Comparison of Growth Curve Estimates of Infants in São Tomé Island, Africa, with the WHO Growth Standards: A Birth Cohort Study


Abstract
:1. Introduction
1.1. Growth in Lower Middle Income Countries
1.2. WHO Standards
1.3. Objective
2. Materials and Methods
2.1. Study Design and Setting
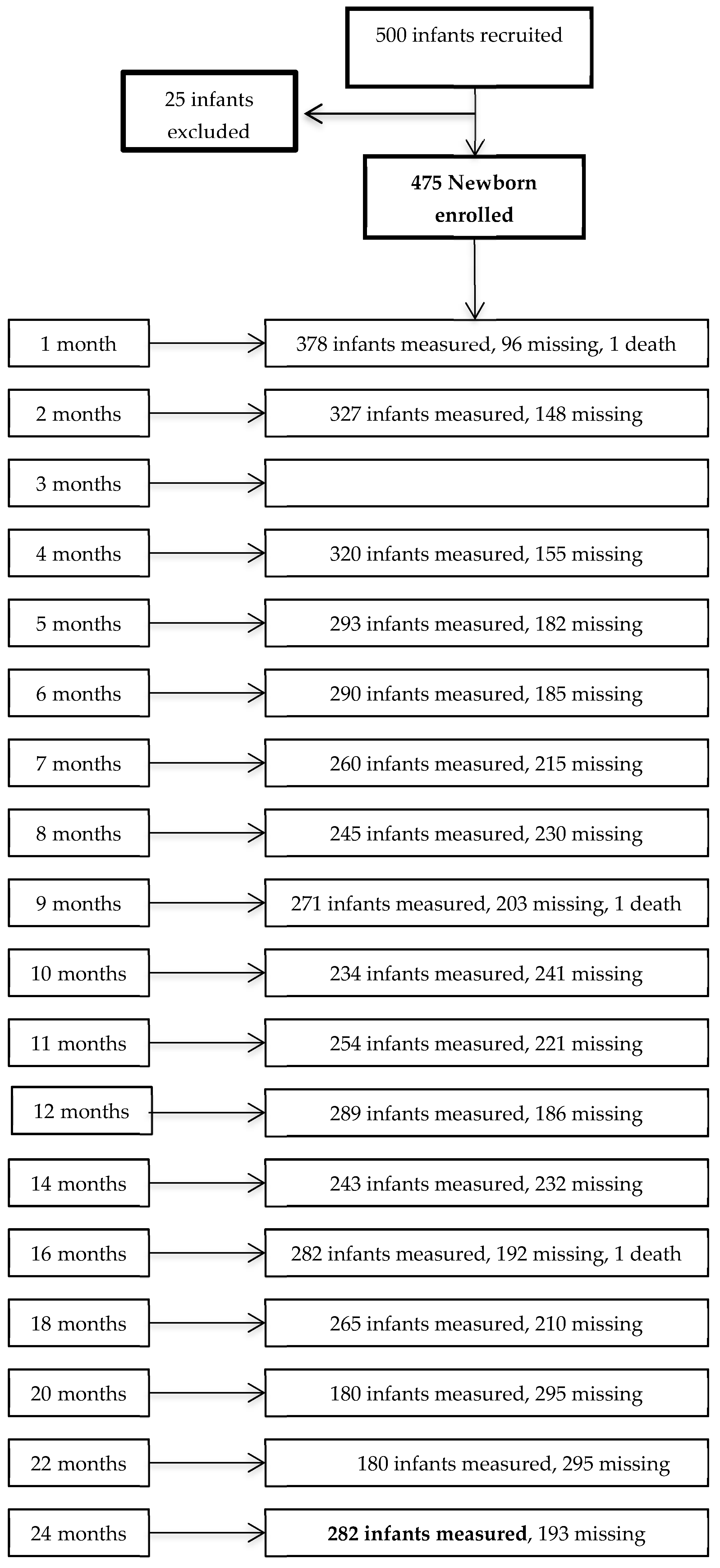
2.2. Birth Cohort and Anthropometry
2.3. Statistical Methods
- BCPE (λ = 0.35, df(µ) = 7, df(σ) = 2, ν = 1, τ = 2) for boys
- BCPE (λ = 0.35, df(µ) = 7, df(σ) = 2, ν = 1, τ = 2) for girls
- BCPE (λ = 0.35, df(µ) = 8, df(σ) = 2, df(ν) = 2) for boys
