1. Introduction
Large variations in cancer survival have been reported between populations worldwide, including between European and high-income countries [
1,
2]. For example, cancer survival is generally lower in Denmark than in a comparable country like Sweden [
1,
3,
4]. Cancer survival differences also occur at sub-national levels, such as lower survival for males than for females in the same country [
5,
6,
7], or differences between regions [
8]. These variations in cancer survival suggest that the gap could be lessened if low-survival populations could approximate survival from the high-survival populations by, among other factors, improving national healthcare systems [
9] or reducing socioeconomic disparities [
10].
Potential explanations of the differences between populations include: more adverse stage at diagnosis [
11], greater burden of certain risk factors (e.g., smoking) [
12], or biological differences [
13]. Studies showed that stage at diagnosis can be a key explanation for cancer differences between countries [
11,
14,
15].
Cancer survival and mortality differences between populations can be studied with descriptive statistics and comparison of survival functions [
1,
14,
15]. These studies show the difference in survival between populations but provide limited information on why these differences occur. For instance, a more adverse stage distribution can be observed in a low-survival population relative to a high-survival population, but this provides no quantification. Regression analyses, such as the Cox proportional hazard model or other forms of generalized linear models, have been used to study the relation between cancer survival or mortality and a set of independent variables (e.g., stage at diagnosis) [
11,
16,
17]. However, regression model assumptions do not always hold (e.g., proportional hazards). Additionally, these models often estimate relative differences only (e.g., hazard ratio, relative risk, or odds ratio), while absolute numbers are sometimes preferable. Absolute differences can be useful for quantifying the differences explained by a specific variable, or the potential gains in survival that could be achieved by modifying that variable.
Non-parametric decomposition methods are valued tools in demography, yet less common in public health [
18], and can quantify the exact contribution of specific components, such as ages and causes of death, to a (usually) absolute difference between populations in a given measure [
19,
20,
21,
22]. Many decomposition methods require no assumptions (structural or distributional) about the data.
We introduce the Kitagawa decomposition method [
22], extend its application to cancer research, and present a novel extension of the method to account for the confounding effect of background population (incl. background survival). We decompose the difference between cancer survival probabilities in two populations by their underlying differences in (1) age composition at diagnosis, (2) stage composition at diagnosis, and (3) age–stage-specific survival. Each of these contributions can relate to different issues in health care. The method is illustrated by decomposing differences in female breast cancer survival between Danish regions. Denmark has five administrative regions: The Capital, Zealand, Southern Denmark, Central Denmark, and Northern Denmark. In 2007, Denmark established a new political and administrative scheme in which the healthcare system is run at three levels: the state, the regions, and the municipalities. The national level regulates and supervises health and elderly care. The regions are responsible for hospitals, general practitioners (GPs), and psychiatric care units. The municipalities mainly oversee primary healthcare services, such as health promotion or extramural rehabilitation [
23]. Given the important role of GPs, hospitals and their interactions in prompt diagnosis, and the important role of hospitals in treatment, all falling under the regions’ responsibility, differences in cancer survival between Danish regions are an instructive test case for the method.
2. Methods
The Kitagawa method quantifies the amount of absolute difference in a crude rate that is due to differences in compositions versus differences in component-specific rates between populations, using multiple standardizations. Extensions and similar techniques have been developed [
24,
25,
26,
27]. The Kitagawa decomposition can also be applied to probabilities. Indeed, the Kitagawa decomposition can be applied whenever one variable can be expressed as the product of two others, one of which is, generally, a composition. For example, we can express a crude survival probability (S) as the product of some x-composition
(e.g., age composition) of a population and the x-specific survival
:
To quantify the absolute difference in a crude survival probability between two populations (Y and Z) due to differences in the composition of variable
(
) and differences in x-specific survival probabilities
, the Kitagawa formula reads as:
where the bar over the indicator (probability s or composition
) represents the x-specific averages across populations Y and Z (e.g.,
) and
is the difference between the two populations (e.g.,
). If variable
is age, then Equation (2) quantifies:
The survival effect: The difference in the crude probability between two populations that is due to the difference in their age-specific probabilities , i.e., the sum of age-specific survival probabilities differences after multiplying for each population by the average age-composition of these two populations (direct standardization).
The age effect (X-effect): The difference in the crude probability between two populations that is due to the difference in their age-specific composition , i.e., the sum of the age composition differences after multiplying for each population by the average age-specific probabilities of these two populations (indirect standardization).
