Public Awareness of Tuberculosis in Southeast China: A Population-Based Study

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area and Population
2.2. Study Design
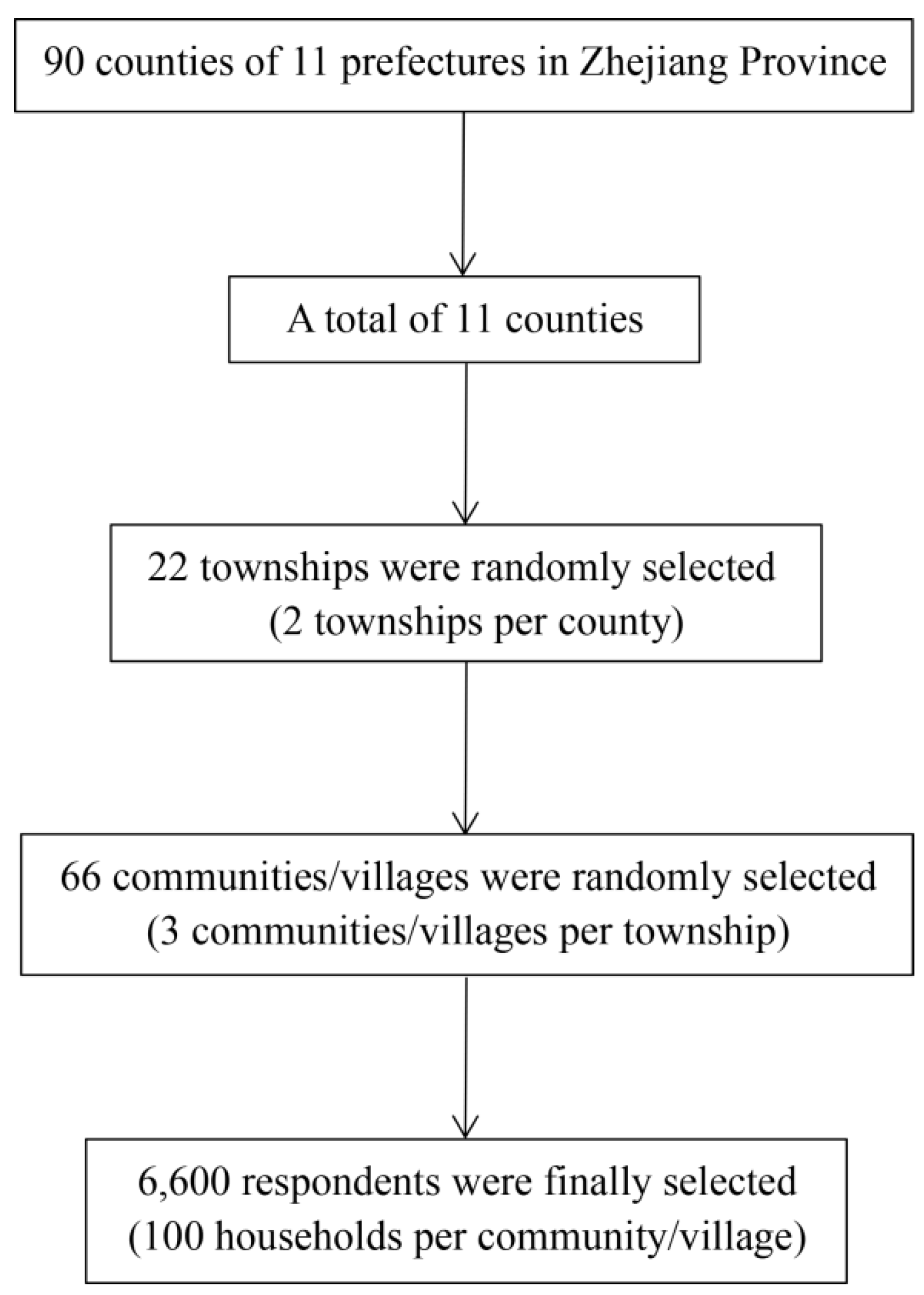
2.2.1. Sampling and Participants
2.2.2. Data Collection and Quality Control
2.2.3. Data Analysis
2.3. Ethical Considerations
3. Results
3.1. Socio-Demographic Characteristics
3.2. General Awareness of TB
3.3. Awareness of Key Information about TB
3.4. Awareness of Key Information about TB among People with Different Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2018. Available online: http://www.who.int/tb/publications/global_report/en/ (accessed on 9 August 2019).
- Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J. Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data. Lancet 2006, 367, 1747–1757. [Google Scholar] [CrossRef]
- Miller, T.L.; McNabb, S.J.; Hilsenrath, P.; Pasipanodya, J.; Weis, S.E. Personal and societal health quality lost to tuberculosis. PLoS ONE 2009, 4, e5080. [Google Scholar] [CrossRef] [PubMed]
- China’s Ministry of Health, Beijing, China. National “Thirteenth Five-Year” Plan for Tuberculosis Prevention and Control. Available online: http://www.gov.cn/zhengce/content/2017-02/16/content_5168491.htm (accessed on 9 August 2019).
- Ilic, M.; Kuruc, V.; Pavlovic, S.; Kopitovic, I.; Kasikovic-Lecic, S.; Zvezdin, B.; Zaric, B.; Kojicic, M. Tuberculosis in a developing country—How much patients know about disease. Cent. Eur. J. Med. 2012, 7, 249–257. [Google Scholar] [CrossRef][Green Version]
- Perriot, J.; Underner, M.; Peiffer, G. Tuberculosis and tobacco smoking. J. Tuberc. 2018, 1, 1–4. [Google Scholar]
- Cegielski, J.P.; McMurray, D.N. The relationship between malnutrition and tuberculosis: Evidence from studies in humans and experimental animals. Int. J. Tuberc. Lung Dis. 2004, 8, 286–298. [Google Scholar]
- Lienhardt, C. From exposure to disease: The role of environmental factors in susceptibility to and development of tuberculosis. Epidemiol. Rev. 2001, 23, 288–301. [Google Scholar] [CrossRef]
- Lu, S.H.; Tian, B.C.; Kang, X.P.; Zhang, W.; Meng, X.P.; Zhang, J.B.; Lo, S.K. Public awareness of tuberculosis in China: A national survey of 69 253 subjects. Int. J. Tuberc. Lung Dis. 2009, 13, 1493–1499. [Google Scholar]
- Tolossa, D.; Medhin, G.; Legesse, M. Community knowledge, attitude, and practices towards tuberculosis in Shinile town, Somali regional state, eastern Ethiopia: A cross-sectional study. BMC Public Health 2014, 14, 804. [Google Scholar] [CrossRef]
- Ma, Y.; Liu, Y.H.; Du, J.; Tan, S.Y.; Fu, Y.Y.; Ma, L.P.; Zhang, L.Y.; Liu, F.Y.; Hu, D.Y.; Zhang, Y.L. Survey on awareness of key message on tuberculosis prevention and control among tuberculosis patients. Chin. J. Antituberc. 2015, 37, 1042–1048. (In Chinese) [Google Scholar]
- Wang, J.; Lv, Q.; Chen, M.T.; Xia, Y.Y.; Chen, J.; Zhao, F.; Zhang, C.Y.; Meng, Q.L. The national awareness survey on key TB message in 2015. Chin. J. Antituberc. 2017, 39, 282–288. (In Chinese) [Google Scholar]
- Huang, Y.; Zhong, J.M.; Chen, B.; Chen, S.H.; Qiu, X.; Wang, X.M. Epidemiological characteristics of tuberculosis in Zhejiang Province, 2010. Dis. Surveill. 2011, 26, 601–603. (In Chinese) [Google Scholar]
- Zhang, M.W.; Chen, S.H.; Zhong, J.M.; Chen, B.; Peng, Y.; He, T.N.; Wang, X.M. Awareness of key knowledge about tuberculosis and its major influencing factors among general population in Zhejiang province. Chin. J. Public Health 2017, 33, 1607–1611. (In Chinese) [Google Scholar]
- Zhejiang Provincial Bureau of Statistics. Zhejiang Statistical Yearbook. Available online: http://tjj.zj.gov.cn/col/col1525563/index.html (accessed on 10 August 2019).
