Workplace-Based Exercise Intervention Improves Work Ability in Office Workers: A Cluster Randomised Controlled Trial

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
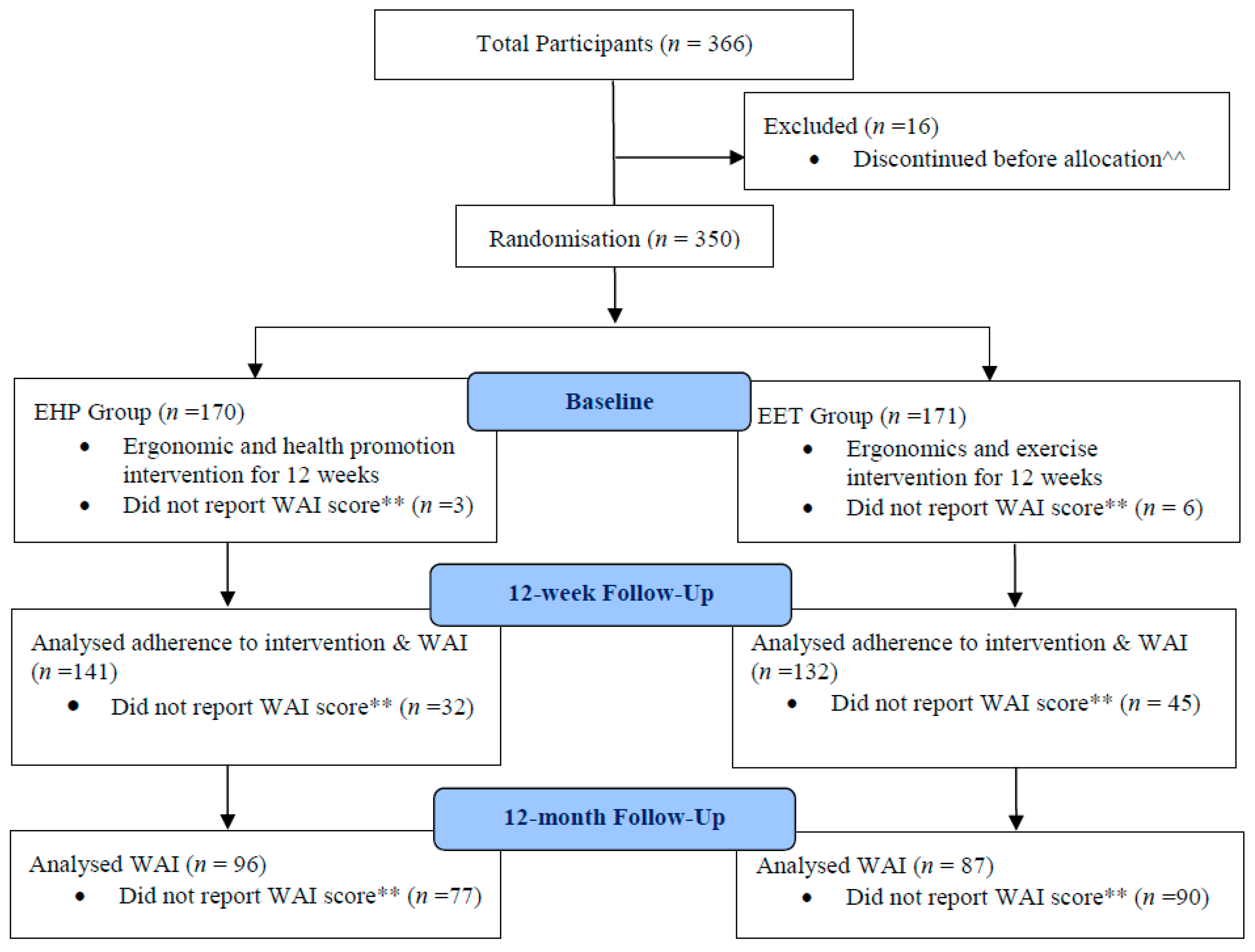
2.2. Procedure
2.3. Primary Outcome
2.4. Independent Variables
2.5. Data Analysis
3. Results
Adverse Events
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pereira, M.J.; Johnston, V.; Straker, L.M.; Sjøgaard, G.; Melloh, M.; O’Leary, S.P.; Comans, T.A. An investigation of self-reported health-related productivity losses in office workers and associations with individual and work-related factors using an employer’s perspective. JOEM 2017, 59, e138–e144. [Google Scholar] [PubMed]
- Cote, P.; van der Velde, G.; Cassidy, J.D.; Carroll, L.J.; Hogg-Johnson, S.; Holm, L.W.; Carragee, E.J.; Haldeman, S.; Nordin, M.; Hurwitz, E.L.; et al. The burden and determinants of neck pain in workers: Results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. J. Manipulative Physiol. Ther. 2009, 32, S70–S86. [Google Scholar] [CrossRef] [PubMed]
- Van Eerd, D.; Côté, P.; Kristman, V.; Rezai, M.; Hogg-Johnson, S.; Vidmar, M.; Dorcas, D. The Course of Work Absenteeism Involving Neck Pain A Cohort Study of Ontario Lost-Time Claimants. Spine 2011, 36, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Hagberg, M.; Tornqvist, E.W.; Toomingas, A. Self-reported reduced productivity due to musculoskeletal symptoms: Associations with workplace and individual factors among white-collar computer users. J. Occup. Rehabil. 2002, 12, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Aas, R.W.; Tuntland, H.; Holte, K.A.; Roe, C.; Lund, T.; Marklund, S.; Moller, A. Workplace interventions for neck pain in workers. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef] [PubMed]
- Leyshon, R.; Chalova, K.; Gerson, L.; Savtchenko, A.; Zakrzewski, R.; Howie, A.; Shaw, L. Ergonomic interventions for office workers with musculoskeletal disorders: A systematic review. Work 2010, 35, 335–348. [Google Scholar] [PubMed]
- Chen, X.; Coombes, B.K.; Sjogaard, G.; Jun, D.; O’Leary, S.; Johnston, V. Workplace-Based Interventions for Neck Pain in Office Workers: Systematic Review and Meta-Analysis. Phys. Ther. 2018, 98, 40–62. [Google Scholar] [CrossRef] [PubMed]
