A Bespoke Social Network for Deaf Women in Ecuador to Access Information on Sexual and Reproductive Health


 ,
,  ,
, 
Abstract
:1. Introduction
2. Overview of Support Systems for SRH
3. An AI-Enhanced Social Network on SRH for Deaf Women
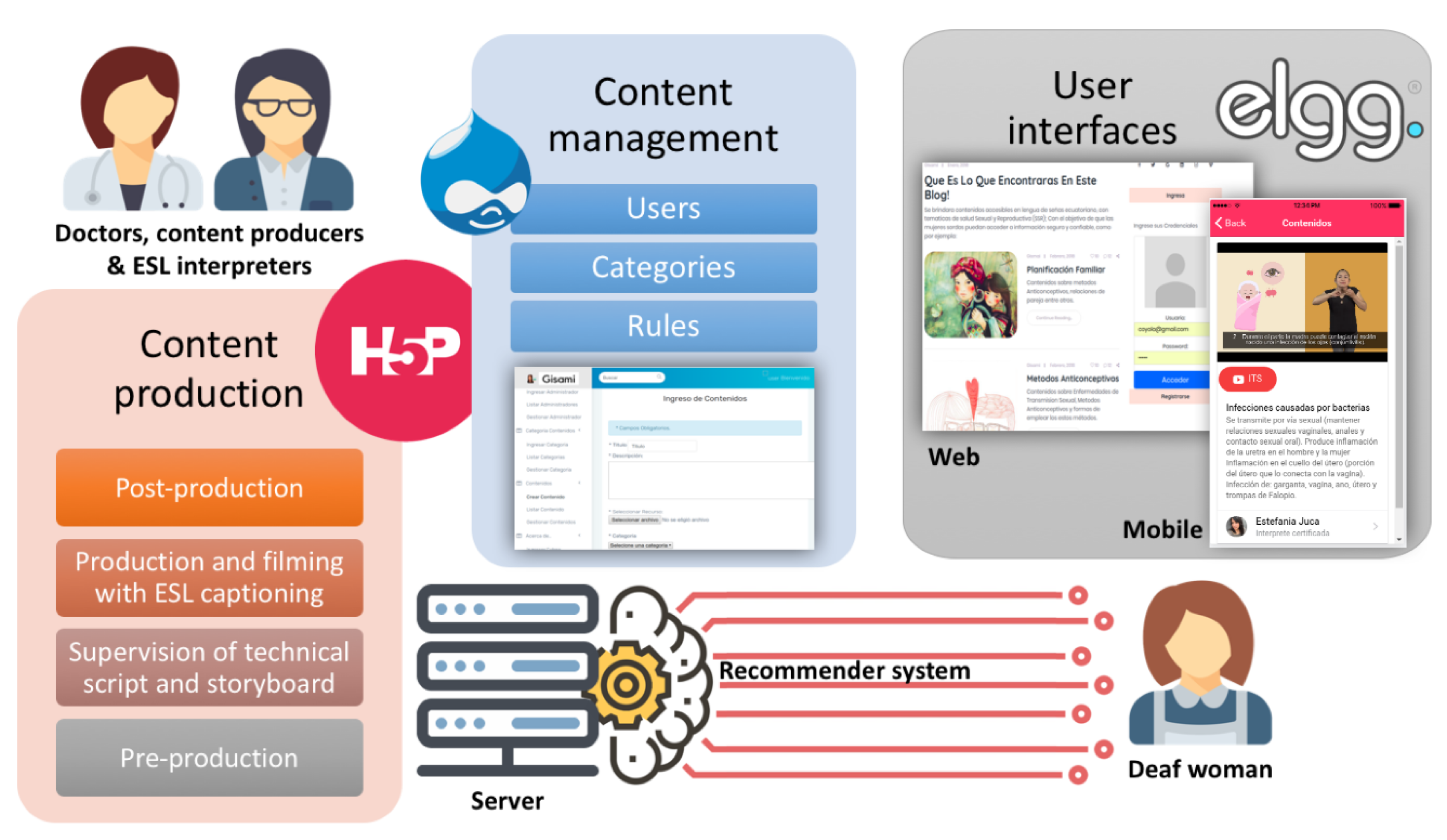
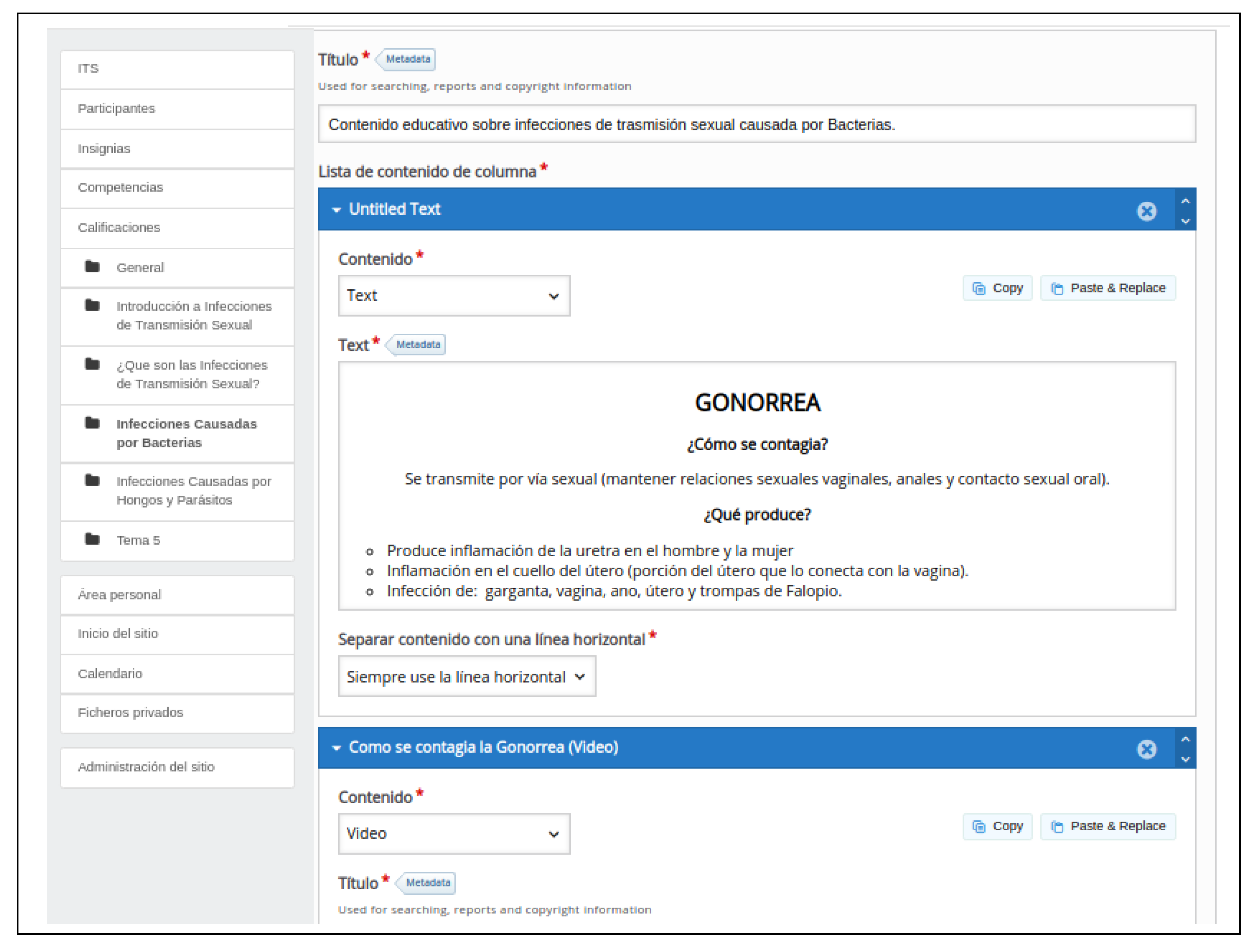
3.1. Content Creation Guidelines
- Firstly, a pre-production stage must be conducted by a multidisciplinary team of experts from areas of medicine, graphic design, education, social communication, computer science and sign language interpretation. Among other tasks, the team determines the terminology and the interpretation techniques that will be used in the new contents, and designs conceptual and graphic scripts for the subsequent stages.
- Following the pre-production, the team of experts develops storyboard notes for the illustration and animation processes. This task helps to substantiate the scripts, with a twofold objective: on the one hand, it allows supervising the sequencing of the different topics, aiming to ensure that the users will not experience any continuity gaps; on the other hand, it facilitates the identification of a coherent set of visual styles and clues.
