A Process-Centered Approach to the Description of Clinical Pathways—Forms and Determinants



Abstract
1. Introduction
- It is the patient, not the disease, who is being treated;
- The treatment process should include the patient and their closest relatives;
- Different clinical and extra-clinical pathways (management, support, logistics, and others) should comprise a cohesive system;
- Clinical pathways should be reflected in IT systems, used on an ongoing basis by physicians and other relevant personnel.
2. Related Works
2.1. Business Processes
- Structured (static, predictable, repetitive) processes—as described above, processes which can be described in detail, in advance, and optimized, due to the pre-defined conditions of all decisions taken at the time of implementation;
- Semi-structured processes, further divided into:
- Structured processes with ad hoc exceptions—processes for which detailed description is possible before the commencement of implementation, and determination of decisions, as a result of which, ad hoc individual tasks not provided for in the process description, can be realized.
- Unstructured processes with pre-defined fragments—processes, for which it is possible, to clearly define goals and the roles of participants, and to describe in detail, the fragments, with which implementation must comply, within the imposed standards.
- Unstructured (unpredictable) processes, where it is possible to define the aims of the process, but is impossible to define as a priority, the exact steps to be taken, in order to successfully execute the process.
- The first principle: comprehensiveness and continuity;
- The second principle: process execution should guarantee evolutionary flexibility;
- The third principle: processes are considered completed, only after having been documented.
2.2. Clinical Pathways as Processes
- Analysis of related works in order to determine the best clinical practice for each medical condition and incorporating it into the CPs;
- Definition of the care process in each CP;
- Creation of the multi-disciplinary teams and granting ownership of each pathway disciplines involved in the care process;
- Invitation of all medical professions to comment on each pathway before their implementation;
- Incorporation of CPs into the patients’ medical records;
- Implementation of the regular feedback loop to all health professionals involved in the CP.
- Patients and their closest relatives,
- Students of medicine and inexperienced doctors making first steps in a given speciality.
- Presenting the planned and performed CPs in a way that is tailored to the requirements of the performers;
- Possibility to present and enter data in the place where the clinical pathway is being executed, that is, at the patient’s bedside, in a clinic, ER, ambulance, or even in the patient’s home;
- An ergonomic approach to data entry, which is cognizant of the limitations faced at each specific phase of the process, with the use of robotic process automation and elements of artificial intelligence, such as voice recognition, image recognition, and recognition of handwriting.
2.3. Analysis of Existing Forms of Describing Clinical Pathways
2.4. Proposal of a Process-Based Approach to Describing Clinical Pathways
- Cumbersome (a size of even A0, i.e., 1 meter in width and height!);
- Cluttered (a large number of small objects and a plethora of interconnections);
- Too complex (includes a large amount of information, which is not pertinent to the specific patient).
- Standard procedures dividing processes into hierarchical levels: maps, process models, and action charts with information, with the adequate level of detail and adequate scope of subject matter [61];
- Standard goals and rules of dividing the entire process into sub-processes on specific levels, and a clear presentation of their interrelations [61];
- Notation of description of processes, independent of the country in question, the geographical area, and the IT tool used to model processes (e.g., Business Process Model and Notation—BPMN) [42].
3. Materials and Methods
- Patient diagnosis and the formulation of a treatment plan (patient diagnosis; preparation of an individual treatment plan (ITP);
- Patient treatment, including eventual modifications to the ITP (modification of the individual treatment plan; adding a step to the individual treatment plan; preparation of a medical treatment/procedure; reminder on the necessity of performing a step of the individual treatment plan; confirmation of the performance of a step of the individual treatment plan; analysis of the performed diagnostic–therapeutic process);
- Ex-post evaluation of the finished treatment (analysis of the course of a finished diagnostic–therapeutic process of an individual patient; comparative analysis of a finished diagnostic–therapeutic process and the clinical pathway; comparative analysis of multiple finished diagnostic–therapeutic processes and the clinical pathway; statistical analysis of finished diagnostic–therapeutic processes; statistical analysis of finished diagnostic–therapeutic processes).
- Clearer form of patient data, making it easier to make correct clinical decisions;
- Possibility of evaluating the treatment on an ongoing basis;
- Possibility of modifying planned ongoing actions on an ongoing basis;
- Possibility of analyzing use resources and the degree of their productivity;
- Limiting mistakes in treatment by monitoring;
- Possibility of easier comparative analysis with the use of anonymized data on the treatment of other patients;
- Better control over the operations of the organization.
4. Results
5. Discussion
6. Conclusions
- The possibility to analyze the treatment on an ongoing basis (27%);
- The possibility to dynamically modify planned and ongoing actions (23%).
6.1. Theoretical Contribution
6.2. Practical Implication
- The level of description;
- The character of the processes (the field that is being modeled), and the group of recipients; but also
- The phases of the process execution.