- Sihawong, R.; Janwantanakul, P.; Sitthipornvorakul, E.; Pensri, P. Exercise therapy for office workers with nonspecific neck pain: A systematic review. J. Manipulative Physiol. Ther. 2011, 34, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Van Eerd, D.; Munhall, C.; Irvin, E.; Rempel, D.; Brewer, S.; van der Beek, A.J.; Dennerlein, J.T.; Tullar, J.; Skivington, K.; Pinion, C.; et al. Effectiveness of workplace interventions in the prevention of upper extremity musculoskeletal disorders and symptoms: An update of the evidence. Occup. Environ. Med. 2016, 73, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Comans, T.; Sjogaard, G.; Straker, L.; Melloh, M.; O’Leary, S.; Chen, X.; Johnston, V. The impact of workplace ergonomics and neck-specific exercise versus ergonomics and health promotion interventions on office worker productivity: A cluster-randomized trial. Scand. J. Work Environ. Health 2019, 45, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J. Work ability—A comprehensive concept for occupational health research and prevention. Scand. J. Work Environ. Health 2009, 35, 1–5. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, T.I.; Elders, L.A.; de Zwart, B.C.; Burdorf, A. The effects of work-related and individual factors on the Work Ability Index: A systematic review. Occup. Environ. Med. 2009, 66, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Kuoppala, J.; Lamminpaa, A.; Husman, P. Work health promotion, job well-being, and sickness absences—A systematic review and meta-analysis. J. Occup. Environ. Med. 2008, 50, 1216–1227. [Google Scholar] [CrossRef] [PubMed]
- Schouten, L.S.; Joling, C.I.; van der Gulden, J.W.; Heymans, M.W.; Bultmann, U.; Roelen, C.A. Screening manual and office workers for risk of long-term sickness absence: Cut-off points for the Work Ability Index. Scand. J. Work Environ. Health 2015, 41, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Nurminen, E.; Malmivaara, A.; Ilmarinen, J.; Ylostalo, P.; Mutanen, P.; Ahonen, G.; Aro, T. Effectiveness of a worksite exercise program with respect to perceived work ability and sick leaves among women with physical work. Scand. J. Work Environ. Health 2002, 28, 85–93. [Google Scholar] [CrossRef]
- Barene, S.; Krustrup, P.; Holtermann, A. Effects of the Workplace Health Promotion Activities Soccer and Zumba on Muscle Pain, Work Ability and Perceived Physical Exertion among Female Hospital Employees. PLoS ONE 2014, 9, e115059. [Google Scholar] [CrossRef]
- Sundstrup, E.; Jakobsen, M.D.; Brandt, M.; Jay, K.; Persson, R.; Aagaard, P.; Andersen, L.L. Workplace strength training prevents deterioration of work ability among workers with chronic pain and work disability: A randomized controlled trial. Scand. J. Work Environ. Health 2014, 40, 244–251. [Google Scholar] [CrossRef]