- Chen, W.; Xia, Y.Y.; Li, T.; Chen, H. Analysis for the global and China TB epidemic situation in 2015. J. Tuberc. Lung Health 2016, 5, 32–36. (In Chinese) [Google Scholar]
- Huang, Y.; Zhong, J.M.; Chen, S.H.; Chen, B.; Wang, X.M. Investigation analysis on public awareness of tuberculosis knowledge in Zhejiang province, 2010. Chin. J. Prev. Med. 2012, 46, 352–354. (In Chinese) [Google Scholar]
- Daniel, W. Biostatistics: A Foundation for Analysis in the Health Science, 4th ed.; Wiley: New York, NY, USA, 1987; pp. 155–156. [Google Scholar]
- Sudha, G.; Nirupa, C.; Rajasakthivel, M.; Sivasusbramanian, S.; Sundaram, V.; Bhatt, S.; Subramaniam, K.; Thiruvalluvan, E.; Mathew, R.; Renu, G.; et al. Factors influencing the care-seeking behaviour of chest symptomatic: A community-based study involving rural and urban population in Tamil Nadu, South India. Trop. Med. Int. Health 2003, 8, 336–341. [Google Scholar] [CrossRef]
- Hoa, N.P.; Diwan, V.K.; Co, N.V.; Thorson, A.E. Knowledge about tuberculosis and its treatment among new pulmonary TB patients in the north and central regions of Vietnam. Int. Tuberc. Lung Dis. 2004, 8, 603–608. [Google Scholar]
- Wan, Y. Effect evaluation on tuberculosis health education intervention among middle school students in Tianjin. Chin. J. Sch. Health 2014, 35, 190–192. (In Chinese) [Google Scholar]
- Wang, Y.; Hu, Z.P. Survey on awareness of the knowledge about TB among middle school students in Shenzhen City. Chin. J. Health Educ. 2010, 26, 516–518. (In Chinese) [Google Scholar]
- Ma, E.; Ren, L.; Wang, W.; Takahashi, H.; Wagatsuma, Y.; Ren, Y.; Gao, F.; Gao, F.; Wang, W.; Bi, L. Demographic and socioeconomic disparity in knowledge about tuberculosis in Inner Mongolia, China. J. Epidemiol. 2015, 25, 312–320. [Google Scholar] [CrossRef]
- Strand, M.A.; Duan, X.; Johnson, R.; Li, Y. Social determinants of delayed diagnosis of tuberculosis in a north China urban setting. Int. Q. Community Health Educ. 2010, 31, 279–290. [Google Scholar] [CrossRef]
- Liu, H.; Li, M.; Jin, M.; Jing, F.; Wang, H.; Chen, K. Public awareness of three major infectious diseases in rural Zhejiang province, China: A cross-sectional study. BMC Infect. Dis. 2013, 13, 192. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, L.X.; Cheng, J.; Meng, Q.L.; Zhang, H. Investigation on the awareness of core information among close contacts of tuberculosis patients. Chin. J. Antituberc. 2015, 37, 1035–1041. (In Chinese) [Google Scholar]
- Chen, F.F.; Feng, X.L.; Chen, W. Investigation and analysis on knowledge rate of tuberculosis control in Guizhou province. Mod. Prev. Med. 2018, 45, 3372–3375. (In Chinese) [Google Scholar]
- Marks, S.M.; Deluca, N.; Walton, W. Knowledge, attitudes and risk perceptions about tuberculosis: US national health interview survey. Int. J. Tuberc. Lung Dis. 2008, 12, 1261–1267. [Google Scholar]
- Haasnoot, P.J.; Boeting, T.E.; Kuney, M.O.; van Roosmalen, J. Knowledge, attitudes, and practice of tuberculosis among Maasai in Simanjiro District, Tanzania. Am. J. Trop. Med. Hyg. 2010, 83, 902–905. [Google Scholar] [CrossRef]
