The Effect of Virtual Reality Games on the Gross Motor Skills of Children with Cerebral Palsy: A Meta-Analysis of Randomized Controlled Trials

Abstract
1. Introduction
2. Methods
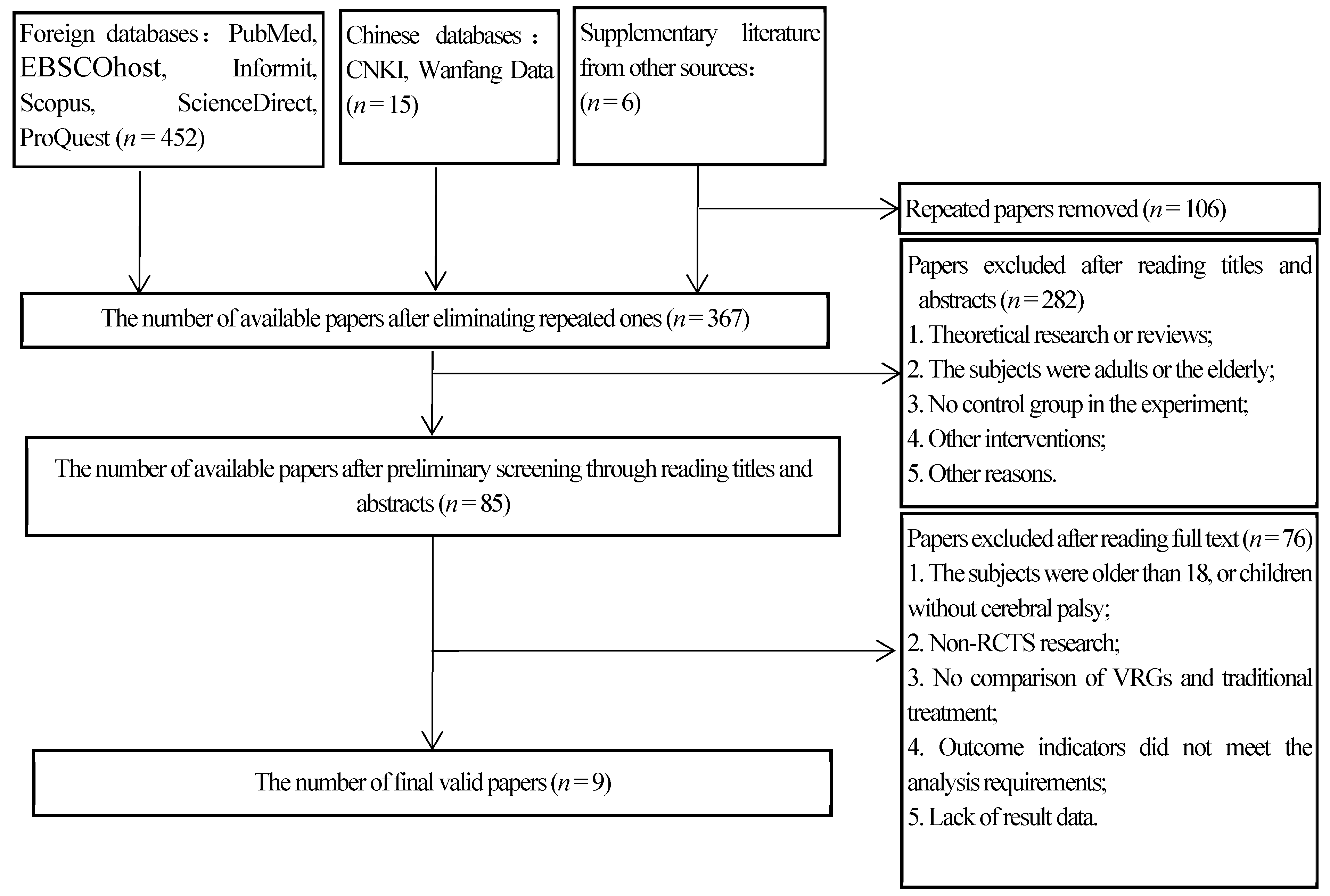
2.1. Literature Retrieval
2.2. Literature Inclusion and Exclusion Criteria
Inclusion Criteria and Exclusion Criteria
2.3. Literature Quality Evaluation
2.4. Data Extraction and Analysis
3. Results
3.1. Retrieval Results
3.2. Literature Characteristics
3.3. Quality Evaluation
3.4. Result of Meta-Analysis
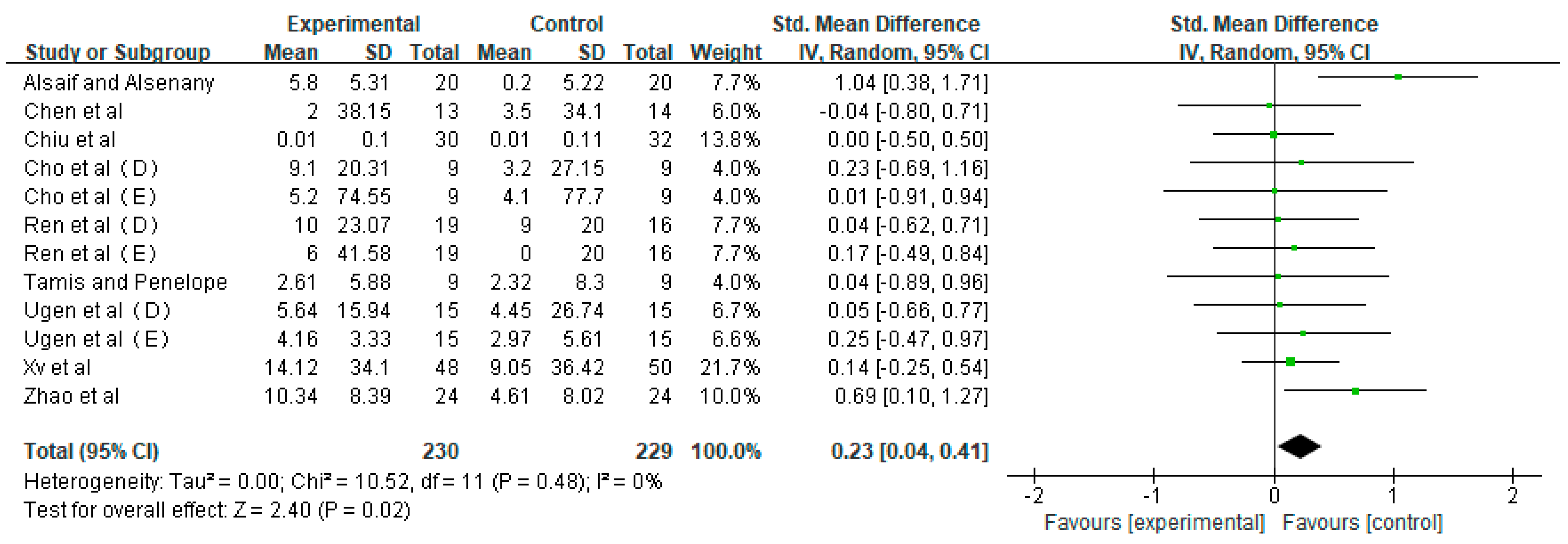
3.4.1. Effects of VRG Group and Control Group on Gross Motor Skills of Children with CP
3.4.2. Analysis of Moderating Effects
4. Discussion
4.1. Meta-Analysis of the Intervention Effect of VRGs on Gross Motor Skills of Children with CP
4.2. Analysis of Influencing Factors of VRG Intervention on Gross Motor Skills of Children with CP
4.2.1. VRGs may Improve the Movement Stability of Children with CP
4.2.2. VRGs may Improve the Postural Control Ability of Children with CP
4.2.3. VRGs may Improve the Motor Ability of Hemiplegic Side of Children with CP
5. Research Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Xiujie, C.; Li, S. Definition, classification and diagnostic conditions of cerebral palsy children. Chin. J. Phys. Med. Rehabil. 2007, 5, 309. [Google Scholar]
- Ping, L.; Zekai, L.; Deng, A. Research progress of family support in children with cerebral palsy. Chin. J. Nurs. 2013, 4, 365–367. [Google Scholar]
- Gormley, M.J. Treatment of neuromuscular and musculoskeletal problems in cerebral palsy. Pediatr. Rehabil. 2001, 4, 5–16. [Google Scholar] [PubMed]
- Bilde, P.E.; Kliim-Due, M.; Rasmussen, B.; Petersen, L.Z.; Petersen, T.H.; Nielsen, J.B. Individualized, home-based interactive training of cerebral palsy children delivered through the Internet. BMC Neurol. 2011, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Yuanchun, R.; Linlin, Z.; Fang, W. Characteristics of physical, behavioral and cognitive functions of children with different levels of gross motor development. J. Beijing Sport Univ. 2013, 3, 79–84. [Google Scholar]
- Juras, G.; Brachman, A.; Michalska, J.; Kamieniarz, A.; Pawlowski, M.; Hadamus, A.; Bialoszewski, D.; Blaszczyk, J.; Slomka, K.J. Standards of Virtual Reality Application in Balance Training Programs in Clinical Practice: A Systematic Review. Games Health J. 2019, 8, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Massion, J.; Alexandrov, A.; Frolov, A. Why and how are posture and movement coordinated? Prog. Brain Res. 2004, 143, 13–27. [Google Scholar] [PubMed]
- van der Heide, J.C.; Fock, J.M.; Otten, B.; Stremmelaar, E.; Hadders-Algra, M. Kinematic characteristics of postural control during reaching in preterm children with cerebral palsy. Pediatr. Res. 2005, 58, 586–593. [Google Scholar] [CrossRef]
