The Disparity in Mental Health Between Two Generations of Internal Migrants (IMs) in China: Evidence from A Nationwide Cross-Sectional Study


Abstract
1. Introduction
1.1. Migration and Health
1.2. The Intergenerational Disparity in Migrants’ Mental Health
2. Methods
2.1. Data Resource
2.2. Study Participants and Data Collection
2.3. Measurement
2.3.1. Outcome Measures
2.3.2. Independent Variable
2.3.3. Confounding Variables
Migration Characteristics
Social Integration
Demographics
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
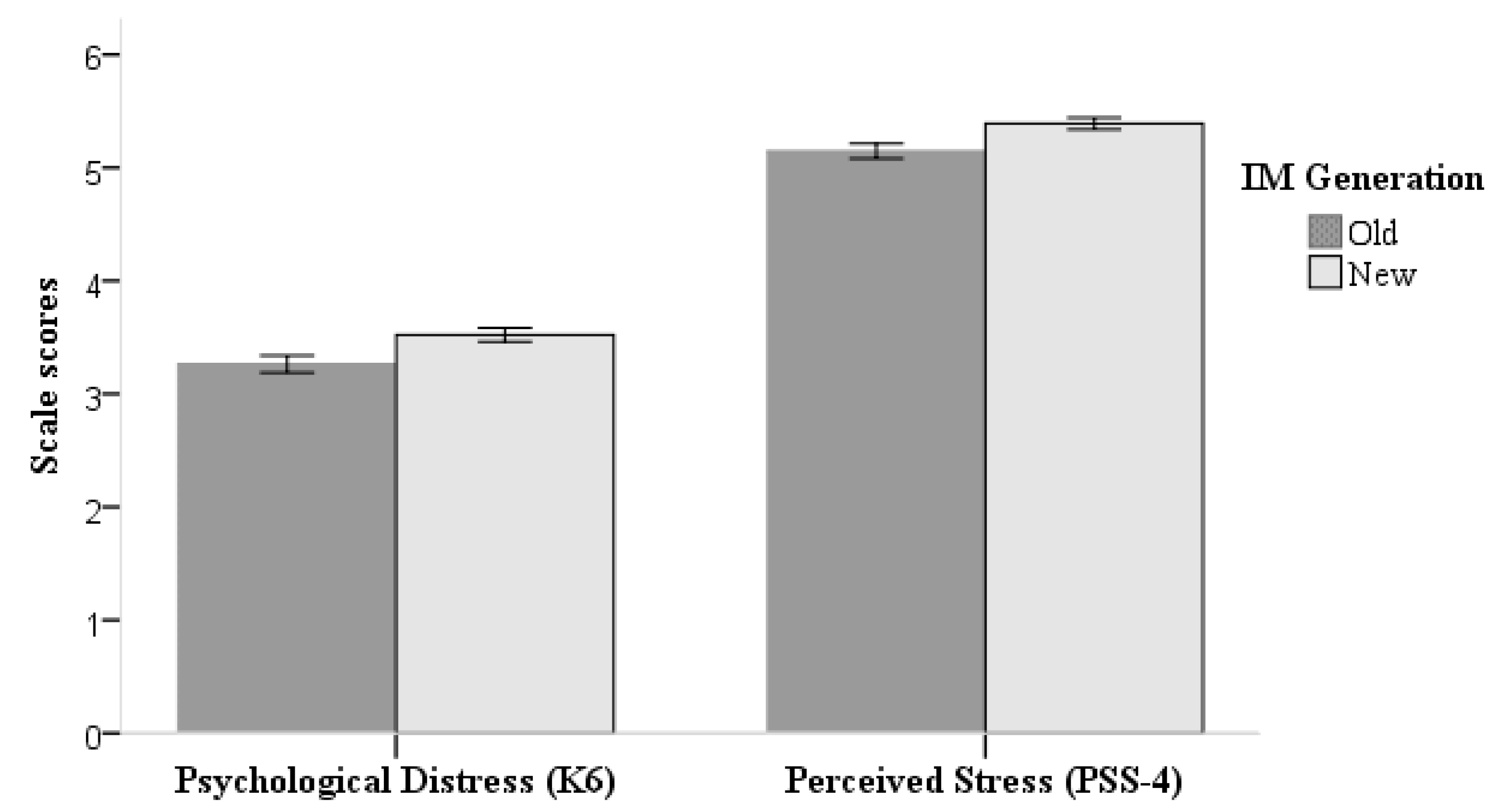
3.2. The Intergenerational Disparity in the Mental Health of IMs
3.3. Correlative Factors of Mental Health of the New- and Old-Generation Internal Migrants
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Disclaimers
Ethics
References
- Department of services and management of migrant population NHFPC of the PRC. Report On China’s Migrant Population Development 2015; China Population Publishing House: Beijing, China, 2015. [Google Scholar]
- United Nations Development Programme. Human Development Report 2009. Overcoming Barriers: Human Mobility and Development; Palgrave Macmillan: New York, NY, USA, 2009. [Google Scholar]
- Ling, L.; Cook, S.; Zhang, S.; Chen, W. Migration and Health in China; China Social Sciences Press: Beijing, China, 2015. [Google Scholar]
- Yue, Z.; Li, S.; Feldman, M.W. Social Integration of Rural-Urban Migrants in China: Current Status, Determinants and Consequences; World Scientific: Singapore, 2015. [Google Scholar]
- De Maio, F.G. Immigration as Pathogenic: A systematic review of the health of immigrants to Canada. Int. J. Equity Health 2010, 9, 27. [Google Scholar] [CrossRef] [PubMed]
- Flores, G.; Brotanek, J. The Healthy Immigrant Effect: A Greater Understanding Might Help Us Improve the Health of All Children. Arch. Pediatr. Adolesc. Med. 2005, 159, 295–297. [Google Scholar] [CrossRef] [PubMed]
- Renzaho, A.M. Globalisation, Migration and Health: Challenges and Opportunities; Imperial College Press: London, UK, 2016. [Google Scholar]
- Domnich, A.; Panatto, D.; Gasparini, R.; Amicizia, D. The “healthy immigrant” effect: Does it exist in Europe today? Ital. J. Public Health 2012, 9, 7531–7537. [Google Scholar]
- Giuntella, O.; Mazzonna, F. Do immigrants improve the health of natives? J. Health Econ. 2015, 43, 140–153. [Google Scholar] [CrossRef] [PubMed]
