Hyaluronic Acid-Based Medical Device for Treatment of Alveolar Osteitis—Clinical Study †

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Composition of the Device
2.2. Study Design
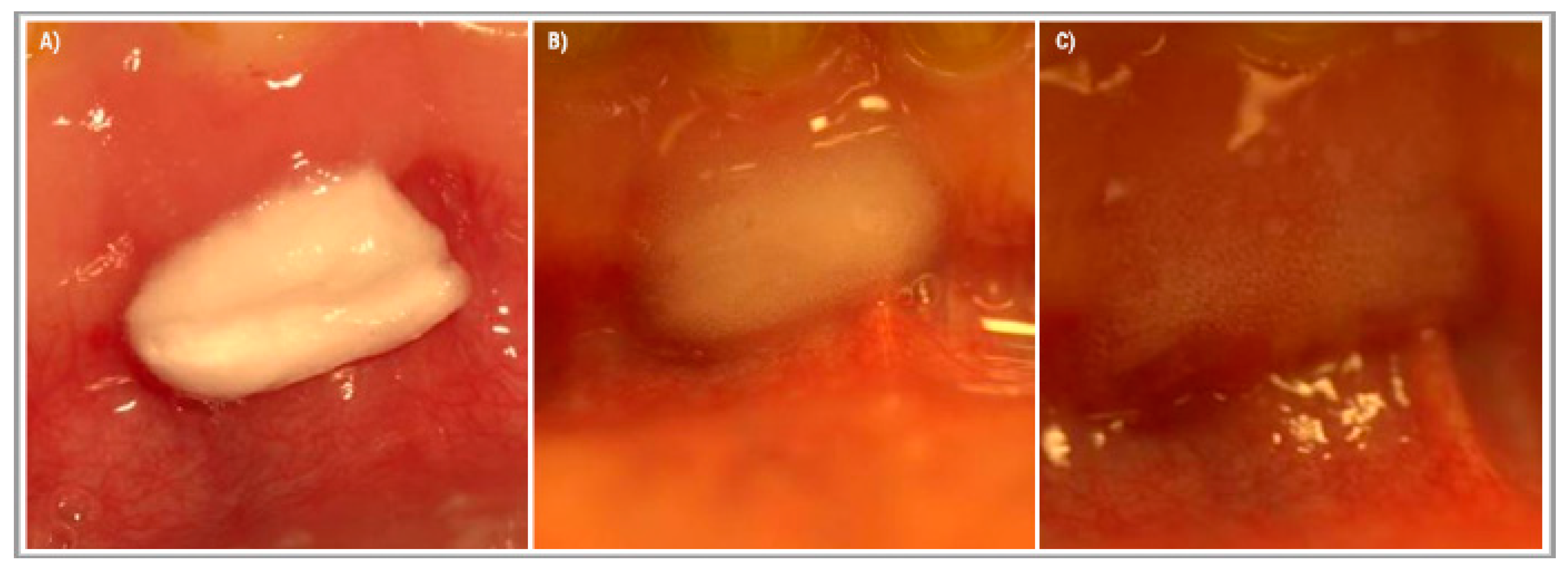
2.3. Treatment Protocol
2.4. Study Objectives
2.5. Statistical Analyses
3. Results
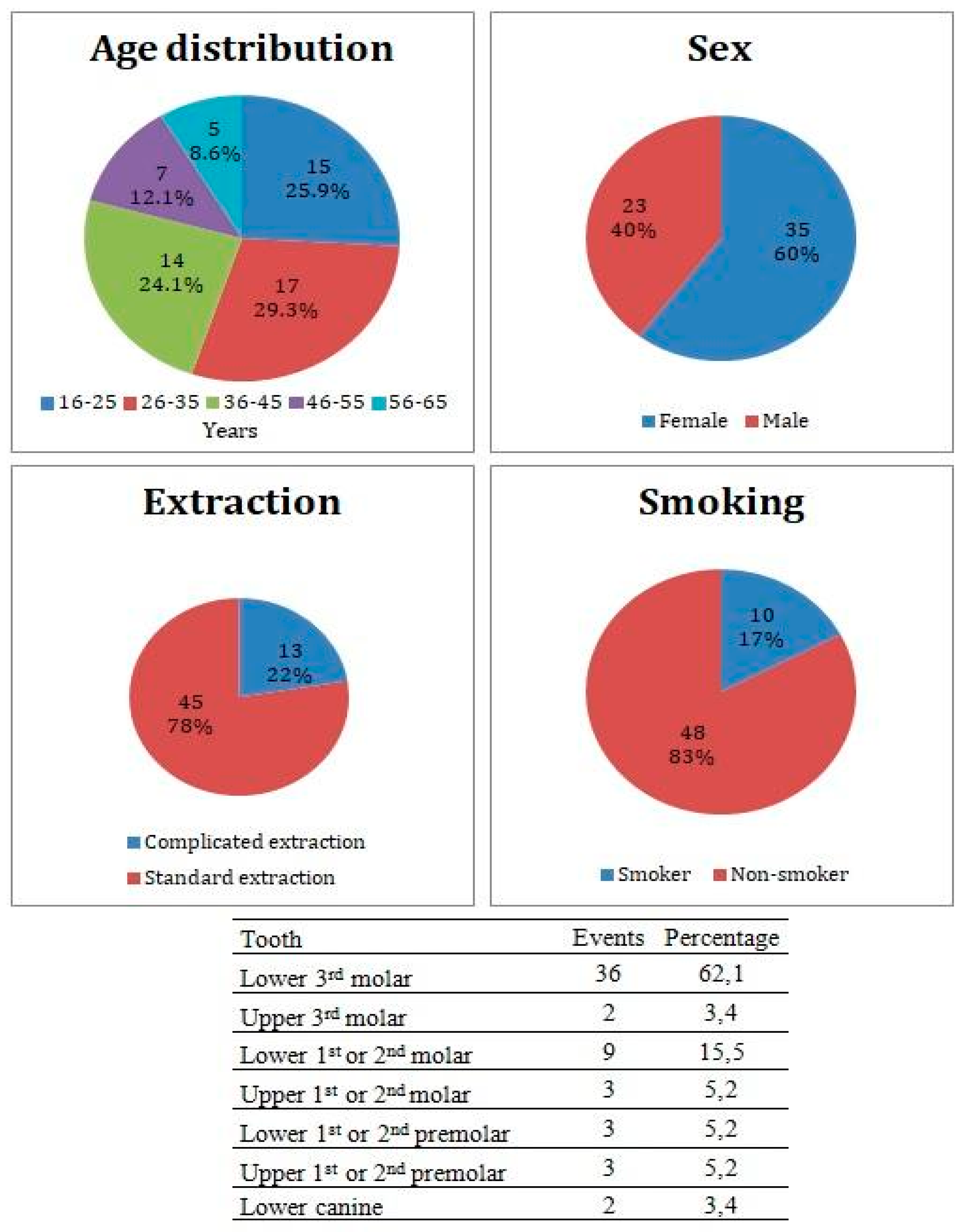
3.1. Patient Cohort
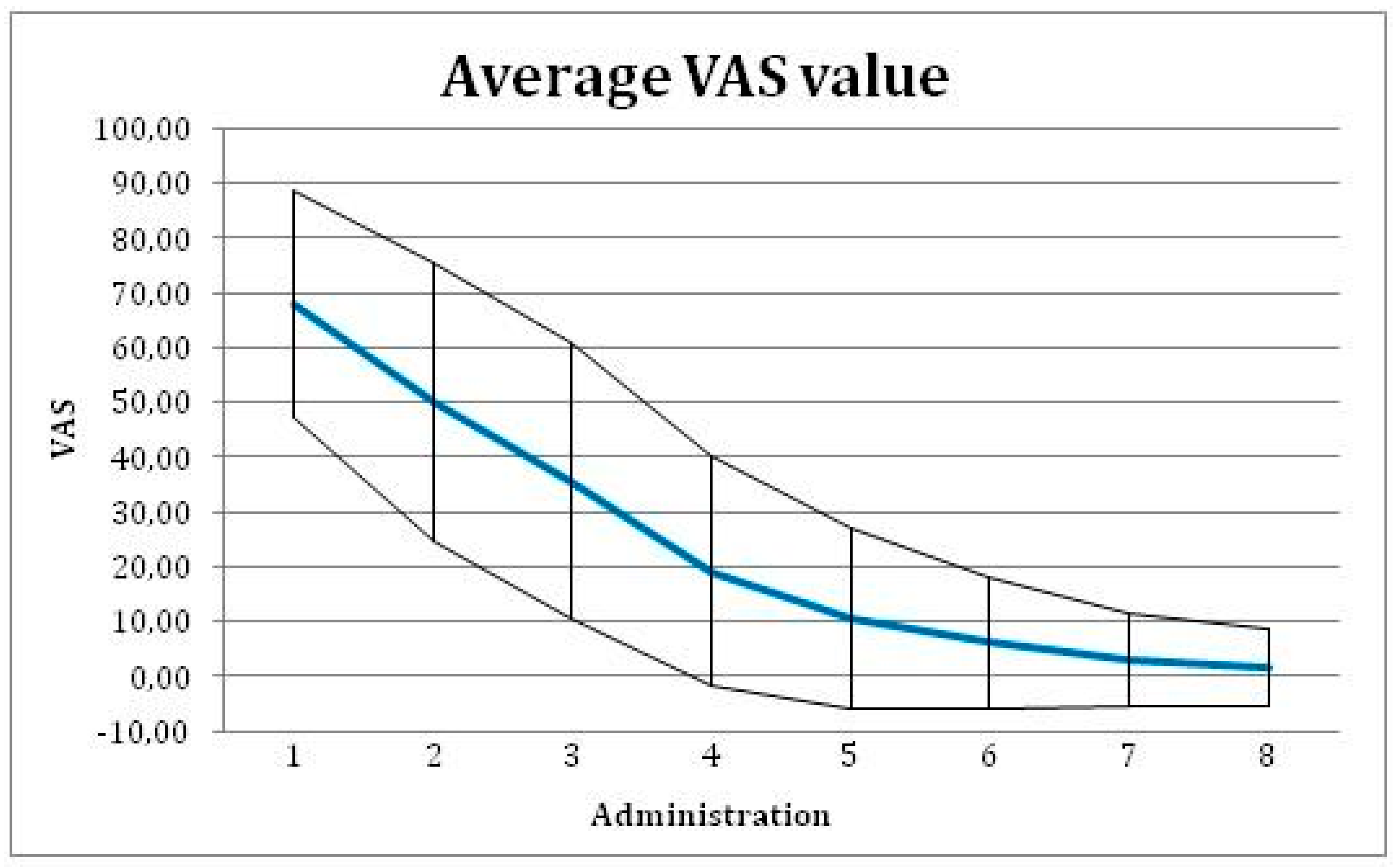
3.2. Study Objectives
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fernandes, G.J.; Hatton, M.N. Prevention of Alveolar Osteitis: A Case Report and Review of Literature. N. Y. State Dent. J. 2016, 82, 21–25. [Google Scholar]
- Sweet, J.B.; Butler, D.P. Increased incidence of postoperative localized osteitis in mandibular third molar surgery associated with patients using oral contraceptives. Am. J. Obstet. Gynecol. 1997, 127, 518–519. [Google Scholar] [CrossRef]
- Sweet, J.B.; Butler, D.P. The relationship of smoking to localized osteitis. J Oral Surg. 1979, 37, 732–735. [Google Scholar] [CrossRef] [PubMed]
- Blum, I.R. Contemporary views on dry socket (alveolar osteitis): A clinical appraisal of standardization, aetiopathogenesis and management: A critical review. Int. J. Oral Maxillofac. Surg. 2002, 31, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Chapnick, P.; Diamond, L.H. A review of dry socket: A Double-Blind study on the effectiveness of clindamycin in reducing the incidence of dry socket. J. Can. Dent. Assoc. 