, D.H.; O’Donovan, G.; Dalton, A.M.; Gray, L.J.; Yates, T.; Edwardson, C.; Hill, S.; Webb, D.R.; Khunti, K.; Davies, M.J.; et al. The association between neighbourhood greenspace and type 2 diabetes in a large cross-sectional study. BMJ Open 2014, 4, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bos, E.H.; van der Meulen, L.; Wichers, M.; Jeronimus, B.F. A primrose path? Moderating effects of age and gender in the association between green space and mental health. Int. J. Environ. Res. Public Health 2016, 13, 492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, E.A.; Mitchell, R. Gender differences in relationships between urban green space and health in the United Kingdom. Soc. Sci. Med. 2010, 71, 568–575. [Google Scholar] [CrossRef] [Green Version]
- Astell-Burt, T.; Mitchell, R.; Hartig, T. The association between green space and mental health varies across the lifecourse. a longitudinal study. J. Epidemiol. Community Health 2014, 68, 578–583. [Google Scholar] [CrossRef]
- Cohen, D.A.; McKenzie, T.L.; Sehgal, A.; Williamson, S.; Golinelli, D.; Lurie, N. Contribution of public parks to physical activity. Am. J. Public Health 2007, 97, 509–514. [Google Scholar] [CrossRef]
- Ho, C.H.; Sasidharan, V.; Elmendorf, W.; Willits, F.K.; Graefe, A.; Godbey, G. Gender and ethnic variations in urban park preferences, visitation, and perceived benefits. J. Leis. Res. 2005, 37, 281–306. [Google Scholar] [CrossRef]
- Evenson, K.R.; Jones, S.A.; Holliday, K.M.; Cohen, D.A.; McKenzie, T.L. Park characteristics, use, and physical activity: A review of studies using SOPARC (System for Observing Play and Recreation in Communities). Prev. Med. (Balt.) 2016, 86, 153–166. [Google Scholar] [CrossRef] [Green Version]
- De Vries, S.; Verheij, R.A.; Groenewegen, P.P.; Spreeuwenberg, P. Natural environments—Healthy environments? An exploratory analysis of the relationship between greenspace and health. Environ. Plan. A 2003, 35, 1717–1731. [Google Scholar] [CrossRef] [Green Version]
- Paquet, C.; Orschulok, T.P.; Coffee, N.T.; Howard, N.J.; Hugo, G.; Taylor, A.W.; Adams, R.J.; Daniel, M. Are accessibility and characteristics of public open spaces associated with a better cardiometabolic health? Landsc. Urban Plan. 2013, 118, 70–78. [Google Scholar] [CrossRef]

{kind=link}
| Quartiles of Green Space Density (within 500 m) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Individual Characteristics | Total | Q1 (High) | Q2 | Q3 | Q4 (Low) | |||||
| Age 1 (years) | 56 | 15 | 56 | 16 | 56 | 14.75 | 56 | 14.75 | 56 | 15 |
| Sex 2 (female) | 911 | 56.06% | 234 | 57.64% | 230 | 56.65% | 225 | 55.42% | 222 | 54.55% |
| Migration status 2 | 315 | 19.38% | 80 | 19.70% | 84 | 20.69% | 81 | 19.95% | 70 | 17.20% |
| Obesity 2 | 462 | 28.43% | 120 | 29.56% | 123 | 30.30% | 110 | 27.09% | 109 | 26.78% |
| Hypertension 2 | 412 | 25.35% | 105 | 25.86% | 93 | 22.91% | 110 | 27.09% | 104 | 25.55% |
| High cholesterol 2 | 502 | 30.89% | 116 | 28.57% | 119 | 29.31% | 121 | 29.80% | 146 | 35.87% |
| Diabetes 2 | 137 | 8.43% | 28 | 6.90% | 44 | 10.84% | 32 | 7.88% | 33 | 8.11% |