- Giuntella, O.; Mazzonna, F.; Nicodemo, C.; Vargas-Silva, C. Immigration and the reallocation of work health risks. J. Popul. Econ. 2019, 32, 1009–1042. [Google Scholar] [CrossRef]
- Pablos-Méndez, A. Mortality among Hispanics. JAMA 1994, 271, 1237. [Google Scholar] [CrossRef] [PubMed]
- Abraído-Lanza, A.F.; Dohrenwend, B.P.; Ng-Mak, D.S.; Turner, J.B. The Latino mortality paradox: A test of the “salmon bias” and healthy migrant hypotheses. Am. J. Public Health 1999, 89, 1543–1548. [Google Scholar] [CrossRef]
- Chen, J. Internal migration and health: Re-examining the healthy migrant phenomenon in China. Soc. Sci. Med. 2011, 72, 1294–1301. [Google Scholar] [CrossRef]
- Lin, Y.; Zhang, Q.; Chen, W.; Shi, J.; Han, S.; Song, X.; Xu, Y.; Ling, L. Association between Social Integration and Health among Internal Migrants in ZhongShan, China. PLoS ONE 2016, 11, e0148397. [Google Scholar] [CrossRef]
- Zhong, B.L.; Liu, T.B.; Chiu, H.F.; Chan, S.S.; Hu, C.Y.; Hu, X.F.; Xiang, Y.T.; Caine, E.D. Prevalence of psychological symptoms in contemporary Chinese rural-to-urban migrant workers: An exploratory meta-analysis of observational studies using the SCL-90-R. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 1569–1581. [Google Scholar] [CrossRef]
- Li, X.; Stanton, B.; Fang, X.; Xiong, Q.; Yu, S.; Lin, D.; Hong, Y.; Zhang, L.; Chen, X.; Wang, B. Mental Health Symptoms among Rural-to-Urban Migrants in China: A Comparison with Their Urban and Rural Counterparts. World Health Popul. 2009, 11, 15–29. [Google Scholar] [CrossRef]
- Li, L.; Wang, H.M.; Ye, X.J.; Jiang, M.M.; Lou, Q.Y.; Hesketh, T. The mental health status of Chinese rural-urban migrant workers: Comparison with permanent urban and rural dwellers. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chang, S.-S.; Yip, P.S.F.; Li, J.; Jordan, L.P.; Tang, Y.; Hao, Y.; Huang, X.; Yang, N.; Chen, C.; et al. Mental wellbeing amongst younger and older migrant workers in comparison to their urban counterparts in Guangzhou city, China: A cross-sectional study. BMC Public Health 2014, 14, 1280. [Google Scholar] [CrossRef] [PubMed]
- Lam, A.M.; Chan, T.S.; Tsoi, K.W. Meaning of family reunification as interpreted by young Chinese immigrants. Int. J. Adolesc. Med. Health 2005, 17, 105–122. [Google Scholar] [CrossRef] [PubMed]
