Self-Assessment of Oral Health-Related Quality of Life in People with Ectodermal Dysplasia in Germany



Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Statistical Analysis
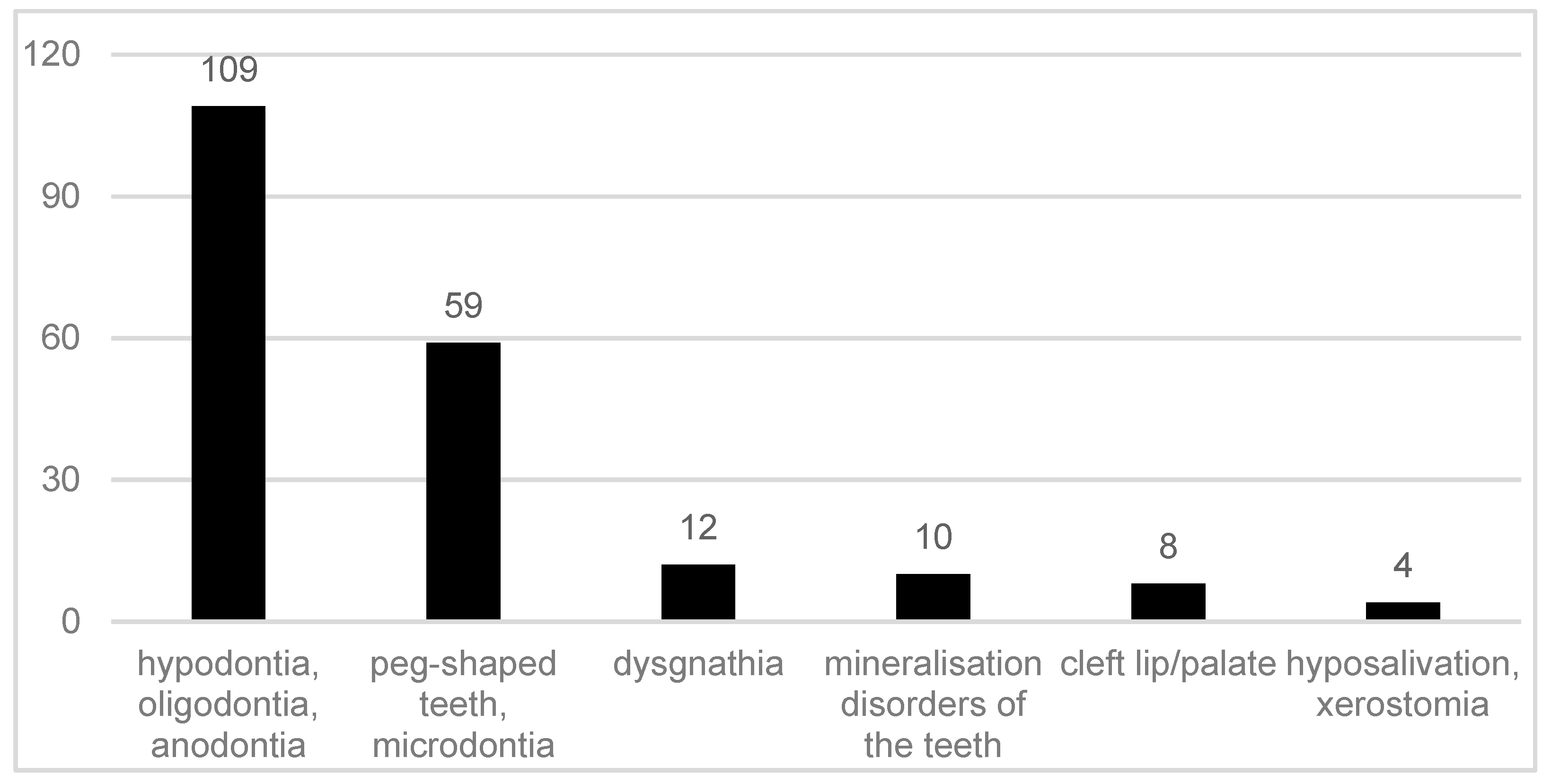
3. Results
4. Discussion
Study limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, Y.; He, J.; Decker, A.M.; Hu, J.C.; Zou, D. Clinical outcomes of implant therapy in ectodermal dysplasia patients: A systematic review. Int. J. Oral Maxillofac. Surg. 2016, 45, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, K.; Vinola, D.; John, J.B. Hypohidrotic ectodermal dysplasia—Diagnostic aids and a report of 5 cases. J. Indian Soc. Pedod. Prev. Dent. 2010, 28, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, S.N.; Kumar, V. Ectodermal dysplasia—Maxillary and mandibular alveolar reconstruction with dental rehabilitation: A case report and review of the literature. Indian J. Plast. Surg. 2010, 43, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Mikkola, M.L. Molecular aspects of hypohidrotic ectodermal dysplasia. Am. J. Med. Genet. A 2009, 149, 2031–2036. [Google Scholar] [CrossRef] [PubMed]
- Visinoni, A.F.; Lisboa-Costa, T.; Pagnan, N.A.; Chautard-Freire-Maia, E.A. Ectodermal dysplasias: Clinical and molecular review. Am. J. Med. Genet. A 2009, 149, 1980–2002. [Google Scholar] [CrossRef] [PubMed]
- Bohring, A.; Stamm, T.; Spaich, C.; Haase, C.; Spree, K.; Hehr, U.; Hoffmann, M.; Ledig, S.; Sel, S.; Wieacker, P.; et al. WNT10A mutations are a frequent cause of a broad spectrum of ectodermal dysplasias with sex-biased manifestation pattern in heterozygotes. Am. J. Hum. Genet. 2009, 85, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Dall’Oca, S.; Ceppi, E.; Pompa, G.; Polimeni, A. X-linked hypohidrotic ectodermal Dysplasia: A tem-year case report and clinical considerations. Eur. J. Ped. Dent. 2008, 9, 14–18. [Google Scholar]
- Hanisch, M.; Bohner, L.; Jung, S.; Kleinheinz, J. Seltene Erkrankungen mit implantologischem Therapiebedarf: Ektodermale Dysplasien. Implantologie 2018, 26, 157–166. [Google Scholar]
- Nordgarden, H.; Jensen, J.L.; Storhaug, K. Oligodontia is associated with extra-oral ectodermal symptoms and low whole salivary flow rates. Oral Dis. 2001, 7, 226–232. [Google Scholar] [PubMed]