| Population density 1 (pop/km2) | 30,784 | 23,067 | 27,333 | 28,610 | 28,391 | 20,360 | 29,604 | 21,766 | 36,840 | 20,643 |
| Socioeconomic status index 1 | −0.37 | 1.24 | −0.40 | 0.81 | −0.44 | 0.90 | −0.42 | 0.94 | 0.17 | 1.93 |
| 300 m | 500 m | 1000 m | 1500 m | |||||
|---|---|---|---|---|---|---|---|---|
| Green Spaces | OR 1 | CI 95% 2 | OR | CI 95% | OR | CI 95% | OR | CI 95% |
| Obesity | ||||||||
| Q1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | ||||
| Q2 | 1.05 | (0.76–1.43) | 1.05 | (0.77–1.44) | 0.95 | (0.69–1.29) | 1.14 | (0.84–1.56) |
| Q3 | 1.08 | (0.79–1.48) | 0.89 | (0.65–1.22) | 0.91 | (0.67–1.25) | 1.20 | (0.88–1.65) |
| Q4 (Low) | 1.00 | (0.72–1.38) | 1.09 | (0.78–1.52) | 0.95 | (0.67–1.34) | 1.05 | (0.73–1.52) |
| Hypertension | ||||||||
| Q1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | ||||
| Q2 | 0.98 | (0.71–1.37) | 0.84 | (0.60–1.18) | 0.89 | (0.64–1.25) | 1.32 | (0.93–1.85) |
| Q3 | 1.01 | (0.72–1.40) | 1.06 | (0.76–1.47) | 1.05 | (0.76–1.46) | 1.38 | (0.98–1.95) |
| Q4 (Low) | 0.92 | (0.65–1.30) | 1.03 | (0.72–1.46) | 1.06 | (0.74–1.53) | 1.20 | (0.81–1.79) |
| High Cholesterol | ||||||||
| Q1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | ||||
| Q2 | 1.28 | (0.93–1.77) | 1.05 | (0.76–1.44) | 1.11 | (0.80–1.53) | 0.90 | (0.65–1.24) |
| Q3 | 1.32 | (0.95–1.83) | 1.06 | (0.77–1.46) | 0.97 | (0.70–1.33) | 1.04 | (0.75–1.43) |
| Q4 (Low) | 1.46 | (1.05–2.03) | 1.47 | (1.05–2.06) | 1.55 | (1.10–2.18) | 1.20 | (0.83–1.71) |
| Diabetes | ||||||||
| Q1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | ||||
| Q2 | 1.61 | (0.98–2.64) | 1.67 | (1.01–2.76) | 1.01 | (0.62–1.67) | 1.15 | (0.70–1.87) |
| Q3 | 1.15 | (0.68–1.95) | 1.15 | (0.68–1.96) | 1.05 | (0.64–1.72) | 0.97 | (0.58–1.61) |
| Q4 (Low) | 1.09 | (0.63–1.90) | 1.44 | (0.82–2.52) | 0.99 | (0.56–1.75) | 1.00 | (0.55–1.83) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plans, E.; Gullón, P.; Cebrecos, A.; Fontán, M.; Díez, J.; Nieuwenhuijsen, M.; Franco, M. Density of Green Spaces and Cardiovascular Risk Factors in the City of Madrid: The Heart Healthy Hoods Study. Int. J. Environ. Res. Public Health 2019, 16, 4918. https://doi.org/10.3390/ijerph16244918
Plans E, Gullón P, Cebrecos A, Fontán M, Díez J, Nieuwenhuijsen M, Franco M. Density of Green Spaces and Cardiovascular Risk Factors in the City of Madrid: The Heart Healthy Hoods Study. International Journal of Environmental Research and Public Health. 2019; 16(24):4918. https://doi.org/10.3390/ijerph16244918
Chicago/Turabian StylePlans, Elena, Pedro Gullón, Alba Cebrecos, Mario Fontán, Julia Díez, Mark Nieuwenhuijsen, and Manuel Franco. 2019. "Density of Green Spaces and Cardiovascular Risk Factors in the City of Madrid: The Heart Healthy Hoods Study" International Journal of Environmental Research and Public Health 16, no. 24: 4918. https://doi.org/10.3390/ijerph16244918
APA StylePlans, E., Gullón, P., Cebrecos, A., Fontán, M., Díez, J., Nieuwenhuijsen, M., & Franco, M. (2019). Density of Green Spaces and Cardiovascular Risk Factors in the City of Madrid: The Heart Healthy Hoods Study. International Journal of Environmental Research and Public Health, 16(24), 4918. https://doi.org/10.3390/ijerph16244918