How Does the Built Environment in Compact Metropolitan Cities Affect Health? A Systematic Review of Korean Studies


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility
- -
- Studies conducted in Korean metropolitan cities.
- -
- Studies that objectively (e.g., geographic information systems) or subjectively (i.e., survey, scale) measured the BE reported as independent variables.
- -
- Studies that objectively (e.g., medical examination) or subjectively measured health-related outcomes (e.g., symptoms, mortality, physical, mental, and social functioning, perceived health status, health-related behaviors) [18].
- -
- Peer-reviewed and fully published articles.
- -
- Published articles written in Korean or English.
- -
- Studies that objectively or subjectively measured indoor facilities and working facilities reported as independent variables.
- -
- Studies that objectively or subjectively measured the natural environment (i.e., non-man-made physical environment) reported as independent variables.
- -
- Systematic reviews.
- -
- Qualitative studies.
- -
- Studies conducted to develop the BE measuring instrument that does not analyze the correlation with health.
- -
- Descriptive studies with only bivariate analysis.
2.3. Information Sources and Search Terms
2.4. Data Extraction
2.5. Synthesis of Results
3. Results
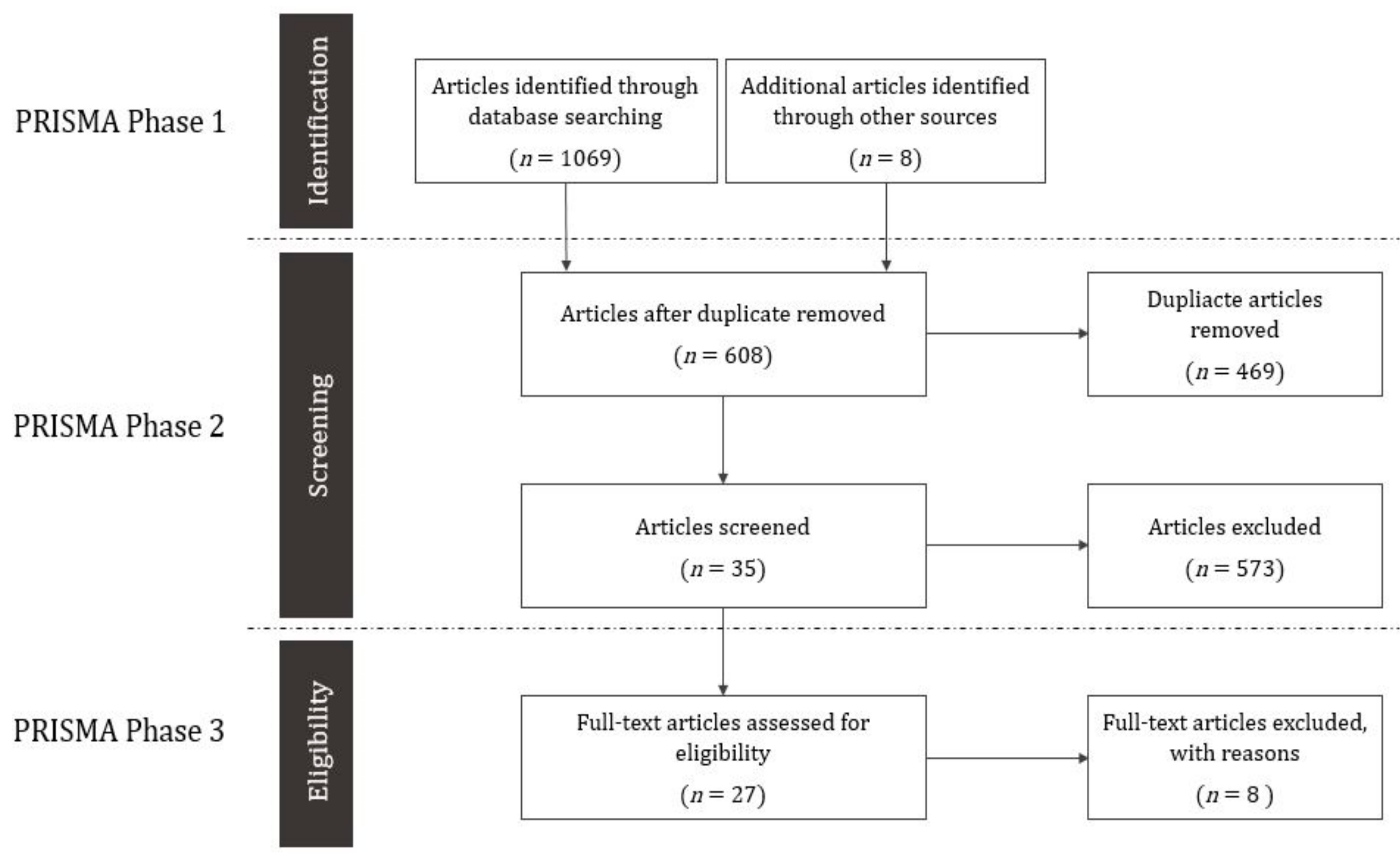
3.1. Study Selection
3.2. Study Characteristics
3.3. Health Variables Related to the Built Environment
3.4. Associations between the Built Environment Characteristics and Health-Related Outcomes
3.4.1. Associations between Land Use and Health-Related Outcomes
3.4.2. Associations between Street Environment and Health-Related Outcomes
3.4.3. Associations between Transportation Infrastructure and Health-Related Outcomes
3.4.4. Associations of Green and Open Spaces with Health-Related Outcomes
3.4.5. Associations between Neighborhood Facilities and Health-Related Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cohen, D.A.; Han, B.; Kraus, L.; Young, D.R. The contribution of the built environment to physical activity among young women. Environ. Behav. 2018, 51, 811–817. [Google Scholar] [CrossRef]