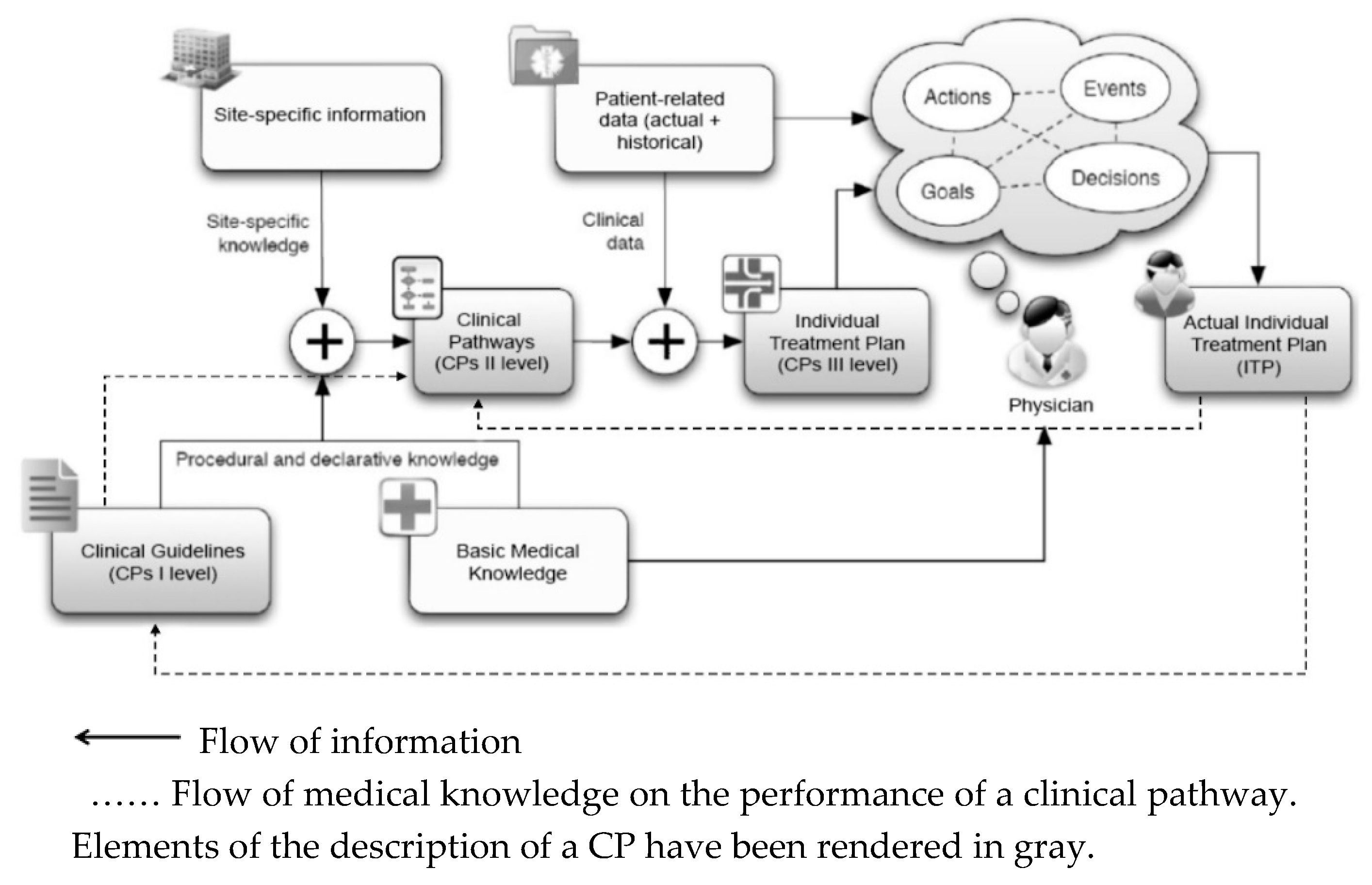
- Updating the medical knowledge contained in them based on the latest achievements of medicine, passing from Clinical Guidelines for Individual Treatment Plan (ITP) [12];
- Updating information on medical procedures that can be implemented within the health care unit, based on the common ontology underlying the CPs;
- Accumulation of knowledge on the basis of implemented or completed diagnostic and therapeutic processes thanks to the use of process mining techniques and the collection of data on clinical decisions taken and their impact on the course and results of therapy.
6.3. Limitations with Future Research Directions
- Analysis of preferences of users of CP presentation form conducted on a wide group of their users (doctors, nurses and other medical personnel);
- The identification of determinants for the description and presentation of CPs in different phases of their execution, on stationary and mobile devices;
- Development of a standard CPs integration format with ontologies describing resources and possible medical procedures, as well as knowledge bases or Evidence Based Medicine (EBM);
- The preparation of guidelines, with respect to the user interface for creators of HIS/EMR systems, as well as, more generally, creators of IT systems supporting dynamic BPM;
- Development and practical verification of the methodology and tools for gathering knowledge based on the implemented CPs and its use for ongoing support of the doctor’s work in the field of clinical decision-making.