1992, 58, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Nusair, Y.M.; Younis, M.H. Prevalence, clinical picture, and risk factors of dry socket in a Jordanian dental teaching center. J. Contemp. Dent. Pract. 2007, 8, 53–63. [Google Scholar] [CrossRef]
- Kolokythas, A.; Olech, E.; Miloro, M. Alveolar osteitis: A comprehensive review of concepts and controversies. Int. J. Dent. 2010. Available online: https://www.hindawi.com/journals/ijd/2010/249073/ (accessed on 14 May 2010). [CrossRef] [PubMed]
- Field, E.A.; Speechley, J.A.; Rotter, E.; Scott, J. Dry socket incidence compared after a 12 year interval. Br. J. Oral Maxillofac. Surg. 1985, 23, 419–427. [Google Scholar] [CrossRef]
- MacGregor, A.J. Aetiology of dry socket: A clinical investigation. Br. Dent. J. 1968, 6, 49–58. [Google Scholar] [CrossRef]
- Turner, P.S. A clinical study of “dry socket”. Int. J. Oral Maxillofac. 1982, 11, 226–231. [Google Scholar] [CrossRef]
- Krogh, H.W. Incidence of dry socket. J. Am. Dent. Assoc. 1937, 24, 1829–1836. [Google Scholar] [CrossRef]
- Swanson, A.E. Reducing the incidence of dry socket: A clinical appraisal. J. Dent. Assoc. S. Afr. 1966, 21, 155–162. [Google Scholar] [PubMed]
- Heasman, P.A.; Jacobs, D.J. A clinical investigation into the incidence of dry socket. Br. J. Oral Maxillofac. Surg. 1984, 22, 115–122. [Google Scholar] [CrossRef]
- Mitchell, R. Treatment of fibrinolytic alveolitis by a collagen paste (formula K): A preliminary report. Int. J. Oral Maxillofac. Surg. 1986, 15, 127–133. [Google Scholar] [CrossRef]