- Gose, M.; Plachta-Danielzik, S.; Willié, B.; Johannsen, M.; Landsberg, B.; Müller, M.J. Longitudinal influences of neighbourhood built and social environment on children’s weight status. Int. J. Environ. Res. Public Health 2013, 10, 5083–5096. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Report on Urban Health: Equitable, Healthier Cities for Sustainable Development; World Health Organization: Geneva, Switzerland, 2016; pp. 67–91. [Google Scholar]
- Galea, S.; Freudenberg, N.; Vlahov, D. Cities and population health. Soc. Sci. Med. 2005, 60, 1017–1033. [Google Scholar] [CrossRef] [PubMed]
- Capolongo, S.; Rebecchi, A.; Dettori, M.; Appolloni, L.; Azara, A.; Buffoli, M.; Ferrante, M.; Moscato, U.; Oberti, I.; Paglione, L.; et al. Healthy design and urban planning strategies, actions, and policy to achieve salutogenic cities. Int. J. Environ. Res. Public Health 2018, 15, 2698. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.D.; Rutter, H.; Compernolle, S.; Glonti, K.; Oppert, J.M.; Charreire, H.; Lakerveld, J.; De Bourdeaudhuij, I.; Brug, J.; Nijpels, G. Obesogenic environments: A systematic review of the association between the physical environment and adult weight status, the SPOTLIGHT project. BMC Public Health 2014, 14, 233–247. [Google Scholar] [CrossRef]
- Vlahov, D.; Freudenberg, N.; Proietti, F.; Ompad, D.; Quinn, A.; Nandi, V.; Galea, S. Urban as a determinant of health. J. Urban Health 2007, 84, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Melis, G.; Gelormino, E.; Marra, G.; Ferracin, E.; Costa, G. The effects of the urban built environment on mental health: A cohort study in a large northern Italian city. Int. J. Environ. Res. Public Health 2015, 12, 14898–14915. [Google Scholar] [CrossRef]
- Evans, G.W. The built environment and mental health. J. Urban Health 2003, 80, 536–555. [Google Scholar] [CrossRef]
- Mazumdar, S.; Learnihan, V.; Cochrane, T.; Davey, R. The built environment and social capital: A systematic review. Environ. Behav. 2018, 50, 119–158. [Google Scholar] [CrossRef]
- OECD. Measuring the performance of a compact city. In Compact City Policies: A Comparative Assessment; OECD Publishing: Paris, France, 2012; pp. 79–114. [Google Scholar]
- Ministry of the Interior and Safety. Local Autonomy Act. Available online: https://elaw.klri.re.kr/kor_mobile/viewer.do?hseq=44511&type=sogan&key=15 (accessed on 11 June 2019).
- World Health Organization. Global Health Observatory (GHO) data. Available online: https://www.who.int/gho/countries/kor/en/ (accessed on 14 July 2019).
