Global Long-Term Care Research: A Scientometric Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Scientometric Analysis in CiteSpace
2.2. Data Collection
3. Results and discussion
3.1. Current Status of LTC Research
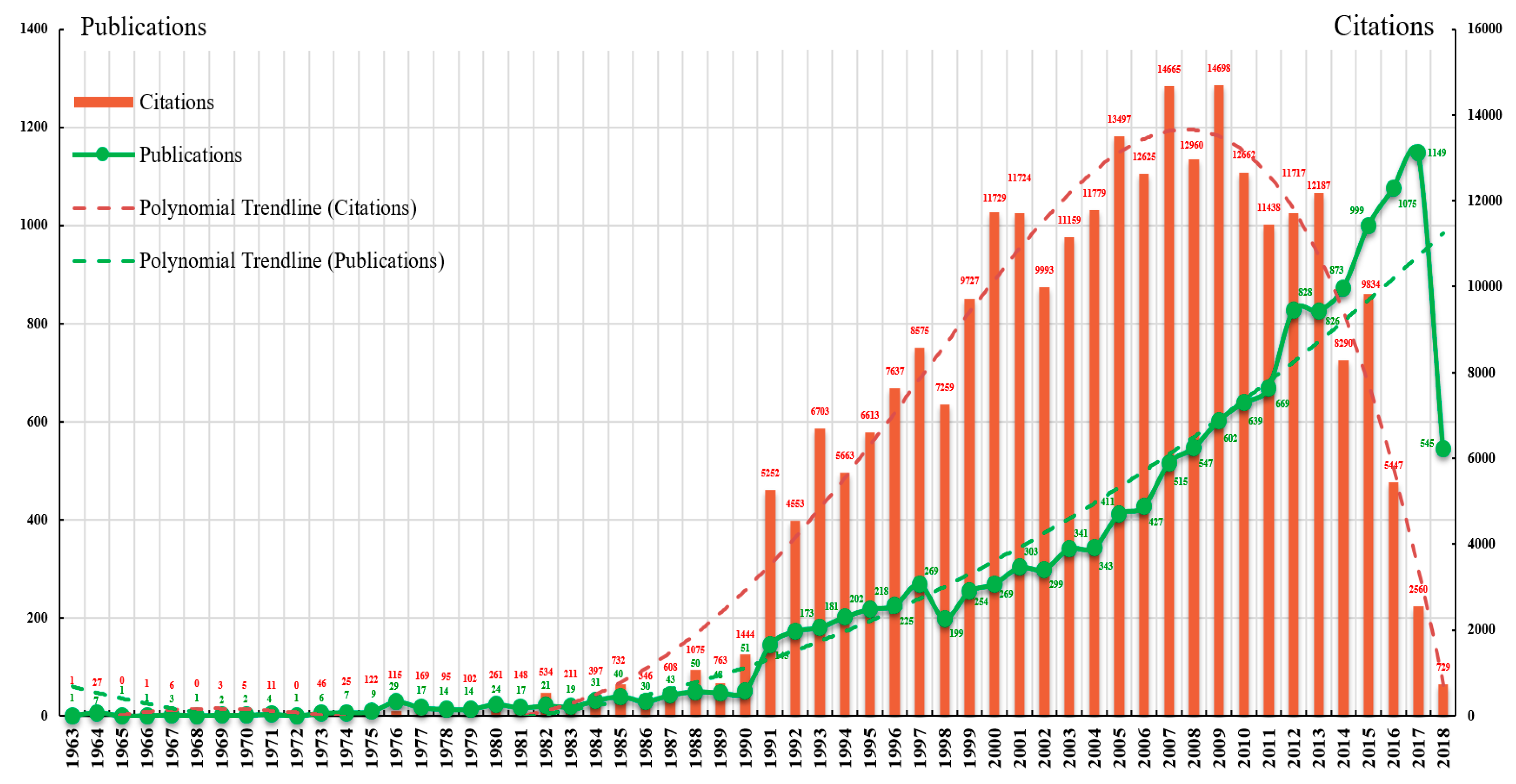
- Low-speed development stage (1963–1975). The annual number of publications increased slowly in this period and never exceeded 10. There was only one article in the years 1963, 1965, 1966, 1968, and 1972. Notably, 1975 was the most productive year with nine articles. In terms of annual citation counts, the dominant position was occupied by the year 1975 with 122 citations; there were fewer than 50 citations in all other years, probably because of a limited number of publications in those years.
- Rapid development stage (1976–1990). With a negligible amount of fluctuation, the number of publications per year increased steadily over this period. The most