- Richard, D.T. Cough in pulmonary tuberculosis: Existing knowledge and general insights. Pulm. Pharmacol. Ther. 2019, 55, 89–94. [Google Scholar]
- Li, Y.; Li, X.; Xie, H.B.; Zhang, H.; Wang, L.X.; Jiang, S.W. Analysis on the reimbursement situation of TB treatment costs in the new rural cooperative medical system. Chin. J. Antituberc. 2010, 32, 685–689. (In Chinese) [Google Scholar]
- Wang, J.M.; Yang, F.; Shen, H.B.; Xu, B. Gender difference in knowledge of tuberculosis and associated health-care seeking behaviors: A cross-sectional study in a rural area of China. BMC Public Health 2008, 8, 354. [Google Scholar] [CrossRef]
- Chen, W.; Xia, Y.; Li, X.; Zhou, L.; Li, C.; Wan, K.; Cheng, S. A tuberculosis outbreak among senior high school students in China in 2011. J. Int. Med. Res. 2012, 40, 1830–1839. [Google Scholar] [CrossRef]
- Menzies, D.; Joshi, R.; Pai, M. Risk of tuberculosis infection and disease associated with work in health care settings. Int. J. Tuberc. Lung Dis. 2007, 11, 593–605. [Google Scholar]
- Chen, B.; Wang, X.M.; Zhong, J.M.; Chen, S.H.; Wu, B.B.; Yeh, H.C.; Jiang, Z.G.; Wang, Z.T.; Gu, H.; Jiang, J.J. Tuberculosis among healthcare workers in southeastern China: A retrospective study of 7-year surveillance data. Int. J. Environ. Res. Public Health 2014, 11, 12042–12052. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.Q. A Study on the Basic Medical Insurance System for Urban Residents in Zhejiang Province; Zhejiang University of Finance and Economics: Hangzhou, China, 2012. [Google Scholar]
- Fan, H.; Yan, Q.; Coyte, P.C.; Yu, W. Does public health insurance coverage lead to better health outcomes? Evidence from Chinese adults. Inquiry 2019, 56, 1–10. [Google Scholar]


{kind=link}
| Characteristic | Number | Percentage (%) |
|---|---|---|
| Sex | ||
| Male | 3323 | 46.32 |
| Female | 3851 | 53.68 |
| Age groups, years | ||
| 12–20 | 307 | 4.28 |
| 21–30 | 709 | 9.88 |
| 31–40 | 1071 | 14.93 |
| 41–50 | 1531 | 21.34 |
| 51–60 | 1753 | 24.44 |
| >60 | 1803 | 25.13 |
| Residence | ||
| Urban | 3097 | 43.17 |
| Rural | 4077 | 56.83 |
| Education | ||
| Illiterate | 817 | 11.39 |
| Primary School | 1786 | 24.9 |
| Secondary school 1 | 2328 | 32.45 |
| High school 2 | 999 | 13.93 |
| Junior college | 561 | 7.82 |
| University | 683 | 9.52 |
| Occupation | ||
| Government staff | 323 | 4.5 |
| Health care workers | 153 | 2.13 |
| Teachers | 223 | 3.11 |
| Professional technicians | 585 | 8.15 |
| Business/Service personnel | 933 | 13.01 |
| Industrial workers | 960 | 13.38 |
| Farmers | 2679 | 37.34 |
| Students | 320 | 4.46 |
| Unemployed | 998 | 13.91 |
| Health insurance | ||
| Medical insurance A 3 | 2571 | 35.84 |
| Medical insurance B 4 | 4317 | 60.18 |
| Commercial insurance | 56 | 0.78 |
| Self-pay | 125 | 1.74 |
| Others | 105 | 1.46 |
| Total | 7174 | 100 |
| Characteristic | Heard of TB | χ2 | P Value | |
|---|---|---|---|---|
| Yes (n, %) | No (n, %) | |||