- McGuire, J.; Li, X.; Wang, B. Social Stigma and Quality of Life among Rural-to-Urban Migrants in China: A Comparison with Their Rural Counterparts. World Health Popul. 2009, 11, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.W.; Cui, Z.T.; Cui, H.W.; Wei, C.N.; Harada, K.; Minamoto, K.; Ueda, K.; Ingle, K.N.; Zhang, C.G.; Ueda, A. Quality of life associated with perceived stigma and discrimination among the floating population in Shanghai, China: A qualitative study. Health Promot. Int. 2010, 25, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.F.K.; Li, C.Y.; Song, H.X. Rural migrant workers in urban China: Living a marginalised life. Int. J. Soc. Welf. 2007, 16, 32–40. [Google Scholar] [CrossRef]
- The United Nations. Migration. In Global Issues. 2019. Available online: https://www.un.org/en/sections/issues-depth/migration/index.html (accessed on 1 July 2019).
- Salas-Wright, C.P.; Kagotho, N.; Vaughn, M.G. Mood, anxiety, and personality disorders among first and second-generation immigrants to the United States. Psychiatry Res. 2014, 220, 1028–1036. [Google Scholar] [CrossRef]
- Nakash, O.; Levav, I.; Gal, G. Common mental disorders in immigrant and second-generation respondents: Results from the Israel-based World Mental Health Survey. Int. J. Soc. Psychiatry 2013, 59, 508–515. [Google Scholar] [CrossRef]
- Beutel, M.E.; Jünger, C.; Klein, E.M.; Wild, P.; Lackner, K.J.; Blettner, M.; Banerjee, M.; Michal, M.; Wiltink, J.; Brähler, E. Depression, anxiety and suicidal ideation among 1st and 2nd generation migrants—Results from the Gutenberg health study. BMC Psychiatry 2016, 16, 288. [Google Scholar] [CrossRef]
- Dorsett, R.; Rienzo, C.; Weale, M. Intergenerational and interethnic mental health: An analysis for the United Kingdom. Popul. Space Place 2018, 25, e2195. [Google Scholar] [CrossRef]
- Salant, T.; Lauderdale, D.S. Measuring culture: A critical review of acculturation and health in Asian immigrant populations. Soc. Sci. Med. 2003, 57, 71–90. [Google Scholar] [CrossRef]
- Sirin, S.R.; Ryce, P.; Gupta, T.; Rogers-Sirin, L. The role of acculturative stress on mental health symptoms for immigrant adolescents: A longitudinal investigation. Dev. Psychol. 2013, 49, 736–748. [Google Scholar] [CrossRef] [PubMed]
- The Number, Structure and Characteristics of New Generation Migrant Workers. Available online: http://www.stats.gov.cn/ztjc/ztfx/fxbg/201103/t20110310_16148.html (accessed on 20 September 2018).