productive year was 1990 with 51 articles. Moreover, an increased number of citations per year were also observed over time. Articles published in 1988 and 1990 received many citations (each more than 1000), and the greatest average number of citations per article (28.31) also belonged to 1990.
- High-speed development stage (1991–2018). Publication output increased rapidly from 145 in 1991 to 1149 in 2017, resulting in a nearly eightfold increase in the past 27 years. In this period, the polynomial trendline of publication growth showed a significant correlation between publication year and publication counts. Through curve fitting, the number of publications was estimated to reach 1217 in 2018 (1222 articles were retrieved from this year) and 1302 in 2019, indicating that LTC research may remain active for many years. Moreover, three publication bursts were found in 1991, 2012, and 2015, increasing by 94, 159, and 126 over the previous year, respectively. Note that WoS provides abstracts and keywords for articles published after 1990. This may be the reason for the strong increase in publications from 1990 to 1991. The bar graph with an inverse U-shaped trendline showed that the number of citations peaked in 2009 with a record of 14,698 and then began to gradually decline, probably as a result of the time required for the accumulated effects of new publications.
3.2. Major Contributors to LTC Research
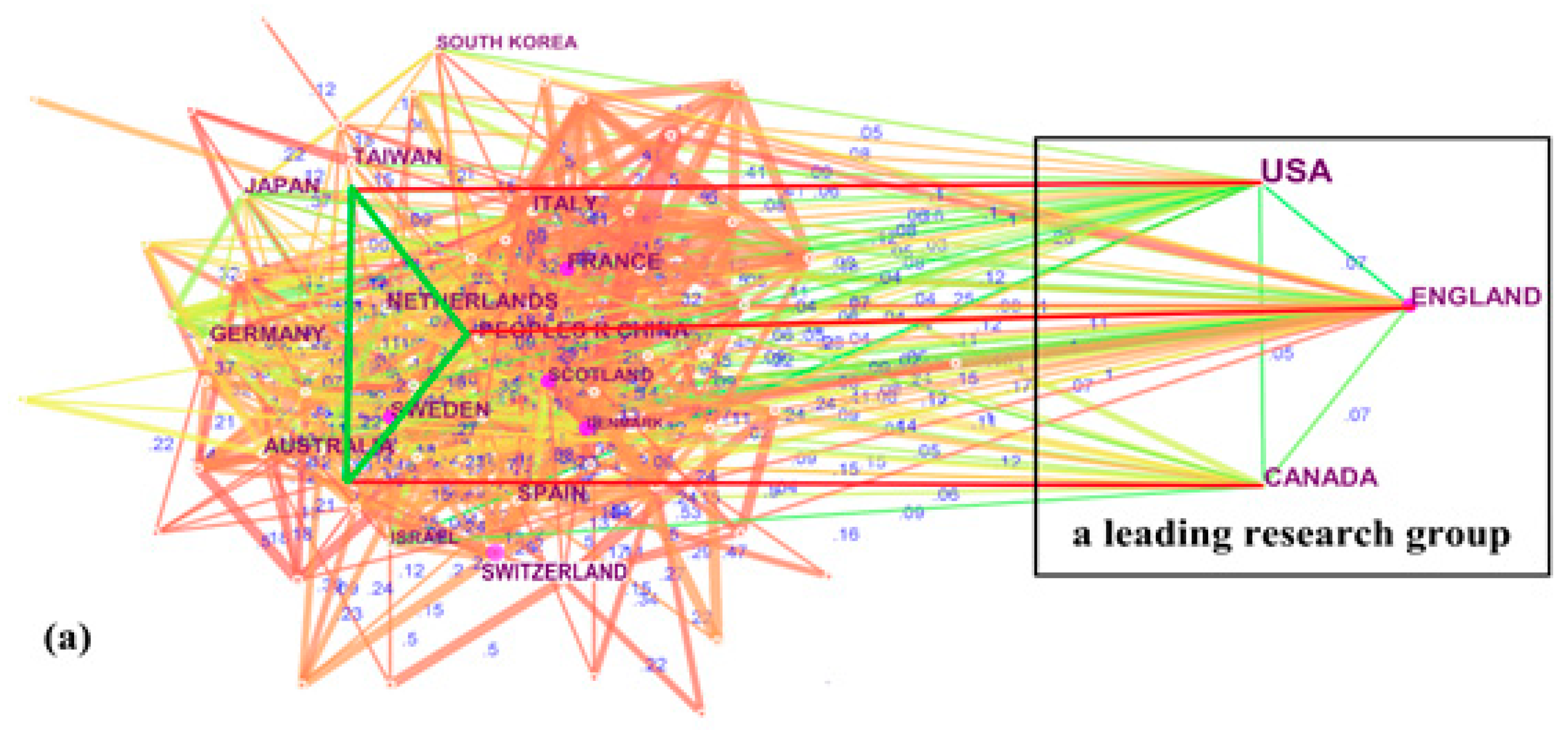
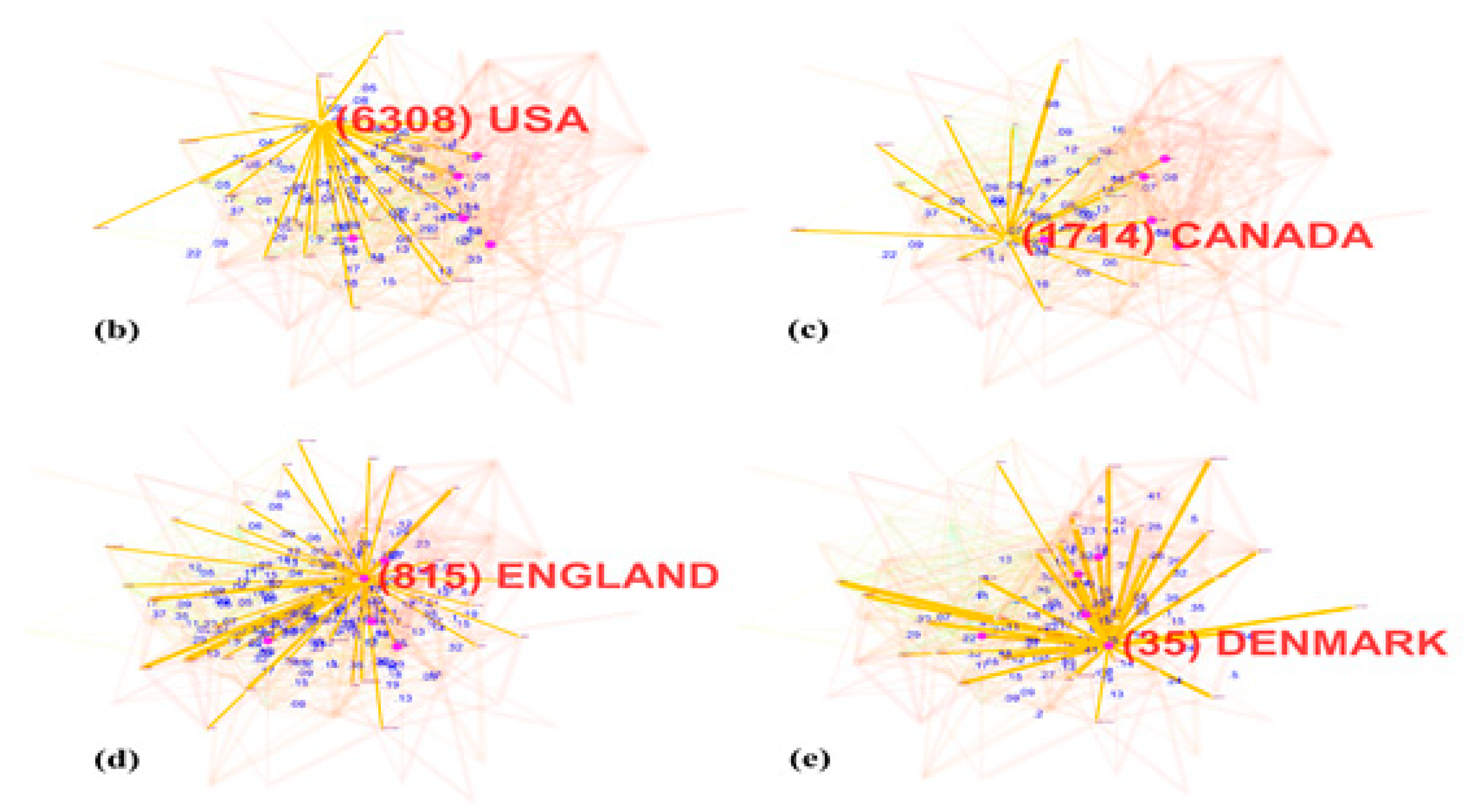
3.2.1. Country Collaboration Analysis
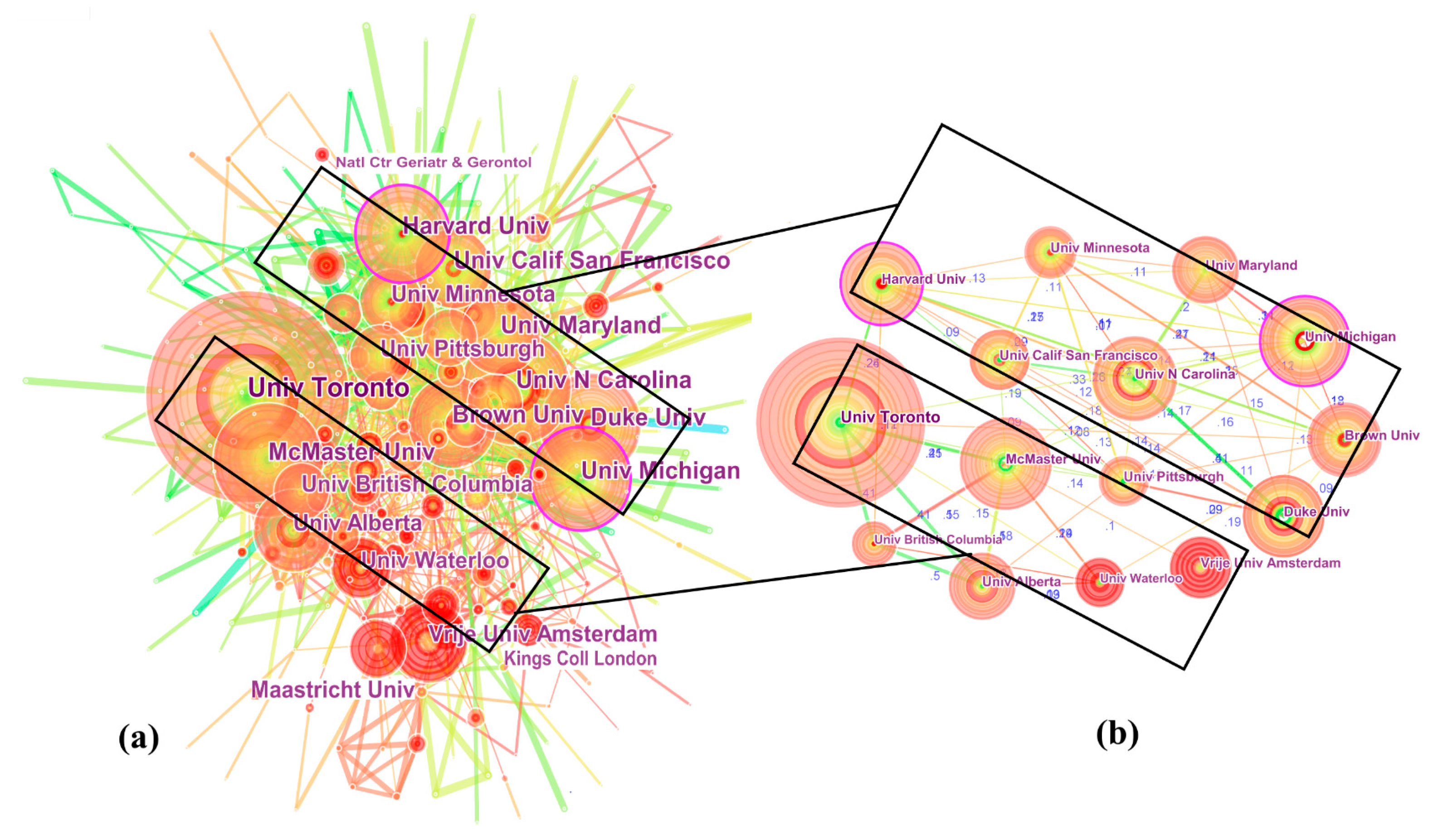
3.2.2. Institution Collaboration Analysis
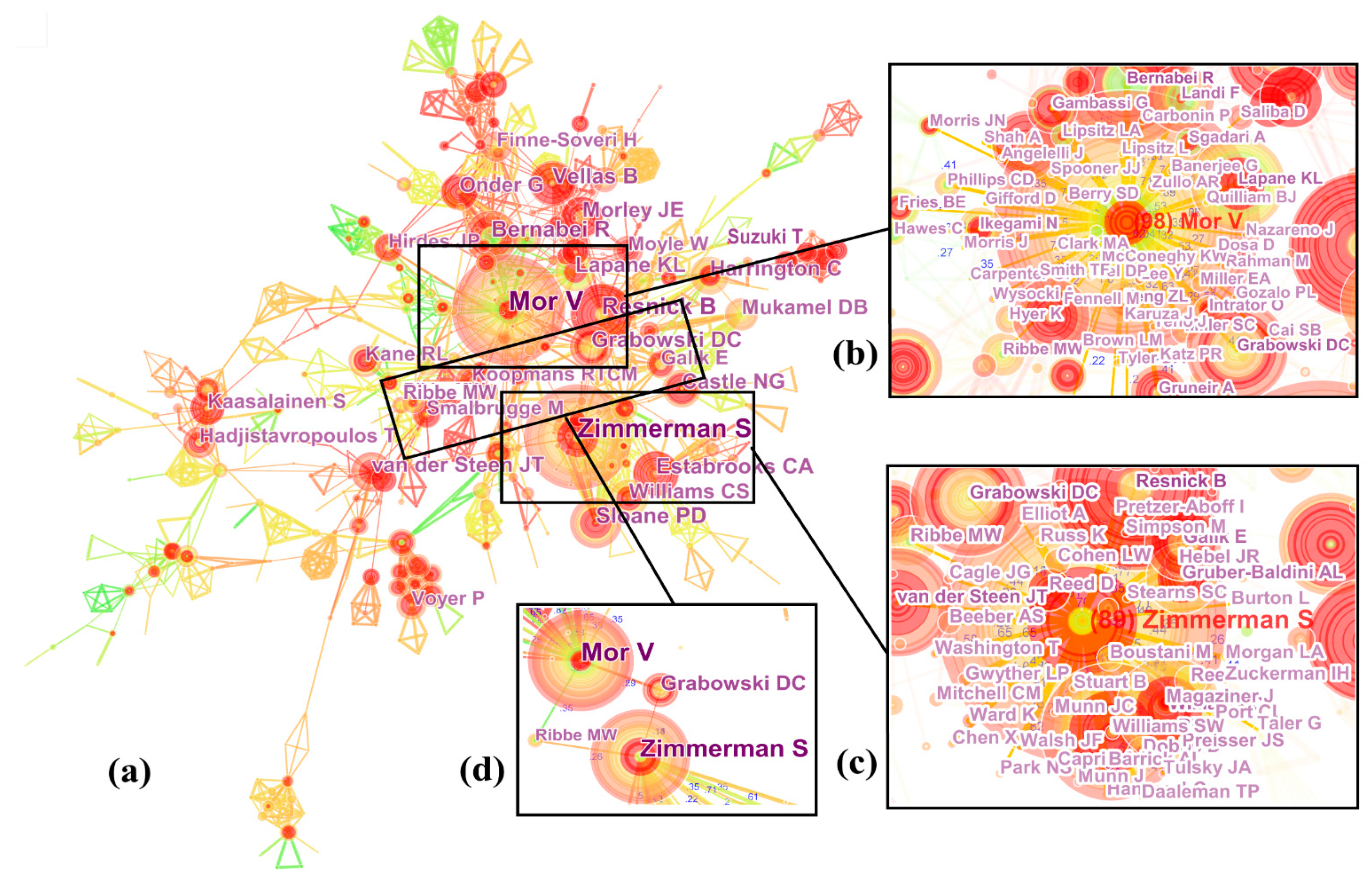
3.2.3. Author Collaboration Analysis
3.3. Intellectual Landscape of LTC Field
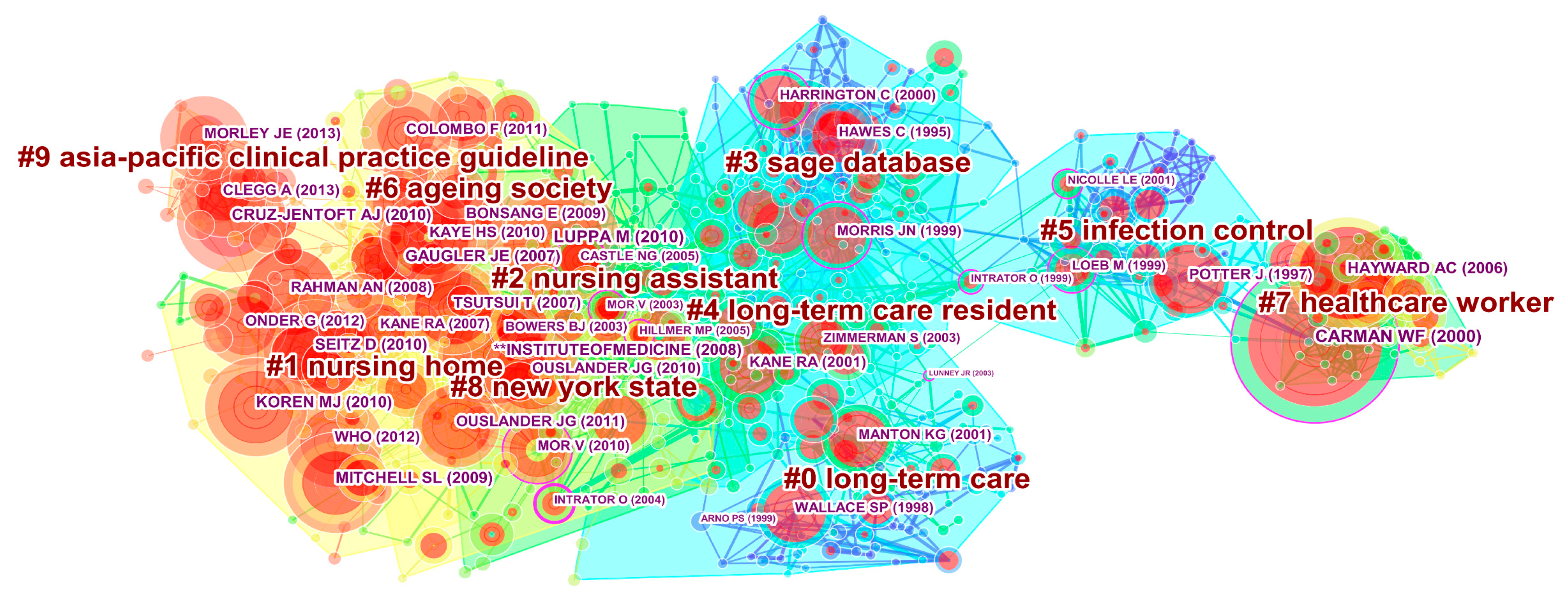
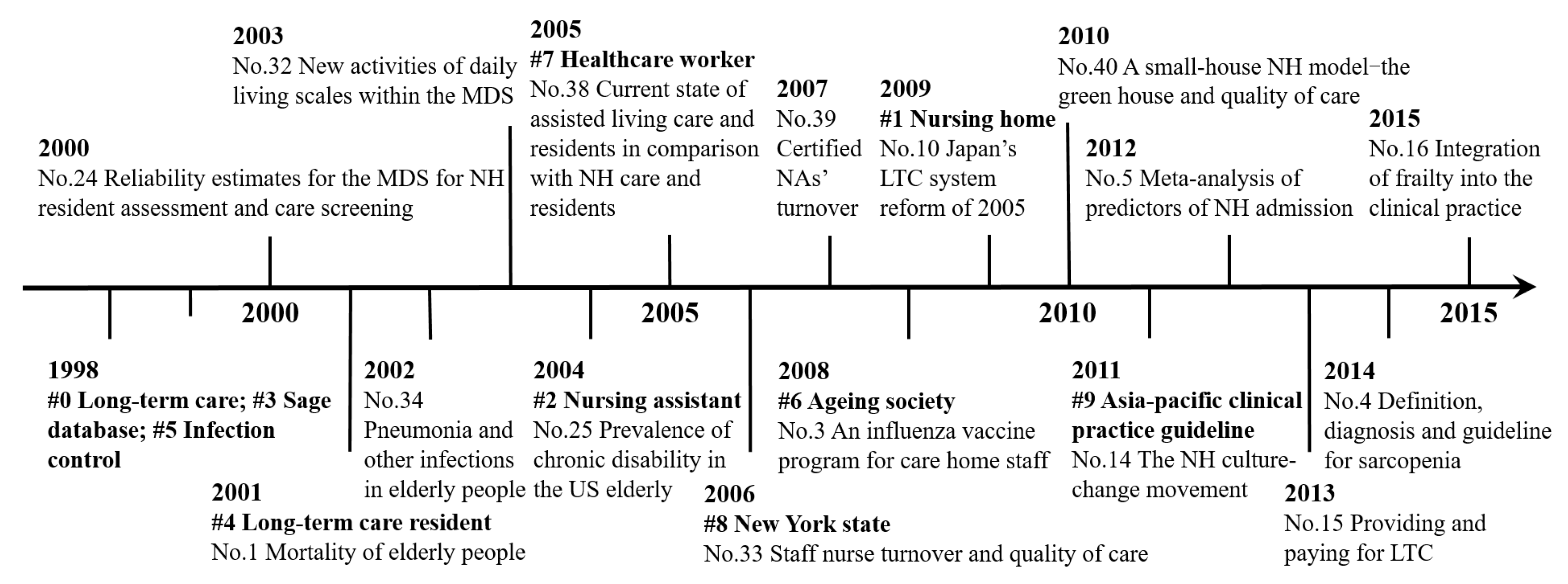
3.3.1. Document Co-citation Analysis