- Jorgensen, M.B.; Faber, A.; Hansen, J.V.; Holtermann, A.; Sogaard, K. Effects on musculoskeletal pain, work ability and sickness absence in a 1-year randomised controlled trial among cleaners. BMC Public Health 2011, 11, 840–851. [Google Scholar] [CrossRef]
- Kettunen, O.; Vuorimaa, T.; Vasankari, T. 12-Mo Intervention of Physical Exercise Improved Work Ability, Especially in Subjects with Low Baseline Work Ability. Int. J. Environ. Res. Public Health 2014, 11, 3859–3869. [Google Scholar] [CrossRef]
- Martimo, K.P.; Shiri, R.; Miranda, H.; Ketola, R.; Varonen, H.; Viikari-Juntura, E. Effectiveness of an ergonomic intervention on the productivity of workers with upper-extremity disorders—A randomized controlled trial. Scand. J. Work. Environ. Health 2010, 36, 25–33. [Google Scholar] [CrossRef][Green Version]
- Justesen, J.B.; Sogaard, K.; Dalager, T.; Christensen, J.R.; Sjogaard, G. The Effect of Intelligent Physical Exercise Training on Sickness Presenteeism and Absenteeism among Office Workers. J. Occup. Environ. Med. 2017, 59, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Johnston, V.; O’Leary, S.; Comans, T.; Straker, L.; Melloh, M.; Khan, A.; Sjogaard, G. A workplace exercise versus health promotion intervention to prevent and reduce the economic and personal burden of non-specific neck pain in office personnel: Protocol of a cluster-randomised controlled trial. J. Physiother. 2014, 60, 233. [Google Scholar] [CrossRef]
- Campbell, M.K.; Elbourne, D.R.; Altman, D.G. CONSORT statement: Extension to cluster randomised trials. BMJ 2004, 328, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Comcare, C.O.A. Officewise: A Guide to Health and Safety in the Office; Commonwealth of Australia: Canberra, Australia, 2008; pp. 1–90. [Google Scholar]
- El Fassi, M.; Bocquet, V.; Majery, N.; Lair, M.L.; Couffignal, S.; Mairiaux, P. Work ability assessment in a worker population: Comparison and determinants of Work Ability Index and Work Ability score. BMC Public Health 2013, 13, 305. [Google Scholar] [CrossRef] [PubMed]
- IPAQ Research Committee. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)—Short and Long Forms. Available online: https://www.researchgate.net/file.PostFileLoader.html?id=5641f4c36143250eac8b45b7&assetKey=AS%3A294237418606593%401447163075131 (accessed on 23 July 2019).