- BCPE (λ = 0.10, df(µ) = 8, df(σ) = 2) for girls
- BCPE (df(µ) = 6, df(σ) = 1, df(ν) = 1, τ = 2) for boys
- BCPE (df(µ) = 5, df(σ) = 3, df(ν) = 1, τ = 2) for girls
- BCPE (λ = 0.30, df(µ) = 7, df(σ) = 2) for boys
- BCPE (λ = 0.31, df(µ) = 8, df(σ) = 2) for girls
- BCPE (λ = 0.64, df(µ) = 5, df(σ) = 2, df(τ) = 1) for boys
- BCPE (λ = 0.09, df(µ) = 7, df(σ) = 3, ν = 1, τ = 2) for girls
- BCPE (λ = 0.05, df(µ) = 12, df(σ) = 6, df(ν) = 3, τ = 2) for boys
- BCPE (λ = 0.05, df(µ) = 12, df(σ) = 5, df(ν) = 4, τ = 2) for girls
- BCPE (λ = 0.05, df(µ) = 9, df(σ) = 7, df(ν) = 1, τ = 2) for boys
- BCPE (λ = 0.05, df(µ) = 10, df(σ) = 7, df(ν) = 1, τ = 2) for girls
3. Results
3.1. Factors Affecting Growth
3.1.1. Socioeconomic Status and Feeding Practices
3.1.2. Morbidity
3.2. Abthropometry
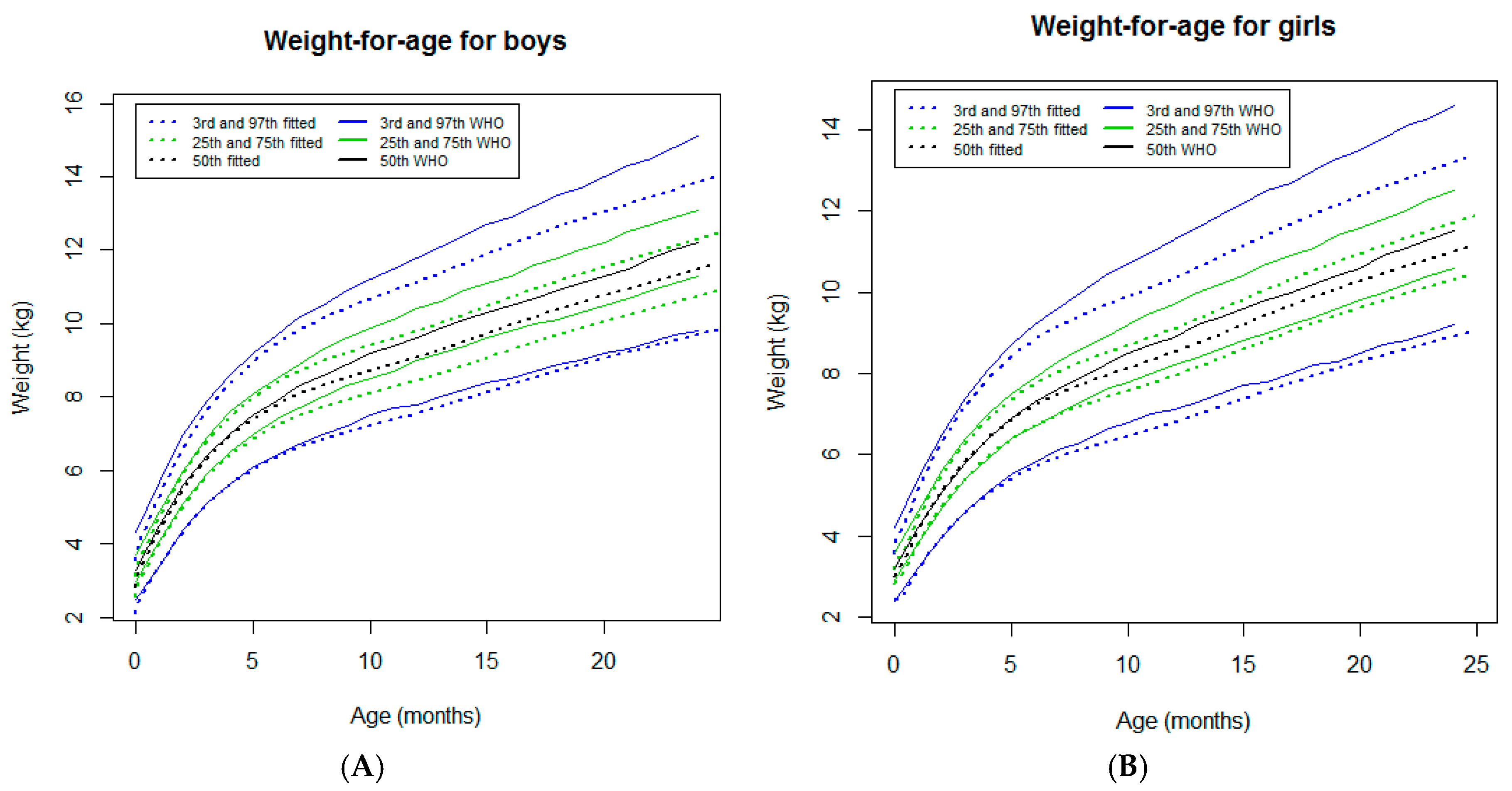
3.2.1. Weight-for-Age
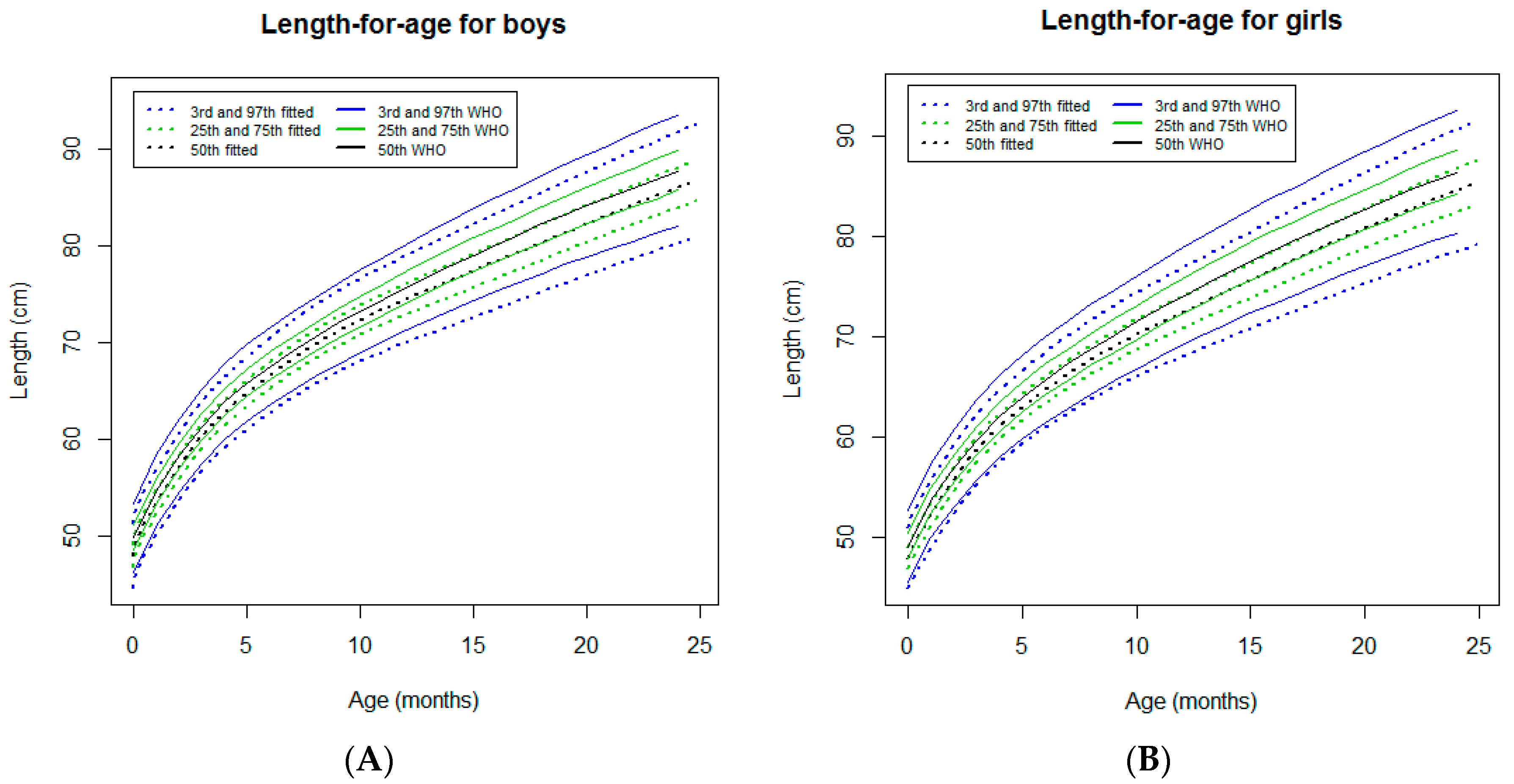
3.2.2. Length-for-Age
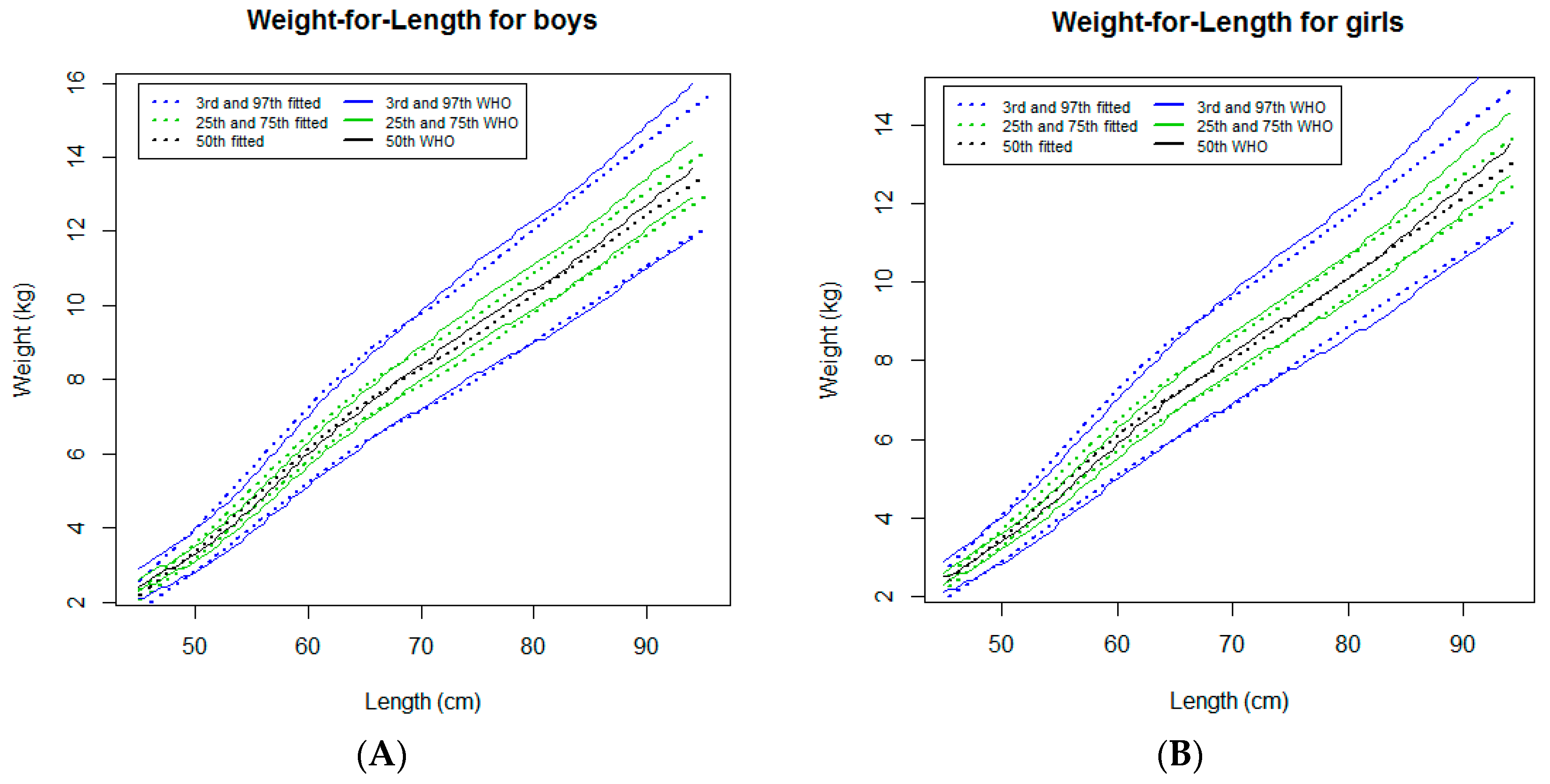
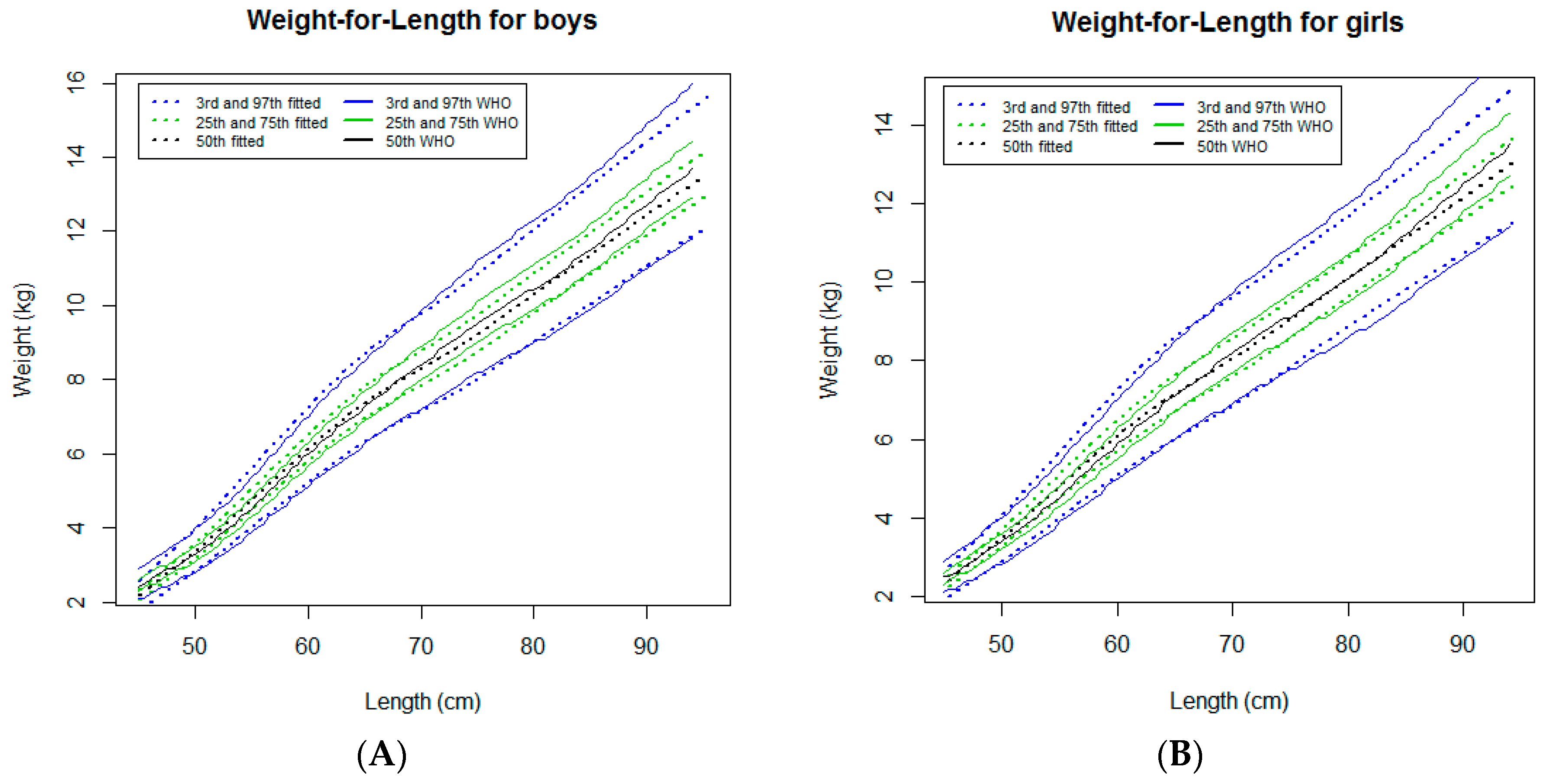
3.2.3. Weight-for-Length
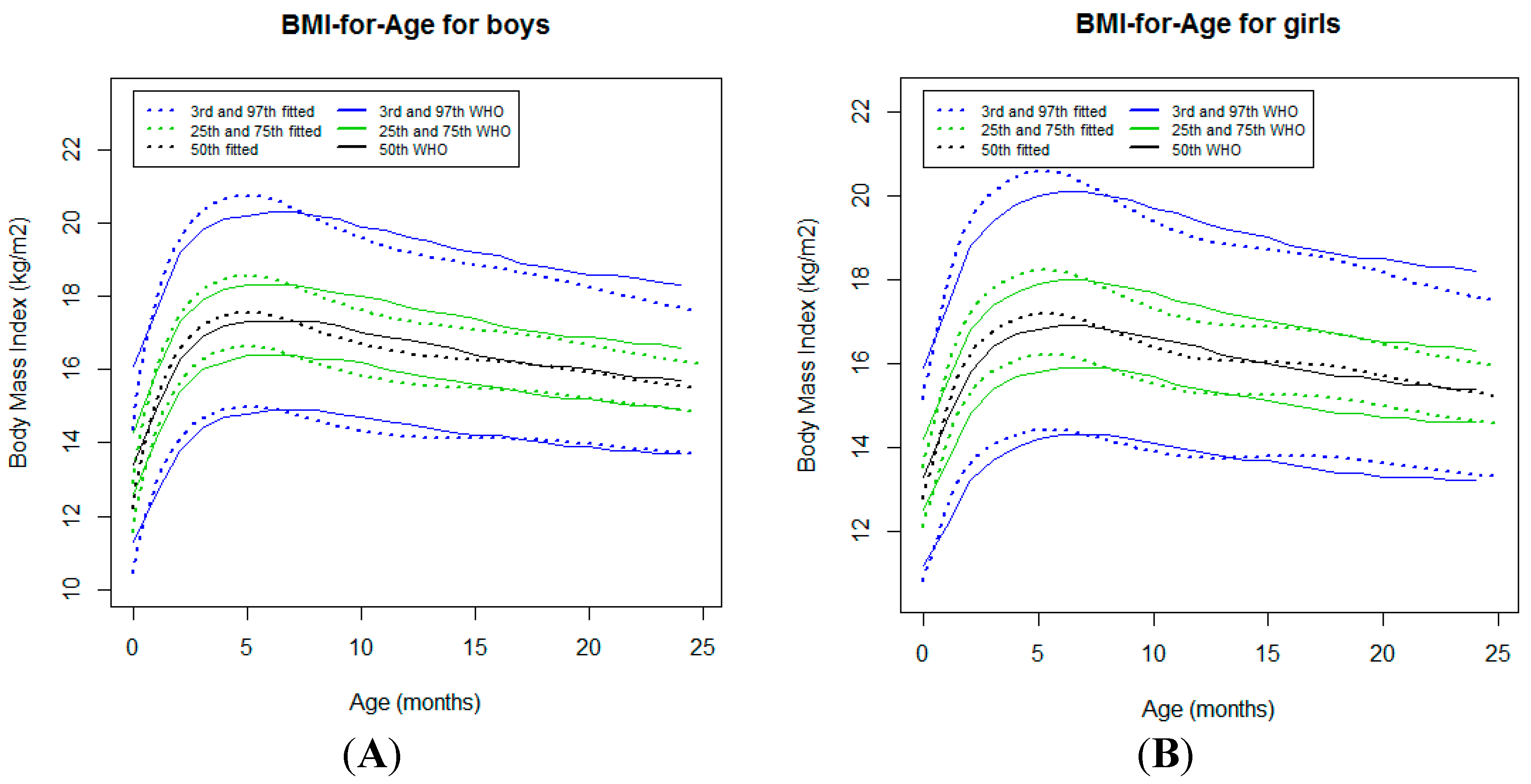
3.2.4. Body Mass Index-for-Age
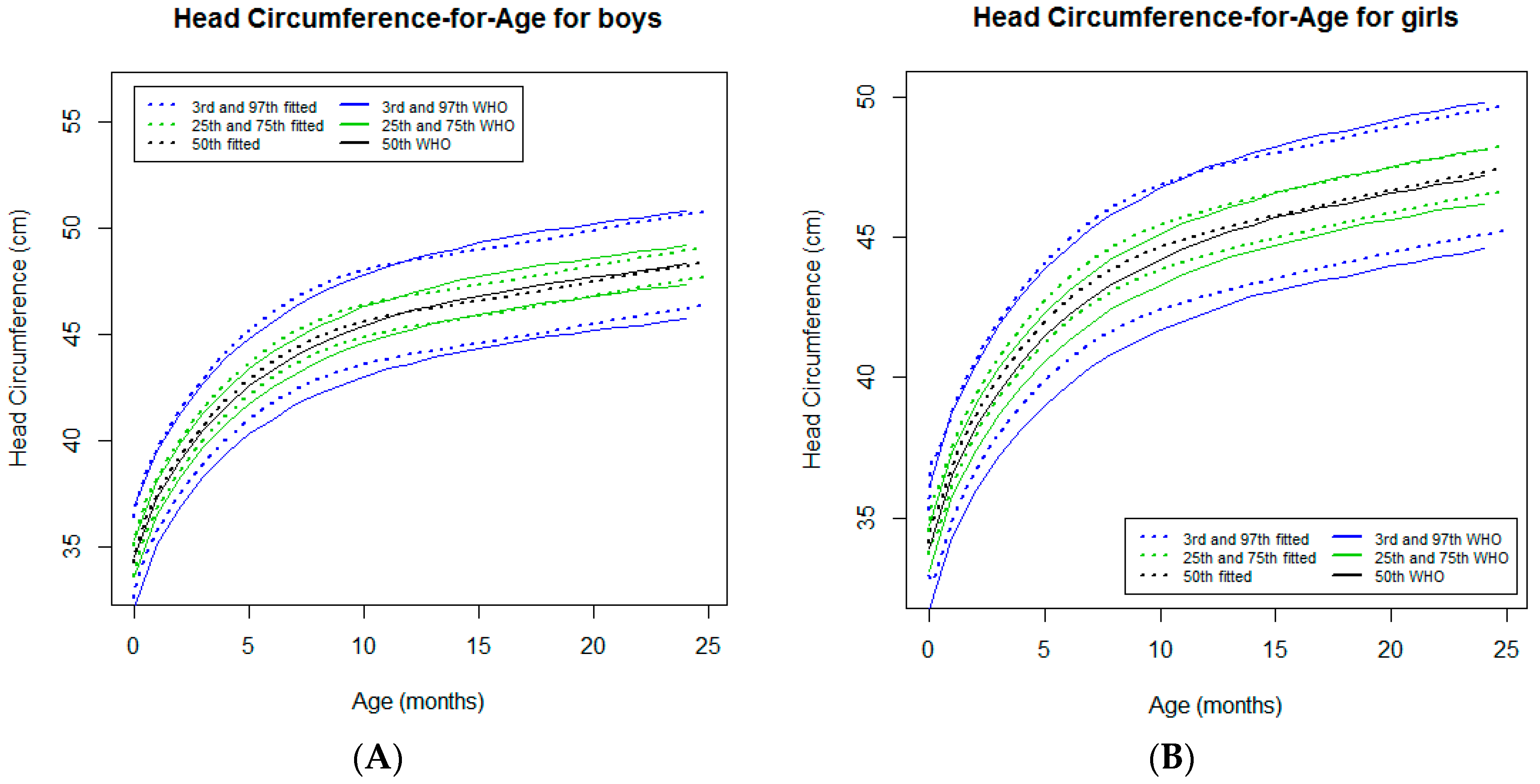
3.2.5. Head Circumference-for-Age