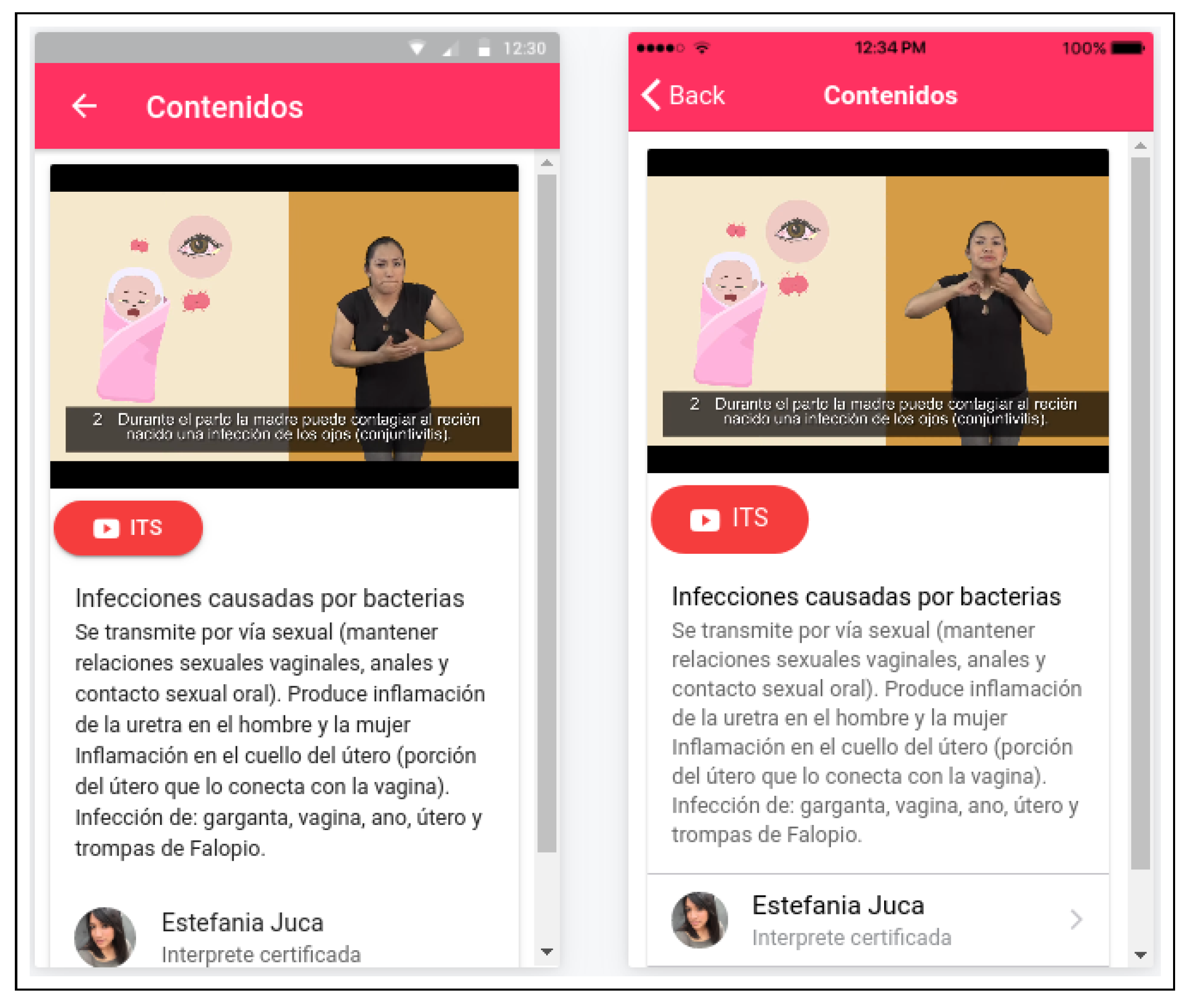
- In preparation for production and filming, proper clothing and spaces must be decided for the sign language interpreters. The design and animation process is carried out, and accessible subtitling is added to help deaf women who have post-linguistic hearing loss and are able to read text.
- Finally, the post-production stage is needed to deal with the editing and optimization of graphics and animations. The resulting materials must be evaluated by a group of deaf women, in order to check whether everything is understable for all age ranges. Only the contents that meet the proper quality and understandability levels are uploaded to the social network.
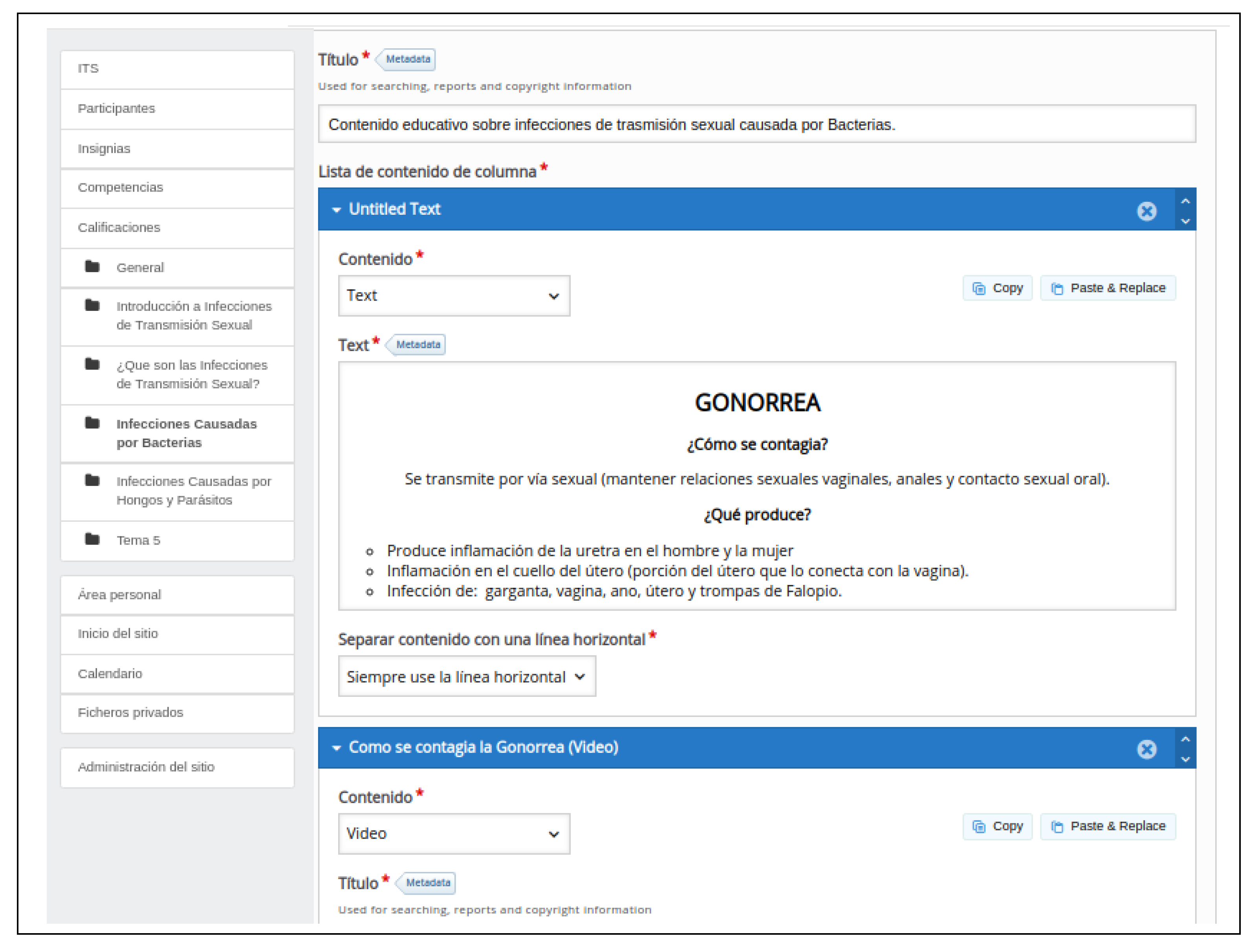
3.2. The Content Management System
- Categories: each piece of content is annotated with a number of categories, which doctors and content producers select from a purpose-made thesaurus that covers all the relevant topics in SRH, with some finer-grained detail for tags related to beauty and nutrition (see Figure 2).
- Users: each user has a profile that keeps track of her interactions with the platform as a whole (e.g., the categories she browses, the queries she types to search for content, etc.) and with each particular piece of content (e.g., her replies to expert-designed questionnaires, how much of a video she has watched, etc.). From the information so gathered, we estimate her levels of knowledge about the different categories.
- Rules: the recommender system that matches users and pieces of content is driven by a set of rules, entered and revised over time by experts. A rule may involve any arithmetic operations on conditions related to (i) the categories linked to each piece of content and (ii) the inclusion of those categories in the user profiles and the corresponding levels of knowledge.