- Nudo, R.J. Recovery after brain injury: Mechanisms and principles. Front. Hum. Neurosci 2013, 7, 887. [Google Scholar] [CrossRef]
- Jensen, J.L.; Marstrand, P.C.; Nielsen, J.B. Motor skill training and strength training are associated with different plastic changes in the central nervous system. J. Appl. Physiol. (1985) 2005, 99, 1558–1568. [Google Scholar] [CrossRef]
- Nielsen, J.B.; Cohen, L.G. The Olympic brain. Does corticospinal plasticity play a role in acquisition of skills required for high-performance sports? J. Physiol. 2008, 586, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Dodd, K.J.; Taylor, N.F.; Graham, H.K. A randomized clinical trial of strength training in young people with cerebral palsy. Dev. Med. Child. Neurol. 2003, 45, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.M.; Cassidy, E.E.; Noorduyn, S.G.; O’Connell, N.E. Exercise interventions for cerebral palsy. Cochrane Database Syst. Rev. 2017, 6, D11660. [Google Scholar] [CrossRef] [PubMed]
- Ketelaar, M.; Vermeer, A.; Hart, H.; van Petegem-van, B.E.; Helders, P.J. Effects of a functional therapy program on motor abilities of children with cerebral palsy. Phys. Ther. 2001, 81, 1534–1545. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; McIntyre, S.; Morgan, C.; Campbell, L.; Dark, L.; Morton, N.; Stumbles, E.; Wilson, S.A.; Goldsmith, S. A systematic review of interventions for children with cerebral palsy: State of the evidence. Dev. Med. Child Neurol. 2013, 55, 885–910. [Google Scholar] [CrossRef]
- Katz-Leurer, M.; Rotem, H.; Keren, O.; Meyer, S. The effects of a ‘home-based’ task-oriented exercise programme on motor and balance performance in children with spastic cerebral palsy and severe traumatic brain injury. Clin. Rehabil. 2009, 23, 714–724. [Google Scholar] [CrossRef]
- Qi, L.; Zhang, A. Players’ experience space composition and emotional characteristics in 3D somatosensory games. Prog. Brain Res. 2012, 12, 191. [Google Scholar]
- Ashkenazi, T.; Laufer, Y.; Orian, D.; Weiss, P.L. Effect of training children with Developmental Coordination Disorders in a virtual environment compared with a conventional environment. In Proceedings of the International Conference on Virtual Rehabilitation, Philadelphia, PA, USA, 26–29 August 2013. [Google Scholar]
- Palaus, M.; Marron, E.M.; Viejo-Sobera, R.; Redolar-Ripoll, D. Neural Basis of Video Gaming: A Systematic Review. Front. Hum. Neurosci. 2017, 11, 248. [Google Scholar] [CrossRef]
- You, S.H.; Jang, S.H.; Kim, Y.H.; Hallett, M.; Ahn, S.H.; Kwon, Y.H.; Kim, J.H.; Lee, M.Y. Virtual reality-induced cortical reorganization and associated locomotor recovery in chronic stroke: An experimenter-blind randomized study. Stroke 2005, 36, 1166–1171. [Google Scholar] [CrossRef]
- Tarakci, D.; Ersoz, H.B.; Tarakci, E.; Razak, O.A. Effects of Nintendo Wii-Fit((R)) video games on balance in children with mild cerebral palsy. Pediatr. Int. 2016, 58, 1042–1050. [Google Scholar] [CrossRef]