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Puah, P.; Tang, N. Business process management, a consolidation of BPR and TQM. In Proceedings of the 2008 IEEE Conference on Cybernetics and Intelligent Systems, Chengdu, China, 21–24 September 2008; pp. 69–75. [Google Scholar]
- Khan, R.N. Business Process Management: A Practical Guide; Meghan-Kiffer Press: Tampa, FL, USA, 2004. [Google Scholar]
- Chang, J.F. Business Process Management Systems: Strategy and Implementation; Auerbach Publications, Taylor & Francis Group: New York, NY, USA, 2006. [Google Scholar]
- Jeston, J.; Nelis, J. Business Process Management. In Practical Guidelines to Successful Implementations; Butterworth-Heinemann: Oxford, UK, 2013. [Google Scholar]
- Dumas, M.; La Rosa, M.; Mendling, J.; Reijers, H. Fundamentals of Business Process Management; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- van Herck, P.; Vanhaecht, K.; Sermeus, W. Effects of Clinical Pathways: Do they work? Int. J. Care Pathw. 2004, 8, 95–105. [Google Scholar] [CrossRef]
- Hindle, D.; Dowdeswell, B.; Yasbeck, A. Report of a Survey of Clinical Pathways and Strategic Asset Planning in 17 EU Countries; EU Health Property Network: Utrecht, The Netherlands, 2004. [Google Scholar]
- Rotter, T.; Kinsman, L.; James, E.; Machotta, A.; Gothe, H.; Willis, J.; Snow, P.; Kugler, J. Clinical Pathways: Effects on Professional Practice, Patient Outcomes, Length of Stay and Hospital Costs. Cochrane Database Syst. Rev. 2010, CD006632. [Google Scholar] [CrossRef] [PubMed]
- Kirchmer, M.; Laengle, S.; Masias, V. Transparency-Driven Business Process Management in Healthcare Settings. IEEE Technol. Soc. Mag. 2013, 32, 14–16. [Google Scholar] [CrossRef]
- Hellman, S.; Kastberg, G.; Siverbo, S. Explaining process orientation failure and success in health care—Three case studies. J. Health Organ. Manag. 2015, 29, 638–653. [Google Scholar] [CrossRef] [PubMed]
- Szelągowski, M. Nowe metody zarządzania procesowego w ochronie zdrowia. e-Mentor 2015, 5, 40–48. [Google Scholar] [CrossRef][Green Version]
- Marrella, M.; Mecella, M.; Sharf, M.; Catarci, T. The TESTMED Project Experience Process-aware Enactment of Clinical Guidelines through Multimodal Interfaces. Available online: https://arxiv.org/pdf/1807.02022.pdf (accessed on 10 October 2018).
- Rummler, G.; Brache, A. Podnoszenie Efektywności Organizacji (Improving Performance); PWE: Warszawa, Poland, 2000. [Google Scholar]
- Knudson, G. What Is BPM? Available online: http://www.bpmleader.com/2013/07/29/what-is-bpm/ (accessed on 10 October 2018).
- Campbell, H.; Hotchkiss, R.; Bradshaw, N.; Porteous, M. Integrated care pathways. Br. Med. J. 1998, 316, 133–137. [Google Scholar] [CrossRef] [PubMed]
- González Sánchez, M.J.; Framiñán Torres, J.M.; Parra Calderón, C.L.; Del Río Ortega, J.A.; Vigil Martín, E.; Nieto Cervera, J. Application of business process management to drive the deployment of a speech recognition system in a healthcare organization. Stud. Health Technol. Inform. 2008, 136, 511–516. [Google Scholar] [PubMed]
- Andellini, M.; Fernandez Riesgo, S.; Morolli, F.; Ritrovato, M.; Cosoli, P.; Petruzzellis, S.; Rosso, N. Experimental application of Business Process Management technology to manage clinical pathways: A pediatric kidney transplantation follow up case. BMC Med. Inform. Decis. Mak. 2017, 17, 151. [Google Scholar] [CrossRef] [PubMed]
- Scheuerlein, H.; Rauchfuss, F.; Dittmar, Y.; Molle, R.; Lehmann, T.; Pienkos, N.; Settmacher, U. New methods for clinical pathways—Business Process Modeling Notation (BPMN) and Tangible Business Process Modeling (t.BPM). Langenbeck’s Arch. Surg. 2012, 397, 755–761. [Google Scholar] [CrossRef]
- Taylor, F.W. The Principles of Scientific Management; Harper & Brothers: New York, NY, USA, 1911. [Google Scholar]
- Zairi, M. Business process management: A boundaryless approach to modern competitiveness. Bus. Process Manag. J. 1997, 3, 64–80. [Google Scholar] [CrossRef]
- Palmberg, K. Exploring process management: Are there any widespread models and definitions? TQM J. 2009, 21, 203–215. [Google Scholar] [CrossRef]
- Röglinger, M.; Pöppelbuß, J.; Becker, J. Maturity Models in Business Process Management. Bus. Process Manag. J. 2012, 18, 328–346. [Google Scholar] [CrossRef]
- Kania, K. Doskonalenie Zarządzania Procesami Biznesowymi w Organizacji z Wykorzystaniem Modeli Dojrzałości i Technologii Informacyjno-Komunikacyjnych; Wydawnictwo Uniwersytetu Ekonomicznego w Katowicach: Katowice, Poland, 2013. [Google Scholar]