- Feng, W.; Gu, B.; Cai, Y. The End of China’s One-Child Policy. Stud. Fam. Plan. 2016, 47, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Li, Z.; Breitung, W. The social networks of new-generation migrants in China’s urbanized villages: A case study of Guangzhou. Habitat Int. 2012, 36, 192–200. [Google Scholar] [CrossRef]
- Gorman, B.K.; Read, J.G.; Krueger, P.M. Gender, Acculturation, and Health among Mexican Americans. J. Health Soc. Behav. 2010, 51, 440–457. [Google Scholar] [CrossRef]
- Bulut, E.; Gayman, M.D. Acculturation and Self-Rated Mental Health Among Latino and Asian Immigrants in the United States: A Latent Class Analysis. J. Immigr. Minor. Health 2016, 18, 836–849. [Google Scholar] [CrossRef] [PubMed]
- Zhong, B.-L.; Liu, T.-B.; Chan, S.S.; Jin, D.; Hu, C.-Y.; Dai, J.; Chiu, H.F. Prevalence and correlates of major depressive disorder among rural-to-urban migrant workers in Shenzhen, China. J. Affect. Disord. 2015, 183, 1–9. [Google Scholar] [CrossRef]
- Kang, Y.-K.; Guo, W.-J.; Xu, H.; Chen, Y.-H.; Li, X.-J.; Tan, Z.-P.; Li, N.; Gesang, Z.-R.; Wang, Y.-M.; Liu, C.-B.; et al. The 6-item Kessler psychological distress scale to survey serious mental illness among Chinese undergraduates: Psychometric properties and prevalence estimate. Compr. Psychiatry 2015, 63, 105–112. [Google Scholar] [CrossRef]
- Warttig, S.L.; Forshaw, M.J.; South, J.; White, A.K. New, normative, English-sample data for the Short Form Perceived Stress Scale (PSS-4). J. Health Psychol. 2013, 18, 1617–1628. [Google Scholar] [CrossRef]
- United Nations Statistics Division. Handbook on Poverty Statistics: Concepts, Methods and Policy Use; Geneva United Nations: Geneva, Switzerland, 2005. [Google Scholar]
- Leung, D.Y.; Lam, T.H.; Chan, S.S. Three versions of Perceived Stress Scale: Validation in a sample of Chinese cardiac patients who smoke. BMC Public Health 2010, 10, 513. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Xu, X.; Li, M.; Rockett, I.R.; Zhu, W.; Ellison-Barnes, A. Mental health status and related characteristics of Chinese male rural-urban migrant workers. Commun. Ment. Health J. 2012, 48, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Zhou, X. Income inequality in today’s China. Proc. Natl. Acad. Sci. USA 2014, 111, 6928–6933. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction With Life Scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Wu, C.; Zheng, R.; Ren, X. The Psychometric Evaluation of the Satisfaction with Life Scale Using a Nationally Representative Sample of China. J. Happiness Stud. 2011, 12, 183–197. [Google Scholar] [CrossRef]
- Zhong, B.-L.; Chan, S.S.; Liu, T.-B.; Jin, D.; Hu, C.-Y.; Chiu, H.F. Mental health of the old-and new-generation migrant workers in China: Who are at greater risk for psychological distress. Oncotarget 2017, 8, 59791–59799. [Google Scholar] [CrossRef]
- Lu, G.; Zhou, X. Investigation on mental health status of migrant workers in cenozoic. Chin. Health Care Nutr. 2012, 22, 2452–2453. [Google Scholar]