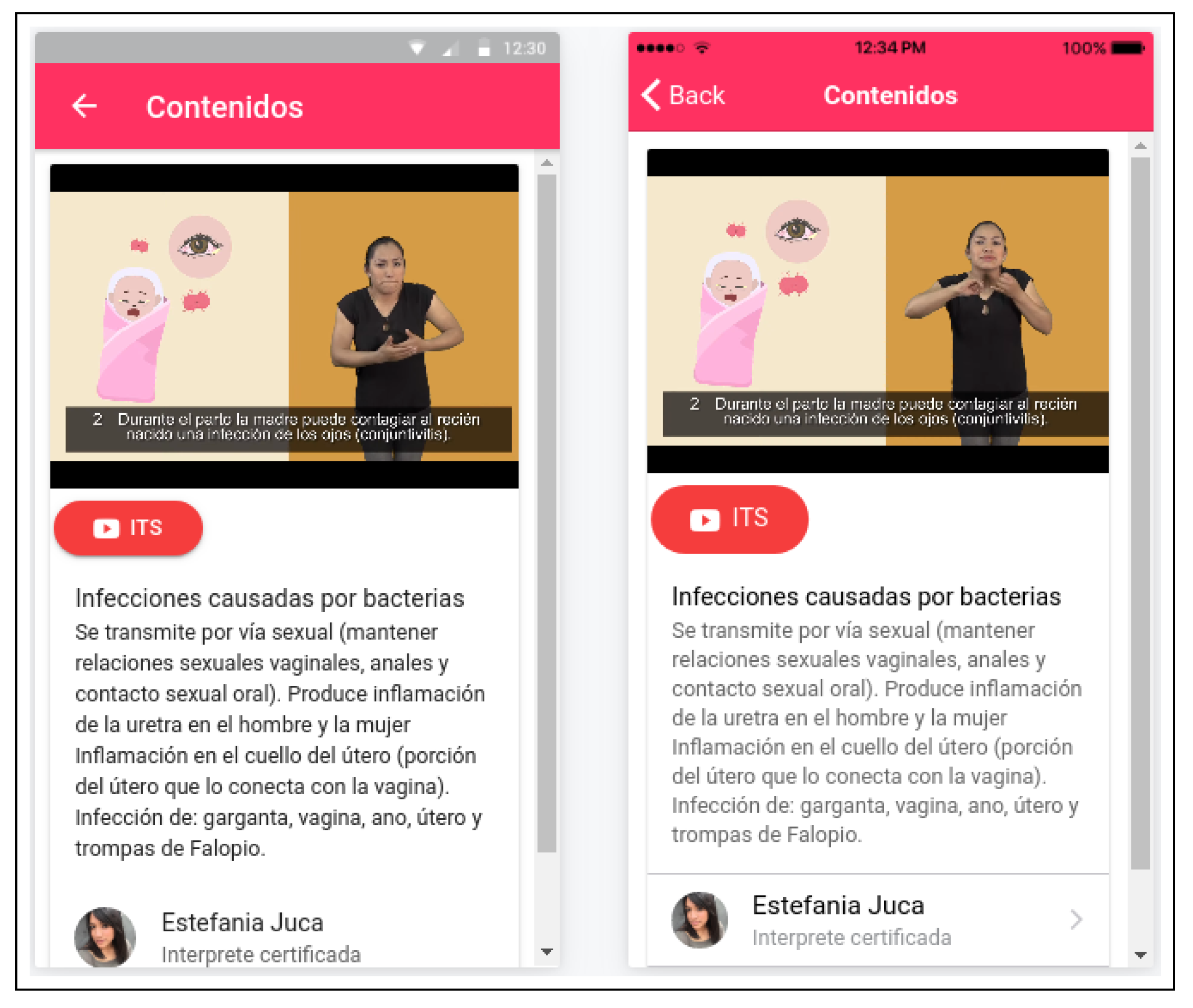
3.3. The User Interfaces
4. Quantitative Evaluation Experiments
- In the first one, in parallel with the ethnographic study of Section 3.1, we worked with 31 deaf women to assess their knowledge about the most relevant SRH topics.
- After the design and development of the social network and the creation of the first set of contents were complete (mid 2017), we offered them to a new group of 26 deaf women and three experts for evaluation.
