The Association between Mortality-to-Incidence Ratios and Health Expenditures in Brain and Nervous System Cancers


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Involving Human Participants
2.2. Informed Consent
2.3. Declarations
3. Results
3.1. Incidence and Mortality of Brain and Nervous System Cancers According to Region
3.2. Incidence and Mortality of Brain and Nervous System Cancers According to Country
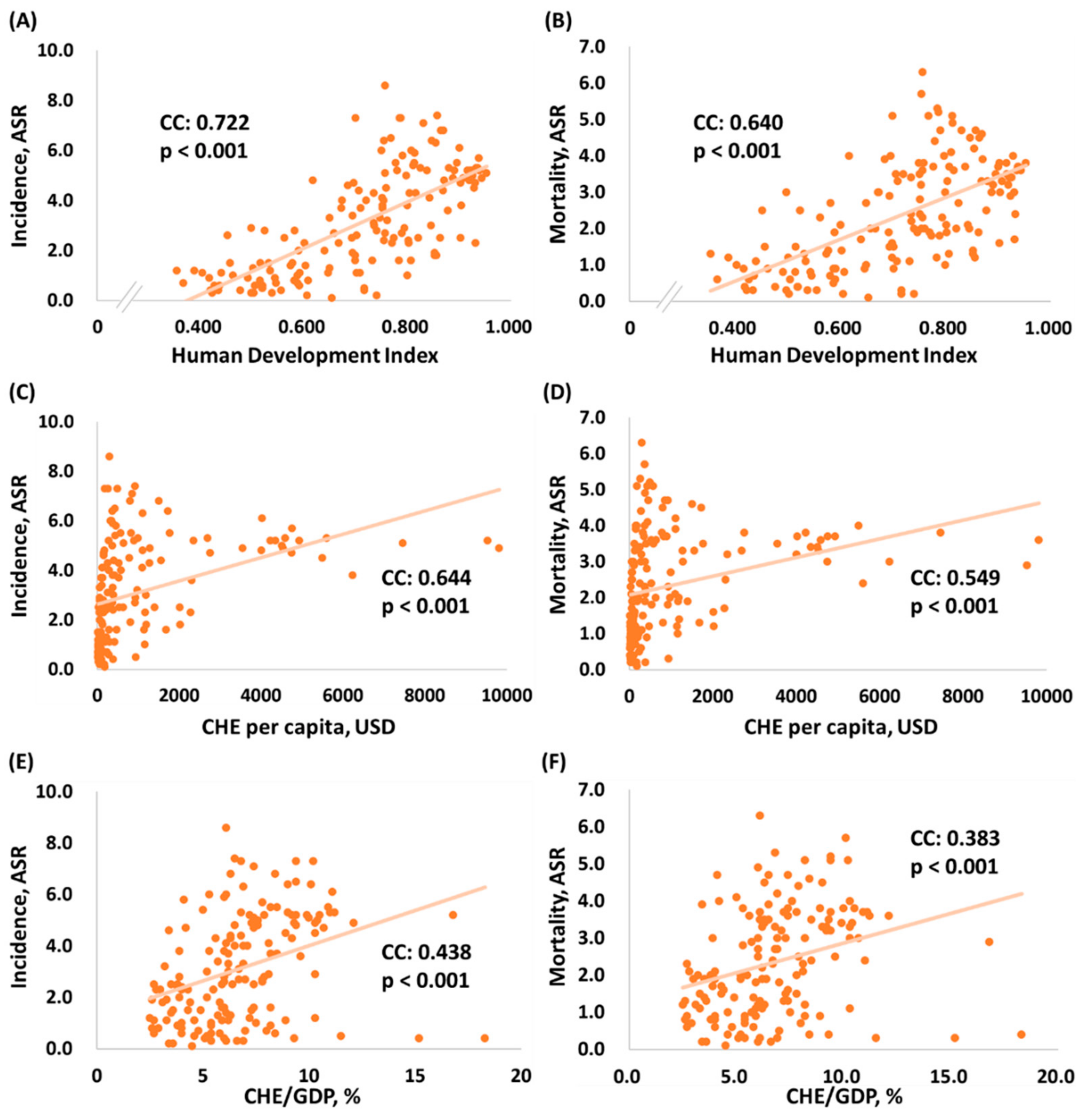
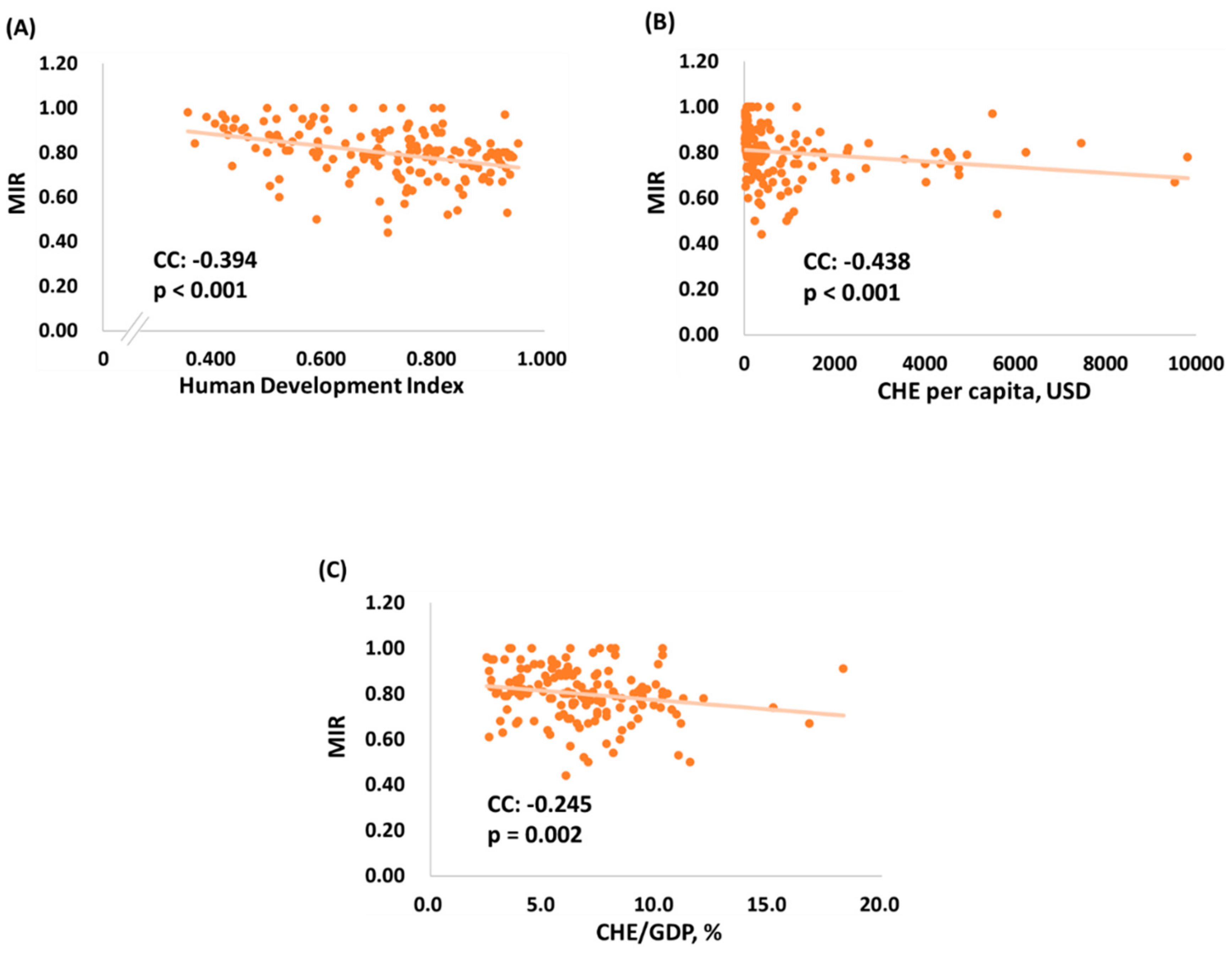
3.3. Association among Human Development Index, CHE Per Capita, CHE/GDP, and MIR in Different Countries
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ASR: | age-standardized rate |
| CC: | correlation coefficient |
| CHE: | current health expenditure |
| CHE/GDP: | current health expenditure as percentage of gross domestic product |
| CR: | crude rate |
| cum. risk: | cumulative risk |
| MIR: | mortality-to-incidence ratio |
| WHO: | World Health Organization |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Fallahi, P.; Foddis, R.; Cristaudo, A.; Antonelli, A. High risk of brain tumors in farmers: A mini-review of the literature, and report of the results of a case control study. Clin. Ter. 2017, 168, e290–e292. [Google Scholar] [PubMed]
- Piel, C.; Pouchieu, C.; Tual, S.; Migault, L.; Lemarchand, C.; Carles, C.; Boulanger, M.; Gruber, A.; Rondeau, V.; Marcotullio, E.; et al. Central nervous system tumors and agricultural exposures in the prospective cohort AGRICAN. Int. J. Cancer 2017, 141, 1771–1782. [Google Scholar] [CrossRef] [PubMed]
- Oddone, E.; Scaburri, A.; Bai, E.; Modonesi, C.; Stracci, F.; Marchionna, G.; Crosignani, P.; Imbriani, M. Occupational brain cancer risks in Umbria (Italy), with a particular focus on steel foundry workers. G. Ital. Med. Lav. Ergon. 2014, 36, 111–117. [Google Scholar] [PubMed]