- Statistics Korea. Community Health Survey. Available online: http://kosis.kr/statisticsList/statisticsListIndex.do?menuId=M_01_01&vwcd=MT_ZTITLE&parmTabId=M_01_01 (accessed on 14 July 2019).
- Kil, H.M.; Park, H.S. An analysis of the health affinity of the urban environment in the Gyeonggi province based on big data. Resid. Environ.: J. Resid. Environ. Inst. Korea 2018, 16, 279–299. [Google Scholar] [CrossRef]
- Lee, S. Research trends and limitations of the integrated study of urban planning and public health for a healthy community. Seoul Stud. 2010, 11, 15–33. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Terwee, C.B.; Prinsen, C.A.C.; Garotti, M.R.; Suman, A.; De Vet, H.C.W.; Mokkink, L.B. The quality of systematic reviews of health-related outcome measurement instruments. Qual. Life Res. 2016, 25, 767–779. [Google Scholar] [CrossRef] [PubMed]
- Casagrande, S.S.; Whitt-Glover, M.C.; Lancaster, K.J.; Odoms-Young, A.M.; Gary, T.L. Built environment and health behaviors among African Americans: A systematic review. Am. J. Prev. Med. 2009, 36, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Shirazi, M.; Falahat, S. Compact urban form, question or solution? Examining the compact city in the Middle Eastern context: Challenges and opportunities. Int. J. Urban Sustain. Dev. 2012, 4, 246–259. [Google Scholar] [CrossRef]
- Yoo, S.; Kim, D.H. Perceived urban neighborhood environment for physical activity of older adults in Seoul, Korea: A multimethod qualitative study. Prev. Med. 2017, 103, S90–S98. [Google Scholar] [CrossRef] [PubMed]
- Rothman, L.; Macpherson, A.K.; Ross, T.; Buliung, R.N. The decline in active school transportation (AST): A systematic review of the factors related to AST and changes in school transport over time in North America. Prev. Med. 2018, 111, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, E.; Hinckson, E.; Witten, K.; Smith, M. Associations of children’s active school travel with perceptions of the physical environment and characteristics of the social environment: A systematic review. Health Place 2018, 54, 118–131. [Google Scholar] [CrossRef]
- Kang, S.J.; Kim, Y.H. The effect of individual, social, and physical environment variables on older adults’ physical activity. KJSP 2011, 22, 113–124. [Google Scholar]
- Kim, Y.J.; Ahn, K.H. Influences of neighborhood’s physical environments on physical and mental health to the elderly. Urban Des. 2011, 12, 89–99. [Google Scholar]
- Kim, E.J.; Kang, M.G. Effects of built environmental factors on obesity and self-reported health status in Seoul metropolitan area using spatial regression model. Korea Spat. Plan. Rev. 2011, 68, 85–98. [Google Scholar]
- Kim, E.J.; Kang, M.G. Effects of built environment and individual characteristics on health condition. J. Korean Reg. Sci. Assoc. 2011, 27, 27–42. [Google Scholar]
- Sung, H.G. A study on the impacts of residential neighborhood built environment on personal health indicators-focused on the planning elements of transit-oriented development. J. Korea Plan. Assoc. 2011, 46, 235–251. [Google Scholar] [CrossRef]
- Kim, H.S.; Miyashita, M.; Harada, K.; Park, J.H.; So, J.M.; Nakamura, Y. Psychological, social, and environmental factors associated with utilization of senior centers among older adults in Korea. J. Prev. Med. Public Health 2012, 45, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.E.; Lee, S.H. A multilevel modeling of factors affecting depression among older Korean adults. Ment. Health Soc. Work 2012, 40, 322–351. [Google Scholar]
- Lee, H.Y.; Joo, Y. An analysis of the effects of neighborhood characteristics on standardized mortality rates in the capital region. JKUGS 2012, 15, 23–37. [Google Scholar]
- Lee, H.S.; Shepley, M.M. Perceived neighborhood environments and leisure-time walking among Korean adults: An application of the theory of planned behavior. HERD 2012, 5, 99–110. [Google Scholar] [CrossRef]