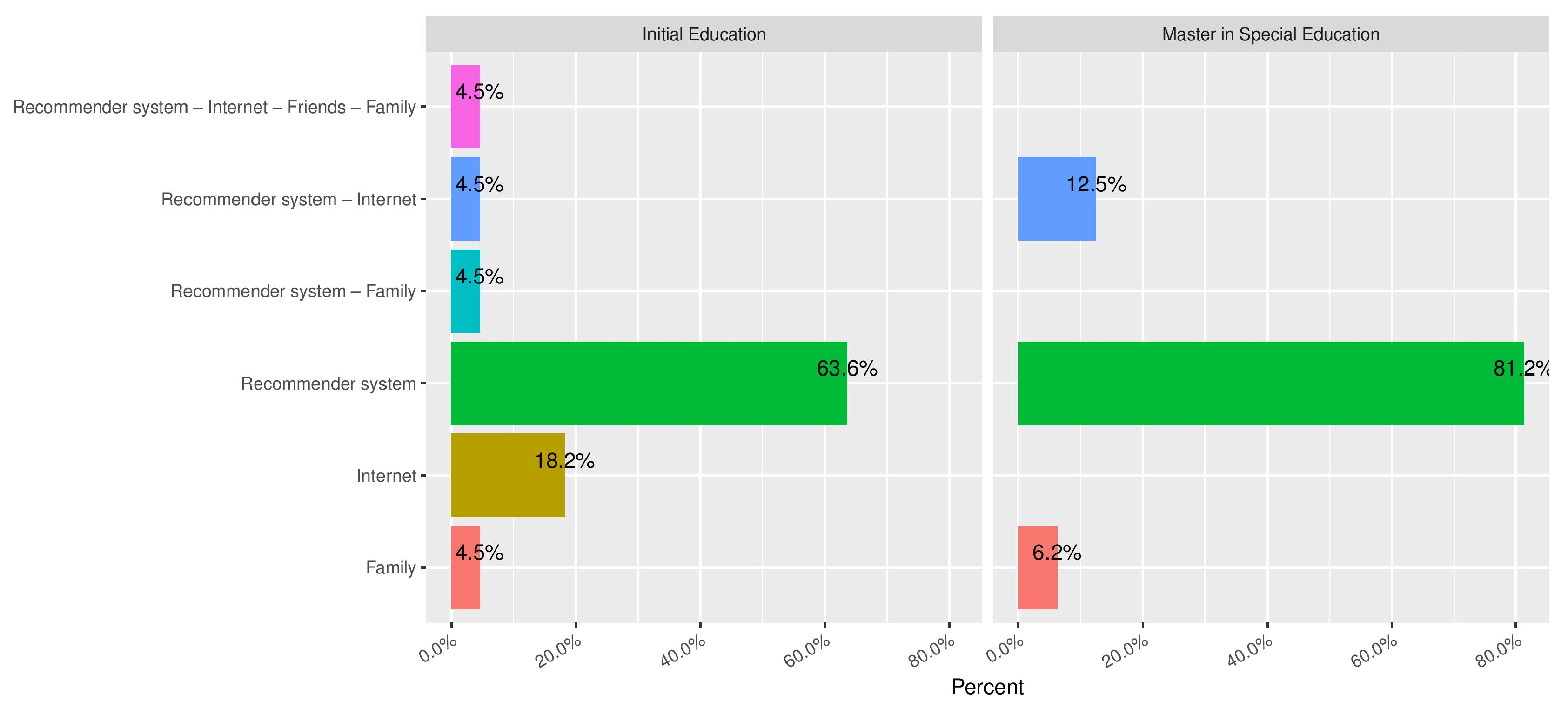
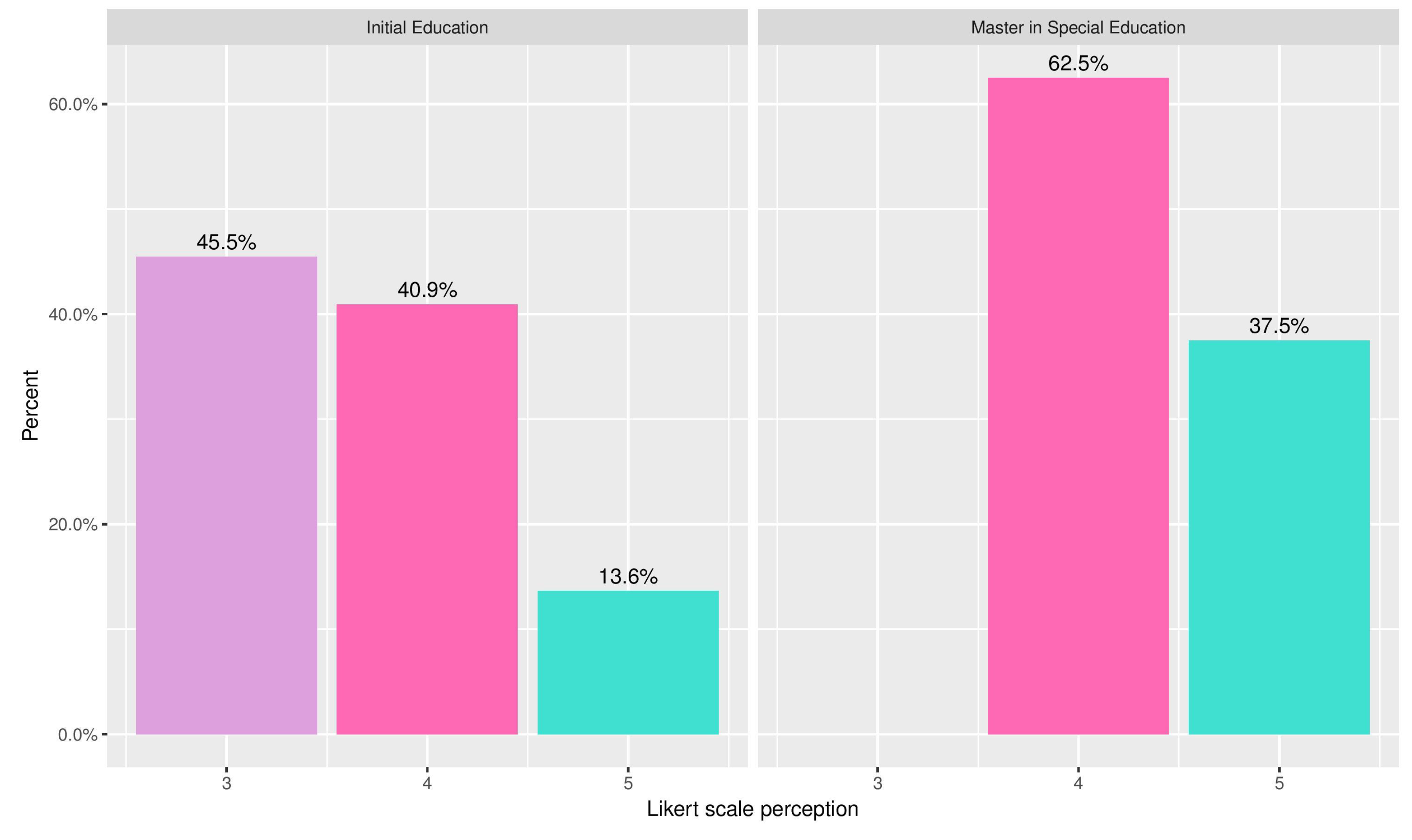
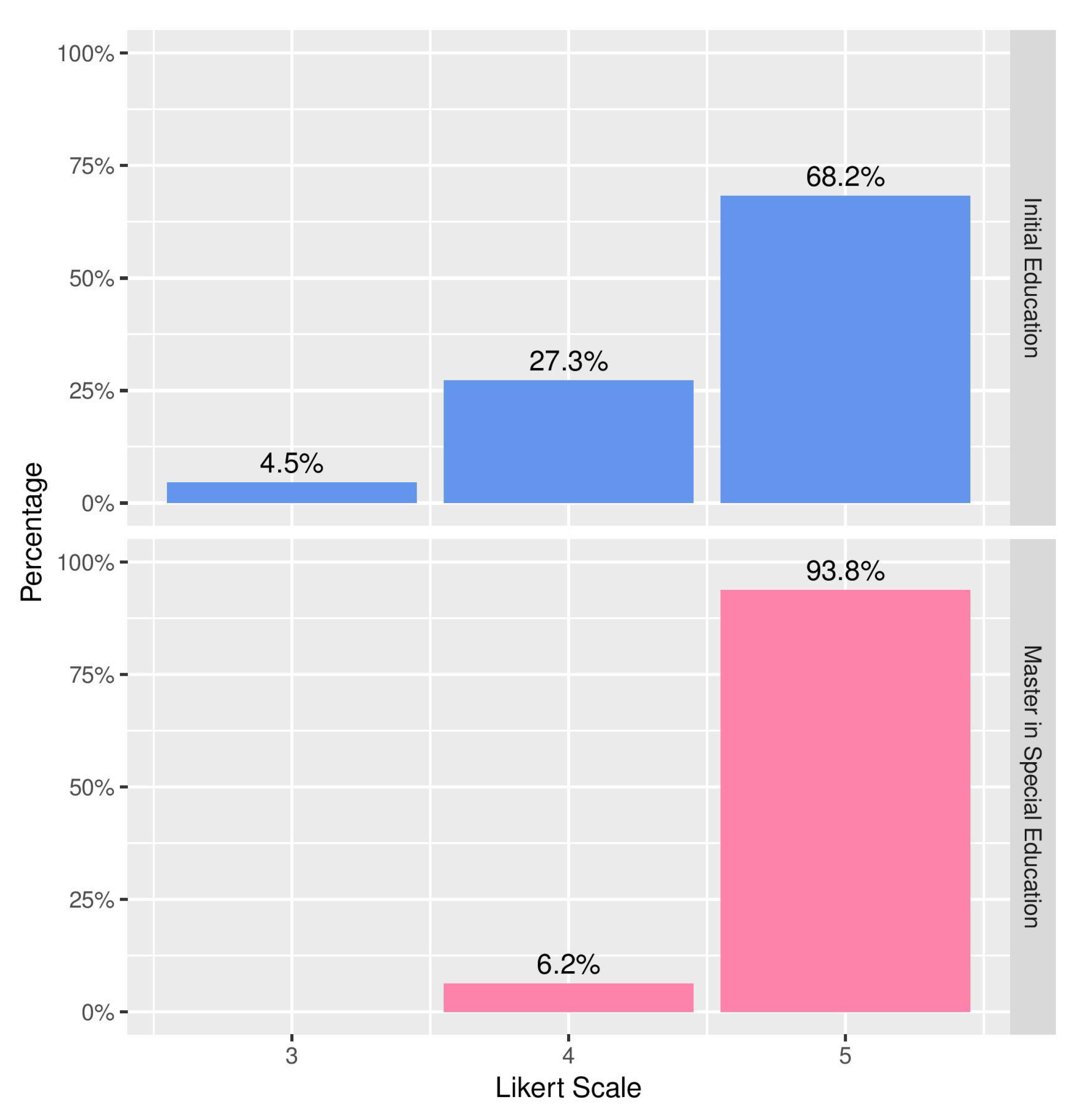
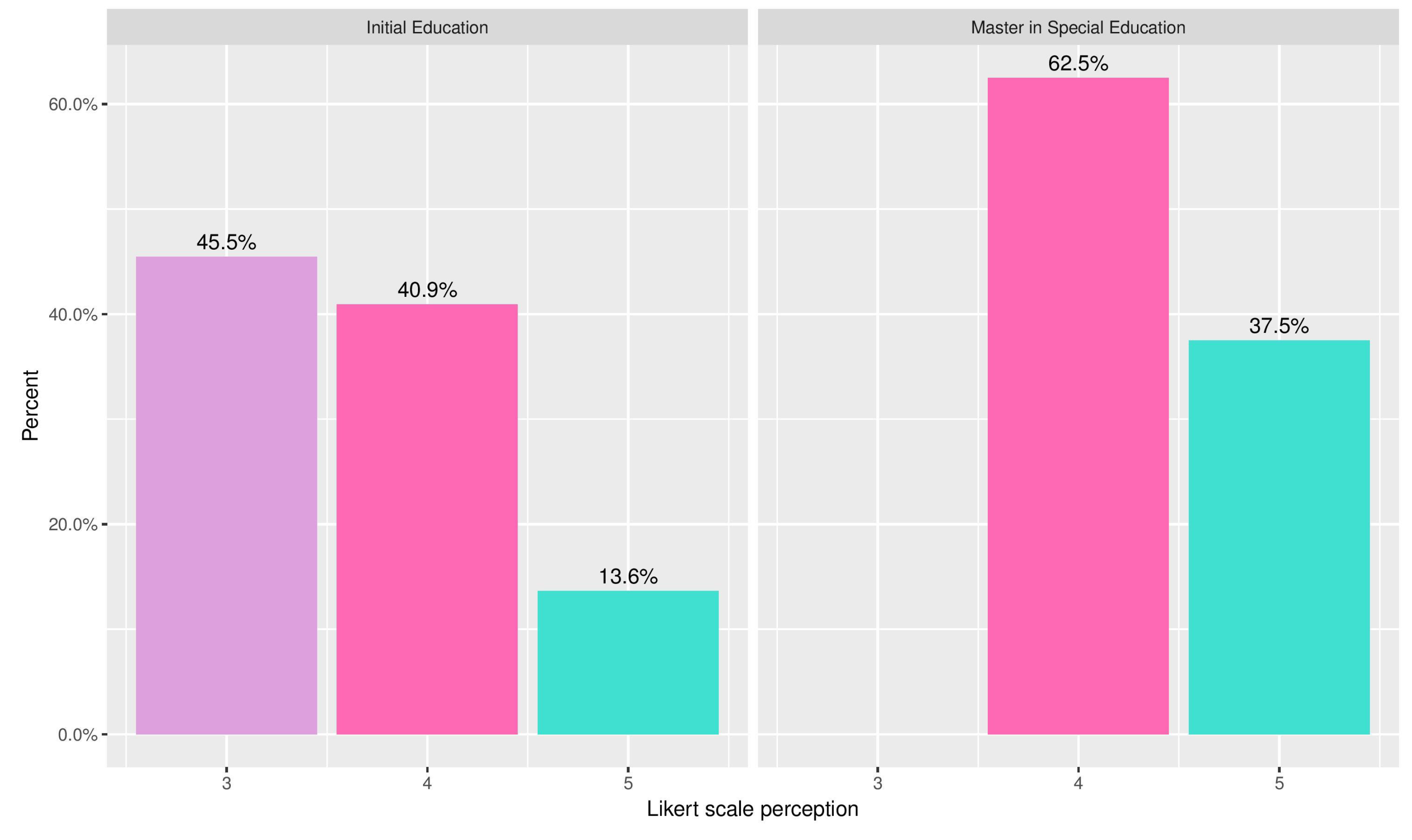
- Finally, during the first semester of 2018, we assessed the value of the recommender system with the aid of 22 students of a Bachelor Degree in Initial Education and 16 students of a Master’s Degree in Special Education.