- He, S.; Wang, K. China’s New Generation Migrant Workers’ Urban Experience and Well-being. In Mobility, Sociability and Well-being of Urban Living; Wang, D., He, S., Eds.; Springer: Berlin/Heidelberg, Gremany, 2016. [Google Scholar]
- Yang, X.; Xu, Y.; Gao, D.; Zhou, Z.; Jin, D.; Zou, X.; Liu, T. Mental wellbeing and resilience amongst migrant workers from service industries in Shenzhen city: A cross-sectional study. Chin. J. Psychiatry 2016, 49, 15–19. [Google Scholar]
- Statistical Information Center of National Health and Family Planning Commission. Report on Health Service Utilization Survey of Migrant Population; Peking Union Medical College Press: Beijing, China, 2016. [Google Scholar]
- Kirkcaldy, B.D.; Furnham, A.F.; Siefen, R.G. The effects of gender and migrant status on physical and psychological well-being. Int. J. Adolesc. Med. Health 2009, 21, 61–72. [Google Scholar] [CrossRef]
- Breslau, J.; Borges, G.; Tancredi, D.; Saito, N.; Kravitz, R.; Hinton, L.; Vega, W.; Medina-Mora, M.E.; Aguilar-Gaxiola, S. Migration from Mexico to the United States and subsequent risk for depressive and anxiety disorders: A cross-national study. Arch. Gen. Psychiatry 2011, 68, 428–433. [Google Scholar] [CrossRef]
- Baochang, G.; Feng, W.; Zhigang, G.; Erli, Z. China’s Local and National Fertility Policies at the End of the Twentieth Century. Popul. Dev. Rev. 2007, 33, 129–148. [Google Scholar] [CrossRef]
- Gui, T.; Koropeckyj-Cox, T. “I Am the Only Child of my Parents:” Perspectives on Future Elder Care for Parents among Chinese only-Children Living overseas. J. Cross Cult. Gerontol. 2016, 31, 255–275. [Google Scholar] [CrossRef] [PubMed]
- Lian, S. Ants Tribe: Settlement Villages for College Students; Guangxi Normal University Press: Guilin, China, 2009. (In Chinese) [Google Scholar]
- Kang, O. Higher Education Reform in China Today. Policy Futures Educ. 2004, 2, 141–149. [Google Scholar] [CrossRef]
- Chen, L.; Li, W.; He, J.; Wu, L.; Yan, Z.; Tang, W. Mental health, duration of unemployment, and coping strategy: A cross-sectional study of unemployed migrant workers in eastern china during the economic crisis. BMC Public Health 2012, 12, 597. [Google Scholar] [CrossRef] [PubMed]
- Vancea, M.; Utzet, M. How unemployment and precarious employment affect the health of young people: A scoping study on social determinants. Scand. J. Public Health 2016, 45, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Liu, S.; Zhang, G.; Wu, S. Internal migration and the health of the returned population: A nationally representative study of China. BMC Public Health 2015, 15, 372. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Generation a | Total a (n = 15,999) | |
|---|---|---|---|
| New (n = 9838) | Old (n = 6161) | ||
| Demographics | |||
| Age mean (SD) | 26.8 (4.5) | 41.8 (5.3) | 32.6 (8.7) *** |
| Weekly working hours mean (SD) | 53.1 (19.7) | 57.7 (21.2) | 54.8 (20.4) *** |
