The Relationship between Vitamin C and Periodontal Diseases: A Systematic Review


Abstract
1. Introduction
1.1. Background
1.2. Objectives
2. Material and Methods
2.1. Literature Search
2.2. Quality Assessments
2.3. Data Extraction
3. Results
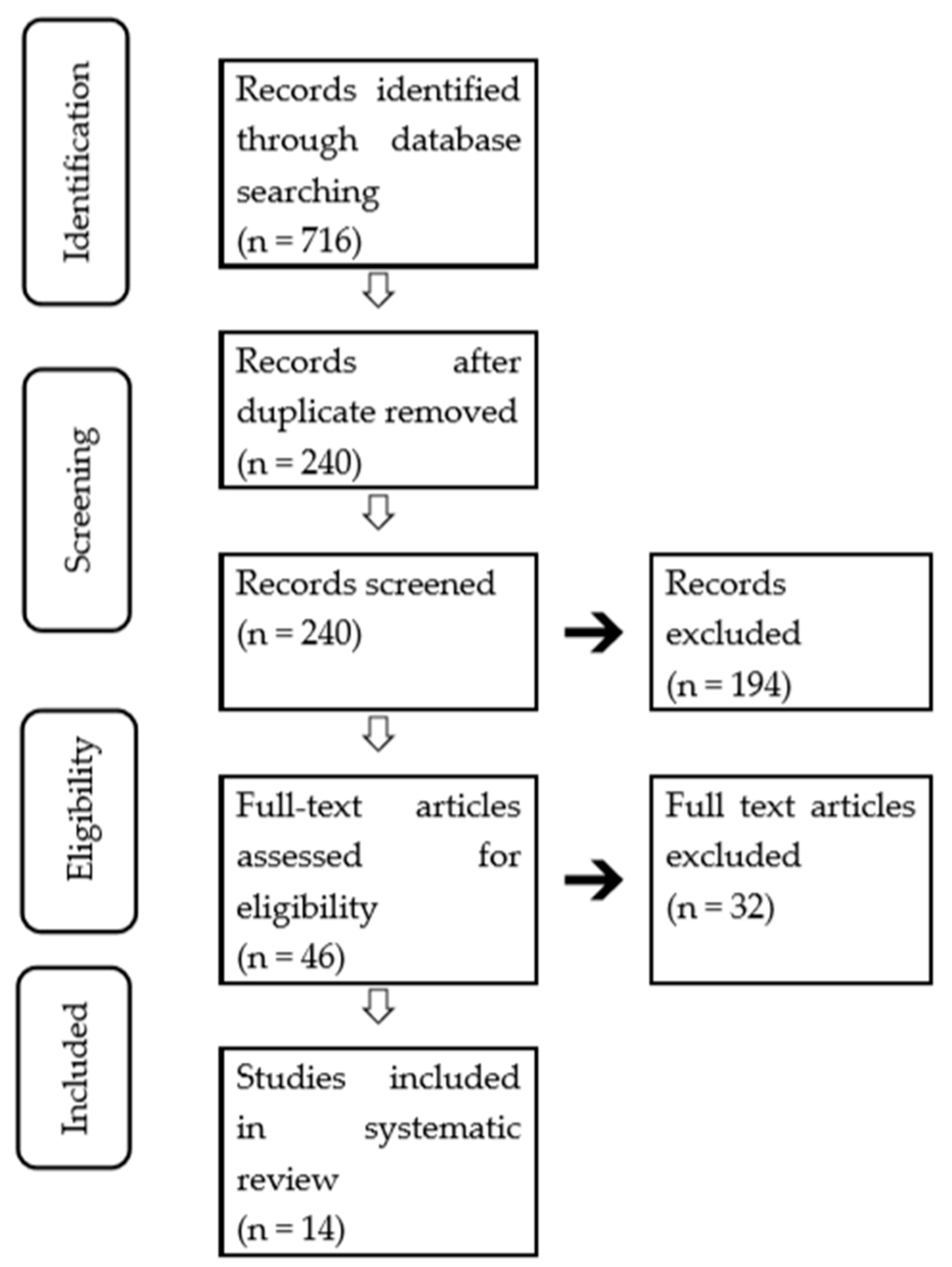
3.1. Literature Searches and Study Characteristics
3.2. Quality Evaluation
3.3. Relationship between Vitamin C Intake/Level to Periodontal Disease in Cross-Sectional Studies
3.4. Relationship between Vitamin C Intake/Level and Periodontal Disease in Case-Control Studies
3.5. Relationship between Vitamin C Intake/Level and Periodontal Disease in Cohort Studies
3.6. Improvement in Periodontal Status by Vitamin C in RCTs
4. Discussion
4.1. Quality Assessment of the Studies
4.2. Impact of Vitamin C on Periodontal Status
4.3. Influence of Other Factors on the Association between Vitamin C and Periodontal Disease
4.4. Limitations
4.5. Future Direction
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guinness World Records (Ed.) Gum disease. In Guinness World Records; Mint Publishers, Incorporated: New York, NY, USA, 2001; p. 175. [Google Scholar]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–2180. [Google Scholar] [CrossRef]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Bartold, P.M.; Van Dyke, T.E. Periodontitis: A host-mediated disruption of microbial homeostasis. Unlearning learned concepts. Periodontology 2013, 62, 203–217. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.R.; Lamster, I.B.; Chasens, A.I. Role of the polymorphonuclear leukocyte in periodontal health and disease. J. Clin. Periodontol. 1984, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, T.E.; Levine, M.J.; Genco, R.J. Neutrophil function and oral disease. J. Oral Pathol. 1985, 14, 95–120. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.T.; Green, E.R.; Mecsas, J. Neutrophils to the ROScue: Mechanisms of NADPH Oxidase Activation and Bacterial Resistance. Front. Cell Infect. Microbiol. 2017, 7, 373. [Google Scholar] [CrossRef]
- Galli, C.; Passeri, G.; Macaluso, G.M. FoxOs, Wnts and oxidative stress-induced bone loss: New players in the periodontitis arena? J. Periodontal Res. 2011, 46, 397–406. [Google Scholar] [CrossRef]