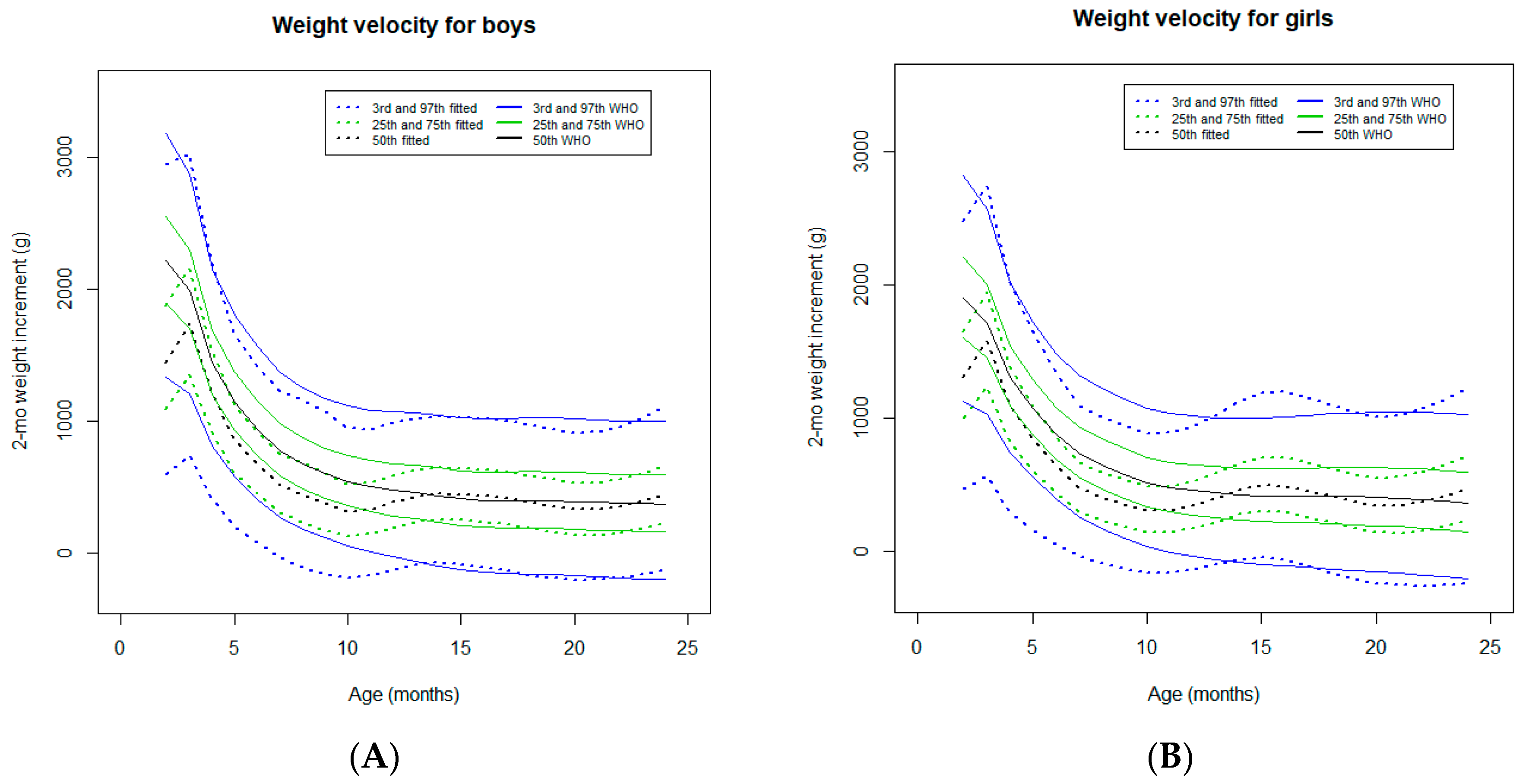
3.2.6. Two-Month Weight Velocity
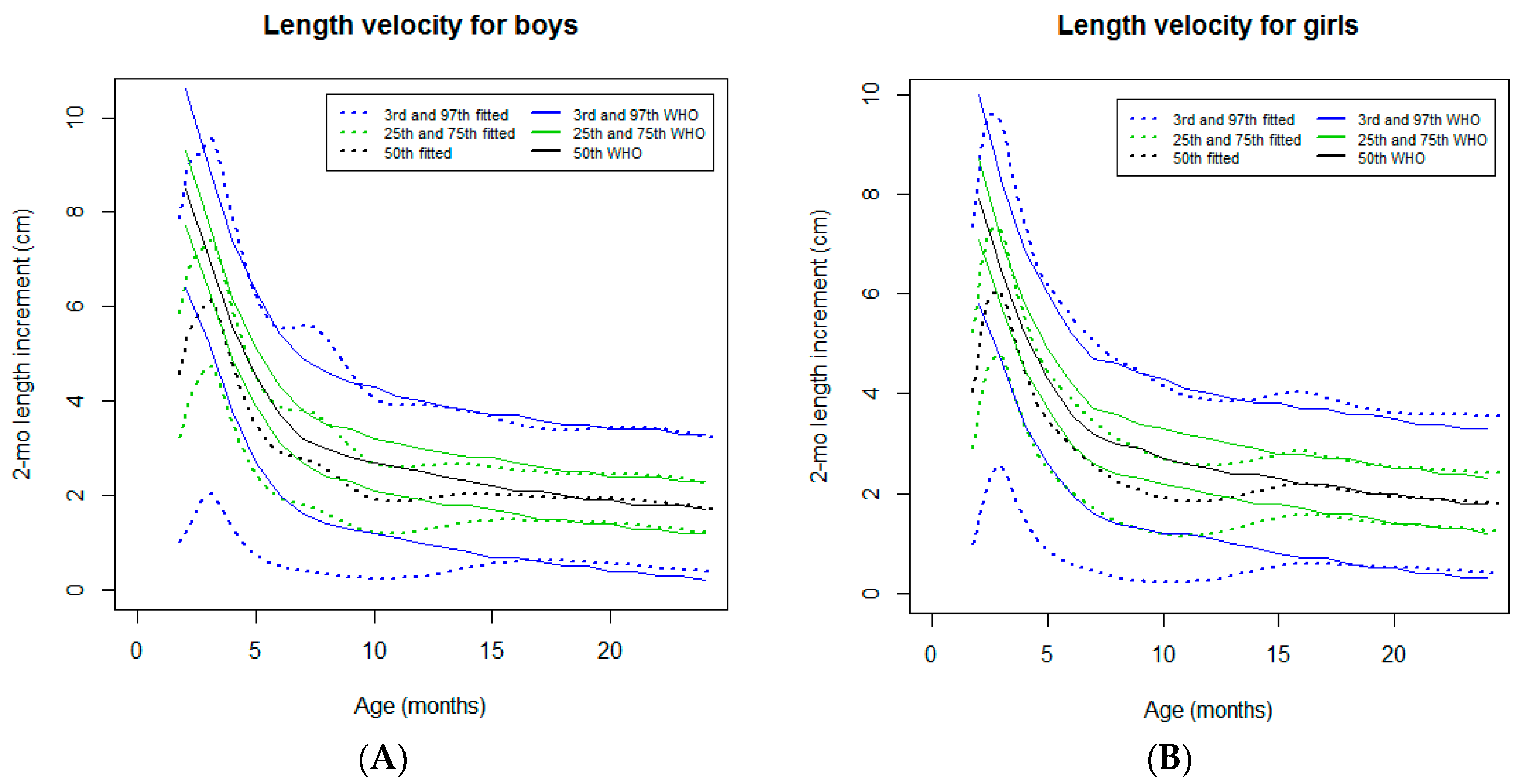
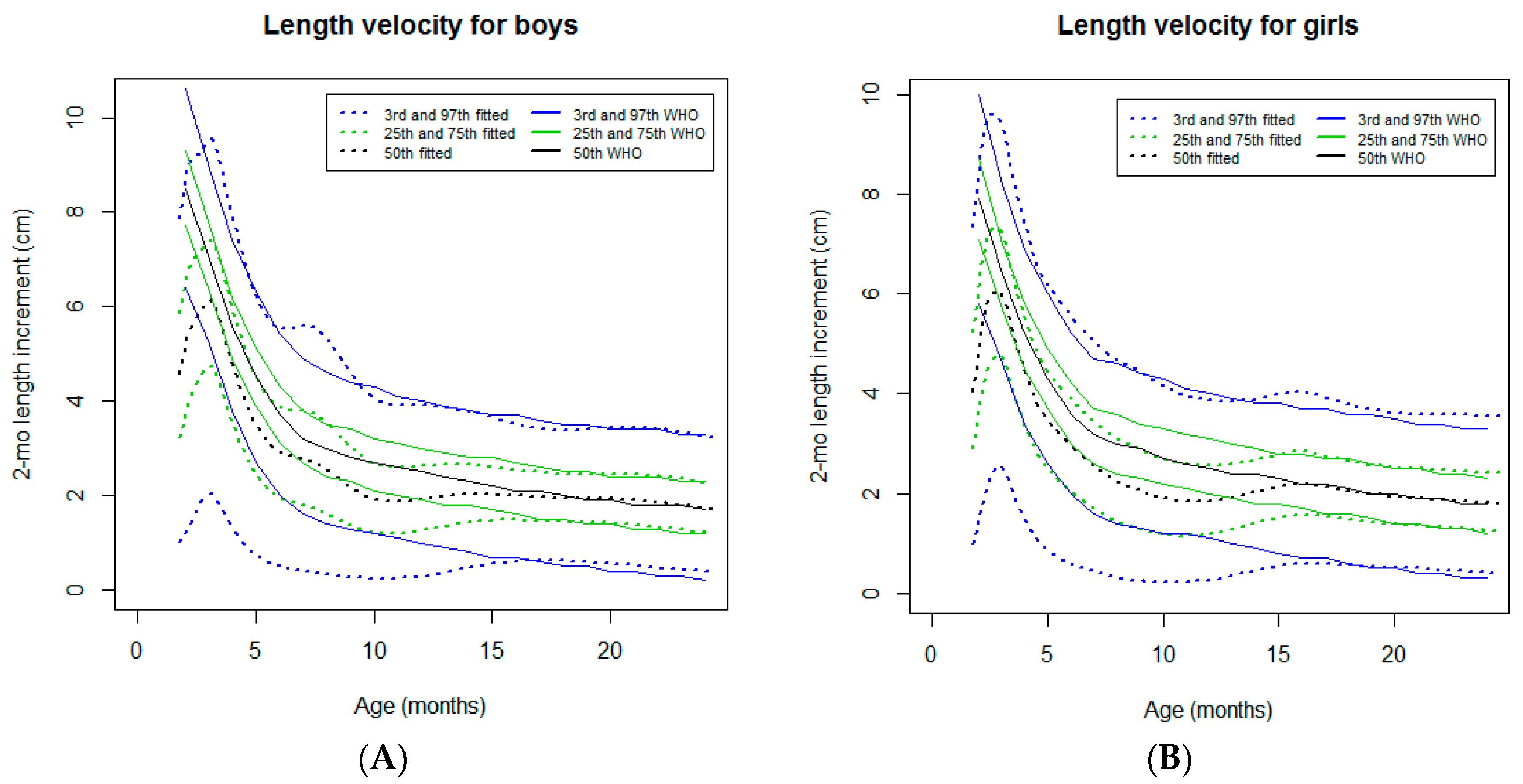
3.2.7. Two-Month Length Velocity
4. Discussion
4.1. Cohort Study Specificities
4.2. Body Weight Curves
4.3. Linear Growth
4.4. Head Growth
4.5. Limitations
4.6. Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chowa, G.; Ansong, D.; Masa, R. Assets and child well-being in developing countries: A research review. Child. Youth Serv. Rev. 2010, 32, 1508–1519. [Google Scholar] [CrossRef]