More than one composition effect can be of interest to understand differences in a rate or probability between two populations. When using any two compositions (
and
i), the crude survival can be expressed as:
where
is the
distribution for each
and
is the
composition for each
. For example, if
is age and
is stage, then
is the stage-composition at age
x. Kitagawa (1955) [
22] provided a way to decompose crude rate differences into two or more composition effects (X and I) and one survival effect:
We used the Kitagawa method to decompose differences in crude survival probabilities (
) between two populations, by an age-at-diagnosis composition effect (X-effect), stage-at-diagnosis composition effect (I-effect), age–stage-specific survival effect (survival effect), and an interaction term between the age and stage compositions, such that:
Confidence intervals (CI) for each contribution and for the total difference were calculated using bootstrapping methods. The original sample was randomly resampled with replacement 1000 times, with the sample size kept constant. The decomposition method was then reapplied to each sample and 95% confidence intervals were calculated based on 2.5% and 97.5% percentiles, as similarly suggested by Wang et al. (2000) [
18].
2.1. Sub-Decompositions to Assess the Effect of the Background Population
The background population can inform about the cancer patient’s chance of survival. For example, a low background survival indicates high risk of death irrespective of cancer and can inform on higher competing risks from other causes. The background age composition is also informative, as an older background population is more likely to have older cancer patients. Therefore, we introduce an extension of the Kitagawa decomposition to quantify the contribution of (1) the background survival and (2) the background age composition to the difference in crude cancer survival between two populations. These contributions can approximate the quantity of the survival effect and age effect that is characteristic of the background population in addition to the differences in survival and age-composition of the cancer patients.
2.1.1. Sub-Decomposition of the Survival Effect
Relative survival (), i.e., the survival of cancer patients after adjustment for other causes of death, is often a favored measure over crude survival in cancer research. Relative survival is the ratio of the survival observed among cancer patients to the survival observed in a background population () with similar demographic characteristics (year, sex, age) (), thus controlling for the effect of overall survival.
The survival effect (sE) can be divided into a relative survival effect (
) and a background survival effect (
), such that
. Given the formula of
, the age–stage-specific survival can be expressed as the product of the relative survival and background survival (
). Because
can be expressed as a product, the Kitagawa decomposition can be applied to decompose
, such that
. By replacing
in Equation (4) by the previous formulas, we obtain:
2.1.2. Sub-Decomposition of the Age Effect
As with survival, the age-at-diagnosis composition is influenced by the age structure of the background population and by the age structure of the cancer patients. Decomposing differences in a composition is however more complex (see the detailed decomposition in
Appendix A). Using compositional data analysis (CoDA) techniques [
28,
29], we can find the age composition
as if the background age composition and the relative age composition were equal between populations Y and Z. The procedure presented in
Appendix A is not an exact decomposition but approximates the difference in age composition closely:
, where
and
are the effect of the background age composition and the effect of the relative age composition, respectively.
Confidence intervals for the background effects (age and survival) using the above described method cannot be estimated, as these effects are based on aggregated data only (see Data section below). These contributions should, thus, be seen as an indication of where the differences between populations emerge: From the background structure and survival, or from characteristics of the cancer patients. However, confidence intervals can be estimated for the relative effects (age and survival)
2.2. Decomposition of standardized survival
Standardized survival can also be decomposed. Standardized probabilities were obtained by separating survival from the confounding effects of the age compositions and background survival. The average background survival and age composition of the two regions compared was used as “reference population” for the standardization (see
Appendix B for details).
4. Results
Central Denmark had the highest survival among the regions for both one-year and five-year survival (95.90% and 82.75% respectively,
Table 2) and, thus, served as benchmark for the other regions.
4.1. Decomposition of Crude Survival Probabilities (Zealand Versus Central Denmark)
The absolute difference in breast cancer survival between Zealand and Central Denmark was 1.62 percent points for one-year survival and 4.14 for five-year survival, for the period 2008–2010. If Zealand had had the same survival as Central Denmark, the number of breast cancer deaths one year after diagnosis would have been 28.3% lower (corresponding to 40 deaths for the period); five years after diagnosis this number would have been 19.4% (corresponding to 103 deaths for the period).
The survival effect accounted for 31.4% and 43.9% of the difference for the one-year and five-year survival, respectively (
Table 3). The survival effect was, however, not significant for the one-year survival. Around 34% of the survival effect can be explained by the background survival components. Central Denmark had better survival from all causes of death combined than Zealand, meaning that cancer patients also benefited from a reduced risk from other causes of death. Female life expectancy for the period 2008–2010 was 81.8 years in Central Denmark and 80.5 in Zealand.