- Porter, M. Competitive Advantazge; Free Press: New York, NY, USA, 1985. [Google Scholar]
- Davenport, T.; Short, J. The new industrial engineering: Information technology and business process redesign. Sloan Manag. Rev. 1990, 31, 11–27. [Google Scholar]
- Richter-von Hagen, C.; Ratz, D.; Povalej, R. Towards Self-Organizing Knowledge Intensive Processes. J. Univers. Knowl. Manag. 2005, 2, 148–169. [Google Scholar]
- Di Ciccio, C.; Marrella, A.; Russo, A. Knowledge-intensive Processes: An Overview of Contemporary Approaches? In Proceedings of the First International Workshop on Knowledge-Intensive Business Processes (KiBP 2012), Rome, Italy, 15 June 2012. [Google Scholar]
- Swenson, K. Mastering the Unpredictable: How Adaptive Case Management Will Revolutionize the Way That Knowledge Workers Get Things Done; Meghan-Kiffer Press: Tampa, FL, USA, 2010. [Google Scholar]
- Szelągowski, M. Konsekwencje dynamic BPM. e-Mentor 2014, 4, 61–68. [Google Scholar] [CrossRef]
- Gartner IT Glossary. Dynamic Business Process Management. Available online: http://www.gartner.com/it-glossary/dynamic-business-process-management-bpm (accessed on 14 October 2018).
- Kemsley, S. The Changing Nature of Work: From Structured to Unstructured, from Controlled to Social. In Business Process Management (BPM); Rinderle-Ma, S., Toumani, F., Wolf, K., Eds.; Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2011; Volume 6896. [Google Scholar]
- Pucher, M. How to link BPM governance and social collaboration through an Adaptive Paradigm. In Social BPM: Work, Planning and Collaboration under the Impact of Social Technology; Swenson, K., Palmer, N., Eds.; Future Strategies Inc.: Lighthouse Point, FL, USA, 2012. [Google Scholar]
- Rothschadl, T. Ad-hoc adaptation of subject-oriented business processes at runtime to support organizational learning. In S-BPM ONE—Scientific Research: 4th International Conference, S-BPM ONE 2012; Stary, C., Ed.; Springer: Vienna, Austria, 2012. [Google Scholar]
- Kemsley, S. Runtime collaboration and dynamic modeling in BPM: Allowing the Business to shape its own processes on the fly. Cut. IT J. 2010, 23, 35–39. [Google Scholar]
- Szelągowski, M. Dynamic BPM in the Knowledge Economy: Creating Value from Intellectual Capital; Series: Lecture Notes in Networks and Systems (LNNS) nr. 71; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Czekaj, J. Metody Zarządzania Procesami w Świetle Studiów i Badań Empirycznych; Uniwersytet Ekonomiczny w Krakowie: Kraków, Poland, 2009; p. 45. [Google Scholar]
- Gronau, N.; Müller, C.; Korf, R. KMDL—Capturing, Analysing and Improving Knowledge-Intensive Business Processes. J. Univers. Comput. Sci. 2005, 4, 452–472. [Google Scholar]
- Di Ciccio, C.; Marrella, A.; Russo, A. Knowledge-intensive Processes Characteristics, Requirements and Analysis of Contemporary Approaches. J. Data Semant. 2015, 4, 29–57. [Google Scholar] [CrossRef]
- Vanhaecht, K.; Ovretveit, J.; Elliott, M.J.; Sermeus, W.; Ellershaw, J.; Panella, M. Have We Drawn the Wrong Conclusions About the Value of Care Pathways? Is a Cochrane Review Appropriate? Eval. Health Prof. 2012, 35, 28–42. [Google Scholar] [CrossRef]
- Davenport, T.; Nohria, N. Case Management and the Integration of Labor. MIT Sloan Management Review Magazine, 15 January 1994. [Google Scholar]
- Zander, K. Nursing case management: Strategic management of cost and quality outcomes. J. Nurs. Adm. 1988, 18, 23–30. [Google Scholar]
- OMG. Business Process Model and Notation (BPMN). Available online: http://www.omg.org/spec/BPMN/2.0.2 (accessed on 12 October 2018).
- Cheah, T.S. Clinical Pathways—The New Paradigm in Healthcare? Med. J. Malays. 1998, 53, 87–96. [Google Scholar]
- De Bleser, L.; Depreitere, R.; De Waele, K.; Vanhaecgt, K.; Vlayen, J.; Sermus, W. Defining pathways. J. Nurs. Manag. 2006, 14, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Kitchiner, D.; Bundred, P. Integrated care pathways. Arch. Dis. Child. 1996, 75, 166–168. Available online: https://adc.bmj.com/content/archdischild/75/2/166.full.pdf (accessed on 14 October 2018). [CrossRef] [PubMed][Green Version]
- Kononowicz, A.; Sałapa, K. Ścieżki kliniczne. In Elementy Informatyki Medycznej; Wydawnictwo Uniwersytetu Jagiellońskiego: Kraków, Poland, 2011; pp. 43–70. [Google Scholar]
- Williams, S.; Radnor, Z. An integrative approach to improving patient care pathways. Int. J. Health Care Qual. Assur. 2017, 31, 810–821. [Google Scholar] [CrossRef] [PubMed]
- European Pathway Association (EPA). Care Pathways. Available online: http://e-p-a.org/care-pathways/ (accessed on 17 October 2018).