- Chen, L.; Lo, W.L.; Mao, Y.R.; Ding, M.H.; Lin, Q.; Li, H.; Zhao, J.L.; Xu, Z.Q.; Bian, R.H.; Huang, D.F. Effect of Virtual Reality on Postural and Balance Control in Patients with Stroke: A Systematic Literature Review. Biomed. Res. Int. 2016, 2016, 7309272. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.; Reid, D. The influence of virtual reality play on children’s motivation. Can. J. Occup. Ther. 2005, 72, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Fehlings, D.; Switzer, L.; Findlay, B.; Knights, S. Interactive computer play as “motor therapy” for individuals with cerebral palsy. Semin. Pediatr. Neurol. 2013, 20, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.P.; Lee, S.Y.; Howard, A.M. Effect of virtual reality on upper extremity function in children with cerebral palsy: A meta-analysis. Pediatr. Phys. Ther. 2014, 26, 289–300. [Google Scholar] [CrossRef]
- Hocking, D.R.; Farhat, H.; Gavrila, R.; Caeyenberghs, K.; Shields, N. Do Active Video Games Improve Motor Function in People With Developmental Disabilities? A Meta-analysis of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2019, 100, 769–781. [Google Scholar] [CrossRef]
- Zou, L.Y.; Loprinzi, P.D.; Yeung, A.S.; Zeng, N.; Huang, T. The beneficial effects of mind-body exercises for people with mild cognitive impairment: A systematic review with meta-analysis. Arch. Phys. Med. Rehabil. 2019, 100, 1556–1573. [Google Scholar] [CrossRef]
- Zou, L.Y.; Sasaki, J.E.; Zeng, N.; Wang, C.Y.; Sun, L. A systematic review with meta-analysis of mindful exercises on rehabilitive outcomes among stroke patients. Arch. Phys. Med. Rehabil. 2018, 99, 2355–2364. [Google Scholar] [CrossRef]
- Guanjian, L.; Wu, T. Forest Plot and Clinical Significance of Meta-analysis. Chin. J. Evid.-Based Med. 2014, 3, 198–201. [Google Scholar] [CrossRef]
- Zou, L.; Zhang, Y.; Yang, L.; Loprinzi, P.D.; Yeung, A.S.; Kong, J.; Chen, K.W.; Song, W.; Xiao, T.; Li, H. Are Mindful Exercises Safe and Beneficial for Treating Chronic Lower Back Pain? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2019, 8, 628. [Google Scholar] [CrossRef]
- AlSaif, A.A.; Alsenany, S. Effects of interactive games on motor performance in children with spastic cerebral palsy. J. Phys. Ther. Sci. 2015, 27, 2001–2003. [Google Scholar] [CrossRef]
- Cho, C.; Hwang, W.; Hwang, S.; Chung, Y. Treadmill Training with Virtual Reality Improves Gait, Balance, and Muscle Strength in Children with Cerebral Palsy. Tohoku J. Exp. Med. 2016, 238, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Rgen, M.; Akbayrak, T.; Gunel, M.; Cankaya, O.; Guchan, Z.; Turkyilmaz, E. Investigation of the effects of the NintendoWii-Fit training on balance and advanced motor performance in children with spastic hemiplegic cerebral palsy: A Randomized Controlled Trial. Int. J. Ther. Rehabil. Res. 2016, 5, 146. [Google Scholar] [CrossRef]