- Saita, M.; Kaneko, J.; Sato, T.; Takahashi, S.S.; Wada-Takahashi, S.; Kawamata, R.; Sakurai, T.; Lee, M.C.; Hamada, N.; Kimoto, K.; et al. Novel antioxidative nanotherapeutics in a rat periodontitis model: Reactive oxygen species scavenging by redox injectable gel suppresses alveolar bone resorption. Biomaterials 2016, 76, 292–301. [Google Scholar] [CrossRef]
- Wang, Y.; Andrukhov, O.; Rausch-Fan, X. Oxidative Stress and Antioxidant System in Periodontitis. Front. Physiol. 2017, 8, 910. [Google Scholar] [CrossRef]
- Sculley, D.V.; Langley-Evans, S.C. Periodontal disease is associated with lower antioxidant capacity in whole saliva and evidence of increased protein oxidation. Clin. Sci. 2003, 105, 167–172. [Google Scholar] [CrossRef]
- Panjamurthy, K.; Manoharan, S.; Ramachandran, C.R. Lipid peroxidation and antioxidant status in patients with periodontitis. Cell. Mol. Biol. Lett. 2005, 10, 255–264. [Google Scholar] [PubMed]
- Sugano, N.; Kawamoto, K.; Numazaki, H.; Murai, S.; Ito, K. Detection of mitochondrial DNA mutations in human gingival tissues. J. Oral Sci. 2000, 42, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Frei, B. Toward a new recommended dietary allowance for vitamin C based on antioxidant and health effects in humans. Am. J. Clin. Nutr. 1999, 69, 1086–1107. [Google Scholar] [CrossRef] [PubMed]
- Padayatty, S.J.; Katz, A.; Wang, Y.; Eck, P.; Kwon, O.; Lee, J.H.; Chen, S.; Corpe, C.; Dutta, A.; Dutta, S.K.; et al. Vitamin C as an antioxidant: Evaluation of its role in disease prevention. J. Am. Coll. Nutr. 2003, 22, 18–35. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.; Matthews, J.B. The role of reactive oxygen and antioxidant species in periodontal tissue destruction. Periodontol 2000 2007, 43, 160–232. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Zeng, W.; Song, S.; Zhang, F.; He, W.; Liang, W.; Niu, Z. Vitamin C induces periodontal ligament progenitor cell differentiation via activation of ERK pathway mediated by PELP1. Protein Cell 2013, 4, 620–627. [Google Scholar] [CrossRef][Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- CASP Qualitative Checklist. Oxford, UK: Critical Appraisal Skills Programme (CASP). Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf (accessed on 15 December 2017).
