Area-Based Socio-Economic Inequalities in Mortality from Lung Cancer and Respiratory Diseases

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Project
2.2. Mortality
2.3. Indicator of the Socioeconomic Status of the Sub-Region (Area-Based SES)
2.4. Other Explanatory Variables
2.5. Statistical Analysis
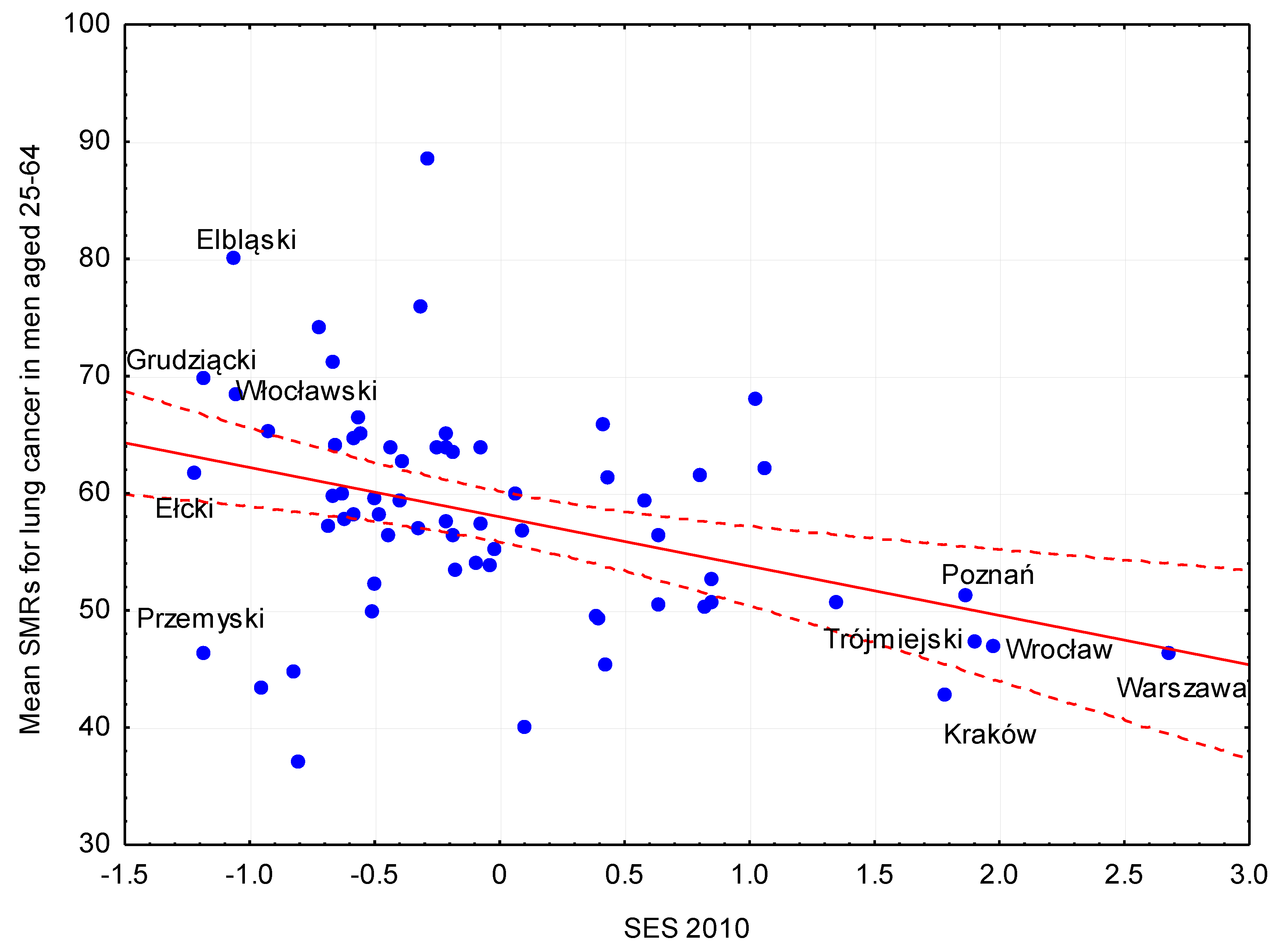
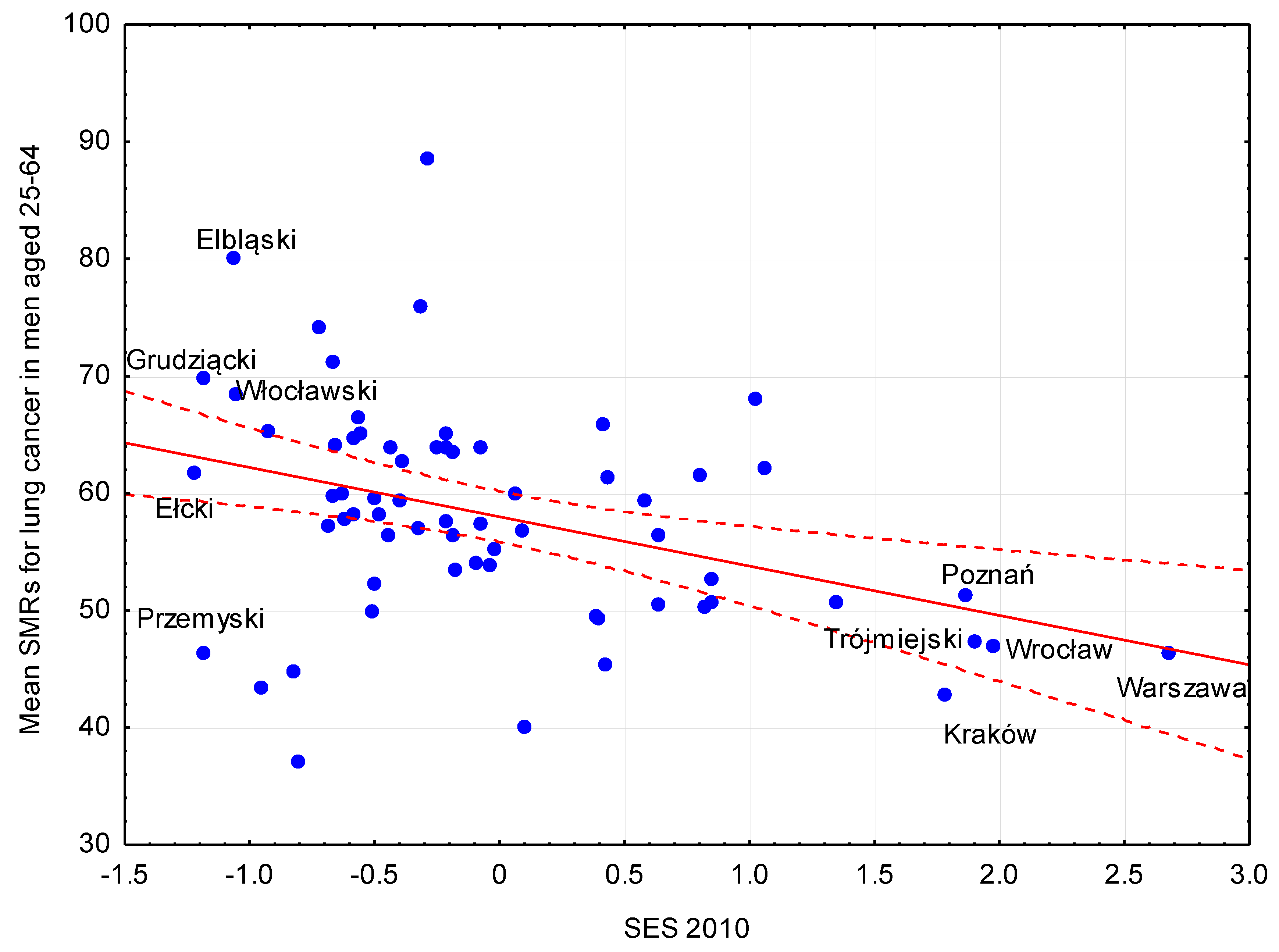
- The estimation of the relationship between mortality rate and the SES indicator of the sub-region calculated for the first year of observation (2010).