- Ren, K.; Gong, X.M.; Zhang, R.; Chen, X.H. Effects of virtual reality training on limb movement in children with spastic diplegia cerebral palsy. Zhongguo Dang Dai Er Ke Za Zhi 2016, 18, 975–979. [Google Scholar] [PubMed]
- Yanyan, X. Effects of virtual reality training combined with repeated transcranial magnetic stimulation on limb motor function in children with cerebral palsy. J. Qiqihar Med Univ. 2019, 11, 213–218. [Google Scholar]
- Pin, T.W.; Butler, P.B. The effect of interactive computer play on balance and functional abilities in children with moderate cerebral palsy: A pilot randomized study. Clin. Rehabil. 2019, 33, 704–710. [Google Scholar] [CrossRef]
- Chen, C.L.; Chen, C.Y.; Liaw, M.Y.; Chung, C.Y.; Wang, C.J.; Hong, W.H. Efficacy of home-based virtual cycling training on bone mineral density in ambulatory children with cerebral palsy. Osteoporos. Int. 2013, 24, 1399–1406. [Google Scholar] [CrossRef]
- Chiu, H.C.; Ada, L.; Lee, H.M. Upper limb training using Wii Sports Resort for children with hemiplegic cerebral palsy: A randomized, single-blind trial. Clin. Rehabil. 2014, 28, 1015–1024. [Google Scholar] [CrossRef]
- Xiaoke, Z.; Yue, Z.; Du, S. Effect of Motion Observation Training Based on Active Video Games on Motor Function of Children with Spastic Cerebral Palsy. Chin. J. Phys. Med. Rehabil. 2018, 12, 916–918. [Google Scholar]
- Zan, G.; Tao, Z.; Stodden, D. Children’s physical activity levels and psychological correlates in interactive dance versus aerobic dance. J. Transp. Health 2013, 2, 146–151. [Google Scholar]
- Pasco, D.; Roure, C.; Kermarrec, G.; Pope, Z.; Gao, Z. The effects of a bike active video game on players’ physical activity and motivation. J. Sport Health Sci. 2017, 6, 25–32. [Google Scholar] [CrossRef]
- Zan, G.; Pope, Z.; Lee, J.E.; Stodden, D.; Roncesvalles, N.; Pasco, D.; Huang, C.C.; Du, F. Impact of exergaming on young children’s school day energy expenditure and moderate-to-vigorous physical activity levels. J. Transp. Health 2017, 6, 15–20. [Google Scholar]
- Zan, G.; Podlog, L.; Huang, C. Associations among children’s situational motivation, physical activity participation, and enjoyment in an active dance video game. J. Transp. Health 2013, 2, 122–128. [Google Scholar]
- Guest, E.W. Children’s motor skill competence, physical activity, fitness, and health promotion. J. Sport Health Sci. 2019, 8, 95. [Google Scholar]
- Gao, Z. Fight fire with fire? Promoting physical activity and health through active video games. J. Sport Health Sci. 2017, 6, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Zeng, N.; Pope, Z.C.; Wang, R.; Yu, F. Effects of exergaming on motor skill competence, perceived competence, and physical activity in preschool children. J. Sport Health Sci. 2019, 8, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Kai, L.; Fan, H. The Application and Research of VR Game Design in Children Autistic Disorder. Sci. Educ. Artic. Collect. (Issue End Mon.) 2018, 11, 165–166. [Google Scholar]