- Lewin, S.; Glenton, C.; Munthe-Kaas, H.; Carlsen, B.; Colvin, C.J.; Gülmezoglu, M.; Noyes, J.; Booth, A.; Garside, R.; Rashidian, A. Using qualitative evidence in decision making for health and social interventions: An approach to assess confidence in findings from qualitative evidence syntheses (GRADE-CERQual). PLoS Med. 2015, 12, e1001895. [Google Scholar] [CrossRef]
- Lee, J.H.; Shin, M.S.; Kim, E.J.; Ahn, Y.B.; Kim, H.D. The association of dietary vitamin C intake with periodontitis among Korean adults: Results from KNHANES IV. PLoS ONE 2017, 12, e0177074. [Google Scholar] [CrossRef]
- Luo, P.P.; Xu, H.S.; Chen, Y.W.; Wu, S.P. Periodontal disease severity is associated with micronutrient intake. Aust. Dent. J. 2018, 63, 193–201. [Google Scholar] [CrossRef]
- Park, J.A.; Lee, J.H.; Lee, H.J.; Jin, B.H.; Bae, K.H. Association of Some Vitamins and Minerals with Periodontitis in a Nationally Representative Sample of Korean Young Adults. Biol. Trace Elem. Res. 2017, 178, 171–179. [Google Scholar] [CrossRef]
- Nishida, M.; Grossi, S.G.; Dunford, R.G.; Ho, A.W.; Trevisan, M.; Genco, R.J. Dietary vitamin C and the risk for periodontal disease. J. Periodontol. 2000, 71, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.; Milward, M.R.; Dietrich, T. The prevalence of inflammatory periodontitis is negatively associated with serum antioxidant concentrations. J. Nutr. 2007, 137, 657–664. [Google Scholar] [CrossRef]
- Amarasena, N.; Ogawa, H.; Yoshihara, A.; Hanada, N.; Miyazakim, H. Serum vitamin C-periodontal relationship in community-dwelling elderly Japanese. J. Clin. Periodontol. 2005, 32, 93–97. [Google Scholar] [CrossRef]
- Amaliya Timmerman, M.F.; Abbas, F.; Loos, B.G.; Van der Weijden, G.A.; Van Winkelhoff, A.J.; Winkel, E.G.; Van der Velden, U. Java project on periodontal diseases: The relationship between vitamin C and the severity of periodontitis. J. Clin. Periodontol. 2007, 34, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Kuzmanova, D.; Jansen, I.D.; Schoenmaker, T.; Nazmi, K.; Teeuw, W.J.; Bizzarro, S.; Loos, B.G.; van der Velden, U. Vitamin C in plasma and leucocytes in relation to periodontitis. J. Clin. Periodontol. 2012. [Google Scholar] [CrossRef] [PubMed]
- Staudte, H.; Kranz, S.; Völpel, A.; Schütze, J.; Sigusch, B.W. Comparison of nutrient intake between patients with periodontitis and healthy subjects. Quintessence Int. 2012, 43, 907–916. [Google Scholar] [PubMed]
- Iwasaki, M.; Moynihan, P.; Manz, M.C.; Taylor, G.W.; Yoshihara, A.; Muramatsu, K.; Watanabe, R.; Miyazaki, H. Dietary antioxidants and periodontal disease in community-based older Japanese: A 2-year follow-up study. Public Health Nutr. 2013, 16, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Manz, M.C.; Taylor, G.W.; Yoshihara, A.; Miyazaki, H. Relations of serum ascorbic acid and α-tocopherol to periodontal disease. J. Dent. Res. 2012, 91, 167–172. [Google Scholar] [CrossRef]
- Shimabukuro, Y.; Nakayama, Y.; Ogata, Y.; Tamazawa, K.; Shimauchi, H.; Nishida, T.; Ito, K.; Chikazawa, T.; Kataoka, S.; Murakami, S. Effects of an ascorbic acid-derivative dentifrice in patients with gingivitis: A double-masked, randomized, controlled clinical trial. J. Periodontol. 2015, 86, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Gokhale, N.H.; Acharya, A.B.; Patil, V.S.; Trivedi, D.J.; Thakur, S.L. A short-term evaluation of the relationship between plasma ascorbic acid levels and periodontal disease in systemically healthy and type 2 diabetes mellitus subjects. J. Diet. Suppl. 2013, 10, 93–104. [Google Scholar] [CrossRef]
