Horsepower of Doctors’ Cars Correlates with Cardiovascular Risk and Sedentary Lifestyle but Not with Sexual Dysfunction or Sexual Satisfaction

 ,
,  and
and
Abstract
1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Statistical Analysis
3. Results
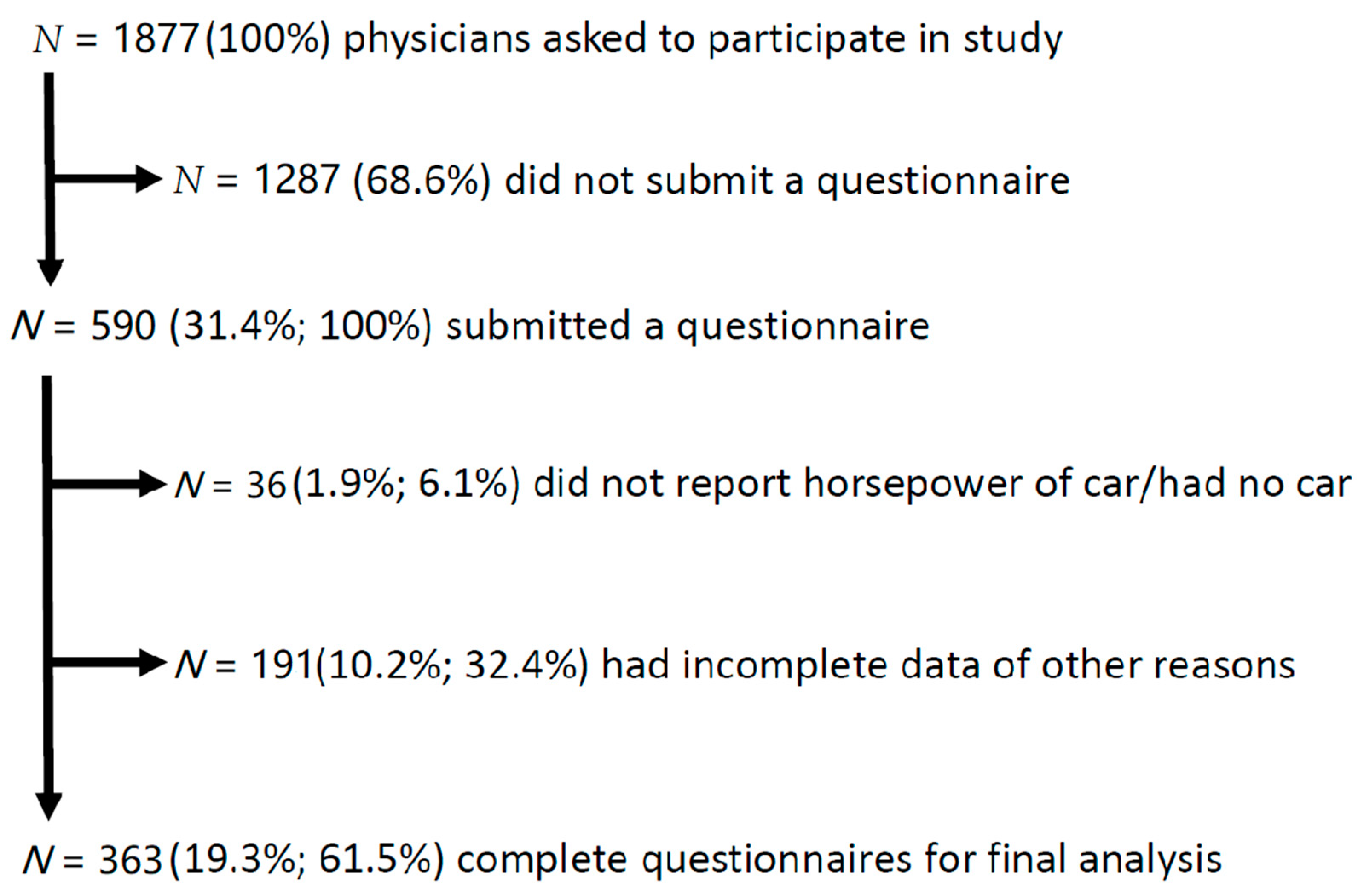
3.1. Participants
3.2. Associations between HP of Physicians’ Cars and Health Determinants
4. Discussion
5. Conclusion
Author Contributions
Funding
Conflicts of Interest
References
- “Horsepower”. Encyclopaedia Britannica Online. Available online: https://www.britannica.com/science/horsepower (accessed on 25 May 2019).
- Directive 2009/3/EC of the European Parliament and of the Council of 11 March 2009. Off. J. Eur. Union 2009, 114, 10–13.