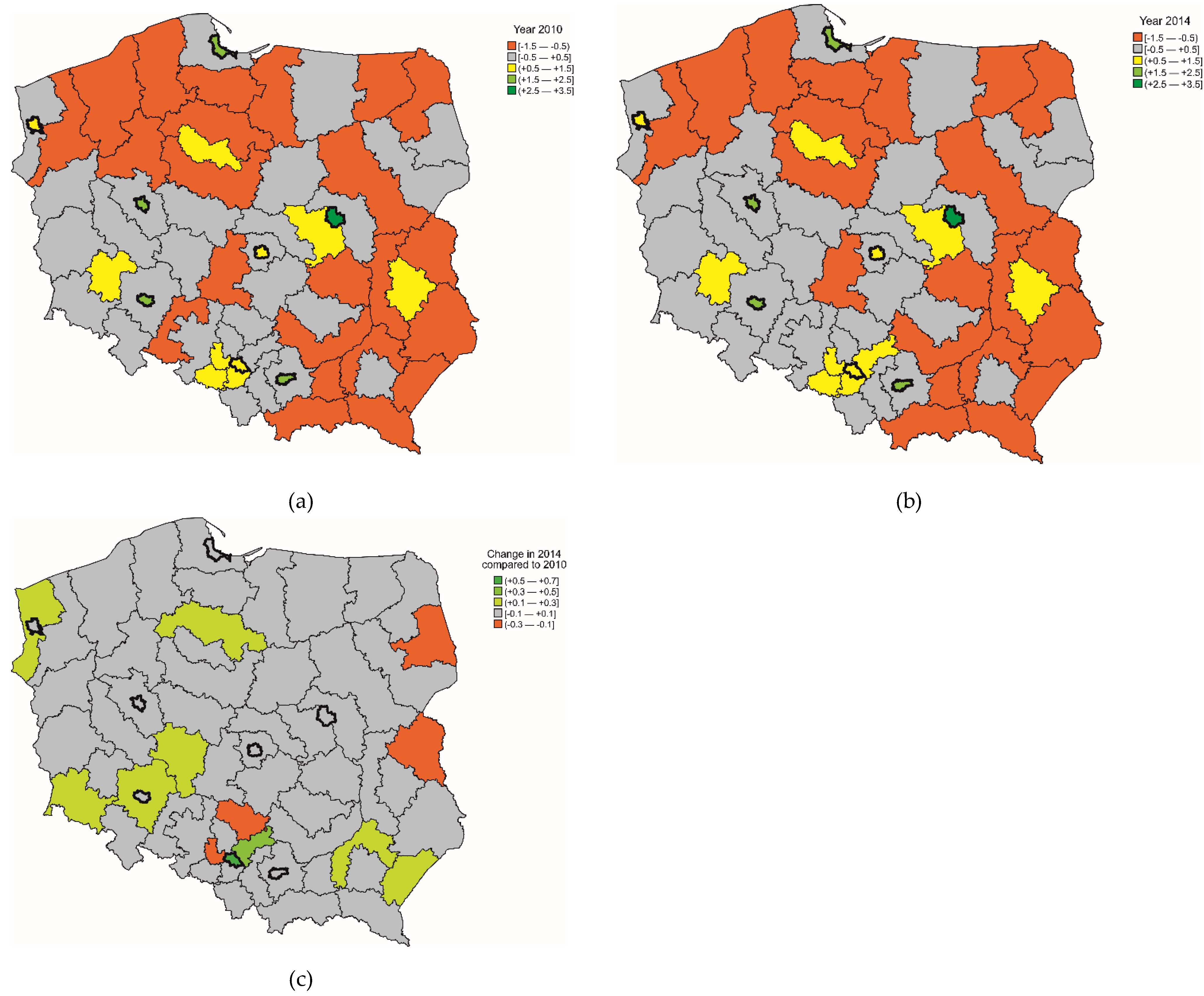
- The estimation of the relationship between the mortality rate and the change in the SES indicator between the years 2010 and 2014.
3. Results
3.1. Mortality Due to Respiratory Diseases and Lung Cancer
3.2. Indicator of the Socioeconomic Status of the Sub-Region (Area-Based SES) and Environmental Pollution
3.3. Area-Based Socioeconomic Inequalities in Mortality
4. Discussion
4.1. Main Findings
4.2. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Murray, C.J.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-Adjusted Life Years (DALYs) for 291 Diseases and Injuries in 21 Regions, 1990–2010: A Systematic Analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Naghavi, M.; Wang, H.; Lozano, R.; Davis, A.; Liang, X.; Zhou, M.; Vollset, S.E.; Ozgoren, A.A.; Abdalla, S.; Abd-Allah, F.; et al. Global, Regional, and National Age-Sex Specific All-Cause and Cause-Specific Mortality for 240 Causes of Death, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar]
- World Health Organization: European Health Information Gateway [2014]. Available online: https://gateway.euro.who.int/en/hfa-explorer/ (accessed on 2 December 2018).