The age effect widened the difference in survival between Zealand and Central Denmark, with a significant contribution for the five-year survival. This difference in the age-at-diagnosis composition of the cancer patients was mainly due the relative age component. The background age component was negative, meaning that Central Denmark had an older background age composition than Zealand. Negative contributions are interpreted as an advantage for Zealand in
Table 3.
Zealand also had a more adverse stage-at-diagnosis distribution than Central Denmark, with 44.9% (one-year) and 26.5% (five-year) of the difference in breast cancer survival between the two regions being attributable to the stage effect (both significant, decompositions for other regions in
Appendix D).
4.2. Decomposition of Standardized Survival Probabilities
For survival standardized by background survival and age, the differences in the one-year and five-year survival between the Zealand and Central Denmark was 1.24 and 2.39 percent points, respectively, for the period 2008–2010.
Table 4 shows the decomposition of the standardized survival by stage-specific survival and stage composition, using the Kitagawa method with one composition effect (Equation (2)). Compared with the contributions of relative survival and stage from the decomposition presented in
Table 3, the stage and relative survival contributions remained equal at a two-decimal rounding when decomposing the crude and standardized survival probabilities. However, after standardizing by age, we cannot separate out the interaction effects, which is contained within the stage effect. Standardizing does not affect the absolute contributions of the components, when using the average between populations as reference (
Appendix B). After removing the age and background effects, the stage effect is the dominant contributor to the difference in the one-year survival between the two regions, explaining 73.5% of the difference.
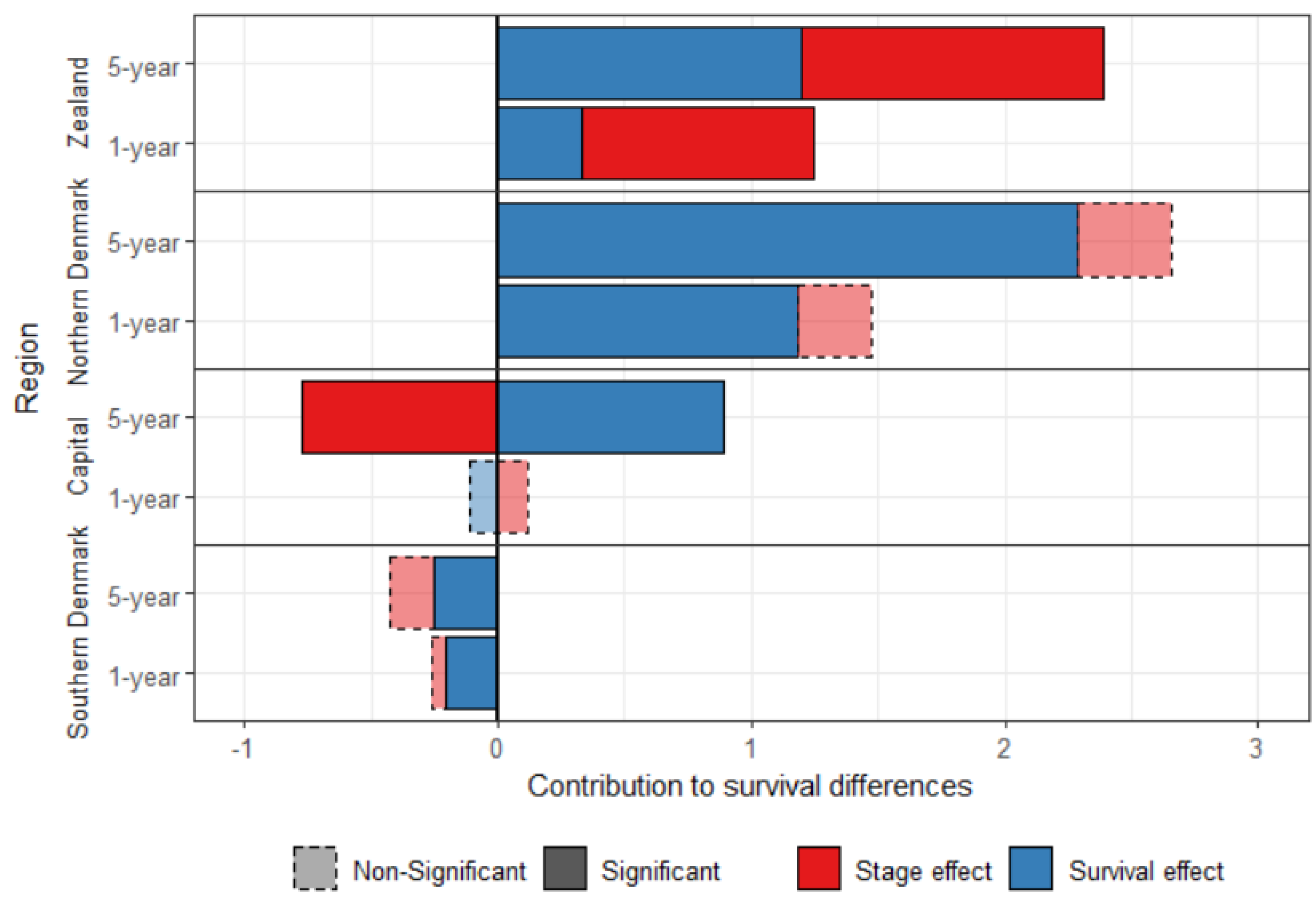