- McCartt, A.T.; Hu, W. Effects of vehicle power on passenger vehicle speeds. Traffic. Inj. Prev. 2017, 4, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Dora, C.; Phillips, M. Transport, Environment and Health; WHO Regional Office Europe: Copenhagen, Denmark, 2000. [Google Scholar]
- Ding, D.; Gebel, K.; Phongsavan, P.; Bauman, A.E.; Merom, D. Driving: A Road to Unhealthy Lifestyles and Poor Health Outcomes. PLoS ONE 2014, 9, e94602. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Wijndaele, K.; Koohsari, M.J.; Tanamas, S.K.; Dunstan, D.W.; Owen, N. Adverse associations of car time with markers of cardio-metabolic risk. Prev. Med. 2016, 83, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Ding, D.; Owen, N. Commuting by car: Weight gain among physically active adults. Am. J. Prev. Med. 2013, 44, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Kawada, T. Commuting by Car, Lifestyles, and Weight Gain. Am. J. Prev. Med. 2013, 45, e1–e2. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.D.; Andresen, M.A.; Schmid, T.L. Obesity relationships with community design, physical activity, and time spent in cars. Am. J. Prev. Med. 2004, 27, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Christian, T.J. Automobile commuting duration and the quantity of time spent with spouse, children, and friends. Prev. Med. 2012, 55, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Christian, T.J. Trade-Offs Between Commuting Time and Health-Related Activities. J. Urban Health 2012, 89, 746–757. [Google Scholar] [CrossRef]
- Rasmussen, C.; Garner, L.; Knapp, T.J. Driving-Induced Stress in Urban College Students. Percept. Mot. Skills 2000, 90, 437–443. [Google Scholar] [CrossRef]
- Small Penis Car. Available online: http://www.urbandictionary.com/define.php?term=small+penis+car (accessed on 25 May 2019).
- Horse Power Male Enhancement. Available online: https://horsepowermaleenhancement.wordpress.com (accessed on 25 May 2019).
- Steger, B.; Colvin, H.P.; Rieder, J. Scientific activity and working hours of physicians in university hospitals: Results from the Innsbruck and Salzburg physician lifestyle assessment (TISPLA). Wien. Klin. Wochenschr. 2009, 121, 685–689. [Google Scholar] [CrossRef] [PubMed]
- Ulmer, H.; Diem, G.; Bischof, H.P.; Ruttmann, E.; Concin, H. Recent trends and sociodemographic distribution of cardiovascular risk factors: Results from two population surveys in the Austrian WHO CINDI demonstration area. Wien. Klin. Wochenschr. 2001, 113, 573–579. [Google Scholar] [PubMed]
- Lansley, G. Cars and socio-economics: Understanding neighbourhood variations in car characteristics from administrative data. Reg. Stud. Reg. Sci. 2016, 3, 264–285. [Google Scholar] [CrossRef]
- Cunningham, C.T.; Quan, H.; Hemmelgarn, B.; Noseworthy, T.; Beck, A.C.; Dixon, E.; Samuel, S.; Ghali, A.W.; Sykes, L.L.; Jetté, N. Exploring physician specialist response rates to web-based surveys. BMC Med. Res. Methodol. 2015, 15, 32. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | <80 HP n = 114 | 80–120 HP n = 175 | 120–160 HP n = 53 | >160 HP n = 21 | p Value | p Value (Corrected for Age) |
|---|---|---|---|---|---|---|
| age (years; mean ± SD) | 35.6 ± 7.7 | 37.8 ± 7.7 | 41.0 ± 8.6 | 39.4 ± 7.9 | <0.001 | n.a. |
| male (n (%)) | 48 (42.1) | 105 (60.0) | 37 (69.8) | 18 (85.7) | <0.001 | <0.001 |
| leading position (n (%)) | 21 (18.4) | 63 (36.0) | 25 (47.2) | 13 (61.9) | <0.001 | <0.001 |