- Vanhaecht, K. The Impact of Clinical Pathways on the Organisation of Care Processes. Ph.D. Dissertation, ACCO, Leuven, Belgium, 2007. [Google Scholar]
- Vanhaecht, K.; Panella, M.; van Zelm, R.; Sermeus, W. An overview on the history and concept of care pathways as complex interventions. Int. J. Care Pathw. 2010, 14, 117–123. [Google Scholar] [CrossRef]
- Wolff, A.; Taylor, S.; McCabe, J. Using checklists and reminders in clinical pathways to improve hospital inpatient care. Med. J. Aust. 2004, 181, 428–431. [Google Scholar] [PubMed]
- Panella, M.; Vanhaecht, K. Is there still need for confusion about pathways? Int. J. Care Pathw. 2010, 14, 1–3. [Google Scholar] [CrossRef]
- Joint Commission on Accreditation of Health Care Organizations. Root Causes for Sentinel Events. Available online: http://www.jointcommission.org/assets/1/18/Root_Causes_Event_Type_2004-3Q2011.pdf (accessed on 22 October 2018).
- Kononowicz, A. System Wspomagania Nauczania Medycyny Oparty na Koncepcji Ścieżek Klinicznych. Ph.D. Dissertation, Akademia Górniczo-Hutnicza w Krakowie, Wydział Elektrotechniki, Automatyki, Informatyki i Elektroniki, Kraków, Poland, 2011. [Google Scholar]
- Zander, K. Integrated care pathways: Eleven international trends. Int. J. Care Pathw. 2002, 6, 101–107. [Google Scholar] [CrossRef]
- Jung, J.; Choi, I.; Song, M. An integration architecture for knowledge management systems and business process management systems. Comput. Ind. 2007, 58, 21–34. [Google Scholar] [CrossRef]
- Schrijvers, G. Integrated care. In Better and Cheaper; Reed Business Information: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Cheah, T.S. The impact of clinical guidelines and clinical pathways on medical practice: Effectiveness and medico-legal aspects. Ann. Acad. Med. 1998, 27, 533–538. [Google Scholar]
- Yao, W.; Kumar, A. CONFlexFlow: Integrating flexible clinical pathways into clinical decision support systems using context and rules. Decis. Support Syst. 2012, 55, 499–515. [Google Scholar] [CrossRef]
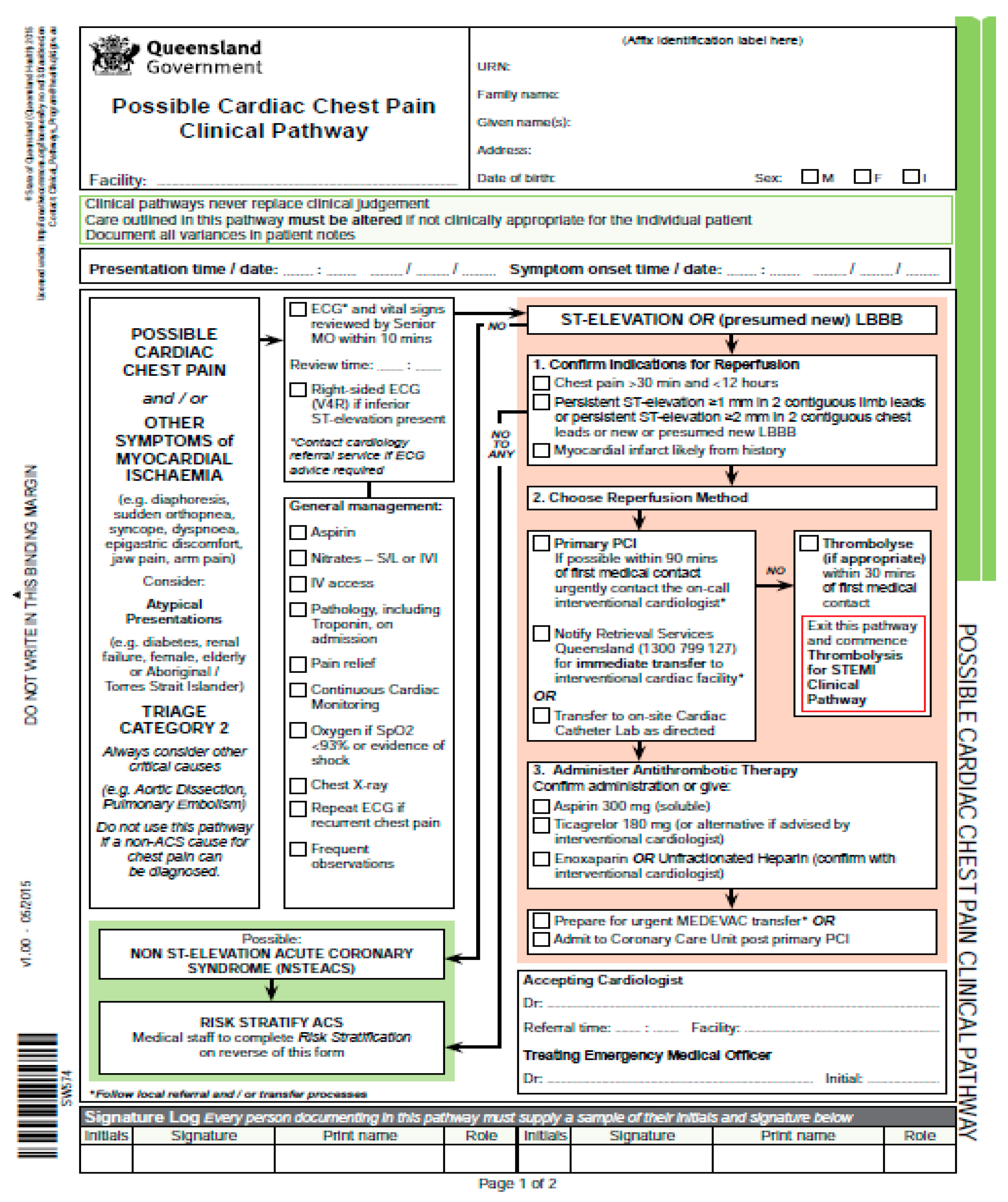
- State of Queensland. Possible Cardiac Chest Pain Clinical Pathway. Available online: https://www.health.qld.gov.au/__data/assets/pdf_file/0021/439131/sw574-chest-pain-pathway.pdf (accessed on 20 October 2018).
- Nuance. Voice-Enabled Virtual Assistants for Healthcare. Available online: https://www.nuance.com/healthcare/ambient-clinical-intelligence/virtual-assistants.html#video (accessed on 20 May 2019).