- Genowska, A.; Fryc, J.; Pinkas, J.; Jamiolkowski, j.; Szafraniec, K.; Szpak, A.; Bojar, L. Social Costs of Loss in Productivity-Related Absenteeism in Poland. Int. J. Occup. Med. Environ. Health 2017, 30, 917–932. [Google Scholar] [CrossRef]
- Niżankowska-Mogilnicka, E.; Mejza, F.; Buist, A.S.; Vollmer, W.M.; Skucha, W.; Harat, R.; Pajak, A.; Gasowski, J.; Frey, J.; Nastalek, P.; et al. Prevalence of COPD and Tobacco Smoking in Malopolska Region-Results from the BOLD Study in Poland. Pol. Arch. Med. Wewn. 2007, 117, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Wziątek-Nowak, W.; Gierczyński, J.; Dąbrowiecki, P.; Gałązka-Sobotka, M.; Fal, A.M.; Gryglewicz, J.; Badyda, A.J. Socioeconomic Effects of Chronic Obstructive Pulmonary Disease from the Public Payer’s Perspective in Poland. Adv. Exp. Med. Biol. 2016, 885, 53–66. [Google Scholar] [PubMed]
- Carter, B.D.; Abnet, C.C.; Feskanich, D. Smoking and Mortality—Beyond Established Causes. New Engl. J. Med. 2015, 372, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.N.; Forey, B.A.; Coombs, K.J. Systematic Review with Meta-Analysis of the Epidemiological Evidence in the 1900s Relating Smoking to Lung Cancer. BMC Cancer. 2012, 12, 385. [Google Scholar] [CrossRef] [PubMed]
- Jedrychowski, W.; Becher, H.; Wahrendorf, J.; Basa-Cierpialek, Z. A Case-Control Study of Lung Cancer with Special Reference to the Effect of Air Pollution in Poland. J. Epidemiol. Community Health 1990, 44, 114–120. [Google Scholar] [CrossRef]
- Mejza, F.; Gnatiuc, L.; Buist, A.S.; Vollmer, W.M.; Lamprecht, B.; Obaseki, D.O.; Nastalek, P.; Nizankowska-Mogilnicka, E.; Burney, P.G.J.; Collaboratorset, B.O.L.D.; et al. Prevalence and Burden of Chronic Bronchitis Symptoms: Results from the BOLD Study. Eur. Respir. J. 2017, 50, 1700621. [Google Scholar] [CrossRef]
- Naess, Ø.; Nafstad, P.; Aamodt, G.; Claussen, B.; Rosland, P. Relation between Concentration of Air Pollution and Cause-Specific Mortality: Four-Year Exposures to Nitrogen Dioxide and Particulate Matter Pollutants in 470 Neighborhoods in Oslo, Norway. Am. J. Epidemiol. 2007, 165, 435–443. [Google Scholar] [CrossRef]
- Wojtyniak, B.; Goryński, P. Sytuacja Zdrowotna Ludności Polski I Jej Uwarunkowania; NIZP-PZH: Warszawa, Poland, 2016. [Google Scholar]
- Walsh, D.; Taulbut, M.; Hanlon, P. The Aftershock of Deindustrialization—Trends in Mortality in Scotland and Other Parts of Post-Industrial Europe. Eur. J. Public Health 2010, 20, 58–64. [Google Scholar] [CrossRef]
- López-Campos, J.L.; Ruiz-Ramos, M.; Soriano, J.B. Mortality Trends in Chronic Obstructive Pulmonary Disease in Europe, 1994–2010: A Joinpoint Regression Analysis. Lancet Respir. Med. 2014, 2, 54–62. [Google Scholar] [CrossRef]
- Strand, B.H.; Grøholt, E.K.; Steingrímsdóttir, O.A.; Blakely, T.; Graff-Lversen, S.; Naess, O. Educational Inequalities in Mortality over Four Decades in Norway: Prospective Study of Middle Aged Men and Women Followed for Cause Specific Mortality, 1960–2000. BMJ 2010, 340, C654. [Google Scholar] [CrossRef]