- Bergendal, B.; Norderyd, J.; Bagesund, M.; Holst, A. Signs and symptoms from ectodermal organs in young Swedish individuals with oligodontia. Int. J. Paediatr. Dent. 2006, 16, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Koul, M.; Dwivedi, R.; Upadhyay, V. Ectrodactyly-ectodermal dysplasia clefting syndrome (EEC syndrome). J. Oral Biol. Craniofac. Res. 2014, 4, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Bergendal, B.; McAllister, A.; Stecksen-Blicks, C. Orofacial dysfunction in ectodermal dysplasias measured using the Nordic Orofacial Test-Screening protocol. Acta Odontol. Scand. 2009, 67, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Hobkirk, J.A.; Brook, A.H. The management of patients with severe hypodontia. J. Oral Rehabil. 1980, 7, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Hanisch, M.; Jung, S.; Kleinheinz, J. Oral Health-Related Quality of Life in Rare Diseases with Oral Manifestations. Gesundheitswesen 2018, 13. [Google Scholar] [CrossRef]
- Wiemann, S.; Frenzel Baudisch, N.; Jordan, R.A.; Kleinheinz, J.; Hanisch, M. Oral Symptoms and Oral Health-Related Quality of Life in People with Rare Diseases in Germany: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 1493. [Google Scholar] [CrossRef] [PubMed]
- Hanisch, M.; Wiemann, S.; Bohner, L.; Kleinheinz, J.; Jung, S. Association between Oral Health-Related Quality of Life in People with Rare Diseases and Their Satisfaction with Dental Care in the Health System of the Federal Republic of Germany. Int. J. Environ. Res. Public Health 2018, 15, 1732. [Google Scholar] [CrossRef] [PubMed]
- Hanisch, M.; Wiemann, S.; Jung, S.; Kleinheinz, J.; Bohner, L. Oral Health-Related Quality of Life in People with Rare Hereditary Connective Tissue Disorders: Marfan Syndrome. Int. J. Environ. Res. Public Health 2018, 15, 2382. [Google Scholar] [CrossRef] [PubMed]
- John, M.T.; Miglioretti, D.L.; LeResche, L.; Koepsell, T.D.; Hujoel, P.; Micheelis, W. German short forms of the Oral Health Impact Profile. Community Dent. Oral Epidemiol. 2006, 34, 277–288. [Google Scholar] [CrossRef] [PubMed]
- The Portal for Rare Diseases and Orphan Drugs. Available online: https://www.orpha.net (accessed on 13 March 2019).