- Choi, T.K.; Kim, H.S. The influence of physical attributes of cities on personal health conditions-the case of 5 metropolitan cities, Korea. J. Korea Plan. Assoc. 2013, 48, 191–203. [Google Scholar]
- Kim, W.J.; Kim, T.Y. A study on the neighborhood physical and social environments and health-the mediating role of perceived environments. J. Community Welf. 2013, 46, 23–47. [Google Scholar] [CrossRef]
- Park, S.; Choi, B.Y.; Wang, Y.; Colantuoni, E.; Gittelsohn, J. School and neighborhood nutrition environment and their association with students’ nutrition behaviors and weight status in Seoul, South Korea. J. Adolesc. Health 2013, 53, 655–662. [Google Scholar] [CrossRef]
- Park, J.Y.; Shin, H.K.; Choi, J.S.; Oh, H.S.; Choi, K.H.; Park, S.M.; Cho, B. Do people have healthier lifestyles in greener environments? An analysis of the association between green environments and physical activity in seven large Korean cities. Korean J. Fam. Med. 2013, 34, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Choi, B. The relationship between physical environment and mental health of the urban and rural adolescents. J. Korean Hous. Assoc. 2014, 25, 73–83. [Google Scholar]
- Sung, H.G.; Lee, S.; Cheon, S. Moderation effects of community physical environment factors on walking activity: With case study of Seoul, Korea. Urban Des. 2014, 15, 173–189. [Google Scholar]
- Jung, Y.J.; Lee, S.K. The study on the causality among built environment, social relationship, and health of the elderly. J. Korean Reg. Dev. Assoc. 2015, 27, 75–94. [Google Scholar]
- Kim, E.J.; Kim, T.H. Correlations between the built environment and residents’ health in Daegu. JKUSGS 2015, 18, 107–120. [Google Scholar]
- Lee, W.S.; Jung, S.G.; Park, Y.E. The effect of neighborhood environmental perception on park use for health improvement-the case of Suseong-gu in Daegu city. J. Korean Inst. Landsc. Archit. 2015, 43, 98–108. [Google Scholar] [CrossRef]
- Yoo, C.; Lee, S. Neighborhood environment, social capital, and social sustainability of community: Explanatory study on causal relationships. J. Korea Plan. Assoc. 2015, 50, 5–23. [Google Scholar] [CrossRef]
- Cho, H.; Lee, S. Impacts of subjectively measured neighborhood environment and walking activity on the formation of social capital: The case study of four municipalities in Seoul, Korea. J. Korea Plan. Assoc. 2016, 51, 59–77. [Google Scholar] [CrossRef]
- Chun, H.J. A study on the effect of urban environment using GIS and spatial econometric models on residents’ health. Resid. Environ.: J. Resid. Environ. Inst. Korea 2016, 14, 109–118. [Google Scholar]
- Jang, C.K.; Jung, S.G.; Lee, W.S. Influence of physical environment perception on park use for health improvement-focused on neighborhood parks in Suseong-gu, Daegu City. J Korean Inst. Landsc. Archit. 2016, 44, 68–80. [Google Scholar] [CrossRef]
- Kim, H.; Choi, Y.; Ma, J.; Hyung, K.; Miyashita, M.; Lee, S. The neighborhood environment walkability scale for the republic of Korea: Reliability and relationship with walking. Iran J. Public Health 2016, 45, 1427–1435. [Google Scholar] [PubMed]
- Kim, H.H.; Lee, C.S.; Yu, S.D.; Lee, J.S.; Chang, J.Y.; Jeon, J.M.; Lim, Y.W.; Son, H.R.; Park, C.J.; Shin, D.C. Near-road exposure and impact of air pollution on allergic diseases in elementary school children: A cross-sectional study. Yonsei Med. J. 2016, 57, 698–713. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Lee, S. Analysis of the impacts of neighborhood environment on physical activity and health status in Seoul, Korea-application of multilevel analysis with the Korea national health and nutrition examination survey (2007–2012). J. Korea Plan. Assoc. 2016, 51, 217–239. [Google Scholar] [CrossRef]