| Annual income/Regional GDP per capita 2013 mean (SD) | 0.65 (0.67) | 0.68 (0.87) | 0.66 (0.76) * |
| Sex n (%) | |||
| Male | 5258 (53.4) | 3541 (57.5) | 8799 (55.0) *** |
| Female | 4580 (46.6) | 2620 (42.5) | 7200 (45.0) |
| Marital status n (%) | |||
| Married | 5835 (59.3) | 5874 (95.3) | 11,709 (73.2) *** |
| Single | 4003 (40.7) | 287 (4.7) | 4290 (26.8) |
| Education level n (%) | |||
| Primary school and less | 307 (3.1) | 1198 (19.4) | 1505 (9.4) *** |
| Secondary school | 4687 (47.6) | 3398 (55.2) | 8085 (50.5) |
| High school | 2892 (29.4) | 1159 (18.8) | 4051 (25.3) |
| College and above | 1952 (19.8) | 406 (6.6) | 2358 (14.7) |
| Self-rated physical health n (%) | |||
| Good | 8992 (91.4) | 5210 (84.6) | 14,202 (88.8) *** |
| Fair | 827 (8.4) | 911 (14.8) | 1738 (10.9) |
| Poor | 19 (0.2) | 40 (0.6) | 59 (0.4) |
| Migration Characteristics | |||
| Duration of migration (months) mean (SD) | 37.0 (39.3) | 72.1 (63.8) | 50.5(53.0) *** |
| Migration path n (%) | |||
| Rural–Urban | 6267 (63.7) | 3745 (60.8) | 10,012 (62.6) *** |
| Urban–Urban | 1102 (11.2) | 725 (11.8) | 1827 (11.4) |
| Rural–Rural | 2340 (23.8) | 1575 (25.6) | 3915 (24.5) |
| Urban–Rural | 129 (1.3) | 116 (1.9) | 245 (1.5) |
| Migrating with families n (%) | |||
| No | 3534 (35.9) | 147 (2.4) | 3681 (23.0) *** |
| Yes | 6304 (64.1) | 6014 (97.6) | 12,318 (77.0) |
| Social Integration | |||
| Integration will (13–52) mean (SD) | 39.1 (4.4) | 39.4 (4.4) | 39.2 (4.4) *** |
| Views about social norms adopted (8–40) mean (SD) | 24.1 (4.1) | 23.4 (4.1) | 23.8 (4.1) *** |
| Income; occupation position compared with the people of the whole society (0–10) mean (SD) | 4.6 (1.7) | 4.7 (1.7) | 4.6 (1.7) ** |
| Degree of respect compared with relatives, friends and colleagues of the current residence (0–10) mean (SD) | 6.0 (1.6) | 6.0 (1.6) | 6.0 (1.6) |
| Willingness to live in current residence for the next 5 years n (%) | |||
| Yes | 5287 (53.7) | 4169 (67.7) | 9456 (59.1) *** |
| No | 1231 (12.5) | 571 (9.3) | 1802 (11.3) |
| Not sure | 3320 (33.7) | 1421 (23.1) | 4741 (29.6) |
| Type of neighbours n (%) | |||
| Outsiders | 4389 (44.6) | 2564 (41.6) | 6953 (43.5) *** |
| The locals | 1959 (19.9) | 1344 (21.8) | 3303 (20.6) |
| Mixed | 3489 (35.5) | 2252 (36.6) | 5741 (35.9) |
| Thinking oneself native or not n (%) | |||
| Yes | 2042 (20.8) | 1474 (23.9) | 3516 (22.0) *** |
| No | 7795 (79.2) | 4686 (76.1) | 12481 (78.0) |
| Personal Autonomy (0–10) mean (SD) | 6.7 (1.8) | 6.8 (1.8) | 6.7 (1.8) *** |
| Satisfaction with Life (5–35) mean (SD) | 21.4 (6.2) | 22.6 (6.3) | 21.9 (6.2) *** |
| Characteristics | Psychological Distress | Perceived Stress | ||
|---|---|---|---|---|
| β (95% CI) | βad (95% CI) # | β (95% CI) | βad (95% CI) # | |
| Generation | ||||
| Old (Ref.) | 0 | 0 | 0 | 0 |
| New | 0.197 (0.099, 0.295) *** | 0.084 (0.026, 0.193) * | 0.222 (0.139, 0.305) *** | 0.118 (0.029, 0.207) ** |