- Zhiwei, L. Kinect-based Somatosensory Rehabilitation System Design for Autistic Children. Hebei Univ. 2018, 1, 66. [Google Scholar]
- Ruihuan, C.; Cuiyan, W. A Study on the Application of Active Video Games in Autistic Children Intervention. J. Suihua Univ. 2017, 10, 92–95. [Google Scholar]
- Xianmei, L.; Liu, Y. A Case Study on the Intervention of Active Video Games in Attention Deficit of Autistic Children. J. Suihua Univ. 2017, 7, 1–7. [Google Scholar]
- Xianmei, L.; Yanhong, L.; Xiaoyi, H. A Study on the Application of Active Video Games to the Intervention in the Motor Skills of Autistic Children. Mod. Spec. Educ. 2016, 20, 36–42. [Google Scholar]
- Yanhong, L.; Xianmei, L.; Xiaoyi, H. Research and Inspiration of Active Video Games for Autistic Children Abroad. Chin. J. Spec. Educ. 2015, 5, 51–56. [Google Scholar]
- Hocking, D.R.; Caeyenberghs, K. What is the Nature of Motor Impairments in Autism, Are They Diagnostically Useful, and What Are the Implications for Intervention? Curr. Dev. Disorders Rep. 2017, 4, 19–27. [Google Scholar] [CrossRef]
- Gomez, A.N.; Venegas, M.A.; Zapata, R.V.; Lopez, F.M.; Maudier, V.M.; Pavez-Adasme, G.; Hemandez-Mosqueira, C. Effect of an intervention based on virtual reality on motor development and postural control in children with Down Syndrome. Rev. Chil. Pediatr. 2018, 89, 747–752. [Google Scholar]
- Silva, V.; Campos, C.; Sa, A.; Cavadas, M.; Pinto, J.; Simoes, P.; Machado, S.; Murillo-Rodriguez, E.; Barbosa-Rocha, N. Wii-based exercise program to improve physical fitness, motor proficiency and functional mobility in adults with Down syndrome. J. Intellect. Disabil. Res. 2017, 61, 755–765. [Google Scholar] [CrossRef]
- Hammond, J.; Jones, V.; Hill, E.L.; Green, D.; Male, I. An investigation of the impact of regular use of the Wii Fit to improve motor and psychosocial outcomes in children with movement difficulties: A pilot study. Child Care Health Dev. 2014, 40, 165–175. [Google Scholar] [CrossRef]
- Salem, Y.; Gropack, S.J.; Coffin, D.; Godwin, E.M. Effectiveness of a low-cost virtual reality system for children with developmental delay: A preliminary randomised single-blind controlled trial. Physiotherapy 2012, 98, 189–195. [Google Scholar] [CrossRef]
- Greg, P.; Geng, P.; Liang, G. Introduction to Human Motor Development; People’s Education Press: Beijing, China, 2008. [Google Scholar]
- Gordon, C.; Roopchand-Martin, S.; Gregg, A. Potential of the Nintendo Wii as a rehabilitation tool for children with cerebral palsy in a developing country: A pilot study. Physiotherapy 2012, 98, 238–242. [Google Scholar] [CrossRef]
- Bei, J.; Xia, C. Analysis of the status quo of children’s writing ability. J. Bio-Education 2018, 1, 30–33. [Google Scholar]