- Abou Sulaiman, A.E.; Shehadeh, R.M. Assessment of total antioxidant capacity and the use of vitamin C in the treatment of non-smokers with chronic periodontitis. J. Periodontol. 2010, 81, 1547–1554. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 1998; pp. 302–320. [Google Scholar]
- Schuch, H.S.; Peres, K.G.; Singh, A.; Peres, M.A.; Do, L.G. Socioeconomic position during life and periodontitis in adulthood: A systematic review. Community Dent. Oral Epidemiol. 2017, 45, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontol 2000 2013, 62, 59–94. [Google Scholar] [CrossRef] [PubMed]
- Gelskey, S.C. Cigarette smoking and periodontitis: Methodology to assess the strength of evidence in support of a causal association. Community Dent. Oral Epidemiol. 1999, 27, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Soskolne, W.A.; Klinger, A. The relationship between periodontal diseases and diabetes: An overview. Ann. Periodontol. 2001, 6, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Herrera, M.; Silvestre-Rangil, J.; Silvestre, F.J. Association between obesity and periodontal disease. A systematic review of epidemiological studies and controlled clinical trials. Med. Oral Patol. Oral Cir. Bucal. 2017, 22, e708–e715. [Google Scholar] [CrossRef]
- Poklepovic, T.; Worthington, H.V.; Johnson, T.M.; Sambunjak, D.; Imai, P.; Clarkson, J.E.; Tugwell, P. Interdental brushing for the prevention and control of periodontal diseases and dental caries in adults. Cochrane Database Syst. Rev. 2013, 12, CD009857. [Google Scholar] [CrossRef] [PubMed]
- Varela-López, A.; Navarro-Hortal, M.D.; Giampieri, F.; Bullón, P.; Battino, M.; Quiles, J.L. Nutraceuticals in Periodontal Health: A Systematic Review on the Role of Vitamins in Periodontal Health Maintenance. Molecules 2018, 23, 1226. [Google Scholar] [CrossRef]
- Muniz, F.W.; Nogueira, S.B.; Mendes, F.L.; Rösing, C.K.; Moreira, M.M.; de Andrade, G.M.; Carvalho Rde, S. The impact of antioxidant agents complimentary to periodontal therapy on oxidative stress and periodontal outcomes: A systematic review. Arch. Oral Biol. 2015, 60, 1203–1214. [Google Scholar] [CrossRef]
- Van der Putten, G.J.; Vanobbergen, J.; De Visschere, L.; Schols, J.; de Baat, C. Association of some specific nutrient deficiencies with periodontal disease in elderly people: A systematic literature review. Nutrition 2009, 25, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Padh, H. Vitamin C: Newer insights into its biochemical functions. Nutr. Rev. 1991, 49, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Staudte, H.; Güntsch, A.; Völpel, A.; Sigusch, B.W. Vitamin C attenuates the cytotoxic effects of Porphyromonas gingivalis on human gingival fibroblasts. Vitamin C attenuates the cytotoxic effects of Porphyromonas gingivalis on human gingival fibroblasts. Arch. Oral Biol. 2010, 55, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Yang, N.; Feng, X.; Sun, T.; Shen, P.; Sun, W. Effect of vitamin C administration on hydrogen peroxide-induced cytotoxicity in periodontal ligament cells. Mol. Med. Rep. 2015, 11, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Leggott, P.J.; Robertson, P.B.; Jacob, R.A.; Zambon, J.J.; Walsh, M.; Armitage, G.C. Effects of ascorbic acid depletion and supplementation on periodontal health and subgingival microflora in humans. J. Dent. Res. 1991, 70, 1531–1536. [Google Scholar] [CrossRef] [PubMed]
- Mathias, T.M.; Silva, J.F.; Sapata, V.M.; Marson, F.C.; Zanoni, J.N.; Silva, C.O. Evaluation of the effects of periodontal treatment on levels of ascorbic acid in smokers. J. Int. Acad. Periodontol. 2014, 16, 109–114. [Google Scholar] [PubMed]