| Variance (estimates) | ||||
| Level-2 | 0.814 | 0.953 | ||
| Level-1 | 8.952 | 6.435 | ||
| ICC (%) | 8.34 | 12.90 | ||
| Characteristics | Psychological Distress βad (95% CI) # | Perceived Stress βad (95% CI) # | ||
|---|---|---|---|---|
| New Generation | Old Generation | New Generation | Old Generation | |
| County-level | ||||
| GDP per capita | −0.007 (−0.045, 0.030) | 0.022 (−0.020, 0.064) | −0.013 (−0.052, 0.025) | 0.025 (−0.011, 0.061) |
| Individual-level | ||||
| Demographics | ||||
| Age | 0.001 (−0.016, 0.019) | −0.017 (−0.031, −0.002) * | −0.011 (−0.025, 0.004) | −0.010 (−0.022, 0.002) |
| Weekly working hours | −0.004 (−0.008, 0.001) | 0.002 (−0.002, 0.006) | 0.001 (−0.003, 0.004) | −0.002 (−0.006, 0.002) |
| Annual income/Regional GDP per capita 2013 | 0.124 (0.029, 0.218) * | −0.037 (−0.124, 0.049) | 0.057 (−0.192, 0.305) | 0.023 (−0.164, 0.210) |
| Sex | ||||
| Female (Ref.) | 0 | 0 | 0 | 0 |
| Male | −0.015 (−0.133, 0.102) | −0.114 (−0262, 0.034) | −0.020 (−0.114, 0.075) | −0.180 (−0.303, −0.057)** |
| Marital status | ||||
| Single (Ref.) | 0 | 0 | 0 | 0 |
| Married | −0.001 (−0.312, 0.309) | 0.159 (−0.316, 0.634) | 0.057 (−0.192, 0.305) | −0.026 (−0.421, 0.369) |
| Education level | ||||
| College and above (Ref.) | 0 | 0 | 0 | 0 |
| Primary school and less | −0.122 (−0.049, 0.248) | −0.234 (−0.610, 0.141) | 0.265 (−0.033, 0.562) | −0.262 (−0.576, 0.052) |
| Secondary school | −0.275 (−0.456, −0.094) ** | −0.294 (−0.627, 0.038) | 0.049 (−0.096, 0.193) | −0.262 (−0.541, 0.016) |
| High school | −0.083 (−0.262, 0.096) | 0.043 (−0.294, 0.381) | 0.089 (−0.054, 0.233) | −0.266 (−0.548, 0.016) |
| Self-rated physical health | ||||
| Poor (Ref.) | 0 | 0 | 0 | 0 |
| Good | −1.944 (−3.359, −0.528) ** | −1.700 (−2.727, −0.673) ** | −1.811 (−2.946, −0.676) ** | −0.923 (−1.799, −0.067) * |
| Fair | −0.760 (−2.188, 0.668) | −1.049 (−2.087, −0.011) * | −0.984 (−2.129, 0.161) | −0.423 (−1.3289, 0.442) |
| Migration Characteristics | ||||
| Duration of migration (months) | −0.000 (−0.002, 0.002) | 0.000 (−0.001, 0.002) | 0.002 (0.000, 0.003) * | −0.000 (−0.001, 0.001) |
| Migration path | ||||
| Rural–Urban (Ref.) | 0 | 0 | 0 | 0 |
| Urban–Urban | 0.201 (0.009, 0.410) * | 0.097 (−0.160, 0.354) | 0.241 (0.073, 0.409) ** | 0.127 (−0.087, 0.341) |
| Urban–Rural | 0.162(−0.013, 0.337) | 0.209 (−0.006, 0.424) | 0.046 (−0.098, 0.189) | 0.162 (−0.018, 0.342) |
| Rural–Rural | 0.410 (−0.118, 0.939) | 0.054 (−0.485, 0.593) | 0.439 (0.014, 0.864) * | 0.098 (−0.352, 0.548) |
| Migrating with families | ||||
| Yes (Ref.) | 0 | 0 | 0 | 0 |
| No | 0.140 (−0.161, 0.440) | 0.394 (−0.252, 1.039) | 0.144 (−0.097, 0.384) | 0.447 (−0.091, 0.984) |
| Social Integration | ||||
| Integration will | −0.040 (−0.054, −0.026) *** | −0.029 (−0.046, −0.012) ** | −0.016 (−0.028, −0.005) ** | −0.027 (−0.041, −0.013) *** |
| Views about social norms adopted | −0.070 (−0.086, −0.055) *** | −0.069 (−0.088, −0.051) *** | −0.042 (−0.054, −0.030) *** | −0.042 (−0.058, −0.027) *** |