- Marí-Dell’Olmo, M.; Gotsens, M.; Palència, L.; Burström, B.; Corman, D.; Costa, G.; Deboosere, P.; Díez, È.; Domínguez-Berjón, F.; Dzúrová, D.; et al. Socioeconomic Inequalities in Cause-Specific Mortality in 15 European Cities. J. Epidemiol. Community Health 2015, 69, 432–441. [Google Scholar] [CrossRef]
- Cho, K.H; Nam, C.M; Lee, E.J; Choi, Y.; Yoo, K.B.; Lee, S.H.; Park, E.C. Effects of Individual and Neighborhood Socioeconomic Status on the Risk of All-Cause Mortality in Chronic Obstructive Pulmonary Disease: A Nationwide Population-Based Cohort Study, 2002–2013. Respir. Med. 2016, 114, 9–17. [Google Scholar] [CrossRef]
- Algren, M.H.; Ekholm, O.; Nielsen, L.; Ersbøll, A.K.; Bak, C.K.; Andersen, P.T. Associations between Perceived Stress, Socioeconomic Status, and Health-Risk Behaviour in Deprived Neighbourhoods in Denmark: A Cross-Sectional Study. BMC Public Health 2018, 18, 250. [Google Scholar] [CrossRef]
- Plug, I.; Hoffmann, R.; Artnik, B.; Bopp, M.; Borrell, C.; Costa, G.; Deboosere, P.; Esnaola, S.; Kalediene, R.; Leinsalu, M.; et al. Socioeconomic Inequalities in Mortality from Conditions Amenable to Medical Interventions: Do They Reflect Inequalities in Access or Quality of Health Care? BMC Public Health 2012, 12, 346. [Google Scholar] [CrossRef]
- Giannaros, D. Twenty Years After the Economic Restructuring of Eastern Europe: An Economic Review. Int. Bus. Econ. Res. J. 2008, 7, 35–38. [Google Scholar] [CrossRef]
- Wojtyniak, B.; Moskalewicz, J.; Stokwiszewski, J.; Rabczenko, D. Gender-Specific Mortality Associated with Alcohol Consumption in Poland in Transition. Addiction 2005, 100, 1779–1789. [Google Scholar] [CrossRef]
- Leinsalu, M.; Stirbu, I.; Vågerö, D.; Kalediene, R.; Kovács, K.; Wojtyniak, B.; Wróblewska, W.; Mackenbach, J.P.; Kunst, A.E. Educational Inequalities in Mortality in four Eastern European Countries: Divergence in Trends during the Post-Communist Transition from 1990 to 2000. Int. J. Epidemiol. 2009, 38, 512–525. [Google Scholar] [CrossRef]
- Golinowska, S.; Sowa, A.; Topór-Mądry, R.; et al. Health Status and Health Care Systems in Central & Eastern European Countries: Bulgaria, Estonia, Poland, Slovakia and Hungary. European Network of Economic Policy, Research Report no. 31, 2006; Eunropean Network of Economic Policy Research Institutes: Brussels, Belgien, 2006. [Google Scholar]
- European Commission: Regions in the European Union. Nomenclature of territorial units for statistics. NUTS 2006/EU-27. Available online: http://ec.europa.eu/eurostat/web/products-manuals-and-guidelines/-/KS-RA-07-020. (accessed on 17 September 2018).
- Diagnoza Społeczna 2011. Available online: www.diagnoza.com (accessed on 25 September 2018).
- Morris, J.A.; Gardner, M.J. Calculating Confidence Intervals for Relative Risks (Odds Ratios) and Standardized Ratios and Rates. BMJ 1988, 296, 1313–1316. [Google Scholar] [CrossRef]
- Chaberko, T.; Grad, N.; Kretowicz, P.; Łebek, S. Geographical Distribution of Poverty in Poland. Inst. Geogr. Gospod. Przestrz. UJ 2012, 43–54. [Google Scholar] [CrossRef]
- Hartigan, J.A.; Wong, M.A.A. K-Means Clustering Algorithm. Appl. Stat. 1979, 28, 100–108. [Google Scholar] [CrossRef]
- Gambaryan, M.H.; Shalnova, S.A.; Deev, A.D.; Drapkina, O.M. Chronic Respiratory Diseases in the Regions of Northern Russia: Epidemiological Distinctions in the Results of a National Population Study. Int. J. Environ. Res. Public Health 2017, 14, 841. [Google Scholar] [CrossRef]