- Browning, T.R. On the alignment of the purposes and views of process models in project management. J. Oper. Manag. 2010, 28, 316–332. [Google Scholar] [CrossRef]
- Braun, R.; Schlieter, H.; Burwitz, M.; Esswein, W. BPMN4CP Revised—Extending BPMN for Multi-Perspective Modeling of Clinical Pathways. In Proceedings of the 49th Hawaii International Conference on System Sciences (HICSS 2016), Kauai, HI, USA, 5–8 January 2016; pp. 3249–3258. [Google Scholar]
- Cardoso, E.; Labunets, K.; Dalpiaz, F.; Mylopoulos, J.; Giorgini, P. Modeling Structured and Unstructured Processes: An Empirical Evaluation. In Improving the Correctness of Some Database Research Using ORA-Semantics; Wang Ling, T., Zeng, Z., Li Lee, M., Ngoc Le, T., Eds.; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Sobczak, A. Architektura korporacyjna. In Aspekty Teoretyczne i Wybrane Zastosowania Praktyczne; Ośrodek Studiów nad Państwem Cyfrowym: Łódź, Poland, 2013. [Google Scholar]
- Centre for Policy on Ageing. The Effectiveness of Care Pathways in Health and Social Care. Available online: http://www.cpa.org.uk/information/reviews/CPA-Rapid-Review-Effectiveness-of-care-pathways.pdf (accessed on 1 December 2018).
- PricewaterhouseCoopers. HealthCast 2020: Creating a Sustainable Future. Available online: https://www.pwc.com/il/he/publications/assets/2healthcast_2020.pdf (accessed on 20 October 2018).
- Isaac, S.; Michael, W.B. Handbook in Research and Evaluation; Educational and Industrial Testing Services: San Diego, CA, USA, 1995. [Google Scholar]
- Hill, R. What sample size is “enough” in internet survey research. Interpers. Comput. Technol. 1998, 6, 1–12. [Google Scholar]
- Dufresne, T.; Martin, J. Process Modeling for E-Business. INFS 770—Methods for Information Systems Engineering: Knowledge Management and E-Business. Available online: http://odesso.com/sites/default/files/ documents/processmodeling.doc (accessed on 22 October 2018).
- Waszkowski, R.; Kiedrowicz, M. Business rules automation standards in business process management systems. In Information Management in Practice; Kubiak, B., Maślankowski, J., Eds.; University of Gdańsk, Faculty Management: Sopot, Poland, 2015. [Google Scholar]
- Betz, S.; Eichhorn, D.; Hickl, S.; Klink, S.; Koschmider, A.; Li, Y.; Trunko, R. 3D Representation of Business Process Models. Available online: http://subs.emis.de/LNI/Proceedings/Proceedings141/gi-proc-141-005.pdf (accessed on 21 October 2018).