| Sex | 2.43 | 0.119 | ||
| Male | 2761 (83.09) | 562 (16.91) | ||
| Female | 3252 (84.45) | 599 (15.55) | ||
| Age groups, years | 177.87 | <0.001 | ||
| 12–20 | 226 (73.62) | 81 (26.38) | ||
| 21–30 | 632 (89.14) | 77 (10.86) | ||
| 31–40 | 984 (91.88) | 87 (8.12) | ||
| 41–50 | 1337 (87.33) | 194 (12.67) | ||
| 51–60 | 1457 (83.11) | 296 (16.89) | ||
| >60 | 1377 (76.37) | 426 (23.63) | ||
| Residence | 24.32 | <0.001 | ||
| Urban | 2672 (86.28) | 425 (13.72) | ||
| Rural | 3341 (81.95) | 736 (18.05) | ||
| Education | 355.00 | <0.001 | ||
| Illiterate | 550 (67.32) | 267 (32.68) | ||
| Primary School | 1403 (78.56) | 383 (21.44) | ||
| Secondary school 1 | 1970 (84.62) | 358 (15.38) | ||
| High school 2 | 907 (90.79) | 92 (9.21) | ||
| Junior college | 527 (93.94) | 34 (6.06) | ||
| University | 656 (96.05) | 27 (3.95) | ||
| Occupation | 221.87 | <0.001 | ||
| Government staff | 308 (95.36) | 15 (4.64) | ||
| Health care workers | 148 (96.73) | 5 (3.27) | ||
| Teachers | 216 (96.86) | 7 (3.14) | ||
| Professional technicians | 538 (91.97) | 47 (8.03) | ||
| Business/Service personnel | 821 (88.00) | 112 (12.00) | ||
| Industrial workers | 847 (88.23) | 113 (11.77) | ||
| Farmers | 2102 (78.46) | 577 (21.54) | ||
| Students | 240 (75.00) | 80 (25.00) | ||
| Unemployed | 793 (79.46) | 205 (20.54) | ||
| Total | 6013 (83.82) | 1161 (16.18) | ||
| Characteristic | Total Answers (N) | Correct Answers (n) | Percentage (%) |
|---|---|---|---|
| Sex | |||
| Male | 16,615 | 7922 | 47.68 |
| Female | 19,255 | 9310 | 48.35 |
| Age groups, years | |||
| 12–20 | 1535 | 572 | 37.26 |
| 21–30 | 3545 | 1789 | 50.47 |
| 31–40 | 5355 | 3042 | 56.81 |
| 41–50 | 7655 | 4039 | 52.76 |
| 51–60 | 8765 | 4185 | 47.75 |
| >60 | 9015 | 3605 | 39.99 |
| Residence | |||
| Urban | 15,485 | 7682 | 49.61 |
| Rural | 20,385 | 9313 | 45.69 |
| Education | |||
| Illiterate | 4085 | 1223 | 29.94 |
| Primary school | 8930 | 3665 | 41.04 |
| Secondary school 1 | 11,640 | 5703 | 48.99 |
| High school 2 | 4995 | 2782 | 55.70 |
| Junior college | 2805 | 1671 | 59.57 |
| University | 3415 | 2188 | 64.07 |
| Occupation | |||
| Unemployed | 4990 | 2013 | 40.34 |
| Government staff | 1615 | 1007 | 62.35 |
| Health care workers | 765 | 606 | 79.22 |
| Teachers | 1115 | 730 | 65.47 |
| Professional technicians | 2925 | 1601 | 54.74 |
| Business/Service personnel | 4665 | 2389 | 51.21 |
| Industrial workers | 4800 | 2405 | 50.10 |
| Farmers | 13,395 | 5873 | 43.84 |
| Students | 1600 | 608 | 38.00 |
| Health insurance | |||
| Medical insurance A 3 | 12,855 | 7525 | 58.54 |
| Medical insurance B 4 | 21,585 | 9115 | 42.23 |
| Commercial insurance | 280 | 133 | 47.50 |
| Self-pay | 625 | 215 | 34.40 |
| Others | 525 | 244 | 46.48 |
| Total | 35,870 | 17,232 | 48.04 |
| Characteristic | The Number of Correctly Answered Key Information Questions | χ2 | P | |||||
|---|---|---|---|---|---|---|---|---|
| 0 (n, %) | 1 (n, %) | 2 (n, %) | 3 (n, %) | 4 (n, %) | 5 (n, %) | |||
| Sex | 5.35 | 0.375 | ||||||