- Lee, G.M.; Lee, W.S.; Jung, S.G.; Jang, C.K. The influence of pedestrian environment perception on pedestrian environment satisfaction and expected health promotion effects-focused on park user for health promotion. J. Korean Inst. Landsc. Archit. 2016, 44, 137–147. [Google Scholar] [CrossRef]
- Lee, E.Y.; Park, S.; Choi, B.Y. Individual, social and physical environmental correlates of physical activity and sedentary behavior among children in Seoul. Korean J. Health Educ. Promot. 2016, 33, 49–60. [Google Scholar] [CrossRef] [Green Version]
- McCormack, G.R.; Shiell, A. In search of causality: A systematic review of the relationship between the built environment and physical activity among adults. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chaudhury, H.; Campo, M.; Michael, Y.; Mahmood, A. Neighbourhood environment and physical activity in older adults. Soc. Sci. Med. 2016, 149, 104–113. [Google Scholar] [CrossRef]
- Chor, D.; Cardoso, L.O.; Nobre, A.A.; Griep, R.H.; Fonseca, M.D.J.M.; Giatti, L.; de Pina Castiglione, D.; Bensenor, I.; Del Carmen Bisi Molina, M.; Aquino, E.M.L.; et al. Association between perceived neighbourhood characteristics, physical activity and diet quality: Results of the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). BMC Public Health 2016, 16, 1–11. [Google Scholar] [CrossRef]
- Cleland, V.; Sodergren, M.; Otahal, P.; Timperio, A.; Ball, K.; Crawford, D.; Salmon, J.; McNaughton, S.A. Associations between the perceived environment and physical activity among adults aged 55–65 years: Does urban-rural area of residence matter? J. Aging Phys. Act. 2015, 23, 55–63. [Google Scholar] [CrossRef]
- Pitt, E.; Gallegos, D.; Comans, T.; Cameron, C.; Thornton, L. Exploring the influence of local food environments on food behaviours: A systematic review of qualitative literature. Public Health Nutr. 2017, 20, 1–13. [Google Scholar] [CrossRef]
- Van Hecke, L.; Deforche, B.; Van Dyck, D.; De Bourdeaudhuij, I.; Veitch, J.; Van Cauwenberg, J. Social and physical environmental factors influencing adolescents’ physical activity in urban public open spaces: A qualitative study using walk-along interviews. PLoS ONE 2016, 11, e0155686. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, M.; Thompson, J.; de Sá, T.H.; Ewing, R.; Mohan, D.; McClure, R.; Roberts, I.; Tiwari, G.; Giles-Corti, B.; Sun, X.; et al. Land use, transport, and population health: Estimating the health benefits of compact cities. Lancet 2016, 388, 2925–2935. [Google Scholar] [CrossRef]
- Brown, B.B.; Yamada, I.; Smith, K.R.; Zick, C.D.; Kowaleski-Jones, L.; Fan, J.X. Mixed land use and walkability: Variations in land use measures and relationships with BMI, overweight, and obesity. Health Place 2009, 15, 1130–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Chung, C.K.; Lee, J.; Kim, K.K.; Jekarl, J.; Yoo, S. systems thinking approach to explore the structure of urban walking and health promotion in Seoul. Korean J. Health Educ. Promot. 2018, 35, 1–16. [Google Scholar] [CrossRef]
- Congiu, T.; Sotgiu, G.; Castiglia, P.; Azara, A.; Piana, A.; Saderi, L.; Dettori, M. Built environment features and pedestrian accidents: An Italian retrospective study. Sustainability 2019, 11, 1064. [Google Scholar] [CrossRef]
- Koo, Y.S.; Song, J.Y.; Joo, E.Y.; Lee, H.J.; Lee, E.; Lee, S.K.; Jung, K.Y. Outdoor artificial light at night, obesity, and sleep health: Cross-sectional analysis in the KoGES study. Chronobiol. Int. 2016, 33, 301–314. [Google Scholar] [CrossRef] [PubMed]
- Mueller, N.; Rojas-Rueda, D.; Cole-Hunter, T.; de Nazelle, A.; Dons, E.; Gerike, R.; Nieuwenhuijsen, M.; Götschi, T.; Int Panis, L.; Kahlmeier, S. Health impact assessment of active transportation: A systematic review. Prev. Med. 2015, 76, 103–114. [Google Scholar] [CrossRef]
- Rojas-Rueda, D.; De Nazelle, A.; Andersen, Z.J.; Braun-Fahrländer, C.; Bruha, J.; Bruhova-Foltynova, H.; Desqueyroux, H.; Praznoczy, C.; Ragettli, M.S.; Tainio, M.; et al. Health impacts of active transportation in Europe. PLoS ONE 2016, 11. [Google Scholar] [CrossRef]