- Effinger, P. A 3D-Navigator for Business Process Models. In Business Process Management Workshops (BPM); La Rosa, M., Soffer, P., Eds.; Lecture Notes in Business Information Processing; Springer: Berlin/Heidelberg, Germany, 2012; Volume 132. [Google Scholar]
- Gawande, A. The Checklist Manifesto How to Get Things Right; Metropolitan Books: New York, NY, USA, 2009. [Google Scholar]
- Krogstie, J.; Sindre, G.; Jørgensen, H. Process models representing knowledge for action: A revised quality framework. Eur. J. Inf. Syst. 2006, 15, 91–102. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Administration and Supervision Priorities | Physicians’ Requirements (Expectations) |
|---|---|
| The standardization of diagnostic and therapeutic processes on the basis of acquired knowledge. | Adapting such processes to the situation at hand and obtaining new knowledge from each subsequent performance. |
| Planning and strict control over performance. | Empowering physicians to make independent clinical decisions. |
| Cost optimization of the performed processes. | Allowing for the accommodation of a given performance to the needs of the individual patient. |
| Form of Description and Presentation of CPs/Phase or Group of Performed Actions | Verbal Description | Structured Description | Block Diagram | Table | Checklist | Process Diagram | Gantt Diagram | 3D Process Map | Total No. Points |
|---|---|---|---|---|---|---|---|---|---|
| patient diagnosis | 2 | 7 | 4 | 6 | 18 | 6 | 0 | 1 | 44 |
| preparation of an individual treatment plan (ITP) | 3 | 6 | 5 | 4 | 19 | 2 | 0 | 3 | 42 |
| Total: The form of description of CPs in the initial diagnosis and treatment planning phase | 5 | 13 | 9 | 10 | 37 | 8 | 0 | 4 | 86 |
| 6% | 15% | 10% | 12% | 43% | 9% | 0% | 5% | ||
| modification of the individual treatment plan | 2 | 3 | 3 | 3 | 16 | 5 | 0 | 0 | 32 |
| adding a step to the individual treatment plan | 9 | 6 | 4 | 7 | 11 | 7 | 0 | 0 | 44 |
| preparation of a medical treatment/procedure | 0 | 6 | 12 | 3 | 12 | 11 | 0 | 0 | 44 |
| reminder on the necessity of performing a step of the individual treatment plan | 6 | 11 | 9 | 3 | 10 | 3 | 0 | 0 | 42 |
| confirmation of the performance of a step of the individual treatment plan | 6 | 11 | 5 | 3 | 9 | 8 | 0 | 0 | 42 |
| analysis of the performed diagnostic-therapeutic process | 0 | 10 | 3 | 7 | 3 | 3 | 10 | 2 | 38 |
| Total: The form of decription of CPs in the patient treatment phase | 23 | 47 | 36 | 26 | 61 | 37 | 10 | 2 | 242 |
| 10% | 19% | 14.9% | 11% | 25% | 15.3% | 4% | 1% | ||
| analysis of the course of a finished diagnostic-therapeutic process of an individual patient | 0 | 0 | 3 | 6 | 7 | 5 | 11 | 9 | 41 |
| comparative analysis of a finished diagnostic-therapeutic process and the clinical pathway | 0 | 2 | 0 | 6 | 5 | 5 | 12 | 8 | 38 |
| comparative analysis of multiple finished diagnostic-therapeutic processes and the clinical pathway | 0 | 2 | 2 | 8 | 2 | 10 | 11 | 3 | 38 |
| statistical analysis of finished diagnostic-therapeutic processes | 0 | 5 | 0 | 4 | 2 | 7 | 12 | 8 | 38 |
| statistical analysis of finished diagnostic-therapeutic processes | 0 | 5 | 0 | 1 | 5 | 7 | 12 | 5 | 35 |
| Total: The form of description of CPs in the ex-post evaluation phase | 0 | 14 | 5 | 25 | 21 | 34 | 58 | 33 | 190 |
| 0% | 7% | 3% | 13% | 11% | 18% | 31% | 17% | ||
| Total: The form of description of CPs expected by physicians | 28 | 74 | 50 | 61 | 119 | 79 | 68 | 39 | 518 |
| 5% | 14% | 10% | 12% | 23% | 15% | 13% | 8% |
| Determinants of the Selection of the Form of Description of CPs/Phase or Group of Performed Actions | Clearer Form of Patient Data, Making it Easier to Make Correct Clinical Decisions | Possibility of Evaluating the Treatment on an Ongoing Basis | Possibility of Modifying Planned and Ongoing Actions on an Ongoing Basis | Possibility of Analysing Used Resources and the Degree of Their Productivity | Limiting Mistakes in Treatment by Monitoring | Possibility of Easier Comparative Analysis with the Use of Anonymized Data on the Treatment of Other Patients | Better Control over the Operations of the Organization | Total No. Points |
|---|---|---|---|---|---|---|---|---|
| patient diagnosis | 9 | 9 | 4 | 0 | 1 | 0 | 2 | 25 |
| preparation of an individual treatment plan | 12 | 12 | 8 | 3 | 1 | 0 | 3 | 39 |
| Total: The form of description of CPs in the initial diagnosis and treatment planning phase | 21 | 21 | 12 | 3 | 2 | 0 | 5 | 64 |