- Preston, D.L.; Ron, E.; Yonehara, S.; Kobuke, T.; Fujii, H.; Kishikawa, M.; Tokunaga, M.; Tokuoka, S.; Mabuchi, K. Tumors of the nervous system and pituitary gland associated with atomic bomb radiation exposure. J. Natl. Cancer Inst. 2002, 94, 1555–1563. [Google Scholar] [CrossRef] [PubMed]
- Galmarini, D.; Galmarini, C.M.; Galmarini, F.C. Cancer chemotherapy: A critical analysis of its 60 years of history. Crit. Rev. Oncol. Hematol. 2012, 84, 181–199. [Google Scholar] [CrossRef]
- Lam, T.C.; Sahgal, A.; Lo, S.S.; Chang, E.L. An update on radiation therapy for brain metastases. Chin. Clin. Oncol. 2017, 6, 35. [Google Scholar] [CrossRef]
- Shah, V.; Kochar, P. Brain Cancer: Implication to Disease, Therapeutic Strategies and Tumor Targeted Drug Delivery Approaches. Recent Pat. Anticancer Drug Discov. 2018, 13, 70–85. [Google Scholar] [CrossRef]
- Dunn-Pirio, A.M.; Vlahovic, G. Immunotherapy approaches in the treatment of malignant brain tumors. Cancer 2017, 123, 734–750. [Google Scholar] [CrossRef]
- Kang, C.; Sun, Y.; Zhu, J.; Li, W.; Zhang, A.; Kuang, T.; Xie, J.; Yang, Z. Delivery of Nanoparticles for Treatment of Brain Tumor. Curr. Drug Metab. 2016, 17, 745–754. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.; Lee, S.; Nhung, B.C.; Suh, M.; Park, B.; Jun, J.K.; Choi, K.S. Cancer mortality-to-incidence ratio as an indicator of cancer management outcomes in Organization for Economic Cooperation and Development countries. Epidemiol. Health 2017, 39, e2017006. [Google Scholar] [CrossRef] [PubMed]
- Sunkara, V.; Hebert, J.R. The application of the mortality-to-incidence ratio for the evaluation of cancer care disparities globally. Cancer 2016, 122, 487–488. [Google Scholar] [CrossRef]