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.L.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Wanous, J.P.; Hudy, M.J. Single-item reliability: A replication and extension. Organ. Res. Methods 2001, 4, 361–375. [Google Scholar] [CrossRef]
- Kaergaard, A.; Andersen, J.H.; Rasmussen, K.; Mikkelsen, S. Identification of neck-shoulder disorders in a 1 year follow-up study. Validation of a questionnaire-based method. Pain 2000, 86, 305–310. [Google Scholar] [CrossRef]
- Dalager, T.; Justesen, J.B.; Sjogaard, G. Intelligent Physical Exercise Training in a Workplace Setting Improves Muscle Strength and Musculoskeletal Pain: A Randomized Controlled Trial. Biomed Res. Int. 2017. [Google Scholar] [CrossRef]
- Larsson, A.; Karlqvist, L.; Gard, G. Effects of work ability and health promoting interventions for women with musculoskeletal symptoms: A 9-month prospective study. BMC Musculoskelet. Disord. 2008, 9, 105. [Google Scholar] [CrossRef]
- Sjogren-Ronka, T.; Ojanen, M.T.; Leskinen, E.K.; Tmustalampi, S.; Malkia, E.A. Physical and psychosocial prerequisites of functioning in relation to work ability and general subjective well-being among office workers. Scand. J. Work Environ. Health 2002, 28, 184–190. [Google Scholar] [CrossRef]
- Foley, B.; Engelen, L.; Gale, J.; Bauman, A.; Mackey, M. Sedentary Behavior and Musculoskeletal Discomfort Are Reduced When Office Workers Trial an Activity-Based Work Environment. J. Occup. Environ. Med. 2016, 58, 924–931. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Five Keys to Healthy Workplaces: No Business Wealth without Workers’ Health. Available online: http://www.who.int/occupational_health/5keys_healthy_workplaces.pdf?ua=1 (accessed on 5 July 2019).
- Bredahl, T.V.; Saervoll, C.A.; Kirkelund, L.; Sjogaard, G.; Andersen, L.L. When Intervention Meets Organisation, a Qualitative Study of Motivation and Barriers to Physical Exercise at the Workplace. Sci. World J. 2015, 518–561. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | All Participants (n = 350) | Neck Cases Sub-Sample (n = 97) | ||
|---|---|---|---|---|
| EHP Group (n = 173) | EET Group (n = 177) | EHP Group (n = 52) | EET Group (n = 45) | |
| Age (years), mean (SD) | 43.00 (9.48) | 41.68 (10.83) | 41.37 (8.41) | 41.46 (10.88) |
| Gender, n (%) | ||||
| Male | 70 (21) | 81 (24) | 18 (19) | 8 (8) |
| Female | 100 (29) | 90 (26) | 34 (35) | 37 (38) |
| Body Mass Index (kg/m2), mean (SD) | 26.46 (5.33) | 26.34 (5.79) | 25.99 (4.24) | 25.51 (5.55) |
| Occupational Category †, n (%) | ||||
| Category 1 | 36 (11) | 39 (11) | 9 (9) | 7 (7) |
| Category 2 | 87 (26) | 86 (25) | 31 (32) | 22 (23) |
| Category 3 | 47 (14) | 46 (13) | 12 (12) | 16 (16) |
| Industry, n (%) | ||||
| Private Sector | 61 (18) | 62 (18) | 19 (20) | 18 (19) |
| Government Sector | 109 (32) | 109 (32) | 33 (34) | 27 (28) |
| Highest Level of Education, n (%) | ||||
| Primary to Year 12 | 33 (10) | 28 (8) | 6 (6) | 6 (6) |
| University | 122 (36) | 119 (35) | 42 (43) | 31 (33) |
| Trade College | 15 (4) | 24 (7) | 4 (4) | 8 (8) |