| 33% | 33% | 19% | 5% | 3% | 0% | 8% | ||
| modification of the individual treatment plan | 10 | 11 | 14 | 0 | 4 | 0 | 3 | 42 |
| adding a step to the individual treatment plan | 10 | 9 | 12 | 0 | 2 | 1 | 2 | 36 |
| preparation of a medical treatment/procedure | 9 | 11 | 9 | 0 | 7 | 2 | 2 | 40 |
| reminder on the necessity of performing a step of the individual treatment plan | 7 | 11 | 10 | 0 | 9 | 0 | 1 | 38 |
| confirmation of the performance of a step of the individual treatment plan | 10 | 14 | 6 | 2 | 3 | 1 | 2 | 38 |
| analysis of the performed diagnostic-therapeutic process | 3 | 14 | 10 | 4 | 2 | 3 | 6 | 42 |
| Total: The form of decription of CPs in the patient treatment phase | 49 | 70 | 61 | 6 | 27 | 7 | 16 | 236 |
| 21% | 30% | 26% | 3% | 11% | 3% | 7% | ||
| analysis of the course of a finished diagnostic-therapeutic process of an individual patient | 0 | 9 | 9 | 6 | 5 | 3 | 7 | 39 |
| comparative analysis of a finished diagnostic-therapeutic process and the clinical pathway | 0 | 6 | 6 | 7 | 7 | 7 | 3 | 36 |
| comparative analysis of multiple finished diagnostic-therapeutic processes and the clinical pathway | 0 | 9 | 9 | 6 | 6 | 6 | 3 | 39 |
| statistical analysis of finished diagnostic-therapeutic processes | 0 | 9 | 7 | 4 | 7 | 5 | 4 | 36 |
| statistical analysis of finished diagnostic-therapeutic processes | 2 | 9 | 6 | 6 | 5 | 5 | 3 | 36 |
| Total: The form of description of CPs in the ex-post evaluation phase | 2 | 42 | 37 | 29 | 30 | 26 | 20 | 186 |
| 1% | 23% | 20% | 16% | 16% | 14% | 11% | ||
| Total: The form of description of CPs expected by physicians | 72 | 133 | 110 | 38 | 59 | 33 | 41 | 486 |
| 15% | 27% | 23% | 8% | 12% | 7% | 8% |
| Phase of the CP Lifecycle | Main Features of the Context of Executing the CP | The Preferred Form of Description of the CP | Determinants of the Choice of the Preferred Form of the CP Description and Presentation by Physicians | |
|---|---|---|---|---|
| I | Initial diagnosis and treatment planning | Usually the lack of direct time constraints. The possibility of consulting and modifying treatment plans multiple times. | 1. Checklist 2. Structured description 3. Table | 1. The possibility of analyzing the treatment on an ongoing basis. 2. Clearer form of patient data, making it easier to make correct clinical decisions. 3. The possibility of dynamically modifying planned and ongoing actions. |
| II | Patient treatment | Time constraints (or very strong time constraints). The necessity of tailoring the prepare treatment plan to the course of a specific treatment, including unpredictable developments. Responsibility (the undertaken actions are often irreversible). | 1. Checklist 2. Structured description 3. Process diagram | 1. The possibility of analyzing the treatment on an ongoing basis. 2. The possibility of dynamically modifying planned and ongoing actions. 3. Clearer form of patient data, making it easier to make correct clinical decisions. |
| III | Ex-post evaluation of finished treatments | No time constraints. The possibilit of consulting and modifying or supplementing the results of analyses multiple times. | 1. Gantt diagram 2. Process diagram 3. Table | 1. The possibility of analyzing the treatment on an ongoing basis. 2. The possibility of dynamically modifying planned and ongoing actions. 3. The possibility of analysing used resources and the degree of their productivity |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szelągowski, M.; Berniak-Woźny, J. A Process-Centered Approach to the Description of Clinical Pathways—Forms and Determinants. Int. J. Environ. Res. Public Health 2019, 16, 2638. https://doi.org/10.3390/ijerph16152638
Szelągowski M, Berniak-Woźny J. A Process-Centered Approach to the Description of Clinical Pathways—Forms and Determinants. International Journal of Environmental Research and Public Health. 2019; 16(15):2638. https://doi.org/10.3390/ijerph16152638
Chicago/Turabian StyleSzelągowski, Marek, and Justyna Berniak-Woźny. 2019. "A Process-Centered Approach to the Description of Clinical Pathways—Forms and Determinants" International Journal of Environmental Research and Public Health 16, no. 15: 2638. https://doi.org/10.3390/ijerph16152638
APA StyleSzelągowski, M., & Berniak-Woźny, J. (2019). A Process-Centered Approach to the Description of Clinical Pathways—Forms and Determinants. International Journal of Environmental Research and Public Health, 16(15), 2638. https://doi.org/10.3390/ijerph16152638