Figure 1 shows the standardized survival decomposition between Central Denmark and the four other regions. After standardization, Southern Denmark has a better survival than Central Denmark, which is mainly attributed to the survival effect. Central Denmark had a better stage-specific survival than the other three regions. The survival effect contributed to 79.8% and 86.0% of the difference in breast cancer one-year and five-year survival, respectively, between Northern Denmark and Central Denmark.
The stage-effect contributed to the disadvantage of Zealand, but played in favor of the Capital region for the five-year survival. There was no significant stage effect explaining the difference between Central Denmark and the Southern and the Northern regions.
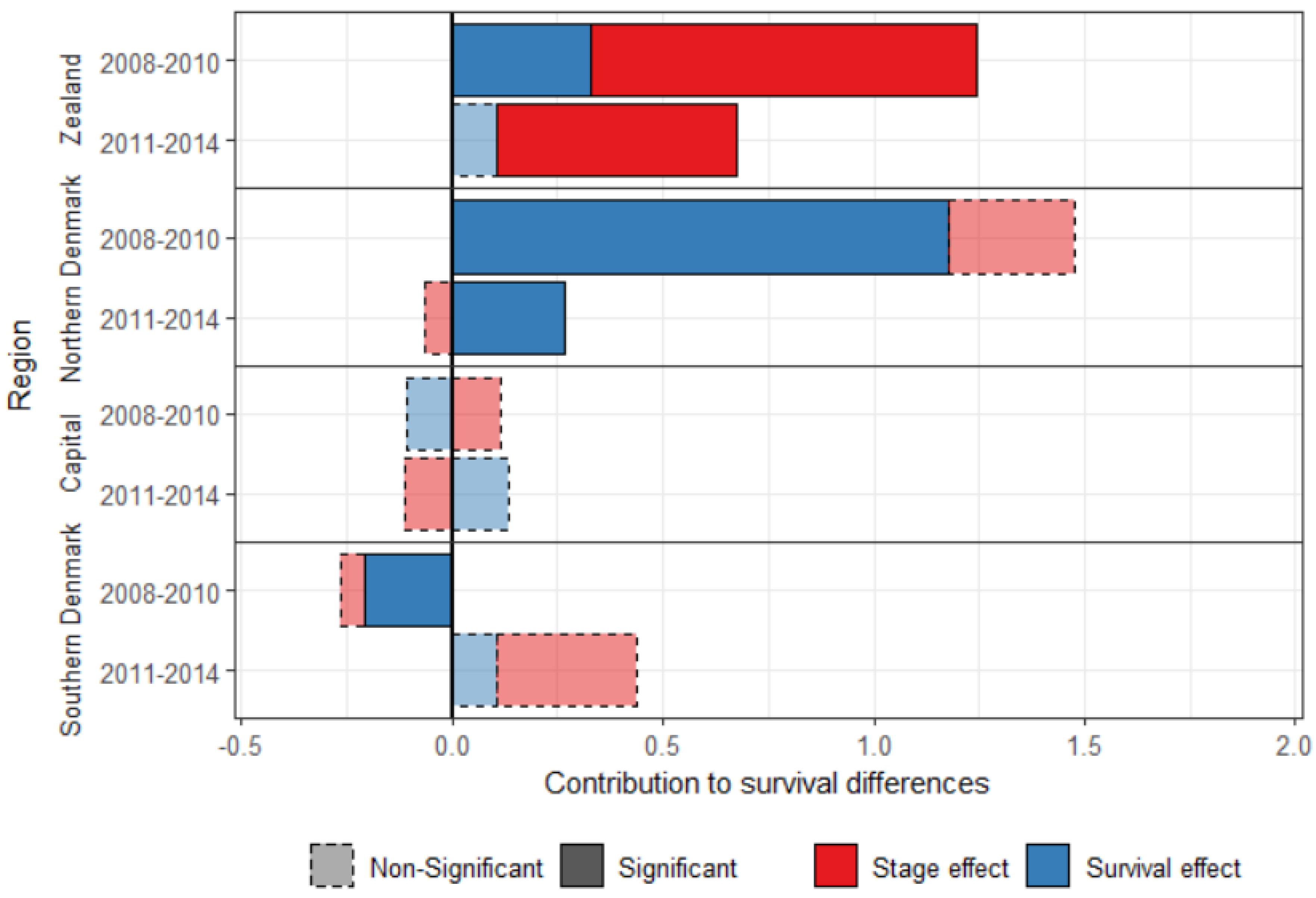
4.3. Diminishing Differences over Time
The five-year survival cannot be calculated for more recent years, but the one-year survival can be calculated for patients diagnosed with breast cancer between 2011 and 2014. Differences between Central Denmark and the other regions have decreased between the periods 2008–2010 and 2011–2014 (
Figure 2), showing evidence of progress towards equality. The survival effect was significant for three regions in 2008–2010, but only for Northern Denmark in 2011–2014, for which it decreased four-fold over the study period.
Central Denmark had an advantage over Southern Denmark in the most recent period, but it is small (0.44 percent points), and the contributions are not significant.
The stage effect was still significant for Zealand in the most recent period, but smaller, and explains 84.6% of the difference in breast cancer survival with Central Denmark in 2011–2014.
5. Comparison with the Cox Proportional Hazard Model
The Kitagawa decomposition differs from the (commonly-used) Cox proportional hazard (CPH) model, and other types of regression models, in important ways (
Table 5).
First, the CPH model assesses which variables influence survival. For example, an increase in the age and stage at diagnosis increases the hazard (
Table 6) and decreases survival. In contrast, the decomposition method quantifies contributions of specific variables to the difference in survival between two populations.
Second, the CPH, and other forms of regression model, estimate coefficients. The coefficients act multiplicatively on the variables’ value and are used to predict survival for an individual with specific characteristics. The decomposition produces variable-specific contributions to the difference, summing up to the total survival difference. The contributions are generally an aggregated value for each variable, without distinction for the value of the variable (e.g., stages 1 to 4).