- Cordero-Morales, A.; Savitzky, M.J.; Stenning-Persivale, K.; Segura, E.R. Conceptual considerations and methodological recommendations for the use of the mortality-to-incidence ratio in time-lagged, ecological-level analysis for public health systems-oriented cancer research. Cancer 2016, 122, 486–487. [Google Scholar] [CrossRef] [PubMed]
- Asadzadeh Vostakolaei, F.; Karim-Kos, H.E.; Janssen-Heijnen, M.L.; Visser, O.; Verbeek, A.L.; Kiemeney, L.A. The validity of the mortality to incidence ratio as a proxy for site-specific cancer survival. Eur. J. Public Health 2011, 21, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, T.M.; Drain, C.M.; Grimm, J. Optical Imaging of Ionizing Radiation from Clinical Sources. J. Nucl. Med. 2016, 57, 1661–1666. [Google Scholar] [CrossRef] [PubMed]
- Tang, F.R.; Loganovsky, K. Low dose or low dose rate ionizing radiation-induced health effect in the human. J. Environ. Radioact. 2018, 192, 32–47. [Google Scholar] [CrossRef]
- Bortkiewicz, A.; Gadzicka, E.; Szymczak, W. Mobile phone use and risk for intracranial tumors and salivary gland tumors—A meta-analysis. Int. J. Occup. Med. Environ. Health 2017, 30, 27–43. [Google Scholar] [CrossRef]
- Jakovljevic, M.M. Comparison of historical medical spending patterns among the BRICS and G7. J. Med. Econ. 2016, 19, 70–76. [Google Scholar] [CrossRef]
- Kar, S.; Majumder, D.D. A mathematical theory of shape and neuro-fuzzy methodology-based diagnostic analysis: A comparative study on early detection and treatment planning of brain cancer. Int. J. Clin. Oncol. 2017, 22, 667–681. [Google Scholar] [CrossRef]
- Abrol, S.; Kotrotsou, A.; Salem, A.; Zinn, P.O.; Colen, R.R. Radiomic Phenotyping in Brain Cancer to Unravel Hidden Information in Medical Images. Top. Magn. Reson. Imaging 2017, 26, 43–53. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Region | New Cases | Deaths | ||||||
|---|---|---|---|---|---|---|---|---|