| Male | 31 (41.89) | 211 (44.23) | 461 (46.24) | 733 (48.16) | 715 (45.69) | 346 (43.96) | ||
| Female | 43 (58.11) | 266 (55.77) | 536 (53.76) | 789 (51.84) | 850 (54.31) | 441 (56.04) | ||
| Residence | 19.11 | 0.002 | ||||||
| Urban | 34 (45.95) | 214 (44.86) | 419 (42.03) | 732 (48.09) | 646 (41.28) | 370 (47.01) | ||
| Rural | 40 (54.05) | 263 (55.14) | 578 (57.97) | 790 (51.91) | 919 (58.72) | 417 (52.99) | ||
| Age groups, years | 128.36 | <0.001 | ||||||
| 12–20 | 5 (6.76) | 23 (4.82) | 37 (3.71) | 41 (2.67) | 38 (2.43) | 40 (5.08) | ||
| 21–30 | 12 (16.22) | 49 (10.27) | 83 (8.32) | 142 (9.33) | 157 (10.03) | 104 (13.21) | ||
| 31–40 | 9 (12.16) | 61 (12.79) | 147 (14.74) | 261 (17.15) | 286 (18.27) | 152 (19.31) | ||
| 41–50 | 13 (17.57) | 76 (15.93) | 207 (20.76) | 383 (25.16) | 345 (22.04) | 204 (25.92) | ||
| 51–60 | 12 (16.22) | 122 (25.58) | 237 (23.77) | 381 (25.03) | 414 (26.45) | 158 (20.08) | ||
| >60 | 23 (31.08) | 146 (30.61) | 286 (28.69) | 314 (20.63) | 325 (20.77) | 129 (16.39) | ||
| Education | 255.93 | <0.001 | ||||||
| Illiterate | 12 (16.22) | 80 (16.77) | 139 (13.94) | 112 (7.36) | 96 (6.13) | 29 (3.68) | ||
| Primary School | 22 (29.73) | 143 (29.98) | 274 (27.48) | 324 (21.29) | 329 (21.02) | 138 (17.53) | ||
| Secondary school 1 | 21 (28.38) | 139 (29.14) | 317 (31.80) | 537 (35.28) | 521 (33.29) | 247 (31.39) | ||
| High school 2 | 8 (10.81) | 63 (13.21) | 117 (11.74) | 250 (16.43) | 265 (16.93) | 135 (17.15) | ||
| Junior college | 7 (9.46) | 19 (3.98) | 83 (8.32) | 130 (8.54) | 144 (9.20) | 104 (13.21) | ||
| University | 4 (5.41) | 33 (6.92) | 67 (6.72) | 169 (11.10) | 211 (13.48) | 134 (17.03) | ||
| Occupation | 285.84 | <0.001 | ||||||
| Government staff | 3 (4.05) | 13 (2.73) | 33 (3.31) | 89 (5.85) | 94 (6.01) | 57 (7.24) | ||
| Health care workers | 0 (0.00) | 4 (0.84) | 4 (0.40) | 25 (1.64) | 51 (3.26) | 63 (8.01) | ||
| Teachers | 1 (1.35) | 4 (0.84) | 28 (2.81) | 50 (3.29) | 80 (5.11) | 40 (5.08) | ||
| Professional technicians | 6 (8.11) | 53 (11.11) | 65 (6.52) | 153 (10.05) | 126 (8.05) | 91 (11.56) | ||
| Business/Service personnel | 12 (16.22) | 52 (10.90) | 138 (13.84) | 238 (15.64) | 218 (13.93) | 95 (12.07) | ||
| Industrial workers | 5 (6.76) | 65 (13.63) | 163 (16.35) | 216 (14.19) | 194 (12.40) | 118 (14.99) | ||
| Farmers | 25 (33.78) | 173 (36.27) | 364 (36.51) | 513 (33.71) | 597 (38.15) | 209 (26.56) | ||
| Students | 8 (10.81) | 21 (4.40) | 43 (4.31) | 41 (2.69) | 47 (3.00) | 38 (4.83) | ||
| Unemployed | 14 (18.92) | 92 (19.29) | 159 (15.95) | 197 (12.94) | 158 (10.10) | 76 (9.66) | ||
| Total (N) | 74 | 477 | 997 | 1522 | 1565 | 787 | ||
| Key Information Questions | Number of Respondents Who Answered (N) | Number of Respondents Who Answered Correctly (n) | Percentage (%) |
|---|---|---|---|
| TB can be transmitted through a close cough, sneezing, etc. | 6013 | 4857 | 80.77 |
| TB should be suspected if a cough and expectoration persist for more than two weeks. | 6013 | 2168 | 36.06 |
| TB should be treated in designated TB hospitals | 6013 | 4026 | 66.95 |