Third, the CPH estimates relative differences between values of a variable. For example, the ratio of the hazard functions of Zealand/Central Denmark is higher than 1 (
Table 6), meaning that people diagnosed with breast cancer in Zealand had a higher hazard than people with similar characteristics in Central Denmark. This approach does not inform, however, on why this difference between region occured. In contrast, the decomposition approach uses absolute differences between two populations. The use of absolute rather than relative differences allows one to quantify the survival that could be gained by improving, for example, stage at diagnosis to the level of a reference region or population: If Zealand had the same stage at diagnosis distribution as Central Denmark in 2008-2010, the five-year crude survival probability (
Table 3) would have been 79.80% rather than 78.61%. It also allows one to quantify directly the number of deaths that could be avoided if one of the components were to change. For example, giving Zealand the stage-at-diagnosis distribution of Central Denmark reduces the number of deaths due to breast cancer one year after the diagnosis by 16.0% for patients diagnosed between 2008 and 2010 (23 deaths) and by 5.6% five years after the diagnosis (30 deaths). Most articles tend to report relative measures only, but existing recommendations suggest reporting both relative and absolute measures [
36].
Fourth, the CPH model makes structural assumptions, primarily the hazards are proportional. With the decomposition model, no distributional or structural assumptions are required: The compositions and component-specific rates or probabilities observed in two populations are directly compared and their effects on survival are quantified.
Finally, the CPH model requires individual data, while the decomposition method can also be used on aggregated data. However, if aggregated data are used, new ways to calculate confidence intervals should be found other than that suggested in the paper.