| Number | Rank | % of All Cancers 1 | Cum. Risk 2 | Number | Rank | % of All Cancers 1 | Cum. Risk 2 | |
| All regions | 296,851 | 18 | 1.84 | 0.31 | 241,037 | 13 | 2.73 | 0.30 |
| Africa | 16,956 | 16 | 1.84 | 0.18 | 14,225 | 15 | 2.35 | 0.17 |
| Asia | 156,217 | 16 | 1.91 | 0.31 | 129,483 | 12 | 2.52 | 0.27 |
| Europe | 64,639 | 17 | 1.72 | 0.56 | 53,027 | 12 | 2.94 | 0.44 |
| Latin America and the Caribbean | 29,539 | 14 | 2.36 | 0.42 | 22,312 | 10 | 3.70 | 0.33 |
| North America | 27,062 | 19 | 1.50 | 0.52 | 19,973 | 10 | 3.16 | 0.36 |
| Oceania | 2438 | 19 | 1.42 | 0.47 | 2,017 | 12 | 3.21 | 0.40 |
| Country | Human Development Index | Current Health Expenditure | Incidence | Mortality | Mortality-to-Incidence Ratio | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Score | Rank | Per Capita | /GDP (%) 1 | ASR 2 | CR 3 | Cum. Risk 4 | ASR 2 | CR 3 | Cum. Risk 4 | ||
| North Macedonia | 0.757 | 80 | 295 | 6.1 | 8.6 | 12.0 | 1.0 | 6.3 | 9.6 | 0.8 | 0.80 |
| Lithuania | 0.858 | 35 | 923 | 6.5 | 7.4 | 11.0 | 0.8 | 4.7 | 7.4 | 0.6 | 0.67 |
| Bosnia and Herzegovina | 0.768 | 77 | 431 | 9.4 | 6.5 | 10.5 | 0.8 | 5.1 | 8.7 | 0.7 | 0.83 |
| Greece | 0.870 | 31 | 1505 | 8.4 | 6.8 | 10.4 | 0.8 | 4.6 | 7.7 | 0.6 | 0.74 |
| Croatia | 0.831 | 46 | 852 | 7.4 | 7.1 | 10.3 | 0.8 | 4.7 | 7.9 | 0.6 | 0.77 |
| Serbia | 0.787 | 67 | 491 | 9.4 | 7.3 | 10.3 | 0.8 | 5.2 | 8.3 | 0.6 | 0.81 |
| Poland | 0.865 | 33 | 797 | 6.3 | 6.8 | 9.7 | 0.7 | 4.5 | 7.3 | 0.6 | 0.75 |
| Albania | 0.785 | 68 | 266 | 6.8 | 7.3 | 9.7 | 0.8 | 5.3 | 7.6 | 0.7 | 0.78 |
| Portugal | 0.847 | 41 | 1722 | 9.0 | 6.4 | 9.5 | 0.7 | 4.5 | 7.6 | 0.5 | 0.80 |
| Republic of Moldova | 0.700 | 112 | 186 | 10.2 | 7.3 | 9.2 | 0.7 | 5.1 | 6.8 | 0.6 | 0.74 |
| Bulgaria | 0.813 | 51 | 572 | 8.2 | 5.5 | 8.8 | 0.6 | 5.1 | 8.8 | 0.6 | 1.00 |
| France | 0.901 | 24 | 4026 | 11.1 | 6.1 | 8.5 | 0.7 | 3.7 | 5.7 | 0.4 | 0.67 |