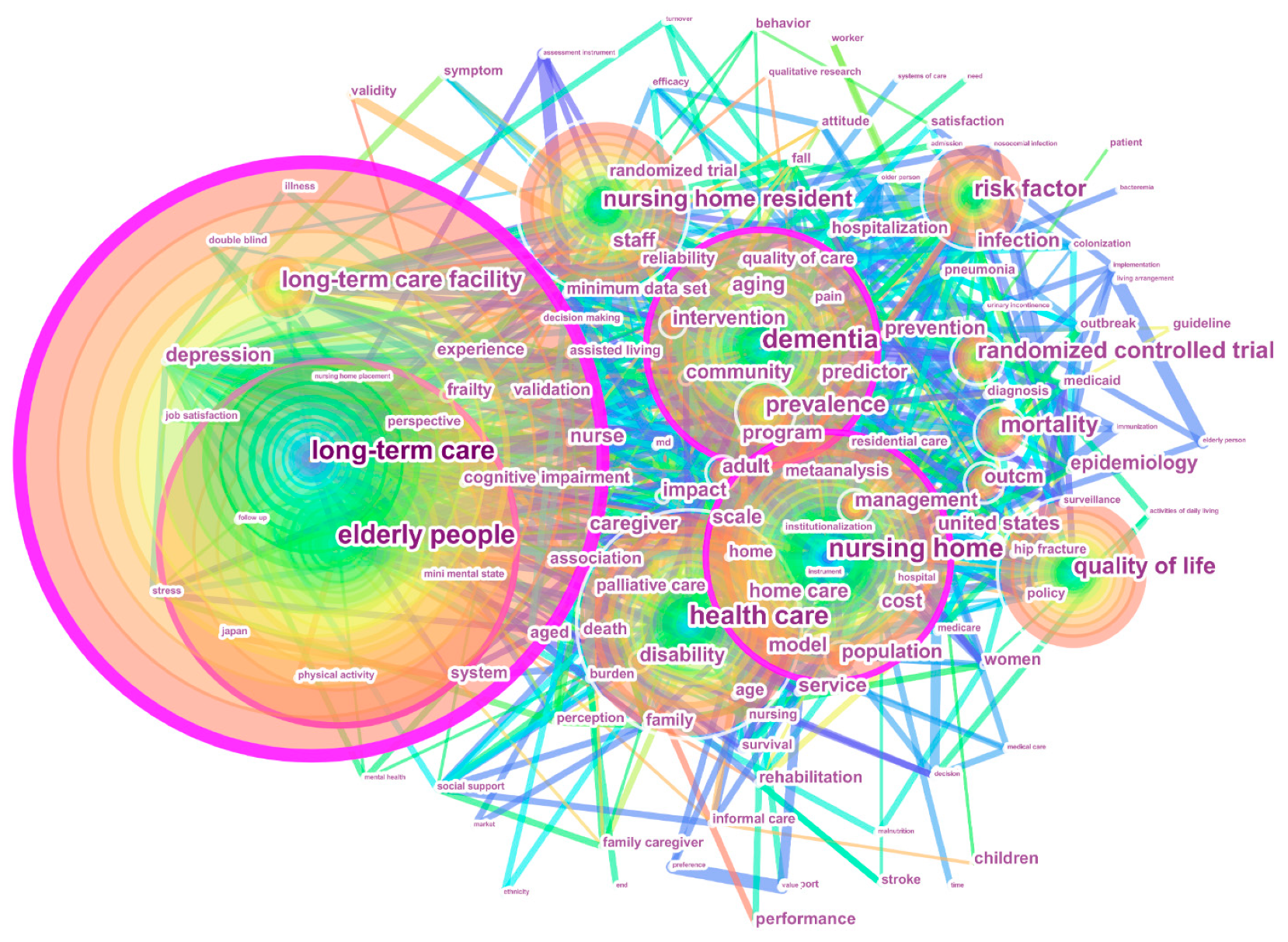
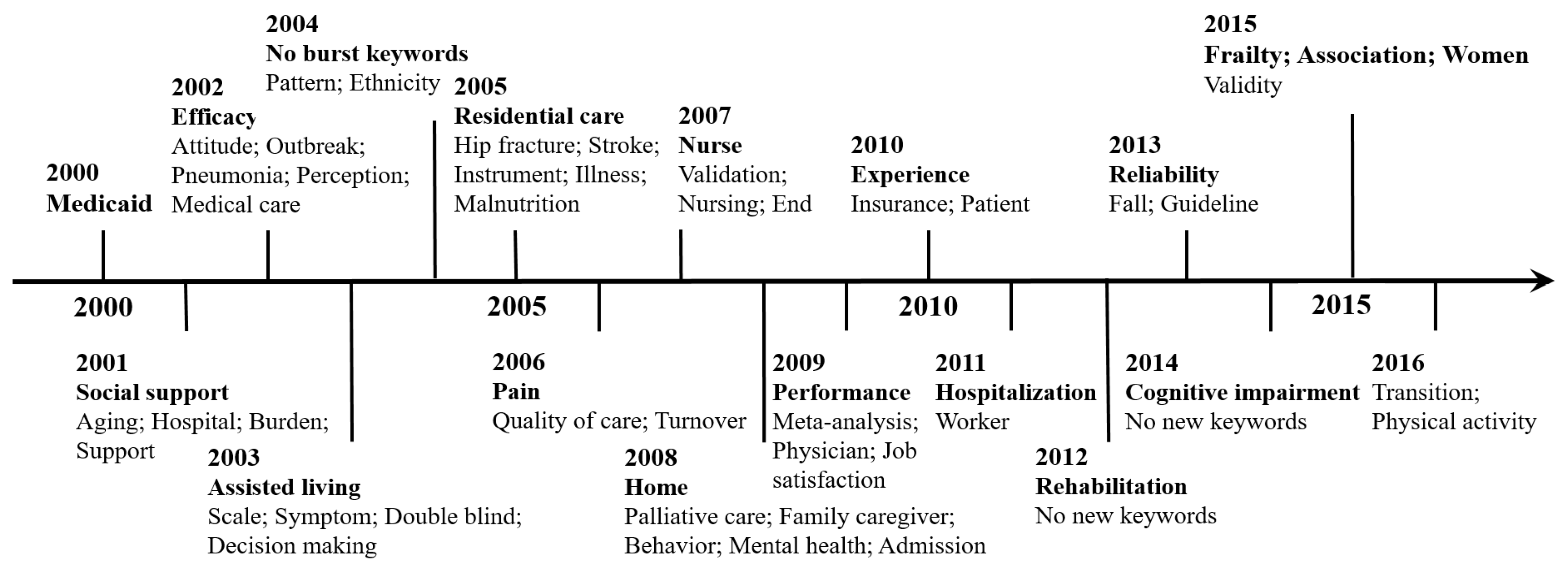
3.3.2. Keyword Co-Occurrence Analysis
- Dementia care was extracted using four keywords “long-term care,” “elderly people,” “dementia,” and “long-term care facility.” With an increasing number of people suffering from dementia, considerable attention is currently focused on improving quality of life for people with dementia [66]. Patients and caregivers are the central stakeholders in dementia care and there has been much research on the health status and care needs of elderly patients with dementia [13,14,67,68]. In terms of dementia caregivers, especially informal caregivers, compelling evidence has suggested that they suffer a high level of care burden [40,66]. Some care models for people with dementia have received increased attention, such as the ABLE model [67], person-centered care model [68], and personhood model [69].