4.1. Deaf Women’s Knowledge about SRH
- Fifteen women came from the National Federation of Deaf People in Ecuador and the Association of Deaf People from the Azuay province—the contacts were facilitated by the two key informants and representatives who had participated in the ethnographic study of Section 3.1.
- Thirteen women came from the Febres Cordero high school and the Dolores J. Torres high school, with which our institution (Universidad Politécnica Salesiana) had signed formal agreements for collaboration in areas of inclusive education.
- Three women came from the Jehovah’s Witnesses Congregation of Cuenca, that was reached through systematic searches on the Internet.
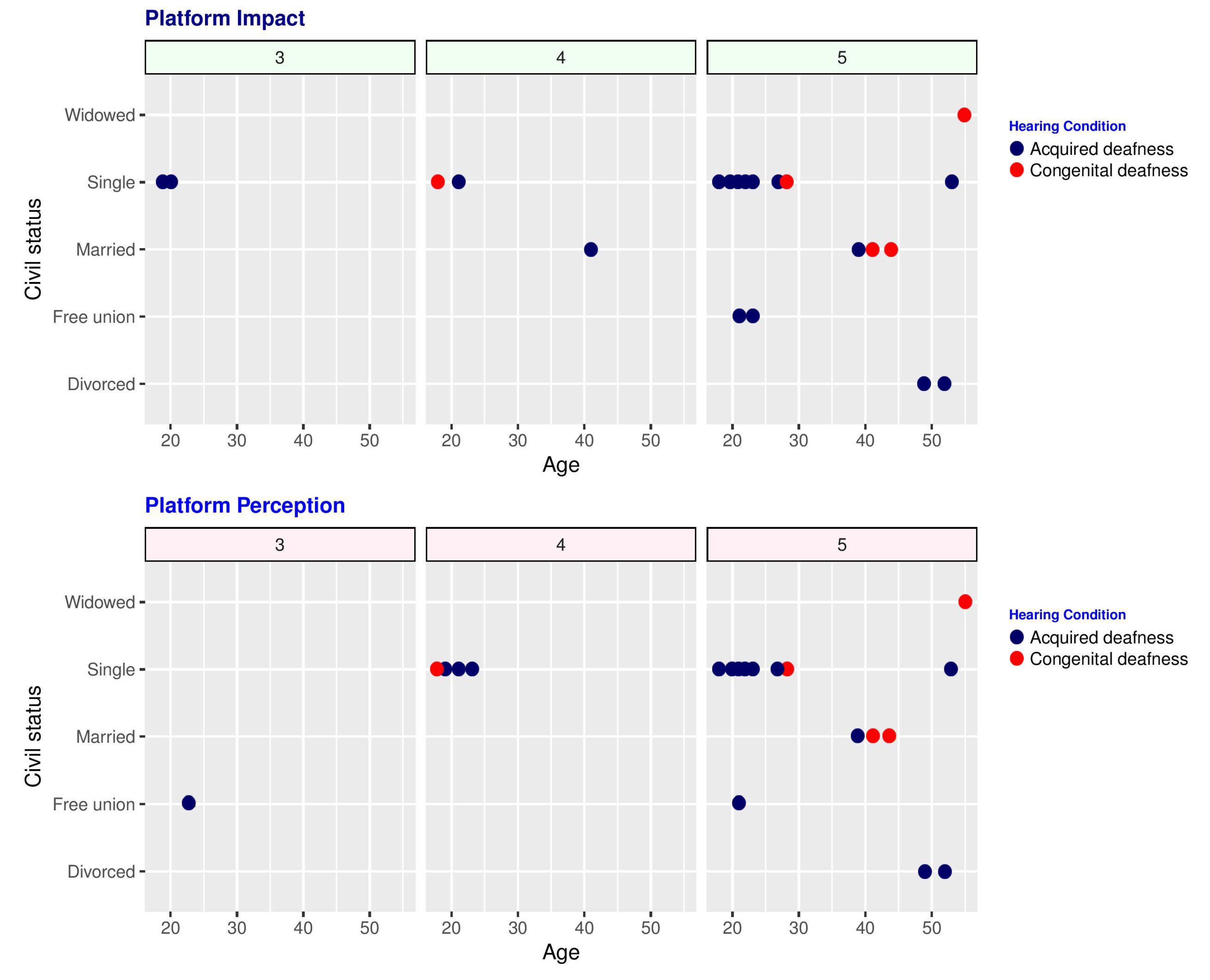
4.2. Deaf Women’s Perceptions about the Social Network
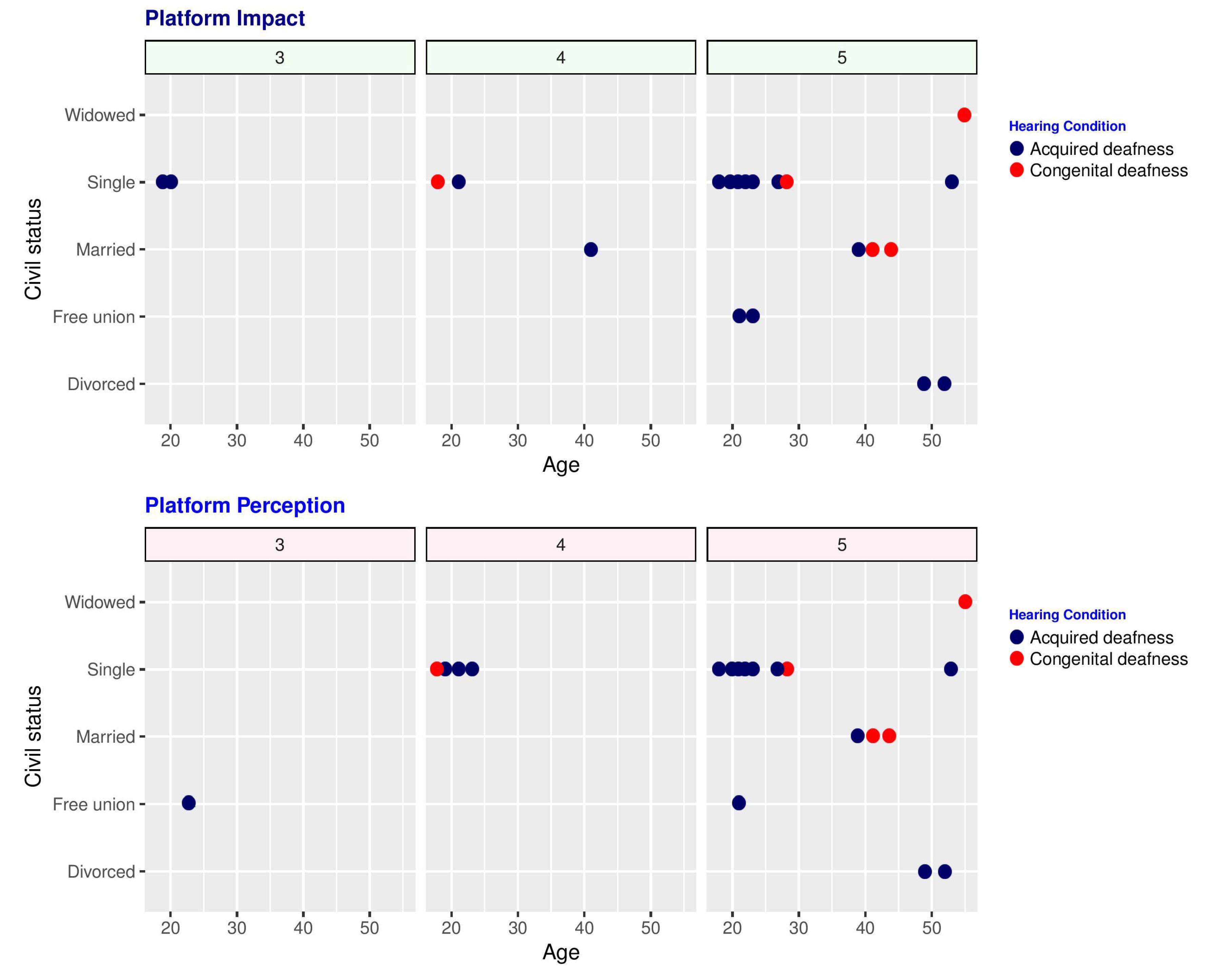
4.3. Evaluation of the Recommender System
5. Conclusions and Future Work
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| ESL | Ecuadorian Sign Language |
| ICT | Information & Communication Technologies |
| SRH | Sexual & Reproductive Health |
| STI | Sexually Transmitted Infections |