- Snider, L.; Majnemer, A.; Darsaklis, V. Virtual reality as a therapeutic modality for children with cerebral palsy. Dev. Neurorehabil. 2010, 13, 120–128. [Google Scholar] [CrossRef]
- van der Heide, J.C.; Begeer, C.; Fock, J.M.; Otten, B.; Stremmelaar, E.; van Eykern, L.A.; Hadders-Algra, M. Postural control during reaching in preterm children with cerebral palsy. Dev. Med. Child Neurol. 2004, 46, 253–266. [Google Scholar] [CrossRef]
- Sgandurra, G.; Ferrari, A.; Cossu, G.; Guzzetta, A.; Fogassi, L.; Cioni, G. Randomized trial of observation and execution of upper extremity actions versus action alone in children with unilateral cerebral palsy. Neurorehabilit. Neural Repair 2013, 27, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.Y.; Han, J.; Li, C.X.; Yeung, A.S.; Hui, S.C.; Tsang, W.W.N.; Ren, Z.B.; Wang, L. Effects of Tai Chi on lower limb proprioception in adults aged over 55: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2019, 100, 1102–1113. [Google Scholar] [CrossRef]
- Zou, L.; Sasaki, J.E.; Wei, G.-X.; Huang, T.; Yeung, A.S.; Neto, O.B.; Chen, K.W.; Hui, S.C. Effects of Mind–Body Exercises (Tai Chi/Yoga) on Heart Rate Variability Parameters and Perceived Stress: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 404. [Google Scholar] [CrossRef]
- Mastmeyer, A.; Wilms, M.; Fortmeier, D.; Schroder, J.; Handels, H. Real-TimeUltrasound Simulation for Training of US-Guided Needle Insertion in Breathing Virtual Patients. Stud. Health Technol. Inform. 2016, 220, 219–226. [Google Scholar] [PubMed]
- Gibson, J.J. The Ecological Approach to Visual Perception; Houghton-Mifflin: Boston, MA, USA, 1979. [Google Scholar]
- Thelen, E.; Smith, L.B. A Dynamic Systems Approach to the Development of Cognition and Action; MIT Press: Cambridge, MA, USA, 1994. [Google Scholar]



{kind=link}
{kind=link}
| Researchers | Country: Language | Subjects | GMFCS Level (Number) | Characteristics of Subjects (Number; Genders; Ages) | Intervention Methods; Frequency of the Intervention Group; Total Time of the Intervention Group | Intervention Location | VRGs Platform | VRGs Category | Outcome Indicators | |
|---|---|---|---|---|---|---|---|---|---|---|
| Experimental Group | Control Group | |||||||||
| Chen et al. [37]. (2012) | Taiwan; English | Spastic diplegia and spastic hemiplegia children with CP | Level 1: 10; Level 2: 3 | Level 1: 11; Level 2: 3 | 27; experimental group: 13; 9 male (8.7 ± 2.2) ; control group: 14; 9 (8.6 ± 2.2) | Warm-up exercise + sitting training + VRGs treatment; 20 min each time, 3 times a week for 12 weeks; 720 min | Rehabilitation Center | The Eloton SimCycle Virtual Cycling System (Eloton, Inc., NV, USA), | Virtual bicycle | (1) |