| Income, occupation position compared with the people of the whole society | −0.044 (−0.084, −0.004) * | 0.006 (−0.044, 0.056) | 0.003 (−0.029, 0.035) | 0.04 7(0.006, 0.089) * |
| Degree of respect compared with relatives, friends, and colleagues of the current residence | −0.018 (−0.060, 0.024) | −0.007 (−0.058, 0.044) | −0.066 (−0.100, −0.033) *** | −0.092 (−0.134, −0.049) *** |
| Willingness to live in current residence for the next five years | ||||
| No (Ref.) | 0 | 0 | 0 | 0 |
| Yes | 0.087 (−0.105, 0.278) | −0.142 (−0.396, 0.113) | −0.201 (−0.354, −0.048) * | −0.264 (−0.477, −0.052) * |
| Not sure | −0.119 (−0310, 0.072) | −0.014 (−0.289, 0.262) | −0.097 (−0.252, 0.056) | 0.010 (−0.219, 0.240) |
| Type of neighbours | ||||
| Outsiders (Ref.) | 0 | 0 | 0 | 0 |
| The locals | 0.009 (−0.165, 0.183) | 0.043 (−0.164, 0.249) | −0.062 (−0.202, 0.078) | 0.004 (−0.168, 0.177) |
| Mixed | −0.104 (−0.242, 0.034) | −0.075 (−0.242, 0.093) | 0.030 (−0.081, 0.141) | −0.029 (−0.168, 0.110) |
| Thinking oneself native or not | ||||
| No (Ref.) | 0 | 0 | 0 | 0 |
| Yes | 0.036 (−0.117, 0.188) | 0.139 (−0.040, 0.318) | −0.125 (−0.247, −0.002) * | −0.084 (−0.233, 0.065) |
| Personal autonomy | −0.403 (−0.441, −0.364) *** | −0.385 (−0.432, −0.339) *** | −0.405 (−0.436, −0.374) *** | −0.397 (−0.435, −0.358) *** |
| Satisfaction with life | −0.070 (−0.081, −0.060) *** | −0.078 (−0.091, −0.064) *** | −0.088 (−0.096, −0.079) *** | −0.096 (−0.107, −0.085) *** |
| Variance (estimates) | ||||
| Level-2 | 0.745 | 0.790 | 0.896 | 0.907 |
| Level-1 | 9.113 | 8.620 | 6.317 | 6.575 |
| ICC (%) | 7.56 | 8.40 | 12.42 | 12.12 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, W.; Zhang, Q.; Renzaho, A.M.N.; Ling, L. The Disparity in Mental Health Between Two Generations of Internal Migrants (IMs) in China: Evidence from A Nationwide Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 2608. https://doi.org/10.3390/ijerph16142608
Chen W, Zhang Q, Renzaho AMN, Ling L. The Disparity in Mental Health Between Two Generations of Internal Migrants (IMs) in China: Evidence from A Nationwide Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2019; 16(14):2608. https://doi.org/10.3390/ijerph16142608
Chicago/Turabian StyleChen, Wen, Qi Zhang, Andre M.N. Renzaho, and Li Ling. 2019. "The Disparity in Mental Health Between Two Generations of Internal Migrants (IMs) in China: Evidence from A Nationwide Cross-Sectional Study" International Journal of Environmental Research and Public Health 16, no. 14: 2608. https://doi.org/10.3390/ijerph16142608
APA StyleChen, W., Zhang, Q., Renzaho, A. M. N., & Ling, L. (2019). The Disparity in Mental Health Between Two Generations of Internal Migrants (IMs) in China: Evidence from A Nationwide Cross-Sectional Study. International Journal of Environmental Research and Public Health, 16(14), 2608. https://doi.org/10.3390/ijerph16142608