| The fees for a TB diagnosis and first-line therapeutic drugs are covered by the government | 6013 | 2284 | 37.98 |
| If standard treatment is adhered to, most cases of TB can be cured | 6013 | 4708 | 78.30 |
| Characteristic | B 1 | S.E. 2 | Wald 3 | Adjusted OR 4 (95% CI 5) | P |
|---|---|---|---|---|---|
| Residence | |||||
| Urban | Reference | ||||
| Rural | −0.31 | 0.07 | 20.17 | 0.74 (0.64–0.84) | <0.001 |
| Education | |||||
| Illiterate | Reference | ||||
| Primary school | 0.43 | 0.12 | 12.70 | 1.54 (1.22–1.96) | <0.001 |
| Secondary school 6 | 0.70 | 0.12 | 34.36 | 2.00 (1.59–2.53) | <0.001 |
| High school 7 | 0.93 | 0.13 | 48.49 | 2.54 (1.95–3.30) | <0.001 |
| Junior college | 0.98 | 0.16 | 38.95 | 2.66 (1.96–3.62) | <0.001 |
| University | 1.02 | 0.16 | 39.88 | 2.79 (2.03–3.83) | <0.001 |
| Occupation | |||||
| Unemployed | Reference | ||||
| Government staff | 0.26 | 0.16 | 2.54 | 1.30 (0.94–1.78) | 0.111 |
| Health care workers | 1.38 | 0.23 | 36.11 | 3.96 (2.53–6.20) | <0.001 |
| Teachers | 0.54 | 0.19 | 8.06 | 1.71 (1.18–2.48) | 0.005 |
| Professional technicians | −0.01 | 0.13 | 0.00 | 0.99 (0.76–1.29) | 0.959 |
| Business/Service personnel | 0.04 | 0.12 | 0.09 | 1.04 (0.83–1.30) | 0.760 |
| Industrial workers | 0.05 | 0.11 | 0.21 | 1.05 (0.84–1.32) | 0.650 |
| Farmers | 0.28 | 0.10 | 7.34 | 1.32 (1.08–1.61) | 0.007 |
| Students | 0.09 | 0.18 | 0.25 | 1.09 (0.77–1.55) | 0.617 |
| Health insurance | |||||
| Medical insurance A 8 | Reference | ||||
| Medical insurance B 9 | −0.20 | 0.08 | 7.28 | 0.82 (0.71–0.95) | 0.007 |
| Commercial insurance | −0.35 | 0.32 | 1.18 | 0.70 (0.37–1.33) | 0.277 |
| Self-pay | −0.47 | 0.26 | 3.36 | 0.62 (0.38–1.03) | 0.067 |
| Others | 0.47 | 0.27 | 3.09 | 1.60 (0.95–2.70) | 0.079 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, X.; Wang, W.; Wang, X.; Chai, C.; Liu, K.; Peng, Y.; Wang, F.; Chen, B.; Jiang, J. Public Awareness of Tuberculosis in Southeast China: A Population-Based Study. Int. J. Environ. Res. Public Health 2019, 16, 4290. https://doi.org/10.3390/ijerph16214290
Chen X, Wang W, Wang X, Chai C, Liu K, Peng Y, Wang F, Chen B, Jiang J. Public Awareness of Tuberculosis in Southeast China: A Population-Based Study. International Journal of Environmental Research and Public Health. 2019; 16(21):4290. https://doi.org/10.3390/ijerph16214290
Chicago/Turabian StyleChen, Xinyi, Wei Wang, Xiaomeng Wang, Chengliang Chai, Kui Liu, Ying Peng, Fei Wang, Bin Chen, and Jianmin Jiang. 2019. "Public Awareness of Tuberculosis in Southeast China: A Population-Based Study" International Journal of Environmental Research and Public Health 16, no. 21: 4290. https://doi.org/10.3390/ijerph16214290
APA StyleChen, X., Wang, W., Wang, X., Chai, C., Liu, K., Peng, Y., Wang, F., Chen, B., & Jiang, J. (2019). Public Awareness of Tuberculosis in Southeast China: A Population-Based Study. International Journal of Environmental Research and Public Health, 16(21), 4290. https://doi.org/10.3390/ijerph16214290