- Reques, L.; Giráldez-García, C.; Miqueleiz, E.; Belza, M.J.; Regidor, E. Educational Differences in Mortality and the Relative Importance of Different Causes of Death: A 7-Year Follow-Up Study of Spanish Adults. J. Epidemiol. Community Health 2014, 68, 1151–1160. [Google Scholar] [CrossRef]
- Slachtová, H.; Tomásková, H.; Splíchalová, A.; Polaufová, P.; Fejtková, P. Czech Socio-Economic Deprivation Index and Its Correlation with Mortality Data. Int. J. Public Health 2009, 54, 267–273. [Google Scholar] [CrossRef]
- Barceló, M.A.; Saez, M.; Saurina, C. Spatial Variability in Mortality Inequalities, Socioeconomic Deprivation, and Air Pollution in Small Areas of the Barcelona Metropolitan Region, Spain. Sci. Total Environ. 2009, 407, 5501–5523. [Google Scholar] [CrossRef]
- Nolasco, A.; Melchor, I.; Pina, J.A.; Pereyra-Zamora, P.; Moncho, J.; Tamayo, N.; García-Senchermes, C.; Zurriaga, O.; Martínez-Beneito, M.A. Preventable Avoidable Mortality: Evolution of Socioeconomic Inequalities in Urban Areas in Spain, 1996–2003. Health Place 2009, 15, 702–711. [Google Scholar] [CrossRef]
- Sánchez-Santos, M.T.; Mesa-Frias, M.; Choi, M.; Nüesch, E.; Barco, A.A.-D.; Amuzu, A.; Smith, G.D.; Ebrahim, S.; Prieto-Merino, D.; Casas, J.P. Area-Level Deprivation and Overall and Cause-Specific Mortality: 12 Years’ Observation on British Women and Systematic Review of Prospective Studies. PLoS ONE 2013, 8, e72656. [Google Scholar] [CrossRef]
- Krzyżanowski, M.; Jedrychowski, W.; Wysocki, M. Factors Associated with the Change in Ventilatory Function and the Development of Chronic Obstructive Pulmonary Disease in a 13-Year Follow-Up of the Cracow Study. Am. Rev. Respir. Dis. 1986, 134, 1011–1019. [Google Scholar] [CrossRef]
- Lowe, K.E.; Make, B.J.; Crapo, J.D.; Kinney, G.L.; Hokanson, J.E.; Kim, V.; Iyer, A.S.; Bhatt, S.P.; Hoth, K.F.; Holm, K.E.; et al. Association of Low Income with Pulmonary Disease Progression in Smokers with and without Chronic Obstructive Pulmonary Disease. ERJ Open Res. 2018, 4, 00069-2008. [Google Scholar] [CrossRef]
- Zanobetti, A.; Bind, M.A.; Schwartz, J. Particulate Air Pollution and Survival in a COPD Cohort. Environ. Health 2008, 7, 48. [Google Scholar] [CrossRef] [PubMed]
- Thurston, G.D.; Ahn, J.; Cromar, K.R.; Shao, Y.; Reynolds, H.R.; Jerrett, M.; Lim, C.C.; Shanley, R.; Park, Y.; Hayes, R.B. Ambient Particulate Matter Air Pollution Exposure and Mortality in the NIH-AARP Diet and Health Cohort. Environ. Health Perspect. 2016, 124, 484–490. [Google Scholar] [CrossRef]
- Alicandro, G.; Frova, L.; Sebastiani, G.; Boffetta, P.; La Vecchia, C. Differences in Education and Premature Mortality: A Record Linkage Study of over 35 Million Italians. Eur. J. Public Health 2018, 28, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Jack, R.H.; Gulliford, M.C.; Ferguson, J.; Moller, H. Explaining Inequalities in Access to Treatment in Lung Cancer. J. Eval. Clin. Pract. 2006, 12, 573–582. [Google Scholar] [CrossRef]