| Chiu et al. [38]. (2014) | Taiwan; English | Hemiplegic children with CP | level 1–3: 21 level 4–5: 11 | level 1–3: 21 level 1–3: 9 | 62; experimental group: 32;15 male; (9.4 ± 1.9) Control group: 30; 13 male; (9.5 ± 1.9) | Routine rehabilitation + VRGs; 40 min, 3 times a week for 6 weeks; 720 min | Family | Nintendo wii | Bowling; flying disc; Aerial movement | (2) |
| Alsaif and Alsenany [31]. (2015) | Saudi-Arabia; English | Spastic diplegia children with CP | Level 3: 20 | Level 3: 20 | 40; experimental group: 20; Control group: 20; Age: 6–10 (NSL) | VRGs; 20 min a day, 7 times a week for 12 weeks; 1680 min | Family | Nintendo wii-fit balance board game | Unspecified specific type | (3) |
| Ren et al. [34]. (2016) | China; Chinese | Spastic diplegia children with CP | Level 1: 8; Level 2: 11 | Level 1: 7; Level 2: 9 | 35; experimental group: 19; 11 male; (53.88 ± 13.58) ; control group: 16; 9 (56.53 ± 9.67) | Routine rehabilitation + VRGs; 40 min each time, 5 times a week for 12 weeks; 2400 min | Hospital | Q4 Situational Interactive Training System (produced by Aomai, model q4) | Unspecified specific type | (4) (5) |
| Rgen et al. [33]. (2016) | Turkey; English | Spastic hemiplegia children with CP | Level 2: 15 | Level 2; 15 | 30; experimental group: 15; 7 male; (11.07 ± 2.37); Control group: 15; 7 male; (11.33 ± 2.19) | Routine rehabilitation + VRGs ; 40 min each time, 2 times a week for 9 weeks; 720 min | Not clear | Nintendo wii-fit | Jogging plus, penguin slide, heading, ski jump, snowball fight, tilt city, perfect 10, and segway circuit play. | (4) (5) |
| Cho et al. [32]. (2016) | South Korea; English | Sputum children with CP | Level 1: 3; Level 2: 1; Level 3: 5 | Level 1: 3; Level 2: 2; Level 3: 4 | 18; experimental group: 9, (10.2 ± 3.); Control group: 9, (9.4 ± 3.8) (NSL) | VRGs; 30 min a day, 3 times a week for 8 weeks; 720 min | Outpatient department | Nintendo wii-fit | Virtual reality treadmill | (4) (5) |
| Zhao et al. [39]. (2018) | China; Chinese | Spastic quadriplegia, spastic diplegia and spastic hemiplegia children with CP | Level 1: 18; Level 2: 6 | Level 1: 17; Level 2: 7 | 48; experimental group: 24 ;11 male; (59.38 ± 11.29) months Control group: 24 people (male 16 female 8); (54.33 ± 10.93) months | Routine rehabilitation + VRGs; 40 min each time, 5 times a week for 5 weeks; 1000 min | Hospital | Microsoft Xbox kinect virtual reality platform | Dance music imitation | (6) |
| Pin and Butler [36] (2019) | China (Hong Kong); English | Spastic diplegia children with CP | Level 3: 8; Level 4: 1 | Level 3: 8; Level 4: 1 | 18; experimental group: 9 people 5 male; (8.92 ± 2.25) Control group: 9 people (male 6 female 3); (9.59 ± 1.87) | Routine rehabilitation + VRGs; 20 min each time, 4 times a week for 6 weeks; 480 min | School | (TYROMOTION GmbH, Graz, Austria) | Unspecified specific type | (1) |