- Quality of care was identified using six keywords “long-term care,” “nursing home,” “health care,” “quality of life,” “quality,” and “outcomes.” The quality of care for NH residents has been a major concern internationally. Despite great improvements in NHs, LTC quality in the context of population ageing remains challenging. Within this theme, three major aspects were addressed: (1) the indicators for measuring quality of care, such as depression symptoms, psychotropic drug use, physical restraints, pain management, pressure ulcers, fall incidents, and mortality rate [53,56]; (2) factors influencing quality of care, such as nurse-staffing levels, NH profit status, and the education level and training of nursing staff [40,56]; and (3) the strategies for improving quality of care, such as implementing health information technology, enhancing quality monitoring systems, strengthening the caregiving workforce, and implementing culture-change practices in NHs [5,19,21].
- Prevalence and risk factors were extracted using the keywords “prevalence,” “risk factor,” and “infection.” Psychiatric disorders are common among elderly people. In an effort to better understand and treat the diseases, some researchers have investigated the prevalence of and risk factors for common psychiatric disorders in LTC facilities, such as dementia, depression, bipolar disorder, anxiety disorders, schizophrenia, and alcohol use disorders [14]. Moreover, much evidence indicates a marked increase in the incidence of healthcare-associated infections caused by multidrug-resistant organisms (MDROs). Hence, prevention and control of MDROs has become a public health priority. In recent years, considerable attention has been paid to determining the prevalence of and risk factors for MDROs, such as methicillin-resistant staphylococcus aureus (MRSA), multidrug-resistant gram-negative bacilli (GNB), and vancomycin-resistant enterococci (VRE) [70].
- Mortality comprised five representative keywords “long-term care,” “elderly people,” “mortality,” “people,” and “population.” Patient death becomes an increasingly common occurrence in LTC literature. Identifying mortality and its predictors is important for implementing of therapeutic management for high-risk patients, with the goal of improving survival. In an LTC context, the focus of this theme can be summarized into two main aspects: (1) mortality trends and differences between different groups, such as mortality of residents with regard to age, gender, and distribution of care levels under home-based or institutional care [71]; and (2) the factors associated with mortality, such as demographic characteristics, functional and cognitive status, specific diseases (cancer and heart disease), antipsychotic drug use, social support, and influenza vaccination of health-care workers [34,72].
- Randomized controlled trial was extracted using one keyword “randomized controlled trial.” As a form of scientific experiment, it aims to evaluate the effectiveness of various types of medical interventions [34,36]. For example, one such trial was designed to determine whether vaccination of health-care workers can lower mortality and the frequency of laboratory-proven influenza infection in elderly patients in long-term care hospitals [34].
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations. World Population Prospects: The 2017 Revision. Available online: https://population.un.org/wpp/Download/Standard/Population/ (accessed on 23 September 2018).
- Huber, M.; Rodrigues, R.; Hoffmann, F.; Gasior, K.; Marin, B. Facts and Figures on Long-Term Care: Europe and North America; Occasional Reports Series 6; European Center: Vienna, Austria, 2009; Available online: https://www.euro.centre.org/publications/detail/385 (accessed on 23 September 2018).
- Stone, R.I. Long-Term Care for the Elderly with Disabilities: Current Policy, Emerging Trends, and Implications for the Twenty-First Century; The Milbank Memorial Fund: New York, NY, USA, 2000. [Google Scholar]
- Tsutsui, T.; Muramatsu, N. Japan’s universal long-term care system reform of 2005: Containing costs and realizing a vision. J. Am. Geriatr. Soc. 2007, 55, 1458–1463. [Google Scholar] [CrossRef] [PubMed]
- Colombo, F.; Llena-Nozal, A.; Mercier, J.; Tjadens, F. Help Wanted? Providing and Paying for Long-Term Care; OECD Health Policy Studies, OECD Publishing, 2011. Available online: https://dx.doi.org/10.1787/9789264097759-en (accessed on 23 September 2018).
- Kaye, H.S.; Harrington, C.; LaPlante, M.P. Long-term care: Who gets it, who provides it, who pays, and how much? Health Aff. 2010, 29, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, J.; Habib, J.; Hirschfeld, M.J. Long-Term Care in Developing Countries: Ten Case Studies; World Health Organization Collection on Long-Term Care; World Health Organization: Geneva, Switzerland, 2003; Available online: https://www.who.int/chp/knowledge/publications/Case_studies/en/ (accessed on 23 September 2018).
- Feng, Z.; Liu, C.; Guan, X.; Mor, V. China’s rapidly aging population creates policy challenges in shaping a viable long-term care system. Health Aff. 2012, 31, 2764–2773. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Mao, Z.F.; Zhong, R. Long-term care arrangements in rural China: Review of recent developments. J. Am. Med. Dir. Assoc. 2009, 10, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Kane, R.A. Long-term care and a good quality of life: Bringing them closer together. Gerontologist 2001, 41, 293–304. [Google Scholar] [CrossRef]
- Lloyd-Sherlock, P. Beyond neglect: Long-term care research in low and middle income countries. Int. J. Gerontol. 2014, 8, 66–69. [Google Scholar] [CrossRef]
- Lunney, J.R.; Lynn, J.; Foley, D.J.; Lipson, S.; Guralnik, J.M. Patterns of functional decline at the end of life. JAMA 2003, 289, 2387–2392. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.L.; Teno, J.M.; Kiely, D.K.; Shaffer, M.L.; Jones, R.N.; Prigerson, H.G.; Volicer, L.; Givens, J.L.; Hamel, M.B. The clinical course of advanced dementia. NEJM 2009, 361, 1529–1538. [Google Scholar] [CrossRef]
- Seitz, D.; Purandare, N.; Conn, D. Prevalence of psychiatric disorders among older adults in long-term care homes: A systematic review. Int. Psychogeriatr. 2010, 22, 1025–1039. [Google Scholar] [CrossRef]
- Gu, D.; Vlosky, D.A. Long-term care needs and related issues in China. In Social Sciences in Health Care and Medicine; Garner, J.B., Christiansen, T.C., Eds.; Nova Science Publishers: New York, NY, USA, 2008; pp. 51–84. [Google Scholar]
- Norton, E.C. Long-term care. Handb. Health Econ. 2000, 1, 955–994. [Google Scholar]
- Castle, N.G.; Engberg, J. Staff turnover and quality of care in nursing homes. Med. Care 2005, 43, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Hussein, S.; Manthorpe, J. An international review of long-term care workforce: Policies and shortages. J. Aging Soc. Policy 2005, 17, 75–94. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Retooling for an Aging America: Building the Health Care Workforce; The National Academies Press: Washington, DC, USA, 2008. [Google Scholar] [CrossRef]
- Karlsson, M.; Mayhew, L.; Plumb, R.; Rickayzen, B. An International Comparison of Long-Term Care Arrangements: An Investigation into the Equity, Efficiency and Sustainability of the Long-Term Care Systems in Germany, Japan, Sweden, the United Kingdom and the United States; Actuarial Research Paper No. 156; Actuarial Research Centre, Cass Business School: London, UK, 2004; Available online: http://www.doc88.com/p-978197968468.html (accessed on 23 September 2018).