- Daniels, R.; Mulley, C. Explaining walking distance to public transport: The dominance of public transport supply. J. Transp. Land Use 2013, 6, 5–20. [Google Scholar] [CrossRef]
- Koohsari, M.J.; Mavoa, S.; Villanueva, K.; Sugiyama, T.; Badland, H.; Kaczynski, A.T.; Giles-Corti, B.; Owen, N. Public open space, physical activity, urban design and public health: Concepts, methods and research agenda. Health Place 2015, 33, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Giles-Corti, B.; Broomhall, M.H.; Knuiman, M.; Collins, C.; Douglas, K.; Ng, K.; Donovan, R.J.; Lange, A. Increasing walking: How important is distance to, attractiveness, and size of public open space? Am. J. Prev. Med. 2005, 28, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S. Built environment as a place for daily living and an opportunity for participation for community health promotion. Health Soc. Sci. 2017, 44, 81–104. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Category | Measurement | |||
|---|---|---|---|---|---|
| Objective Qualities of Built Environment | Perceived Environment | ||||
| Absolute | Relative | Composite | |||
| Land use | Residential use | Number of households, Number of residents per a room, Residential area | Apartment area ratio, Detached house area ratio, Townhouse area ratio | ||
| Non-residential use | Industrial area, Industrial floor area, Commercial area, Commercial floor area, Office floor area | ||||
| Mixed land use | Index of mixed land use, Index of residential and non-residential, Index of Population-employees, Entropy index of residential and non-residential, Entropy index of three non-residential use | Accessibility, Convenience | |||
| Street environment | Pedestrian sidewalk and pedestrian zone | Pedestrian sidewalk length, width, and area | Pedestrian sidewalk ratio, Ratio of road area to sidewalk area | Safety | |
| Walking facility and barrier | Number of walking rest facilities, temporary walking barrier, and permanent walking barrier, Number of pedestrian sidewalk lighting facilities | Convenience, Pleasantness | |||
| Intersection | Number of intersections, Number of intersections to population, Number of intersections to employees | Density of intersections, 4-way intersection ratio | Accessibility, Safety | ||
| Crosswalk | Number of crosswalk subsidiaries, Number of traffic lights | Crosswalk density | Accessibility Safety | ||
| Street connectivity and hierarchy | Number of sidewalk cuts | Entropy index of street hierarchy | Accessibility | ||
| Building and block | Building height, Block size | Window ratio of first floors | Aesthetics, Pleasantness | ||
| Transportation infrastructure | Bicycle road | Length of bicycle roads | Bicycle road accessibility | Accessibility | |
| Bus stop and route | Number of bus stops, Number of bus routes, Bus stop distance | Bus stop density | Bus stop accessibility | Accessibility, Convenience | |
| Subway and railway | Number of subway stations, Railway station distance | Subway station density | Subway accessibility | Accessibility, Convenience | |
| Vehicle use | Number of car accidents, Passing vehicle speed | Safety | |||
| Parking | Number of parking lots, Number of illegally parked cars | ||||
| Road | Number of road lanes | Road density | Road connectivity | Safety | |
| Green and open spaces | Park | Number of parks, Number of park entrances, Total area of parks, Park shortest network distance, Park shortest straight distance | Park area ratio, Ratio of park area to city area, Park area per capita | Park accessibility | Accessibility, Aesthetics, Convenience, Pleasantness |
| Green spaces | Total area of green spaces | Green spaces area ratio, Green spaces per capita | Accessibility, Pleasantness | ||
| Open spaces | Open spaces area ratio | Safety | |||