- Swanson, A.E. Prevention of dry socket: An overview. Oral Surg. Oral Med. Oral Pathol. 1990, 70, 131–136. [Google Scholar] [CrossRef]
- Vezeau, P.J. Dental extraction wound management: Medicating postextraction sockets. J. Oral Maxillofac. Surg. 2000, 58, 531–537. [Google Scholar] [CrossRef]
- Ren, Y.F.; Malmstrom, H.S. Effectiveness of antibiotic prophylaxis in third molar surgery: A Meta-Analysis of randomized controlled clinical trials. J. Oral Maxillofac. Surg. 2007, 65, 1909–1921. [Google Scholar] [CrossRef]
- Summers, L.; Matz, L.R. Extraction wound sockets. Histological changes and paste packs—A trial. Br. Dent. J. 1976, 141, 377–379. [Google Scholar] [CrossRef]
- Syrjänen, S.M.; Syrjänen, K.J. Influence of Alvogyl on the healing of extraction wound in man. Int. J. Oral Surg. 1979, 8, 22–30. [Google Scholar] [CrossRef]
- Matou-Nasri, S.; Gaffney, J.; Kumar, S.; Slevin, M. Oligosaccharides of hyaluronan induce angiogenesis through distinct CD44 and RHAMM-mediated signalling pathways involving Cdc2 and γ-adducin. Int. J. Oncol. 2009, 35, 761–773. [Google Scholar]
- Longaker, M.T.; Chiu, E.S.; Adzick, N.S.; Stern, M.; Harrison, M.R.; Stern, R. Studies in fetal wound healing. V. A prolonged presence of hyaluronic acid characterizes fetal wound fluid. Ann. Surg. 1991, 213, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.J.; Abatangelo, G. Functions of hyaluronan in wound repair. Wound Repair Regen. 