| Xv et al. [35]. (2019) | China; Chinese | Children with CP | Not clear | Not clear | 98; experimental group: 50; 22 male; (45.01 ± 8.25) months Control group: 48; 22 male; (43.87 ± 8.25) months | tDCS + VRGs; 20 min each time, 5 times a week for 4 weeks; 400 min | Hospital | Limb a2 feedback system (Guangzhou) | Unspecified specific type | (6) |
| Included Studies | A | B | C | D | E | F | G | H | I | J | K | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chen et al. [37] (2012) | Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | No | 6/11 |
| Chiu et al. [38] (2014) | Yes | Yes | No | Yes | Yes | Yes | No | Yes | Yes | Yes | No | 8/11 |
| Alsaif et al. [31] (2015) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | No | 6/11 |
| Ren et al. [34] (2016) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | No | 6/11 |
| Rgen et al. [33] (2016) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | No | 5/11 |
| Cho et al. [32] (2016) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | No | 6/11 |
| Zhao et al. [39] (2018) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | No | 6/11 |
| Pin et al. [36] (2019) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | No | 7/11 |
| Xv et al. [35] (2019) | Yes | Yes | No | Yes | No | No | No | Yes | Unclear | Yes | No | 5/11 |
| Intervention Plan | Level | Data | SMD | 95%CI | I2 | Intergroup Difference |
|---|---|---|---|---|---|---|
| p Value | ||||||
| Single Intervention Time | ≥17 min; <40 min | 6 | 0.26 | −0.07, 0.60 | 0% | 0.77 |
| ≥40 min | 6 | 0.20 | −0.05, 0.46 | 0% | ||
| Intervention Frequency | ≥2 times per week; <5 times per week | 7 | 0.06 | −0.21, 0.34 | 0% | 0.15 |
| ≥5 times per week | 5 | 0.40 | 0.04, 0.75 | 0% | ||
| Intervention Cycle | ≥4 weeks; <12 weeks | 8 | 0.19 | −0.03, 0.41 | 0% | 0.64 |
| ≥12 weeks | 4 | 0.32 | −0.18, 0.81 | 0% | ||
| Overall Intervention Time | ≥400 min; <1000 min | 8 | 0.09 | −0.14, 0.32 | 0% | 0.11 |
| ≥1000 min | 4 | 0.49 | 0.05, 0.94 | 0% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, Z.; Wu, J. The Effect of Virtual Reality Games on the Gross Motor Skills of Children with Cerebral Palsy: A Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2019, 16, 3885. https://doi.org/10.3390/ijerph16203885
Ren Z, Wu J. The Effect of Virtual Reality Games on the Gross Motor Skills of Children with Cerebral Palsy: A Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2019; 16(20):3885. https://doi.org/10.3390/ijerph16203885
Chicago/Turabian StyleRen, Zhanbing, and Jinlong Wu. 2019. "The Effect of Virtual Reality Games on the Gross Motor Skills of Children with Cerebral Palsy: A Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 16, no. 20: 3885. https://doi.org/10.3390/ijerph16203885
APA StyleRen, Z., & Wu, J. (2019). The Effect of Virtual Reality Games on the Gross Motor Skills of Children with Cerebral Palsy: A Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health, 16(20), 3885. https://doi.org/10.3390/ijerph16203885