- Polak, M.; Szafraniec, K.; Kozela, M.; Wolfshaut-Wolak, R.; Bobak, M.; Pająk, A. Socioeconomic Status and Pulmonary Function, Transition from Childhood to Adulthood: Cross-Sectional Results from the Polish Part of the HAPIEE Study. BMJ Open 2019, 9, e022638. [Google Scholar] [CrossRef]
- Kozela, M.; Pająk, A.; Micek, A.; Besala, A.; Kubinova, R.; Malyutina, S.; Tamosiunas, A.; Pikhart, H.; Peasey, A.; Nikitin, Y.; et al. Impact of Perceived Control on All-Cause and Cardiovascular Disease Mortality in Three Urban Populations of Central and Eastern Europe: the HAPIEE Study. J. Epidemiol. Community Health 2017, 71, 771–778. [Google Scholar] [CrossRef]
- Tillmann, T.; Pikhart, H.; Peasey, A.; Kubinova, R.; Pajak, A.; Tamosiunas, A.; Malyutina, S.; Steptoe, A.; Kivimäki, M.; Marmot, M.; et al. Psychosocial and Socioeconomic Determinants of Cardiovascular Mortality in Eastern Europe: A Multicentre Prospective Cohort Study. PLoS Med. 2017, 14, e1002459. [Google Scholar] [CrossRef]
- Galobardes, B.; Lynch, J.; Smith, G.D. Measuring Socioeconomic Position in Health Research. Br. Med. Bull. 2007, 81, 1–17. [Google Scholar] [CrossRef]
- Singh, G.K.; Siahpush, M. Increasing Inequalities in All-Cause and Cardiovascular Mortality among US Adults Aged 25–64 Years by Area Socioeconomic Status, 1969–1998. Int. J. Epidemiol. 2002, 31, 600–613. [Google Scholar] [CrossRef]
- Fukuda, Y.; Nakamura, K.; Takano, T. Municipal Socioeconomic Status and Mortality in Japan: Sex and Age Differences, and Trends in 1973–1998. Soc. Sci. Med. 2004, 59, 2435–2445. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Age Group (Years) | Respiratory Diseases (J00-99) | Lung Cancer (C33-34) | ||||
|---|---|---|---|---|---|---|
| Mean SMRs | Min–Max | CV (%) | Mean SMRs | Min–Max | CV (%) | |
| men | ||||||
| ≥15 | 72.4 | 36–110 | 22 | 101 | 70–215 | 20 |
| 25–64 | 23.7 | 15–41 | 25 | 58.1 | 37–89 | 16 |
| ≥65 | 442.2 | 207–662 | 23 | 466.6 | 347–661 | 14 |
| women | ||||||
| ≥15 | 46 | 26–77 | 22 | 36.3 | 18–53 | 25 |
| 25–64 | 9.6 | 5–16 | 25 | 26.7 | 14–41 | 24 |
| ≥65 | 207.7 | 100–357 | 30 | 103.9 | 51–173 | 29 |
| Age Group (Years) | Model | Men | Women | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Respiratory Diseases (J00−J99) | Lung Cancer (C33−34) | Respiratory Diseases (J00−J99) | Lung Cancer (C33−34) | ||||||||||
| β | 95% WCI | p | β | 95% WCI | p | β | 95% WCI | p | β | 95% WCI | p | ||
| ≥15 | A | −5.8 | (−10.23; −1.40) | 0.01 | −7.4 | (−13.06; −1.70) | 0.012 | 2.8 | (−1.04; 6.55) | 0.15 | 3.3 | (0.70; 5.90) | 0.01 |
| B | −5.2 | (−9.6; −0.79) | 0.02 | −6.8 | (−12.58; −1.10) | 0.02 | 0.5 | (−3.62; 4.68) | 0.80 | −0.4 | (−2.60; 1.72) | 0.69 | |
| C | −2.0 | (−6.63; 2.63) | 0.39 | −5.2 | (−11.64; 1.19) | 0.109 | 3.0 | (−1.40; 7.39) | 0.18 | −0.1 | (−2.51; 2.29) | 0.93 | |
| 25–64 | A | −0.6 | (−2.34; 1.10) | 0.47 | −4.2 | (−6.8; −1.62) | 0.002 | 0.1 | (−0.59; 0.84) | 0.73 | 0.04 | (−1.87; 1.96) | 0.96 |
| B | −0.2 | (−1.86; 1.42) | 0.79 | −3.7 | (−6.2; −1.17) | 0.005 | −0.4 | (−1.19; 0.32) | 0.25 | −2.5 | (−4.19; −0.86) | 0.004 | |
| C | 0.1 | (−1.75; 1.93) | 0.92 | −3.3 | (−6.13; −0.47) | 0.023 | −0.4 | (−1.20; 0.47) | 0.39 | −2.5 | (−4.35; −0.63) | 0.01 | |