- Rahman, A.N.; Schnelle, J.F. The nursing home culture-change movement: Recent past, present, and future directions for research. Gerontologist 2008, 48, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.C.; Leung, J. Long-term care in China: Issues and prospects. J. Gerontol. Soc. Work 2012, 55, 570–586. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.M. CiteSpace II: Detecting and visualizing emerging trends and transient patterns in scientific literature. J. Am. Soc. Inf. Sci. Technol. 2006, 57, 359–377. [Google Scholar] [CrossRef]
- Chen, C.D.; Ibekwe-SanJuan, F.; Hou, J.H. The structure and dynamics of co-citation clusters: A multiple perspective co-citation analysis. J. Am. Soc. Inf. Sci. Technol. 2010, 61, 1386–1409. [Google Scholar] [CrossRef]
- Chen, C.M.; Dubin, R.; Kim, M.C. Orphan drugs and rare diseases: A scientometric review (2000–2014). Expert Opin. Orphan Drugs 2014, 2, 709–724. [Google Scholar] [CrossRef]
- Chen, Y.; Wu, C. The hot spot transformation in the research evolution of maker. Scientometrics 2017, 113, 1307–1324. [Google Scholar] [CrossRef]
- Kim, M.C.; Chen, C. A scientometric review of emerging trends and new developments in recommendation systems. Scientometrics 2015, 104, 239–263. [Google Scholar] [CrossRef]
- Lee, Y.C.; Chen, C.M.; Tsai, X.T. Visualizing the knowledge domain of nanoparticle drug delivery technologies: A scientometric review. Appl. Sci. 2016, 6, 11. [Google Scholar] [CrossRef]
- Song, J.B.; Zhang, H.L.; Dong, W.L. A review of emerging trends in global PPP research: Analysis and visualization. Scientometrics 2016, 107, 1111–1147. [Google Scholar] [CrossRef]
- Xie, P. Study of international anticancer research trends via co-word and document co-citation visualization analysis. Scientometrics 2015, 105, 611–622. [Google Scholar] [CrossRef]
- Zhu, J.; Hua, W.J. Visualizing the knowledge domain of sustainable development research between 1987 and 2015: A bibliometric analysis. Scientometrics 2017, 110, 893–914. [Google Scholar] [CrossRef]
- Fang, Y.; Yin, J.; Wu, B.H. Climate change and tourism: A scientometric analysis using CiteSpace. J. Sustain. Tour. 2017, 26, 108–126. [Google Scholar] [CrossRef]
- Jin, Y.R.; Ji, S.F.; Li, X.; Yu, J.N. A scientometric review of hotspots and emerging trends in additive manufacturing. J. Manuf. Technol. Manag. 2017, 28, 18–38. [Google Scholar] [CrossRef]
- Carman, W.F.; Elder, A.G.; Wallace, L.A.; McAulay, K.; Walker, A.; Murray, G.D.; Stott, D.J. Effects of influenza vaccination of health-care workers on mortality of elderly people in long-term care: A randomised controlled trial. Lancet 2000, 355, 93–97. [Google Scholar] [CrossRef]
- Luppa, M.; Luck, T.; Weyerer, S.; Konig, H.H.; Brahler, E.; Riedel-Heller, S.G. Prediction of institutionalization in the elderly: A systematic review. Age Ageing 2010, 39, 31–38. [Google Scholar] [CrossRef]
- Hayward, A.C.; Harling, R.; Wetten, S.; Johnson, A.M.; Munro, S.; Smedley, J.; Murad, S.; Watson, J.M. Effectiveness of an influenza vaccine programme for care home staff to prevent death, morbidity, and health service use among residents: Cluster randomised controlled trial. BMJ 2006, 333, 1241–1244B. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Gaugler, J.E.; Duval, S.; Anderson, K.A.; Kane, R.L. Predicting nursing home admission in the U.S: A meta-analysis. BMC Geriatr. 2007, 7, 13. [Google Scholar] [CrossRef]
- Koren, M.J. Person-centered care for nursing home residents: The culture-change movement. Health Aff. 2010, 29, 312–317. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Dementia: A Public Health Priority. Available online: https://www.who.int/mental_health/publications/dementia_report_2012/en/ (accessed on 23 September 2018).
- Ouslander, J.G.; Lamb, G.; Perloe, M.; Givens, J.H.; Kluge, L.; Rutland, T.; Atherly, A.; Saliba, D. Potentially avoidable hospitalizations of nursing home residents: Frequency, causes, and costs. J. Am. Geriatr. Soc. 2010, 58, 627–635. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Vellas, B.; van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Ouslander, J.G.; Lamb, G.; Tappen, R.; Herndon, L.; Diaz, S.; Roos, B.A.; Grabowski, D.C.; Bonner, A. Interventions to reduce hospitalizations from nursing homes: Evaluation of the INTERACT II collaborative quality improvement project. J. Am. Geriatr. Soc. 2011, 59, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Onder, G.; Carpenter, I.; Finne-Soveri, H.; Gindin, J.; Frijters, D.; Henrard, J.C.; Nikolaus, T.; Topinkova, E.; Tosato, M.; Liperoti, R.; et al. Assessment of nursing home residents in Europe: The services and health for elderly in long term care (SHELTER) study. BMC Health Serv. Res. 2012, 12, 5. [Google Scholar] [CrossRef] [PubMed]
- Potter, J.; Stott, D.J.; Roberts, M.A.; Elder, A.G.; O’Donnell, B.; Knight, P.V.; Carman, W.F. Influenza vaccination of health care workers in long-term-care hospitals reduces the mortality of elderly patients. J. Infect. Dis. 1997, 175, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bonsang, E. Does informal care from children to their elderly parents substitute for formal care in Europe? J. Health Econ. 2009, 28, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Wallace, S.P.; Levy-Storms, L.; Kington, R.S.; Andersen, R.M. The persistence of race and ethnicity in the use of long-term care. J. Gerontol Ser. B 1998, 53B, S104–S112. [Google Scholar] [CrossRef]
- Hawes, C.; Morris, J.N.; Phillips, C.D.; Mor, V.; Fries, B.E.; Nonemaker, S. Reliability estimates for the minimum data set for nursing home resident assessment and care screening (MDS). Gerontologist 1995, 35, 172–178. [Google Scholar] [CrossRef]
- Manton, K.G.; Gu, X.L. Changes in the prevalence of chronic disability in the United States black and nonblack population above age 65 from 1982 to 1999. Proc. Natl. Acad. Sci. USA 2001, 98, 6354–6359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Intrator, O.; Zinn, J.; Mor, V. Nursing home characteristics and potentially preventable hospitalizations of long-stay residents. J. Am. Geriatr. Soc. 2004, 52, 1730–1736. [Google Scholar] [CrossRef] [PubMed]
- Harrington, C.; Carrillo, H.; Wellin, V.; Miller, N.; LeBlanc, A. Predicting state medicaid home and community based waiver participants and expenditures, 1992–1997. Gerontologist 2000, 40, 673–686. [Google Scholar] [CrossRef] [PubMed]