- Cervino, G.; Terranova, A.; Briguglio, F.; De Stefano, R.; Famà, F.; D’Amico, C.; Amoroso, G.; Marino, S.; Gorassini, F.; Mastroieni, R.; et al. Diabetes: Oral Health Related Quality of Life and Oral Alterations. Biomed. Res. Int. 2019, 5907195. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, A.J.; Taylor, P.B.; Lunec, J.; Girling, A.J.; Barnettm, A.H. Low plasma ascorbate levels in patients with type 2 diabetes mellitus consuming adequate dietary vitamin C. Diabet. Med. 1994, 11, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Khatami, M. Na+-linked active transport of ascorbate into cultured bovine retinal pigment epithelial cells: Heterologous inhibition by glucose. Membr. Biochem. 1987, 7, 115–130. [Google Scholar] [CrossRef]
- Khatami, M.; Li, W.Y.; Rockey, J.H. Kinetics of ascorbate transport by cultured retinal capillary pericytes. Inhibition by glucose. Investig. Ophthalmol. Vis. Sci. 1986, 27, 1665–1671. [Google Scholar]
- Carr, A.C.; Maggini, S. Vitamin C and Immune Function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.A.; Hassan, K.H.; Hassanein, K.M.; Waly, H. Role of vitamin C and selenium in attenuation of nicotine induced oxidative stress, P53 and Bcl2 expression in adult rat spleen. Pathophysiology 2014, 21, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium and Carotenoids; National Academy Press: Washington, DC, USA, 2000. [Google Scholar]
- Fiorillo, L.; Cervino, G.; Herford, A.S.; Lauritano, F.; D’Amico, C.; Lo Giudice, R.; Laino, L.; Troiano, G.; Crimi, S.; Cicciù, M. Interferon Crevicular Fluid Profile and Correlation with Periodontal Disease and Wound Healing: A Systemic Review of Recent Data. Int. J. Mol. Sci. 2018, 19, 1908. [Google Scholar] [CrossRef] [PubMed]
- Dahl, H.; Degré, M. The effect of ascorbic acid on production of human interferon and the antiviral activity in vitro. Acta. Pathol. Microbiol. Scand. 1976, 84, 280–284. [Google Scholar] [CrossRef]
- Su, C.W.; Yen, A.F.; Lai, H.; Lee, Y.; Chen, H.H.; Chen, S.S. Effects of risk factors on periodontal disease defined by calibrated community periodontal index and loss of attachment scores. Oral Dis. 2017, 23, 949–955. [Google Scholar] [CrossRef] [PubMed]
- Staudte, H.; Sigusch, B.W.; Glockmann, E. Grapefruit consumption improves vitamin C status in periodontitis patients. Br. Dent. J. 2005, 199, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, L. Chlorhexidine Gel Use in the Oral District: A Systematic Review. Gels 2019, 5, 31. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | 1 | 2 | 3 | 4 | 5a | 5b | 6 | 7 | Quality Evaluation |
|---|---|---|---|---|---|---|---|---|---|
| Lee [21] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | Moderate |
| Luo [22] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | High |
| Park [23] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | Moderate |
| Nishida [24] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | Moderate |
| Chapple [25] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | Moderate |
| Amarasena [26] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | Moderate |
| Amaliya [27] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | Moderate |
| Reference | 1 | 2 | 3 | 4 | 5a | 5b | 6 | 7 | Quality Evaluation |
|---|---|---|---|---|---|---|---|---|---|
| Kuzmanova [28] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | High |
| Staudte [29] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | moderate |
| Reference | 1 | 2 | 3 | 4 | 5a | 5b | 6a | 6b | 7 | 8 | Quality Evaluation |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Iwasaki [30] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | Moderate |
| Iwasaki [31] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | Moderate |
| Reference | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Quality Evaluation |
|---|---|---|---|---|---|---|---|---|---|---|