- John, M.T.; Micheelis, W. Mundgesundheitsbezogene Lebensqualität in der Bevölkerung: Grundlagen und Ergebnisse des OHIP aus einer repräsentativen Stichprobe in Deutschland. IDZ-Inf. 2003, 1, 1–28. [Google Scholar]
- Für eine ausreichende, zweckmäßige und wirtschaftliche vertragszahnärztliche Versorgung. Available online: https://www.g-ba.de/downloads/62-492-78/RL-Z_Behandlung_2006-03-01.pdf (accessed on 27 December 2018).
- Hanisch, M.; Hanisch, L.; Kleinheinz, J.; Danesh, G.; Benz, K.; Jackowski, J. Orthodontically-Relevant Manifestations in People with Rare Diseases. Med. Princ. Pract. 2019. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean (Standard Deviation) | Median (Interquartil Range) | 95% CI | p-Value | |
|---|---|---|---|---|
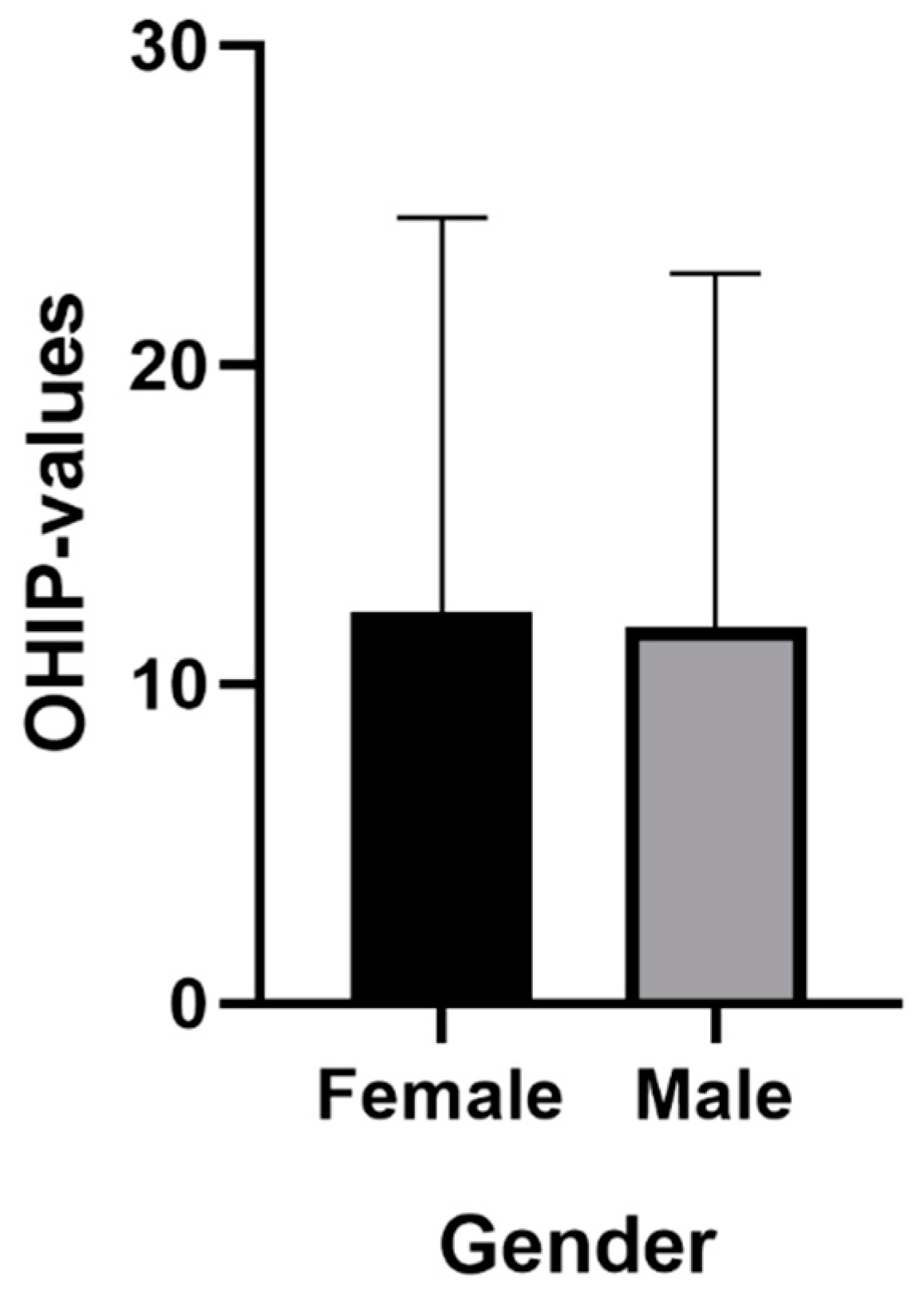
| Gender | 0.781 | |||