| Slovakia | 0.855 | 38 | 1108 | 6.9 | 6.3 | 8.5 | 0.7 | 4.2 | 6.4 | 0.5 | 0.75 |
| Montenegro | 0.814 | 50 | 382 | 6.0 | 5.9 | 8.5 | 0.7 | 4.9 | 7.6 | 0.7 | 0.89 |
| Romania | 0.811 | 52 | 442 | 5.0 | 5.4 | 8.3 | 0.6 | 4.1 | 6.7 | 0.5 | 0.81 |
| Italy | 0.880 | 28 | 2700 | 9.0 | 5.3 | 8.2 | 0.6 | 3.3 | 6.0 | 0.4 | 0.73 |
| Slovenia | 0.896 | 25 | 1772 | 8.5 | 5.5 | 8.2 | 0.6 | 3.5 | 6.4 | 0.5 | 0.78 |
| Armenia | 0.755 | 83 | 366 | 10.1 | 6.4 | 8.1 | 0.7 | 5.7 | 7.5 | 0.7 | 0.93 |
| Germany | 0.936 | 5 | 4592 | 11.2 | 5.3 | 7.8 | 0.6 | 3.6 | 6.1 | 0.4 | 0.78 |
| Spain | 0.891 | 26 | 2354 | 9.2 | 5.2 | 7.7 | 0.6 | 3.2 | 5.3 | 0.4 | 0.69 |
| Belarus | 0.808 | 53 | 352 | 6.1 | 6.0 | 7.7 | 0.6 | 3.7 | 5.3 | 0.4 | 0.69 |
| Cuba | 0.777 | 73 | 826 | 10.9 | 5.5 | 7.7 | 0.6 | 3.7 | 5.5 | 0.4 | 0.71 |
| Hungary | 0.838 | 45 | 894 | 7.2 | 5.2 | 7.4 | 0.6 | 3.7 | 6.0 | 0.4 | 0.81 |
| Czechia | 0.888 | 27 | 1284 | 7.3 | 4.9 | 7.3 | 0.5 | 3.0 | 5.0 | 0.4 | 0.68 |
| Ireland | 0.938 | 4 | 4757 | 7.8 | 5.7 | 7.3 | 0.6 | 3.7 | 5.1 | 0.5 | 0.70 |
| Switzerland | 0.944 | 2 | 9818 | 12.1 | 4.9 | 7.3 | 0.6 | 3.6 | 5.7 | 0.4 | 0.78 |
| United Kingdom | 0.922 | 14 | 4356 | 9.9 | 5.2 | 7.2 | 0.6 | 3.4 | 5.4 | 0.4 | 0.75 |
| Belgium | 0.916 | 17 | 4228 | 10.5 | 5.2 | 7.1 | 0.5 | 3.8 | 5.7 | 0.4 | 0.80 |
| Sweden | 0.933 | 7 | 5600 | 11.0 | 5.3 | 7.0 | 0.5 | 2.4 | 3.7 | 0.3 | 0.53 |
| Estonia | 0.871 | 30 | 1112 | 6.5 | 4.8 | 6.9 | 0.5 | 3.9 | 5.8 | 0.5 | 0.84 |
| Georgia | 0.780 | 70 | 281 | 7.9 | 5.2 | 6.9 | 0.6 | 4.4 | 6.2 | 0.5 | 0.90 |
| Finland | 0.920 | 15 | 4005 | 9.4 | 4.8 | 6.8 | 0.5 | 3.2 | 5.1 | 0.4 | 0.75 |
| Australia | 0.939 | 3 | 4934 | 9.4 | 5.2 | 6.8 | 0.6 | 3.7 | 5.4 | 0.5 | 0.79 |
| Austria | 0.908 | 20 | 4536 | 10.3 | 4.9 | 6.8 | 0.5 | 3.3 | 5.4 | 0.4 | 0.79 |