| Shimabukuro [32] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | High |
| Gokhale [33] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | High |
| Abou [34] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | High |
| Key Finding | Studies Supporting Key Finding | Methodological limitations | Relevance | Coherence | Adequacy | Overall Assessment of Confidence | Explanation of Judgement |
|---|---|---|---|---|---|---|---|
| ① Adults with a lower dietary vitamin C intake have a higher incidence and severity, and more progressions of periodontal disease than those with a higher dietary vitamin C intake | [21,22,23,24,28,30] | Minor methodological concerns in 1/6 studies, with adjustment for confounding factors | No or very minor concerns about relevance | No or very minor concerns about coherence | Minor concerns about adequacy, as information lacked richness (1/6) | High | Finding graded as high because of only minor concerns about methodological quality and adequacy of contributing papers |
| ② Adults with lower blood vitamin C levels have a higher incidence and severity, and more progressions of periodontal disease than those with a higher dietary vitamin C level | [25,26,27,28,29,31] | Moderate methodological concerns in 3/6 studies, with adjustment for confounding factors, and in one study with sampling | No or very minor concerns about relevance | No or very minor concerns about coherence | Moderate concerns about adequacy, as information lacked richness (2/5) | Moderate | Finding downgraded because of concerns about methodological quality and adequacy of contributing papers |
| ③ Administration of vitamin C improving periodontal disease | [32,33,34] | No or very minor methodological concerns | Minor concerns about relevance on the specification of intervention (1/3) | Minor concerns about coherence, given that the effect is limited on gingivitis | Moderate concerns about adequacy of data, given the small number of studies | Moderate | Finding downgraded because of relevance, coherence, and adequacy concerns of contributing papers |
| Reference | Study Sample | Measurement of Vitamin C | Measurement of Periodontal Status | Control of Confounding Factors a | Key Results |
|---|---|---|---|---|---|
| Lee et al. [21] | 10,930 individuals (≥19 years; Korea) | A 24-h dietary record (adequate/inadequate vitamin C intake) | CPI score; periodontitis; CPI = 3 or 4 | 1, 2, 3, 4, and 5 | Lowest intake (<47.3 mg/day) vs highest intake (≥132.2 mg/day); adjusted odds ratio (aOR) = 1.28 (95% confidence interval (CI) = 1.10–1.50) |
| Park et al. [23] | 2049 individuals (19–39 years; Korea) | Complete one-day 24-h recall interviews | CPI score; periodontitis; CPI = 3 or 4 | 1, 2, 3, and 4 | Lower intake (<81.3 mg/day) vs higher intake (≥81.3 mg/day); aOR = 1.66 (95% CI = 1.04–2.64) for women; aOR = 1.49 (95% CI = 1.04–2.14) for nonsmokers |
| Luo et al. [22] | 6415 individuals (≥30 years; U.S.) | 24-h recall interviews | PD; AL; increased severity | 1, 2, 3, 4, and 5 | Vitamin C intake ≤20.65 mg/day vs ≥112.91/da7; aOR = 1.401 (95% CI = 1.12–1.74) |
| Nishida et al. [24] | 12,419 individuals (20 years and over; U.S.) | 24-h dietary record | Clinical attachment level; periodontal disease ≥1.5 | 1 and 3 | Vitamin C intake (<0–29 mg/day) vs (>180 mg/day); aOR = 1.30 |
| Chapple et al. [25] | 11,895 individuals (≥20 years; U.S.) | Serum vitamin C and anti-oxidant concentration | AL; PD; severe periodontitis: ≥2; mesiobuccal sites with AL ≥5 mm and ≥1; mesiobuccal sites with PD ≥4 mm | 1, 2, 3, and 5 | Serum vitamin C concentration: highest (>70.41 mmol/L) vs lowest (<8.52 mmol/L); aOR = 0.53 (95% CI = 0.42–0.68) |