- Mor, V.; Berg, K.; Angelelli, J.; Gifford, D.; Morris, J.; Moore, T. The quality of quality measurement in US nursing homes. Gerontologist 2003, 43, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Mor, V.; Intrator, O.; Feng, Z.L.; Grabowski, D.C. The revolving door of rehospitalization from skilled nursing facilities. Health Aff. 2010, 29, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Nicolle, L.E. Urinary tract infections in long-term care facilities. Infect. Control Hosp. Epidemiol. 2001, 22, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Hillmer, M.P.; Wodchis, W.P.; Gill, S.S.; Anderson, G.M.; Rochon, P.A. Nursing home profit status and quality of care: Is there any evidence of an association? Med. Care Res. Rev. 2005, 62, 139–166. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.N.; Fries, B.E.; Morris, S.A. Scaling ADLs within the MDS. J. Gerontol. Ser. A-Biol. Sci. Med. Sci. 1999, 54, M546–M553. [Google Scholar] [CrossRef]
- Loeb, M.; McGeer, A.; McArthur, M.; Walter, S.; Simor, A.E. Risk factors for pneumonia and other lower respiratory tract infections in elderly residents of long-term care facilities. Arch. Intern. Med. 1999, 159, 2058–2064. [Google Scholar] [CrossRef]
- Intrator, O.; Castle, N.G.; Mor, V. Facility characteristics associated with hospitalization of nursing home residents – Results of a national study. Med. Care 1999, 37, 228–237. [Google Scholar] [CrossRef]
- Arno, P.S.; Levine, C.; Memmott, M.M. The economic value of informal caregiving. Health Aff. 1999, 18, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, S.; Gruber-Baldini, A.L.; Sloane, P.D.; Eckert, J.K.; Hebel, J.R.; Morgan, L.A.; Stearns, S.C.; Wildfire, J.; Magaziner, J.; Chen, C.; et al. Assisted living and nursing homes: Apples and oranges? Gerontologist 2003, 43, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Bowers, B.J.; Esmond, S.; Jacobson, N. Turnover reinterpreted CNAs talk about why they leave. J. Gerontol. Nurs. 2003, 29, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Kane, R.A.; Lum, T.Y.; Cutler, L.J.; Degenholtz, H.B.; Yu, T.C. Resident outcomes in small-house nursing homes: A longitudinal evaluation of the initial green house program. J. Am. Geriatr. Soc. 2007, 55, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Sanford, A.M.; Orrell, M.; Tolson, D.; Abbatecola, A.M.; Arai, H.; Bauer, J.M.; Cruz-Jentoft, A.J.; Dong, B.R.; Ga, H.; Goel, A.; et al. An international definition for “nursing home”. J. Am. Med. Dir. Assoc. 2015, 16, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Cai, S.B.; Mukamel, D.B.; Veazie, P.; Katz, P.; Temkin-Greener, H. Hospitalizations in nursing homes: Does payer source matter? Evidence from New York State. Med. Care Res. Rev. 2011, 68, 559–578. [Google Scholar]
- Zimmerman, S.; Sloane, P.D.; Williams, C.S.; Reed, P.S.; Preisser, J.S.; Eckert, J.K.; Boustani, M.; Dobbs, D. Dementia care and quality of life in assisted living and nursing homes. Gerontologist 2005, 45, 133–146. [Google Scholar] [CrossRef]
- Roberts, G.; Morley, C.; Walters, W.; Malta, S.; Doyle, C. Caring for people with dementia in residential aged care: Successes with a composite person-centered care model featuring Montessori-based activities. Geriatr. Nurs. 2015, 36, 106–110. [Google Scholar] [CrossRef]
- Stein-Parbury, J.; Chenoweth, L.; Jeon, Y.H.; Brodaty, H.; Haas, M.; Norman, R. Implementing person-centered care in residential dementia care. Clin. Gerontol. 2012, 35, 404–424. [Google Scholar] [CrossRef]
- Buron, B. Levels of personhood: A model for dementia care. Geriatr. Nurs. 2008, 29, 324–332. [Google Scholar] [CrossRef]
- Lim, C.J.; Cheng, A.C.; Kennon, J.; Spelman, D.; Hale, D.; Melican, G.; Sidjabat, H.E.; Paterson, D.L.; Kong, D.C.M.; Peleg, A.Y. Prevalence of multidrug-resistant organisms and risk factors for carriage in long-term care facilities: A nested case-control study. J. Antimicrob. Chemother. 2014, 69, 1972–1980. [Google Scholar] [CrossRef] [PubMed]
- Seger, W.; Sittaro, N.A.; Lohse, R.; Rabba, J. Comparison of survival under domestic or institutional care: The Hannover morbidity and mortality long-term care study. Dtsch. Med. Wochenschr. 2011, 136, 1465–1471. [Google Scholar] [CrossRef] [PubMed]
- Carey, E.C.; Covinsky, K.E.; Lui, L.Y.; Eng, C.; Sands, L.P.; Walter, L.C. Prediction of mortality in community-living frail elderly people with long-term care needs. J. Am. Geriatr. Soc. 2008, 56, 68–75. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rank | Country/Region | Count | Centrality | Rank | Country/Region | Centrality | Count |
|---|---|---|---|---|---|---|---|
| 1 | USA | 6308 | 0.07 | 1 | England | 0.16 | 815 |
| 2 | Canada | 1714 | 0.03 | 2 | Denmark | 0.15 | 35 |
| 3 | England | 815 | 0.16 | 3 | France | 0.12 | 380 |
| 4 | Germany | 650 | 0.02 | 4 | Scotland | 0.12 | 91 |
| 5 | Japan | 635 | 0.01 | 5 | Sweden | 0.11 | 323 |
| 6 | Netherlands | 628 | 0.02 | 6 | Switzerland | 0.10 | 180 |
| 7 | Australia | 517 | 0.05 | 7 | USA | 0.07 | 6308 |
| 8 | France | 380 | 0.12 | 8 | Spain | 0.07 | 312 |
| 9 | Taiwan | 372 | 0.01 | 9 | Czech Republic | 0.07 | 55 |
| 10 | Italy | 353 | 0.03 | 10 | India | 0.07 | 16 |
| 11 | Sweden | 323 | 0.11 | 11 | Singapore | 0.06 | 80 |
| 12 | Spain | 312 | 0.07 | 12 | Portugal | 0.06 | 40 |
| 13 | China | 250 | 0.05 | 13 | Mexico | 0.06 | 26 |
| 14 | Israel | 219 | 0.01 | 14 | Australia | 0.05 | 517 |
| 15 | South Korea | 207 | 0.01 | 15 | China | 0.05 | 250 |
| Rank | Institution | Count | Centrality | Country |
|---|---|---|---|---|
| 1 | University of Toronto (UT) | 406 | 0.07 | Canada |
| 2 | University of North Carolina (UNC) | 233 | 0.08 | USA |
| 3 | Harvard University (Harvard) | 231 | 0.14 | USA |
| 4 | University of Michigan (UM) | 222 | 0.12 | USA |
| 5 | McMaster University (McMaster) | 222 | 0.08 | Canada |
| 6 | Duke University (Duke) | 219 | 0.03 | USA |
| 7 | Brown University (Brown) | 205 | 0.09 | USA |
| 8 | University of Maryland (UMD) | 197 | 0.06 | USA |
| 9 | University of California, San Francisco (UCSF) | 188 | 0.07 | USA |
| 10 | University of Minnesota (UMN) | 173 | 0.04 | USA |
| 11 | University of Alberta (UA) | 173 | 0.03 | Canada |
| 12 | Vrije Universiteit Amsterdam (VU) | 155 | 0.02 | Netherlands |
| 13 | University of Pittsburgh (PITT) | 151 | 0.07 | USA |
| 14 | University of British Columbia (UBC) | 138 | 0.03 | Canada |
| 15 | University of Waterloo (UW) | 134 | 0.02 | Canada |
| Author | Title of Articles | Year | Count |
|---|---|---|---|
| Mor, V (98, Brown University) | Randomised trial of impact of model of integrated care and case management for older people living in the community | 1998 | 242 |
| Driven to tiers: Socioeconomic and racial disparities in the quality of nursing home care | 2004 | 187 | |