1999, 7, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Koburger, T.; Hübner, N.O.; Braun, M.; Siebert, J.; Kramer, A. Standardized comparison of antiseptic efficacy of triclosan, PVP–iodine, octenidine dihydrochloride, polyhexanide and chlorhexidine digluconate. J. Antimicrob. Chemother. 2010, 65, 1712–1719. [Google Scholar] [CrossRef] [PubMed]
- Hübner, N.O.; Siebert, J.; Kramer, A. Octenidine dihydrochloride, a modern antiseptic for skin, mucous membranes and wounds. Skin Pharmacol. Physiol. 2010, 23, 244–258. [Google Scholar] [CrossRef] [PubMed]
- Dogan, A.A.; Cetin, E.S.; Hüssein, E.; Adiloglu, A.K. Microbiological evaluation of octenidine dihydrochloride mouth rinse after 5 days’ use in orthodontic patients. Angle Orthod. 2009, 79, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Briese, V.; Neumann, G.; Waldschläger, J.; May, T.W.; Siebert, J.; Gerber, B. Efficacy and tolerability of a local acting antiseptic agent in the treatment of vaginal dysbiosis during pregnancy. Arch. Gynecol. Obstet. 2011, 283, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Hussain, I.; Singh, S.; Jain, H.; Kumar, S.; Anand, K.R.; Batool, N.; Saikia, J. A prospective randomised clinical study on evaluation of platelet-rich fibrin versus zinc oxide eugenol in the management of alveolar osteitis. Oral Surg. 2018, 11, 41–49. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2015; Available online: http://www.R-project.org/ (accessed on 2 October 2015).