| Amarasena et al. [26] | 413 individuals (70 years and older; Japan) | Serum vitamin C | AL | 1, 3, 4, and 5 | Serum vitamin C level-attachment loss: coefficient = −0.04 (95% CI = −0.06 to −0.005) |
| Amaliya et al. [27] | 123 individuals (33–43 years; Indonesia) | Plasma vitamin C | AL | 1, 2, 3, and 4 | Plasma vitamin C- attachment loss; coefficient = −0.199 |
| Reference | Study Sample | Measurement of Vitamin C | Measurement of Periodontal Status | Key Results |
|---|---|---|---|---|
| Kuzmanova et al. [28] | 21 patients with periodontitis and 21 controls (≥19 years, Dutch) | Vitamin C plasma level | Bone loss periodontitis >1/3 of the root length | Plasma vitamin C level: periodontitis patients < controls (p = 0.03) |
| Staudte et al. [29] | 42 patients with periodontitis (mean age 43.7 years) and 38 controls (mean age 40.5 years; Germany) | Seven-day food record; vitamin C plasma level | PD; chronic periodontitis: having ≥5 teeth with periodontal sites exhibiting PDs ≥3.5mm | Plasma vitamin C level: periodontitis patients < controls (p < 0.05); dietary intake of vitamin C: patients < controls (p < 0.05) |
| Reference | Study Sample | Measurement of Vitamin C | Measurement of Periodontal Status | Control of Confounding Factors a | Key Results |
|---|---|---|---|---|---|
| Iwasaki et al. [30] | 264 individuals (77 years; Japan) | Food frequency questions | Number of teeth having an AL of 3 mm or greater regression (8 years prospective) | 1, 2, 3, 4, and 5 | Lowest vitamin C intake (reference) vs. middle: 0.76 (0.60–0.97) vs. highest: 0.72 (0.56–0.93) |
| Iwasaki et al. [31] | 264 individuals (72 years; Japan) | Serum vitamin C | Number of teeth having AL of 3 mm or greater regression (2 years retrospective) | 1, 2, 3, 4, and 5 | Highest vitamin C level (reference) vs. middle: 1.12 (1.01–1.26) vs. lowest: 1.30 (1.16–1.47) |
| References | Study Sample | Intervention | Measurement of Periodontal Status | Key Results |
|---|---|---|---|---|
| Abou et al. [34] | 30 individuals with chronic periodontitis (Syria) | Non-surgical periodontal therapy and vitamin C administration | PD; CAL; BOP; GI | Vitamin C did not offer an additional effect to non-surgical periodontal therapy on the improvement in clinical measures |
| Shimabukuro et al. [32] | 300 individuals with gingivitis (Japan) | Dentifrice containing L-ascorbic acid 2-phosphate magnesium salt | GSI | GI test group: from 1.22 ± 0.03 to 0.73 ± 0.03; GI control: from 1.16 ± 0.03 to 0.84 ± 0.03; GSI test group: from 1.09 ± 0.04 to 0.69 ± 0.03; GSI control: from 1.13 ± 0.04 to 0.78 ± 0.03 |
| Gokhale et al. [33] | 120 individuals (30–60 years; India) | Non-surgical periodontal therapy (scaling and root planning: SRP) and vitamin C administration | SBI; PD | SBI—mean of differences (scores at baseline − scores after two weeks); SRP + vitamin C: 0.56 ± 0.26; SRP: 0.28 ± 0.12; PI and PD were not unaffected |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tada, A.; Miura, H. The Relationship between Vitamin C and Periodontal Diseases: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 2472. https://doi.org/10.3390/ijerph16142472
Tada A, Miura H. The Relationship between Vitamin C and Periodontal Diseases: A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(14):2472. https://doi.org/10.3390/ijerph16142472
Chicago/Turabian StyleTada, Akio, and Hiroko Miura. 2019. "The Relationship between Vitamin C and Periodontal Diseases: A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 14: 2472. https://doi.org/10.3390/ijerph16142472
APA StyleTada, A., & Miura, H. (2019). The Relationship between Vitamin C and Periodontal Diseases: A Systematic Review. International Journal of Environmental Research and Public Health, 16(14), 2472. https://doi.org/10.3390/ijerph16142472