| Computer Hours/Day, n (%) | ||||
| Less Than 6 Hours | 32 (9) | 36 (11) | 9 (9) | 8 (8) |
| More Than 6 Hours | 138 (40) | 135 (40) | 43 (44) | 37 (38) |
| Total comorbidities, mean (SD) (0–5) | 0.69 (0.92) | 0.54 (0.90) | 0.65 (0.88) | 0.69 (0.99) |
| Job Satisfaction, mean (SD) (1–7) | 4.92 (1.09) | 4.78 (1.21) | 4.83 (1.18) | 4.69 (1.20) |
| Psychological Distress, mean (SD) (0–15) | 3.56 (2.92) | 3.81 (3.17) | 4.06 (3.12) | 4.24 (3.36) |
| Total ergonomic score, mean (SD) (0–38) | 31.37 (3.39) | 32.23 (2.82) | 30.83 (3.37) | 32.02 (2.92) |
| Severity of Neck Pain in the last 7 days, mean (SD) (0–9) | 1.77 (2.26) | 1.50 (2.00) | 4.73 (1.65) | 4.44 (1.42) |
| IPAQ ∆, n (%) | ||||
| Category 1 | 63 (18) | 61 (18) | 18 (19) | 19 (20) |
| Category 2 | 90 (26) | 91 (27) | 30 (31) | 22 (23) |
| Category 3 | 17 (5) | 19 (6) | 4 (4) | 4 (4) |
| EHP vs. EET All Participants | |||||||
| Work Ability * | ITT | Per-Protocol | |||||
| b | 95% CI | p | b | 95% CI | p | ||
| Group | 0.02 | −0.25 to 0.29 | 0.89 | 0.05 | −0.41 to 0.51 | 0.83 | |
| Time | 12 weeks | −0.01 | −0.22 to 0.20 | 0.93 | −0.05 | −0.41 to 0.30 | 0.77 |
| 12 months | −0.08 | −0.32 to 0.17 | 0.54 | −0.09 | −0.49 to 0.31 | 0.66 | |
| Group × Time | 12 weeks | 0.24 | −0.06 to 0.55 | 0.12 | 0.24 | −0.26 to 0.73 | 0.35 |
| 12 months | 0.11 | −0.24 to 0.46 | 0.53 | 0.14 | −0.40 to 0.68 | 0.61 | |
| EHP vs. EET in Neck Cases | |||||||
| Work Ability* | ITT | Per-Protocol | |||||
| b | 95% CI | p | b | 95% CI | p | ||
| Group | −0.16 | −0.67 to 0.34 | 0.52 | −0.53 | −1.24 to 0.17 | 0.14 | |
| Time | 12 weeks | −0.03 | −0.43 to 0.37 | 0.88 | −0.37 | −1.02 to 0.28 | 0.27 |
| 12 months | −0.17 | −0.65 to 0.32 | 0.50 | −0.46 | −1.20 to 0.27 | 0.21 | |
| Group × Time | 12 weeks | 0.40 | −0.21 to 1.01 | 0.20 | 1.11 | 0.14 to 2.08 | 0.03 |
| 12 months | 0.54 | −0.17 to 1.25 | 0.14 | 1.02 | −0.05 to 2.08 | 0.06 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ting, J.Z.R.; Chen, X.; Johnston, V. Workplace-Based Exercise Intervention Improves Work Ability in Office Workers: A Cluster Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 2633. https://doi.org/10.3390/ijerph16152633
Ting JZR, Chen X, Johnston V. Workplace-Based Exercise Intervention Improves Work Ability in Office Workers: A Cluster Randomised Controlled Trial. International Journal of Environmental Research and Public Health. 2019; 16(15):2633. https://doi.org/10.3390/ijerph16152633
Chicago/Turabian StyleTing, Joshua Zheng Rui, Xiaoqi Chen, and Venerina Johnston. 2019. "Workplace-Based Exercise Intervention Improves Work Ability in Office Workers: A Cluster Randomised Controlled Trial" International Journal of Environmental Research and Public Health 16, no. 15: 2633. https://doi.org/10.3390/ijerph16152633
APA StyleTing, J. Z. R., Chen, X., & Johnston, V. (2019). Workplace-Based Exercise Intervention Improves Work Ability in Office Workers: A Cluster Randomised Controlled Trial. International Journal of Environmental Research and Public Health, 16(15), 2633. https://doi.org/10.3390/ijerph16152633