| M | 11.79 (11.08) | 9 (17.25) | (8.97; 14.60) | |
| F | 12.23 (12.39) | 8 (18) | (7.91; 16.55) | |
| Difficulties in finding a dentist | 0.001 * | |||
| No | 9.21 (8.58) | 5 (13) | (6.94; 11.47) | |
| Yes | 19.72 (13.06) | 19 (20.50) | (14.32; 25.11) | |
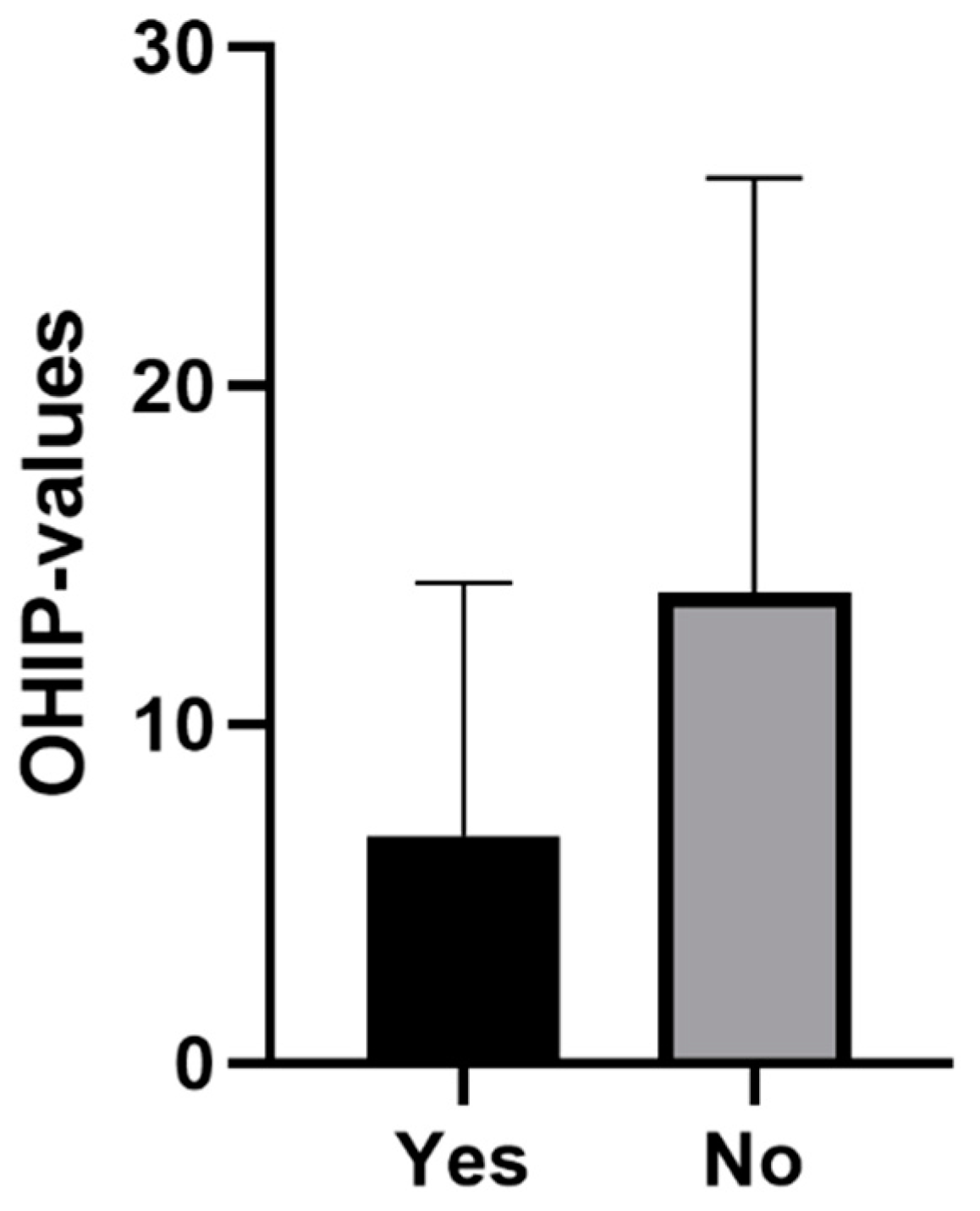
| Satisfaction with the Health System | 0.007 * | |||
| No | 13.91 (12.22) | 10 (20) | (10.97; 16.84) | |
| Yes | 6.92 (7.48) | 5 (11) | (3.96; 9.88) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanisch, M.; Sielker, S.; Jung, S.; Kleinheinz, J.; Bohner, L. Self-Assessment of Oral Health-Related Quality of Life in People with Ectodermal Dysplasia in Germany. Int. J. Environ. Res. Public Health 2019, 16, 1933. https://doi.org/10.3390/ijerph16111933
Hanisch M, Sielker S, Jung S, Kleinheinz J, Bohner L. Self-Assessment of Oral Health-Related Quality of Life in People with Ectodermal Dysplasia in Germany. International Journal of Environmental Research and Public Health. 2019; 16(11):1933. https://doi.org/10.3390/ijerph16111933
Chicago/Turabian StyleHanisch, Marcel, Sonja Sielker, Susanne Jung, Johannes Kleinheinz, and Lauren Bohner. 2019. "Self-Assessment of Oral Health-Related Quality of Life in People with Ectodermal Dysplasia in Germany" International Journal of Environmental Research and Public Health 16, no. 11: 1933. https://doi.org/10.3390/ijerph16111933
APA StyleHanisch, M., Sielker, S., Jung, S., Kleinheinz, J., & Bohner, L. (2019). Self-Assessment of Oral Health-Related Quality of Life in People with Ectodermal Dysplasia in Germany. International Journal of Environmental Research and Public Health, 16(11), 1933. https://doi.org/10.3390/ijerph16111933