| Does receipt of hospice care in nursing homes improve the management of pain at the end of life? | 2002 | 157 | |
| Validity of diagnostic and drug data in standardized nursing home resident assessments-Potential for geriatric pharmacoepidemiology | 1998 | 141 | |
| The OBRA-87 nursing home regulations and implementation of the resident assessment instrument: Effects on process quality | 1997 | 141 | |
| A comprehensive clinical assessment tool to inform policy and practice: Applications of the Minimum Data Set | 2004 | 121 | |
| Zimmerman, S (89, University of North Carolina (UNC) at Chapel Hill) | Nursing home facility risk factors for infection and hospitalization: Importance of registered nurse turnover, administration, and social factors | 2002 | 139 |
| Attitudes, stress, and satisfaction of staff who care for residents with dementia | 2005 | 125 | |
| Assisted living and nursing home: Apples and oranges? | 2003 | 121 | |
| Dementia care and quality of life in assisted living and nursing homes | 2005 | 117 | |
| Evaluating the quality of life of long-term care residents with dementia | 2005 | 103 | |
| High-intensity environmental light in dementia: Effect on sleep and activity | 2007 | 74 |
| No. | Count | Centrality | Strength | Reference | Year | Begin | End | Cluster ID |
|---|---|---|---|---|---|---|---|---|
| 1 | 93 | 0.17 | 28.45 | Carman et al. [34] | 2000 | 2001 | 2008 | #7 |
| 2 | 74 | 0.01 | 17.96 | Luppa et al. [35] | 2010 | 2012 | 2017 | #6 |
| 3 | 65 | 0.02 | 21.85 | Hayward et al. [36] | 2006 | 2008 | 2013 | #7 |
| 4 | 61 | 0.00 | 25.53 | Cruz-Jentoft et al. [37] | 2010 | 2014 | 2017 | #9 |
| 5 | 61 | 0.04 | 19.61 | Gaugler et al. [38] | 2007 | 2012 | 2015 | #6 |
| 6 | 58 | 0.05 | 14.56 | Mitchell et al. [13] | 2009 | 2011 | 2015 | #1 |
| 7 | 57 | 0.04 | 16.49 | Seitz et al. [14] | 2010 | 2012 | 2017 | #1 |
| 8 | 57 | 0.06 | 14.60 | Institute of Medicine [19] | 2008 | 2010 | 2017 | #2 |
| 9 | 57 | 0.01 | 23.84 | Koren [39] | 2010 | 2014 | 2017 | #1 |
| 10 | 54 | 0.08 | 14.63 | Tsutsui and Muramatsu [4] | 2007 | 2009 | 2015 | #2 |
| 11 | 53 | 0.01 | 22.15 | WHO [40] | 2012 | 2014 | 2017 | #1 |
| 12 | 53 | 0.04 | 15.07 | Ouslander et al. [41] | 2010 | 2013 | 2017 | #8 |
| 13 | 53 | 0.03 | 17.95 | Kaye et al. [6] | 2010 | 2014 | 2017 | #6 |
| 14 | 50 | 0.06 | 15.45 | Rahman and Schnelle [21] | 2008 | 2011 | 2017 | #1 |
| 15 | 50 | 0.01 | 17.51 | Colombo et al. [5] | 2011 | 2013 | 2017 | #6 |
| 16 | 49 | 0.04 | 23.41 | Morley et al. [42] | 2013 | 2015 | 2017 | #9 |
| 17 | 48 | 0.01 | 22.93 | Clegg et al. [43] | 2013 | 2015 | 2017 | #9 |
| 18 | 48 | 0.01 | 16.81 | Ouslander et al. [44] | 2011 | 2013 | 2017 | #8 |
| 19 | 46 | 0.02 | 16.10 | Onder et al. [45] | 2012 | 2013 | 2017 | #1 |
| 20 | 45 | 0.05 | 19.65 | Potter et al. [46] | 1997 | 2000 | 2005 | #5 |
| 21 | 44 | 0.06 | 14.98 | Kane [10] | 2001 | 2003 | 2009 | #4 |
| 22 | 44 | 0.02 | 18.36 | Bonsang [47] | 2009 | 2014 | 2017 | #6 |
| 23 | 42 | 0.03 | 18.33 | Wallace et al. [48] | 1998 | 2000 | 2005 | #0 |
| 24 | 41 | 0.02 | 22.06 | Hawes et al. [49] | 1995 | 2000 | 2003 | #3 |
| 25 | 40 | 0.05 | 15.12 | Manton and Gu [50] | 2001 | 2004 | 2009 | #0 |
| 26 | 20 | 0.25 | 8.37 | Intrator et al. [51] | 2004 | 2007 | 2011 | #8 |
| 27 | 34 | 0.19 | 12.69 | Harrington et al. [52] | 2000 | 2001 | 2007 | #3 |
| 28 | 20 | 0.18 | 6.48 | Mor et al. [53] | 2003 | 2004 | 2010 | #2 |
| 29 | 38 | 0.17 | 9.04 | Mor et al. [54] | 2010 | 2015 | 2017 | #8 |
| 30 | 16 | 0.15 | 6.90 | Nicolle [55] | 2001 | 2005 | 2009 | #5 |
| 31 | 16 | 0.14 | 6.46 | Hillmer et al. [56] | 2005 | 2009 | 2013 | #2 |
| 32 | 38 | 0.12 | 17.40 | Morris et al. [57] | 1999 | 2003 | 2007 | #4 |
| 33 | 28 | 0.12 | 11.92 | Castle and Engberg [17] | 2005 | 2006 | 2010 | #2 |
| 34 | 26 | 0.12 | 10.93 | Loeb et al. [58] | 1999 | 2002 | 2007 | #5 |
| 35 | 5 | 0.11 | - | Lunney et al. [12] | 2003 | - | - | #0 |
| 36 | 13 | 0.10 | 5.45 | Intrator et al. [59] | 1999 | 2002 | 2007 | #5 |
| 37 | 11 | 0.10 | - | Arno et al. [60] | 1999 | - | - | #0 |
| 38 | 32 | 0.01 | 12.15 | Zimmerman et al. [61] | 2003 | 2005 | 2010 | #4 |
| 39 | 27 | 0.02 | 11.31 | Bowers et al. [62] | 2003 | 2007 | 2011 | #2 |
| 40 | 38 | 0.02 | 14.91 | Kane et al. [63] | 2007 | 2010 | 2014 | #1 |
| No. | Count | Centrality | Keyword | No. | Strength | Begin | End | Keyword |
|---|---|---|---|---|---|---|---|---|
| 1 | 4837 | 0.29 | Long-term care | 18 | 19.29 | 2000 | 2008 | Medicaid |
| 2 | 2351 | 0.11 | Elderly people | 19 | 10.73 | 2001 | 2008 | Social support |
| 3 | 2137 | 0.12 | Nursing home | 20 | 13.33 | 2002 | 2005 | Efficacy |
| 4 | 2072 | 0.09 | Health care | 21 | 11.47 | 2003 | 2005 | Assisted living |
| 5 | 1872 | 0.13 | Dementia | 22 | 17.95 | 2005 | 2009 | Residential care |
| 6 | 1647 | 0.10 | Nursing home resident | 23 | 15.28 | 2006 | 2010 | Pain |
| 7 | 1217 | 0.07 | Risk factor | 24 | 21.74 | 2007 | 2012 | Nurse |
| 8 | 983 | 0.09 | Quality of life | 25 | 7.37 | 2008 | 2009 | Home |
| 9 | 879 | 0.05 | Prevalence | 26 | 15.00 | 2009 | 2010 | Performance |
| 10 | 873 | 0.08 | Mortality | 27 | 10.61 | 2010 | 2015 | Experience |
| 11 | 861 | 0.07 | Long-term care facility | 28 | 9.79 | 2011 | 2012 | Hospitalization |
| 12 | 737 | 0.02 | People | 29 | 11.05 | 2012 | 2013 | Rehabilitation |
| 13 | 688 | 0.04 | Randomized controlled trial | 30 | 23.40 | 2013 | 2015 | Reliability |
| 14 | 643 | 0.04 | Quality | 31 | 16.94 | 2014 | 2017 | Cognitive impairment |
| 15 | 617 | 0.05 | Management | 32 | 46.40 | 2015 | 2017 | Frailty |
| 16 | 568 | 0.02 | Outcomes | 33 | 36.48 | 2015 | 2017 | Association |
| 17 | 561 | 0.02 | Population | 34 | 9.18 | 2015 | 2017 | Women |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, L.; Sun, Z.; He, L.; Liu, F.; Jing, X. Global Long-Term Care Research: A Scientometric Review. Int. J. Environ. Res. Public Health 2019, 16, 2077. https://doi.org/10.3390/ijerph16122077
Fu L, Sun Z, He L, Liu F, Jing X. Global Long-Term Care Research: A Scientometric Review. International Journal of Environmental Research and Public Health. 2019; 16(12):2077. https://doi.org/10.3390/ijerph16122077
Chicago/Turabian StyleFu, Liping, Zhaohui Sun, Lanping He, Feng Liu, and Xiaoli Jing. 2019. "Global Long-Term Care Research: A Scientometric Review" International Journal of Environmental Research and Public Health 16, no. 12: 2077. https://doi.org/10.3390/ijerph16122077
APA StyleFu, L., Sun, Z., He, L., Liu, F., & Jing, X. (2019). Global Long-Term Care Research: A Scientometric Review. International Journal of Environmental Research and Public Health, 16(12), 2077. https://doi.org/10.3390/ijerph16122077