| Norway | 0.953 | 1 | 7464 | 10.0 | 5.1 | 6.8 | 0.5 | 3.8 | 5.7 | 0.5 | 0.84 |
| Denmark | 0.929 | 11 | 5497 | 10.3 | 4.5 | 6.8 | 0.5 | 4.0 | 6.6 | 0.5 | 0.97 |
| Netherlands | 0.931 | 10 | 4746 | 10.7 | 4.7 | 6.7 | 0.5 | 3.0 | 4.9 | 0.4 | 0.73 |
| Canada | 0.926 | 12 | 4508 | 10.4 | 5.0 | 6.6 | 0.5 | 3.4 | 5.3 | 0.4 | 0.80 |
| New Zealand | 0.917 | 16 | 3554 | 9.3 | 4.9 | 6.5 | 0.5 | 3.5 | 5.0 | 0.4 | 0.77 |
| United States of America | 0.924 | 13 | 9536 | 16.8 | 5.2 | 6.4 | 0.5 | 2.9 | 4.3 | 0.4 | 0.67 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, T.-H.; Sung, W.-W.; Chan, L.; Lee, H.-L.; Chen, S.-L.; Huang, Y.-H.; Kwan, A.-L. The Association between Mortality-to-Incidence Ratios and Health Expenditures in Brain and Nervous System Cancers. Int. J. Environ. Res. Public Health 2019, 16, 2739. https://doi.org/10.3390/ijerph16152739
Lee T-H, Sung W-W, Chan L, Lee H-L, Chen S-L, Huang Y-H, Kwan A-L. The Association between Mortality-to-Incidence Ratios and Health Expenditures in Brain and Nervous System Cancers. International Journal of Environmental Research and Public Health. 2019; 16(15):2739. https://doi.org/10.3390/ijerph16152739
Chicago/Turabian StyleLee, Tsung-Han, Wen-Wei Sung, Lung Chan, Hsiang-Lin Lee, Sung-Lang Chen, Yu-Hui Huang, and Aij-Lie Kwan. 2019. "The Association between Mortality-to-Incidence Ratios and Health Expenditures in Brain and Nervous System Cancers" International Journal of Environmental Research and Public Health 16, no. 15: 2739. https://doi.org/10.3390/ijerph16152739
APA StyleLee, T.-H., Sung, W.-W., Chan, L., Lee, H.-L., Chen, S.-L., Huang, Y.-H., & Kwan, A.-L. (2019). The Association between Mortality-to-Incidence Ratios and Health Expenditures in Brain and Nervous System Cancers. International Journal of Environmental Research and Public Health, 16(15), 2739. https://doi.org/10.3390/ijerph16152739