Appendix A. New Terms Added to the Ecuadorian Sign Language Dictionary
- Consent
- Privacy
- Confidentiality
- Promiscuity
- Prejudices
- Colic
- Burning
- Secretions
- Ectopic pregnancy
- Lymph nodes
- Fungi
- Parasites
- Microorganisms
- Bacteria
- Vulva
- Serious congenital malformations
- Sexual transmission
- Anal, oral, vaginal sexual contagion
- Vaccines
- HIV
- Fetid
- Injury
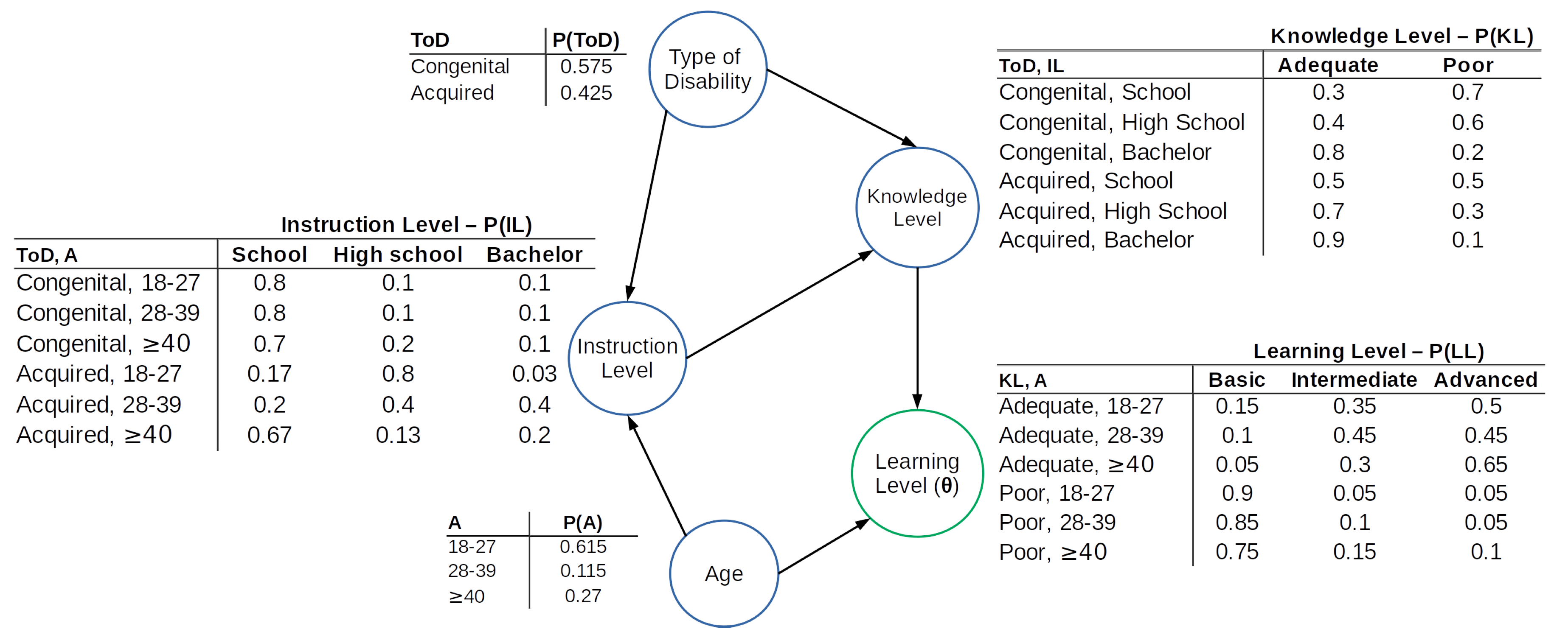
Appendix B. The Recommender System
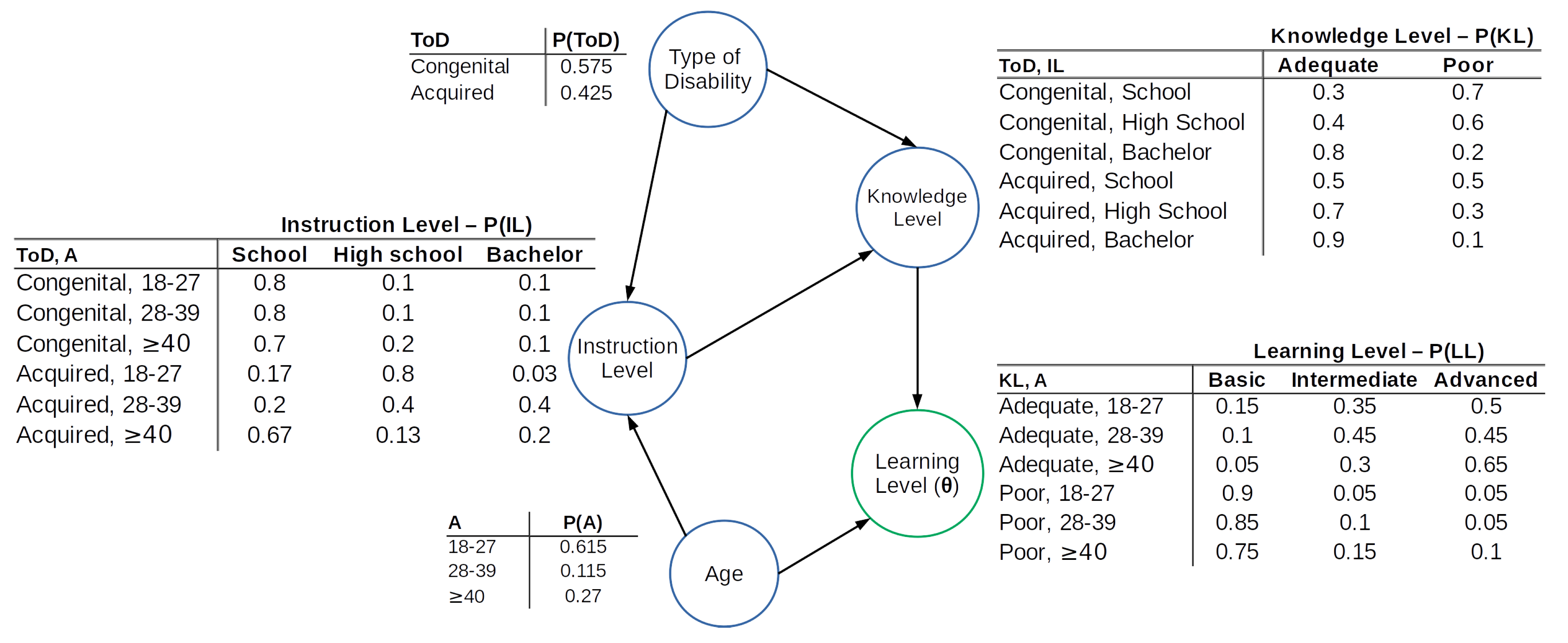
- The type of disability () variable represents the hearing loss diagnosis. We found it sufficient to differentiate only two options: congenital (the woman was born with deafness) and acquired (the woman lost her auditory skills due to an accident or a disease).The probability that a randomly chosen deaf woman has congenital deafness is determined by Equation (A1):where represents the set of congenital hearing impairments defined by the International Classification of Diseases (ICD) [37]. For example, is the code for “Congenital conductive hearing loss”. In turn, the probability of acquired deafness is obviously computed as .