| ≥65 | A | −42.9 | (−71.71; −14.24) | 0.004 | −34.3 | (−52.27; −16.36) | <0.001 | 14.1 | (−4.26; 32.44) | 0.13 | 9.6 | (−2.34; 21.58) | 0.21 |
| B | −40.4 | (−69.44; −11.31) | 0.007 | −31.1 | (−48.80; −13.49) | 0.001 | −6.6 | (−29.80; 16.78) | 0.68 | −5.2 | (−12.74; 1.18) | 0.31 | |
| C | −16.8 | (−46.83; 13.15) | 0.27 | −27.7 | (−47.53; −7.86) | 0.007 | −3.6 | (−18.95; 11.75) | 0.80 | −3.7 | (−11.26; 3.85) | 0.49 | |
| Age Group (Years) | Model | Men | Women | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Respiratory Diseases (J00−J99) | Lung Cancer (C33−34) | Respiratory Diseases (J00−J99) | Lung Cancer (C33−34) | ||||||||||
| β | 95% WCI | p | β | 95% WCI | p | β | 95% WCI | p | β | 95% WCI | p | ||
| ≥15 | A | −29.7 | (−58.96; −0.33) | 0.048 | 0.8 | (−38.04; 39.67) | 0.97 | −20.4 | (−44.96; 4.19) | 0.10 | 12.1 | (−5.42; 29.59) | 0.17 |
| B | −29.3 | (−57.84; −0.71) | 0.045 | 1.2 | (−37.32; 39.67) | 0.92 | −30.5 | (−53.94; −6.98) | 0.012 | −0.7 | (−13.59; 12.15) | 0.91 | |
| C | −29.1 | (−54.75; −3.39) | 0.027 | 1.3 | (−36.26; 38.92) | 0.94 | −31.5 | (−54.1; −8.84) | 0.007 | −0.9 | (−13.82; 12.03) | 0.89 | |
| 25–64 | A | −2.0 | (−13.20; 9.26) | 0.727 | −4.3 | (−22.48; 13.84) | 0.64 | 0.6 | (−4.04; 5.25) | 0.79 | 9.4 | (−2.8; 21.62) | 0.13 |
| B | −1.8 | (−12.29; 8.76) | 0.738 | −4.0 | (−21.19; 13.17) | 0.64 | −1.1 | (−5.62; 3.42) | 0.63 | 2.5 | (−8.14; 13.08) | 0.64 | |
| C | −1.8 | (−12.31; 8.81) | 0.742 | −4.0 | (−20.85; 12.95) | 0.64 | −1.2 | (−5.70; 3.36) | 0.61 | 2.2 | (−8.35; 12.79) | 0.68 | |
| ≥65 | A | −226.6 | (−418.05; −35.23) | 0.021 | 19.2 | (−110.23; 148.55) | 0.77 | −109.1 | (−227.59; 9.40) | 0.07 | 31.4 | (−27.02; 89.83) | 0.29 |
| B | −224.8 | (−414.37; −35.32) | 0.021 | 21.2 | (−102.83; 145.14) | 0.73 | −156.0 | (−269.96; −42.08) | 0.008 | −12.0 | (−54.24; 30.17) | 0.57 | |
| C | −223.3 | (−387.66; −58.98) | 0.009 | 21.7 | (−98.96; 142.3) | 0.72 | −161.1 | (−270.55; −51.57) | 0.005 | −12.2 | (−54.75; 30.4) | 0.57 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polak, M.; Genowska, A.; Szafraniec, K.; Fryc, J.; Jamiołkowski, J.; Pająk, A. Area-Based Socio-Economic Inequalities in Mortality from Lung Cancer and Respiratory Diseases. Int. J. Environ. Res. Public Health 2019, 16, 1791. https://doi.org/10.3390/ijerph16101791
Polak M, Genowska A, Szafraniec K, Fryc J, Jamiołkowski J, Pająk A. Area-Based Socio-Economic Inequalities in Mortality from Lung Cancer and Respiratory Diseases. International Journal of Environmental Research and Public Health. 2019; 16(10):1791. https://doi.org/10.3390/ijerph16101791
Chicago/Turabian StylePolak, Maciej, Agnieszka Genowska, Krystyna Szafraniec, Justyna Fryc, Jacek Jamiołkowski, and Andrzej Pająk. 2019. "Area-Based Socio-Economic Inequalities in Mortality from Lung Cancer and Respiratory Diseases" International Journal of Environmental Research and Public Health 16, no. 10: 1791. https://doi.org/10.3390/ijerph16101791
APA StylePolak, M., Genowska, A., Szafraniec, K., Fryc, J., Jamiołkowski, J., & Pająk, A. (2019). Area-Based Socio-Economic Inequalities in Mortality from Lung Cancer and Respiratory Diseases. International Journal of Environmental Research and Public Health, 16(10), 1791. https://doi.org/10.3390/ijerph16101791