- Alexander, R.E. Dental extraction wound management: A case against medicating postextraction sockets. J. Oral Maxillofac. Surg. 2000, 58, 538–551. [Google Scholar] [CrossRef]
- Taberner-Vallverdú, M.; Nazir, M.; Sánchez-Garcés, M.Á.; Gay-Escoda, C. Efficacy of different methods used for dry socket management: A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2015, 20, 633–639. [Google Scholar] [CrossRef]
- Burgoyne, C.C.; Giglio, J.A.; Reese, S.E.; Sima, A.P.; Laskin, D.M. The efficacy of a topical anesthetic gel in the relief of pain associated with localized alveolar osteitis. J. Oral Maxillofac. Surg. 2010, 68, 144–148. [Google Scholar] [CrossRef]
- Kaya, G.S.; Yapıcı, G.; Savas, Z.; Güngörmüş, M. Comparison of alvogyl, SaliCept patch, and low-level laser therapy in the management of alveolar osteitis. J. Oral Maxillofac. Surg. 2011, 69, 1571–1577. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Center | Number of Treated Patients |
|---|---|
| 1 | 22 |
| 2 | 4 |
| 3 | 1 |
| 4 | 7 |
| 5 | 7 |
| 6 | 4 |
| 7 | 5 |
| 8 | 8 |
| Device Administrations | Number of Observed Events | Proportion of Fade Away of Inflammatory Symptoms (%) | 95 % Confidence Interval |
|---|---|---|---|
| 1 | 10 | 20.0 | 6.9, 26.4 |
| 2 | 9 | 38.0 | 19.5, 43.8 |
| 3 | 12 | 62.0 | 39.5, 65.9 |
| 4 | 9 | 80.0 | 56.7, 81.4 |
| 5 | 5 | 90.0 | 68.1, 90.4 |
| 6 | 1 | 92.0 | 70.7, 92.8 |
| 7 | 2 | 96.0 | 75.7, 97.8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suchánek, J.; Ivančaková, R.K.; Mottl, R.; Browne, K.Z.; Pilneyová, K.C.; Pilbauerová, N.; Schmidt, J.; Suchánková Kleplová, T. Hyaluronic Acid-Based Medical Device for Treatment of Alveolar Osteitis—Clinical Study. Int. J. Environ. Res. Public Health 2019, 16, 3698. https://doi.org/10.3390/ijerph16193698
Suchánek J, Ivančaková RK, Mottl R, Browne KZ, Pilneyová KC, Pilbauerová N, Schmidt J, Suchánková Kleplová T. Hyaluronic Acid-Based Medical Device for Treatment of Alveolar Osteitis—Clinical Study. International Journal of Environmental Research and Public Health. 2019; 16(19):3698. https://doi.org/10.3390/ijerph16193698
Chicago/Turabian StyleSuchánek, Jakub, Romana Koberová Ivančaková, Radovan Mottl, Klára Zoe Browne, Kristýna Charlotte Pilneyová, Nela Pilbauerová, Jan Schmidt, and Tereza Suchánková Kleplová. 2019. "Hyaluronic Acid-Based Medical Device for Treatment of Alveolar Osteitis—Clinical Study" International Journal of Environmental Research and Public Health 16, no. 19: 3698. https://doi.org/10.3390/ijerph16193698
APA StyleSuchánek, J., Ivančaková, R. K., Mottl, R., Browne, K. Z., Pilneyová, K. C., Pilbauerová, N., Schmidt, J., & Suchánková Kleplová, T. (2019). Hyaluronic Acid-Based Medical Device for Treatment of Alveolar Osteitis—Clinical Study. International Journal of Environmental Research and Public Health, 16(19), 3698. https://doi.org/10.3390/ijerph16193698