| Neighborhood facilities | Food environment | Number of traditional markets, Number of large-scale marts, Number of groceries, Number of street vendors, Number of fast food restaurants, Number of snack bars, Number of convenient stores | Fast food restaurants per area, Convenient stores per area | Accessibility to large-scale marts, Accessibility to traditional market | Accessibility, Convenience |
| Healthcare facility | Number of medical facilities | Accessibility to medical facility | Accessibility, Convenience | ||
| Education facility | Number of schools | Schools per area | Accessibility, Convenience, Pleasantness | ||
| Community facility | Number of welfare centers, Number of sports facilities | Accessibility to elderly welfare center, Accessibility to sports facility, Index of mixed community facilities | Accessibility, Convenience | ||
| Retail shop | Number of stores | Store accessibility | Accessibility, Convenience | ||
| Surveillance | Number of CCTV | Safety | |||
| Authors (year) | Research Fields | Setting | Participants (Age) | Sample Size | Sampling a | Data b | BE Measurement | Statistical Analysis |
|---|---|---|---|---|---|---|---|---|
| Kang and Kim (2011) [24] | Sport sciences | C | Older adults (65+) | 290 | Non-probability | 1 | O, P | MR |
| Kim and Ahn (2011) [25] | Civil and environmental engineering | C | Older adults (60+) | 381 | Non-probability | 1 | O | SEM |
| Kim and Kang (2011a) [26] | Urban planning | C | Residents (All ages) | NR | Probability | 2 | O | SR |
| Kim and Kang (2011b) [27] | Urban planning | C | Residents (All ages) | 1982 | Probability | 2 | O | MA |
| Sung (2011) [28] | Transportation | C | Adults (19+) | 976 | Probability | 2 | O | MA |
| Kim et al. (2012) [29] | Sport sciences | C | Older adults (65+) | 418 | Probability | 1 | O, P | LR |
| Ko and Lee (2012) [30] | Social welfare | C | Older adults (65+) | 1413 | Probability | 2 | O | HLM |
| Lee and Joo (2012) [31] | Urban and regional planning | C | Residents (All ages) | NR | Other | 2 | O | SR |
| Lee and Shepley (2012) [32] | Landscape architecture | C | Residents (All ages) | 412 | Non-probability | 1 | P | PA |
| Choi and Kim (2013) [33] | Urban planning and engineering | M | Residents (All ages) | 1329 | Probability | 2 | O | HLM |
| Kim and Kim (2013) [34] | Social welfare | C | Residents (All ages) | 45,605 | Probability | 2 | P | MA |
| Park et al. (2013) [35] | Medicine/Public health | C | Adolescents (11–16) | 939 | Probability | 1 | O | MA |
| Park et al. (2013) [36] | Medicine | C, M | Residents (All ages) | 4,055 | Probability | 2 | O | MR |
| Lee and Choi (2014) [37] | Housing environmental design | C | Adolescents (17) | 446 | Non-probability | 1 | P | MR |
| Sung et al. (2014) [38] | Transportation/Urban planning and engineering | C | Residents (All ages) | 1823 | Probability | 1 | O | MA |
| Jung and Lee (2015) [39] | Urban planning | C, M | Older adults (65+) | 11,407 | Probability | 2 | P | SEM |
| Kim and Kim (2015) [40] | Urban planning | M | Adults (19+) | NR | Probability | 2 | O, P | CA |
| Lee et al. (2015) [41] | Landscape architecture | M | Residents (All ages) | 303 | Non-probability | 1 | P | LR |
| Yoo and Lee (2015) [42] | Urban planning and engineering | M | Residents (All ages) | 9,406 | Probability | 2 | P | SEM |
| Cho and Lee (2016) [43] | Urban planning and engineering | C | Adults (19–64) | 484 | Non-probability | 1 | P | SEM |
| Chun (2016) [44] | Urban and regional planning | C | Adults (19–64) | NR | Probability | 2 | O | SR |
| Jang et al. (2016) [45] | Landscape architecture | M | Residents (All ages) | 143 | Non-probability | 1 | P | MR |
| Kim et al. (2016) [46] | Sport science | C | Adults (20–59) | 1407 | Probability | 1 | P | CA |
| Kim et al. (2016) [47] | Public health/Environmental science | C, M | Adolescents (9–13) | 4404 | Non-probability | 1 | O | LR |