The CPH and decomposition models serve different purposes and the use of one rather than the other should be determined by the aim of the study. If the aim is to understand the determinants of cancer survival, the CPH model, or other regression models, should be used. However, if the aim is to understand differences in survival between populations or quantify potential gains in survival by modifying one variable, the introduced decomposition method can be preferable. Both methods could also be used to complement each other.
6. Discussion
We presented a non-parametric decomposition method that uncovers the causes of differences in cancer survival probabilities between populations. In the test case of the Danish regions, we found that later stage at diagnosis explained a large share of the difference in breast cancer survival between Zealand and Central Denmark, which tentatively suggests that Zealand could improve cancer survival by diagnosing at an earlier stage, in addition to recent and ongoing improvements.
By the end of 2007, all Danish regions were required to start a breast cancer screening program, the rollout being completed in 2009. However, some differences between regions remained. Zealand recorded more fluctuations in the breast cancer detection rates over time (in contrast to the other regions) with a particularly low detection rate of 0.53% compared with the national average of 0.61% in the fourth screening round (2014–2015) [
37]. This could explain, in part, the later stages at diagnosis in Zealand and might be caused by a shortage of experienced radiologist in the region [
37].
Lower socioeconomic status has been associated with later cancer stage at diagnosis [
38]. Zealand has the highest proportion of residents with low education level among the Danish regions [
39], which could also explain its more adverse stage-at-diagnosis distribution. However, Ibfelt et al. (2018) [
17] found that even after controlling for differences in socioeconomic status (education and income), the odds ratio of being diagnosed at a later stage remained higher in Zealand than in the Capital region for malignant melanoma. This led the authors to suspect differences in the referral process to specialized care between regions. Other possible explanations include fewer specialized doctors in the outer regions, such as Zealand and Northern Denmark, and other unmeasured social, cultural and behavioral factors [
17]. Patient awareness of breast cancer symptoms is high in Denmark, especially in highly educated respondents [
40], which suggests that patient delay may be a factor in regions where education is generally lower.
Given the importance of family doctors in the Danish healthcare system, without whose referral one cannot consult a specialist, regional differences in organization, attitudes and number of GPs are likely to lead to some differences in stage distribution. Looking into regional differences in England, Maclean et al. (2015) [
41] found that for female breast cancer, being in a practice with short waiting times until referral or detection was associated with a lower proportion of patients diagnosed in stage 3 or 4 rather than stage 1 or 2. Membership of a practice where people thought it less easy to book an appointment was associated with a higher percentage diagnosed later. It would be helpful to know how this translates to the case of Zealand GPs. Presumably, such an effect will depend on the quality, attitudes and organization of family doctors, which may lead to regional differences.
As for stage-specific survival, there are known cases where, while treatment was in principle available, the application of active treatment was different between regions in one country, such as lung cancer in England [
42]. However, the Danish Breast Cancer Group (DBCG) established mandatory treatment guidelines, especially regarding the surgical treatment and the (neo)adjuvant treatment [
43] (DBCG guidelines,
www.DBCG.dk). In principle, patients should get the same treatment across all Denmark’s hospitals. Furthermore, DBCG regularly publish a quality indicator report to identify any variation in the treatment of early breast cancer, showing only small differences [
43] (DBCG quality indicator report,
www.DBCG.dk). Differences in treatment are, thus, unlikely to cause the differences observed in stage-specific survival between Danish regions (survival effect).
It has also been found that rural dwellers have poorer cancer survival [
44]. It is unclear why this would apply only to Northern Denmark, although the vicinity of the capital may make Zealand effectively a little less “rural” than Northern Denmark.
In 2007, many changes occurred regarding breast cancer diagnosis and treatment in Denmark, including the screening program, updates of the national guidelines, and the new regional scheme. These changes might be the cause for the decreasing differences across regions over time, but we cannot assess if or which of these changes are responsible for the convergence, or if it can be the result of previous programs.
More information could be added in the decomposition to further explain the regional differences. If additional data were available, possible extensions could include the compositional difference of socioeconomic status, smoking habits, or medical treatments. The contributions of unspecified components are grouped in the survival-effect, or in the composition effects if an unspecified composition correlates with the age or stage compositions. For example, in
Table 3, if the stage at diagnosis was not included in the analysis, the survival effect would be approximated by the sum of the survival and stage effects (e.g., 1.24 for the one-year survival) and the age effect would be the sum of the age and interaction effects (e.g., 0.38 for the one-year survival). This is similar to unmeasured confounders in regression analysis.

 and
and 
{kind=link}
{kind=link}