- A woman’s age (A) is strongly related to the contents that must be covered during the learning of SRH concepts. As above, we derive the probabilities corresponding to the different age ranges by counting how many deaf women fall in each range and dividing by the total number. The age table in Figure A1 does not have a category for women younger than 18 because we did not involve minors in our experiments of delivering SRH content.
- We used Equation (A2) to derive the conditional probabilities of the different instruction levels (IL), which in our experiments came down to 3 classes: primary school, secondary school or university. The probabilities are conditional to type of disability and age, so is the a priori probability that a deaf woman reached instruction level given that she has type of disability and age a (In Equation (A2) it is assumed that the type of disability does not depend on age a, hence ):
- By knowledge levels (KL) we represent a deaf woman’s overall apprehension of SRH topics, simply differentiating average from poor. Just like above, we used Equation (A3) to derive the probabilities for the PGM, where denotes the a priori probability that a woman reached knowledge level given that she has type of disability and instruction level .
- From the preceding variables, the PGM can determine which learning level (LL) should be used for a deaf woman for whom we do not have precise observations yet. To this aim, we use Equation (A4), where denotes the a priori probability of choosing learning level for a woman who has instruction level and age a (In Equation (A4) it is assumed that the knowledge level does not depend on age a, hence . These and all other assumptions were proven valid on all our datasets by the Belief and Decision Networks tool provided by AIspace [38]):

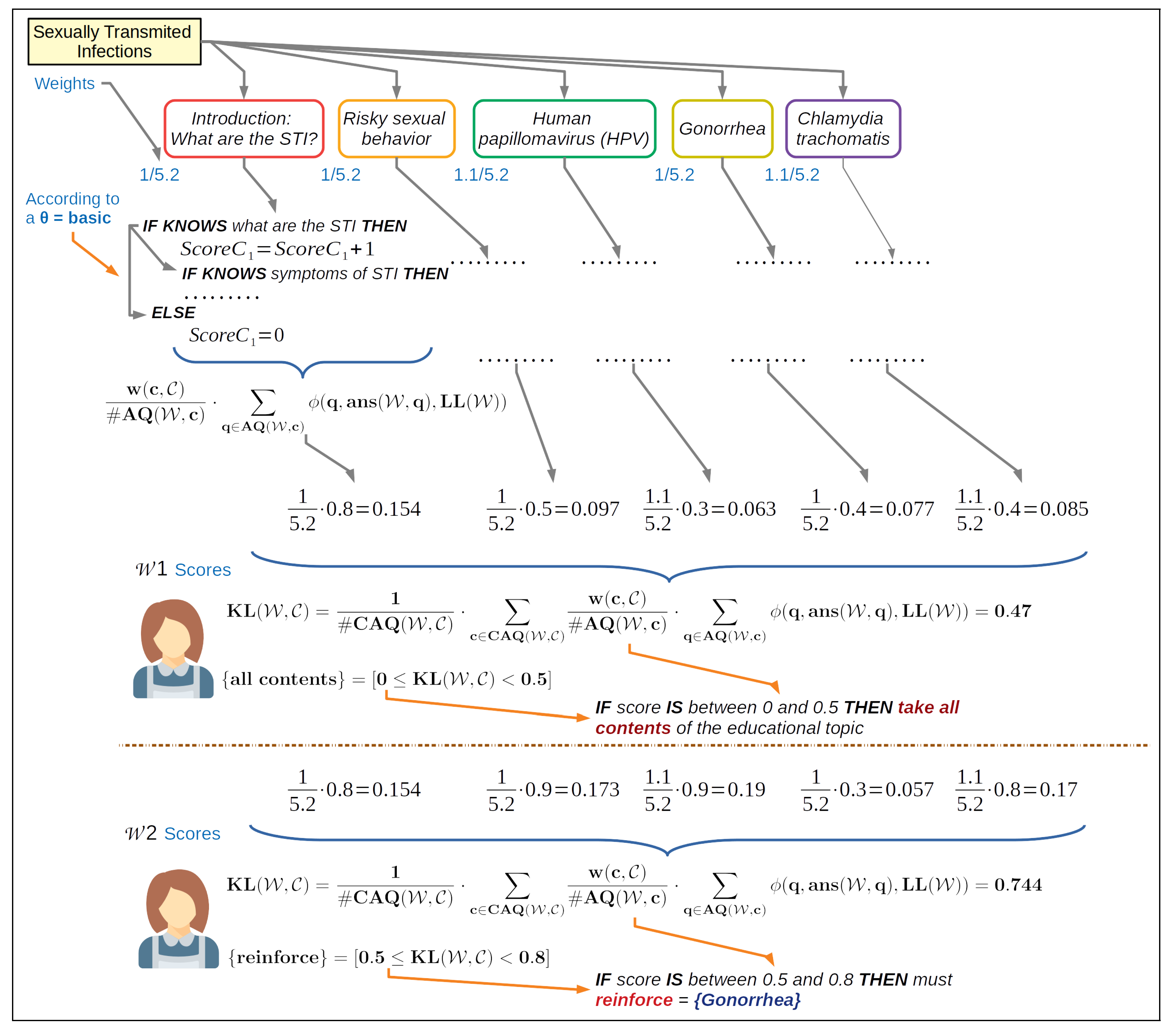
- is the new knowledge level for user about category .
- is the set of contents linked to category and to questionnaires that user has answered to. is the cardinality of that set, i.e., the number of contents in it.
- is the weight of a piece of content c in relation to the category .
- is the set of questionnaires linked to content c that user has replied to. is the cardinality of that set.
- is a function that, given a questionnaire q, the set of answers provided to it by a given user () and the learning level of that user, returns a mark for the questionnaire by checking the applicability of the rules and performing the corresponding computations.
References
- World Health Organization (WHO). Deafness and Hearing Loss. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss (accessed on 27 March 2019).
- Wilbur, J.; Bright, T.; Mahon, T.; Hameed, S.; Torondel, B.; Mulwafu, W.; Kuper, H.; Polack, S. Developing behaviour change interventions for improving access to health and hygiene for people with disabilities: Two case studies from Nepal and Malawi. Int. J. Environ. Res. Public Health 2018, 15, 2746. [Google Scholar] [CrossRef]
- Bright, T.; Wallace, S.; Kuper, H. A systematic review of access to rehabilitation for people with disabilities in low- and middle-income countries. Int. J. Environ. Res. Public Health 2018, 15, 2165. [Google Scholar] [CrossRef]
- Haualand, H.; Allen, C. Deaf People and Human Rights; World Federation of the Deaf and Swedish National Association of the Deaf: Helsinki, Finland, 2009. [Google Scholar]
- World Health Organization. World Report on Disability; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Zuurmond, M.; Mactaggart, I.; Kannuri, N.; Murthy, G.; Oye, J.E.; Polack, S. Barriers and facilitators to accessing health services: A qualitative study amongst people with disabilities in Cameroon and India. Int. J. Environ. Res. Public Health 2019, 16, 1126. [Google Scholar] [CrossRef]
- Chan, K.L.; Lo, C.K.M.; Ho, F.K.; Ip, P. Disability-specific associations with child health and functioning. Int. J. Environ. Res. Public Health 2019, 16, 1024. [Google Scholar] [CrossRef]
- Yun, C.; Wang, Z.; Gao, J.; He, P.; Guo, C.; Chen, G.; Zheng, X. Prevalence and social risk factors for hearing impairment in Chinese children—A national survey. Int. J. Environ. Res. Public Health 2017, 14, 88. [Google Scholar] [CrossRef]
- Naseribooriabadi, T.; Sadoughi, F.S.A. Barriers and facilitators of health literacy among D/deaf individuals: A review article. Iran. J. Public Health 2017, 46, 1465–1474. [Google Scholar]
- Morgan, L. Best Practice Patient Teaching Strategies to Promote Health Literacy When Working with Individuals with Deafness. 2013. Available online: https://research.libraries.wsu.edu/xmlui/bitstream/handle/2376/4376/L_Morgan_10716550.pdf (accessed on 30 September 2019).
- Pollard, R.; Barnett, S. Health-related vocabulary knowledge among deaf adults. Rehabil. Psychol. 2009, 54, 182–185. [Google Scholar] [CrossRef]
- Rey, M.I. El cuerpo en la construcción de la identidad de los sordos; Centro de Estudios Interdisciplinarios en Etnolingüística y Antropología Socio-Cultural: Rosario, Argentina, 2008; Volume 16. [Google Scholar]
- DeBeaudrap, P.; Mouté, C.; Pasquier, E.; Mac-Seing, M.; Mukangwije, P.U.; Beninguisse, G. Disability and access to Sexual and Reproductive Health services in Cameroon: A mediation analysis of the role of socioeconomic factors. Int. J. Environ. Res. Public Health 2019, 16, 417. [Google Scholar] [CrossRef]
- Federación Andaluza de Asociaciones de Personas Sordas. Guía práctica de la salud. 2018. Available online: https://www.semfyc.es/formacion-y-recursos/guias/guia-practica-de-la-salud/?tab=1 (accessed on 6 September 2018).