| Lee and Lee (2016) [48] | Urban planning | C | Adults (19+) | 5692 | Probability | 2 | O | MA |
| Lee et al. (2016) [49] | Landscape architecture | M | Residents (All ages) | 278 | Non-probability | 1 | P | PA |
| Lee et al. (2016) [50] | Public health/Food science and nutrition | C | Adolescents (12–13) | 1134 | Non-probability | 1 | O, P | HLM |
| Health Domain | Variables | Measurement | ||
|---|---|---|---|---|
| Objective | Subjective | |||
| Physical health | Health-related behaviors | Eating behaviors | [35] | |
| Moderate or vigorous physical activity | [36,40,48,50] | [24] | ||
| Sedentary behaviors | [50] | |||
| Walking a | [29,32,38,40,41,45,46] | [32] | ||
| Illness or Death | Allergic diseases | [47] | ||
| Mortality rate | [31] | |||
| Obesity | [26,27,35,40,44,48] | [28] | ||
| Perceived health status | [33,34,39,49] | |||
| Mental health | Depression | [25,28,30,37] | ||
| Self-efficacy | [37] | |||
| Stress | [28,40] | |||
| Social health | Social interaction | [25] | [42,43] | |
| Social participation | [43] | |||
| Social reciprocity | [42,43] | |||
| Social trust | [42,43] | |||
| Characteristics of Built Environment | Association with Health Promotion | Objective Qualities of Environment | Perceived Environment | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Absolute (number, area, width, length, distance) | Relative (ratio, density, percent) | Composite (combined index) | Accessibility | Aesthetics | Convenience | Pleasantness | Safety | ||
| Land use | Positive | [48] a,1 | [48] a,1 | [28] a,2, [38] a,1, [40] a,2 | [43] c,2, [46] a,1 | [46] a,1 | |||
| Negative | [47] a,1 | ||||||||
| Null | [33] a,2 | [26] a,1, [27] a,1, [28] b,2, [33] a,2 | |||||||
| Street environment | Positive | [25] c,1, [38] a,1 | [38] a,1, [40] a,1 | [38] a,1 | [34] a,2, [41] a,1, [43] c,2, [49] a,2 | [49] a,2 | [37] b,2, [43] c,2, [49] a,2 | [32] a,1, [34] a,2, [41] a,1, [49] a,2 | |
| Negative | |||||||||
| Null | |||||||||
| Transportation infrastructure | Positive | [25] c,1, [33] a,2, [38] a,1, [40] a,2, [48] a,1 | [26] a,1, [27] a,1, [40] a,2 | [25] c,1 | [24] a,2, [39] a,2, [43] c,2 | [40] a,2 | |||
| Negative | [44] a,1 | [31] a,1 | |||||||
| Null | [33] a,2 | ||||||||
| Green and open spaces | Positive | [40] b,2, [48] a,1, [50] a,1 | [26] a,1, [27] a,1, [31] a,1, [36] a,1, [40] a,1, [48] a,1 | [28] a,2 | [24] a,2, [41] a,1, [45] a,1 | [45] a,1 | [41] a,1, [42] c,2, [45] a,1 | [45] a,1 | |
| Negative | |||||||||
| Null | [30] b,2, [33] a,2, [44] a,1 | [33] a,2 | |||||||
| Neighborhood Facility | Positive | [25] b,2, [29] a,1, [40] a,1, [50] a,1 | [40] a,1, [48] a,1 | [25] b,2, c,1 | [24] a,2, [29] a,1, [39] a,2, [41] a,2, [43] c,2 | [41] a,1 | [37] b,2 | [37] b,2 | [42] c,2, [43] c,2, [50] a,1 |
| Negative | [26] a,1, [35] a,1 | ||||||||
| Null | [27] a,1 | ||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.H.; Yoo, S. How Does the Built Environment in Compact Metropolitan Cities Affect Health? A Systematic Review of Korean Studies. Int. J. Environ. Res. Public Health 2019, 16, 2921. https://doi.org/10.3390/ijerph16162921
Kim DH, Yoo S. How Does the Built Environment in Compact Metropolitan Cities Affect Health? A Systematic Review of Korean Studies. International Journal of Environmental Research and Public Health. 2019; 16(16):2921. https://doi.org/10.3390/ijerph16162921
Chicago/Turabian StyleKim, Dong Ha, and Seunghyun Yoo. 2019. "How Does the Built Environment in Compact Metropolitan Cities Affect Health? A Systematic Review of Korean Studies" International Journal of Environmental Research and Public Health 16, no. 16: 2921. https://doi.org/10.3390/ijerph16162921
APA StyleKim, D. H., & Yoo, S. (2019). How Does the Built Environment in Compact Metropolitan Cities Affect Health? A Systematic Review of Korean Studies. International Journal of Environmental Research and Public Health, 16(16), 2921. https://doi.org/10.3390/ijerph16162921