| monthly income (Euro, rounded; mean ± SD) | 1800 ± 300 | 2100 ± 500 | 2400 ± 400 | 2500 ± 400 | <0.001 | <0.001 |
| scientific output (IF; mean ± SD) | 26.3 ± 61.0 | 25.5 ± 45.5 | 60.8 ± 91.8 | 33.7 ± 42.1 | 0.206 | 0.001 |
| scientific output (publications; mean ± SD) | 8.4 ± 20.7 | 11.0 ± 20.6 | 22.4 ± 30.6 | 10.9 ± 17.4 | 0.032 | <0.001 |
| daily travel by walking/cycling (no travel, n (%)) | 30 (26.3) | 48 (27.4) | 24 (45.3) | 8 (38.1) | 0.010 | 0.262 |
| fitness level (1-very good; 5-bad) | 2.73 ± 0.88 | 2.84 ± 0.88 | 2.77 ± 0.98 | 3.24 ± 1.00 | 0.118 | 0.837 |
| BMI (kg/m2; mean ± SD) | 23.0 ± 3.0 | 23.4 ± 3.1 | 23.7 ± 3.0 | 24.7 ± 3.0 | 0.088 | <0.001 |
| hypercholesteremia (n (%)) | 9 (7.89%) | 13 (7.43%) | 8 (15.09%) | 6 (28.75%) | 0.009 | 0.001 |
| max. weight (kg; mean ± SD) | 74.4 ± 17.0 | 76.9 ± 16.5 | 79.4 ± 15.3 | 84.3 ± 10.7 | 0.004 | <0.001 |
| maternity leave (n (%)) | 23 (20.18%) | 35 (20.00%) | 3 (5.66%) | 1 (4.76%) | 0.002 | <0.001 |
| current smokers (n (%)) | 25 (22.5%) | 41 (23.8%) | 10 (18.9%) | 9 (42.9%) | 0.148 | 0.486 |
| former smokers (n (%)) | 25 (22.5%) | 47 (27.3%) | 20 (37.7%) | 3 (14.3%) | 0.148 | 0.486 |
| never smokers (n (%)) | 61 (55.0) | 84 (48.8) | 23 (43.4) | 9 (42.9) | 0.148 | 0.486 |
| Arterial hypertension (n (%)) | 5 (4.4) | 6 (3.4) | 5 (9.4) | 2 (9.5) | 0.244 | 0.002 |
| sexual dysfunction (n (%)) | 6 (12.5) | 4 (3.8) | 4 (10.8) | 2 (11.1) | 0.191 | 0.614 |
| sexual dysfunction (n (% of male subgroup)) | 6 (12.8) | 4 (3.9) | 4 (5.6) | 2 (11.1) | 0.203 | 0.104 |
| sexual satisfaction (1-very good, 5-bad; mean ± SD) | 3.23 ± 1.36 | 3.36 ± 1.23 | 3.46 ± 1.10 | 3.10 ± 1.34 | 0.455 | 0.424 |
| sexual satisfaction in male subgroup (1-very good, 5-bad; mean ± SD) | 3.21 ± 1.41 | 3.40 ± 1.13 | 3.53 ± 1.16 | 3.11 ± 1.41 | 0.527 | 0.190 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niederseer, D.; Gilhofer, T.; Schmied, C.; Steger, B.; Dankl, C.; Colvin, H.P.; Rieder, J.; Neunhäuserer, D.; Niebauer, J.; Datz, C. Horsepower of Doctors’ Cars Correlates with Cardiovascular Risk and Sedentary Lifestyle but Not with Sexual Dysfunction or Sexual Satisfaction. Int. J. Environ. Res. Public Health 2019, 16, 1932. https://doi.org/10.3390/ijerph16111932
Niederseer D, Gilhofer T, Schmied C, Steger B, Dankl C, Colvin HP, Rieder J, Neunhäuserer D, Niebauer J, Datz C. Horsepower of Doctors’ Cars Correlates with Cardiovascular Risk and Sedentary Lifestyle but Not with Sexual Dysfunction or Sexual Satisfaction. International Journal of Environmental Research and Public Health. 2019; 16(11):1932. https://doi.org/10.3390/ijerph16111932
Chicago/Turabian StyleNiederseer, David, Thomas Gilhofer, Christian Schmied, Bernhard Steger, Christian Dankl, Hans Peter Colvin, Josef Rieder, Daniel Neunhäuserer, Josef Niebauer, and Christian Datz. 2019. "Horsepower of Doctors’ Cars Correlates with Cardiovascular Risk and Sedentary Lifestyle but Not with Sexual Dysfunction or Sexual Satisfaction" International Journal of Environmental Research and Public Health 16, no. 11: 1932. https://doi.org/10.3390/ijerph16111932
APA StyleNiederseer, D., Gilhofer, T., Schmied, C., Steger, B., Dankl, C., Colvin, H. P., Rieder, J., Neunhäuserer, D., Niebauer, J., & Datz, C. (2019). Horsepower of Doctors’ Cars Correlates with Cardiovascular Risk and Sedentary Lifestyle but Not with Sexual Dysfunction or Sexual Satisfaction. International Journal of Environmental Research and Public Health, 16(11), 1932. https://doi.org/10.3390/ijerph16111932