- Jensen, L.G.; Nakaji, M.; Harry, K.M.; Gallegos, N.; Malcarne, V.L.; Sadler, G.R. Ovarian cancer: Deaf and hearing women’s knowledge before and after an educational video. J. Cancer Educ. 2013, 28, 647–655. [Google Scholar] [CrossRef]
- Palmer, C.G.; Boudreault, P.; Berman, B.A.; Wolfson, A.; Duarte, L.; Venne, V.L.; Sinsheimer, J.S. Bilingual approach to online cancer genetics education for Deaf American Sign Language users produces greater knowledge and confidence than English text only: A randomized study. Disabil. Health J. 2017, 10, 23–32. [Google Scholar] [CrossRef]
- Legeay, M.; Saillard, J. Favoriser l’accès à la santé des sourds et malentendants: Exemple d’atelier d’éducation aux médias. Santé Publique 2013, 2, 235–239. [Google Scholar] [CrossRef]
- Gingiss, D. How Social Media Became a Game-Changer for the Deaf Community. Social Media Today, 9 January 2018. [Google Scholar]
- Bone, T.A. No one is listening: Members of the Deaf community share their depression narratives. Soc. Work Ment. Health 2019, 17, 1–22. [Google Scholar] [CrossRef]
- Ragsdale, K.; Harper, S.K.; Kathuria, S.; Bardwell, J.H.; Penick, C.B.; Breazeale, M. Social Media to Enhance Sexual Health Education for Youth: FactNotFiction’s (Re) Design and Launch. Case Stud. Strateg. Commun. 2015, 4, 88–112. [Google Scholar]
- Goldfrab, A.; Tucker, C. Economic and business dimensions: Online advertising, behavioral targeting and privacy. Commun. ACM 2011, 54, 25–27. [Google Scholar] [CrossRef]
- Simon, L.; Daneback, K. Adolescents’ use of the Internet for sex education: A thematic and critical review of the literature. Int. J. Sex. Health 2013, 25, 305–319. [Google Scholar] [CrossRef]
- Council of Europe. Enabling Access to the Media for All; European Audiovisual Observatory: Strasbourg, France, 2014. [Google Scholar]
- World Wide Web Consortium. W3C Accessibility Standards Overview. 2019. Available online: https://www.w3.org/WAI/standards-guidelines/ (accessed on 25 April 2019).
- Marie Stopes International. Delivering Sexual and Reproductive Health Services to Young People; Marie Stopes International: London, UK, 2012. [Google Scholar]
- Denno, D.M.; Hoopes, A.J.; Chandra-Mouli, V. Effective strategies to provide adolescent sexual and reproductive health services and to increase demand and community support. J. Adolesc. Health 2015, 56, S22–S41. [Google Scholar] [CrossRef]
- Ajao, O.; Jurek, A.; Gough, A.; Hunter, R.F.; Barrett, E.; McKeown, G.; Hong, J.; Kee, F. Feasibility study of social media for public health behaviour changes. arXiv 2017, arXiv:1701.06431. [Google Scholar]
- Boll, F.; Brune, P. Online support for the elderly –Why service and social network platforms should be integrated. Procedia Comput. Sci. 2016, 98, 395–400. [Google Scholar] [CrossRef]
- Paz, V.; Salamanca, M. Elementos de la cultura sorda: Una base para el currículum intercultural. REXE: Revista de Estudios y Experiencias en Educación 2009, 8, 31–49. [Google Scholar]
- Consejo Nacional de Igualdad de Discapacidades (CONADIS). Diccionario de Lengua de Señas Ecuatoriana “Gabriel Román”. 2019. Available online: https://www.consejodiscapacidades.gob.ec/diccionario-de-lengua-de-senas-ecuatoriano-gabriel-roman/ (accessed on 26 February 2018).
- Morgan, C.; McKenzie, T.; Sallis, J.; Broyles, S.; Zive, M.; Nader, P. Personal, social, and environmental correlates of physical activity in a bi-ethnic sample of adolescents. Pediatr. Exerc. Sci. 2003, 15, 288–301. [Google Scholar] [CrossRef]
- Núñez, A.; Robertson-James, C.; Reels, S.; Jeter, J.; Rivera, H.; Yusuf, Z.; Liu. Exploring the role of gender norms in nutrition and sexual health promotion in a piloted school-based intervention: The Philadelphia Ujima experience. Eval. Program Plan. 2015, 51, 70–77. [Google Scholar]
- Santos, J.R.A. Cronbach’s Alpha: A tool for assessing the reliability of scales. J. Ext. 1999, 37, 1–5. [Google Scholar]
- Croasmun, J.T.; Ostrom, L. Using Likert-type scales in the social sciences. J. Adult Educ. 2011, 40, 19–22. [Google Scholar]
- Guerrero-Vásquez, L.F.; Landy-Rivera, D.X.; Bravo-Torres, J.F.; López-Nores, M.; Castro-Serrano, R.; Vintimilla-Tapia, P.E. AVATAR: Contribution to Human-Computer Interaction processes through the adaptation of semi-personalized virtual agents. In Proceedings of the IEEE Biennial Congress of Argentina (ARGENCON), San Miguel de Tucuman, Argentina, 6–8 June 2018; pp. 1–4. [Google Scholar]
- Schein, A.; Popescul, A.; Ungar, L.; Pennock, D. Methods and metrics for cold-start recommendations. In Proceedings of the SIGIR Forum 25th annual international ACM SIGIR conference on Research and development in information retrieval, Tampere, Finland, 11–15 August 2002; pp. 253–260. [Google Scholar]
- World Health Organization. International Classification of Diseases (ICD); World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Porter, K.; Poole, D.; Kisynski, J.; Sueda, S.; Knoll, B.; Mackworth, A.; Hoos, H.; Gorniak, P.; Conati, C. Belief and Decision Networks, version 5.1.10. 2019. Available online: http://www.aispace.org/bayes/index.shtml (accessed on 27 September 2019).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Assessment | Average | ||
|---|---|---|---|---|
| Expert 1 | Expert 2 | Expert 3 | ||
| Applicability: to what extent the platform can be realistically used to promote knowledge about SRH in Ecuadorian Sign Language? | 6 | 8 | 7 | 7 |
| Learning support: to what extent the platform design and features such as tutoring facilities, the assessment quizzes and the recommender system can effectively foster SRH knowledge acquisition? | 10 | 10 | 10 | 10 |
| Self-Learning: to what extent the platform can become a self-education environment? | 5 | 5 | 5 | 5 |
| Attractiveness: to what extent the platform can keep the deaf women engaged and with motivation to learn about SRH? | 10 | 10 | 10 | 10 |
| Suitability: to what extent the available contents are suitable for the whole spectrum of deaf women? | 10 | 10 | 10 | 10 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robles-Bykbaev, Y.; Oyola-Flores, C.; Robles-Bykbaev, V.E.; López-Nores, M.; Ingavélez-Guerra, P.; Pazos-Arias, J.J.; Pesántez-Avilés, F.; Ramos-Cabrer, M. A Bespoke Social Network for Deaf Women in Ecuador to Access Information on Sexual and Reproductive Health. Int. J. Environ. Res. Public Health 2019, 16, 3962. https://doi.org/10.3390/ijerph16203962
Robles-Bykbaev Y, Oyola-Flores C, Robles-Bykbaev VE, López-Nores M, Ingavélez-Guerra P, Pazos-Arias JJ, Pesántez-Avilés F, Ramos-Cabrer M. A Bespoke Social Network for Deaf Women in Ecuador to Access Information on Sexual and Reproductive Health. International Journal of Environmental Research and Public Health. 2019; 16(20):3962. https://doi.org/10.3390/ijerph16203962
Chicago/Turabian StyleRobles-Bykbaev, Yaroslava, Christian Oyola-Flores, Vladimir Espartaco Robles-Bykbaev, Martín López-Nores, Paola Ingavélez-Guerra, José Juan Pazos-Arias, Fernando Pesántez-Avilés, and Manuel Ramos-Cabrer. 2019. "A Bespoke Social Network for Deaf Women in Ecuador to Access Information on Sexual and Reproductive Health" International Journal of Environmental Research and Public Health 16, no. 20: 3962. https://doi.org/10.3390/ijerph16203962
APA StyleRobles-Bykbaev, Y., Oyola-Flores, C., Robles-Bykbaev, V. E., López-Nores, M., Ingavélez-Guerra, P., Pazos-Arias, J. J., Pesántez-Avilés, F., & Ramos-Cabrer, M. (2019). A Bespoke Social Network for Deaf Women in Ecuador to Access Information on Sexual and Reproductive Health. International Journal of Environmental Research and Public Health, 16(20), 3962. https://doi.org/10.3390/ijerph16203962