- Victora, C.G.; de Onis, M.; Hallal, P.C.; Blossner, M.; Shrimpton, R. Worldwide timing of growth faltering: Revisiting implications for interventions. Pediatrics 2010, 125, e473–e480. [Google Scholar] [CrossRef] [PubMed]
- Danaei, G.; Andrews, K.G.; Sudfeld, C.R.; Fink, G.; McCoy, D.C.; Peet, E.; Sania, A.; Fawzi, M.C.S.; Ezzati, M. Risk Factors for Childhood Stunting in 137 Developing Countries: A Comparative Risk Assessment Analysis at Global, Regional, and Country Levels. PLoS Med. 2016, 13, 1002164. [Google Scholar] [CrossRef] [PubMed]
- Garzón, M.; Pereira-da-Silva, L.; Seixas, J.; Papoila, A.L.; Alves, M. Subclinical enteric parasitic infections and growth faltering in infants in São Tomé, Africa: A birth cohort study. Int. J. Environ. Res. Public Health 2018, 15, 688. [Google Scholar] [CrossRef] [PubMed]
- Alkire, S.; Santos, M.E. Acute Multidimensional Poverty: A New Index for Developing Countries; Working Papers 38; University of Oxford: Oxford, UK, 2010; ISBN 978-1-907194-22-1. [Google Scholar]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2006; Available online: https://www.who.int/childgrowth/standards/technical_report/en/ (accessed on 3 March 2019).
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. Suppl. 2006, 450, 76–85. [Google Scholar]
- de Onis, M.; Garza, C.; Onyango, A.W.; Rolland-Cachera, M.F. WHO growth standards for infants and young children [French]. Arch. Pediatr. 2009, 16, 47–53. [Google Scholar] [CrossRef] [PubMed]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Garza, C.; Yang, H. Comparison of the World Health Organization (WHO) Child Growth Standards and the National Center for Health Statistics/WHO international growth reference: Implications for child health programmes. Public Health Nutr. 2006, 9, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Zorlu, G. New WHO child growth standards catch on. Bull. World Health Organ. 2011, 89, 250–251. [Google Scholar] [PubMed]
- Garzón, M.; Pereira-Da-Silva, L.; Seixas, J.; Papoila, A.L.; Alves, M.; Ferreira, F.; Reis, A. Association of enteric parasitic infections with intestinal inflammation and permeability in asymptomatic infants of São Tomé Island. Pathog. Health 2017, 111, 116–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A.C.; Katz, J.; Blencowe, H.; Cousens, S.; Kozuki, N.; Vogel, J.P.; Adair, L.; Baqui, A.H.; Bhutta, Z.A.; Caulfield, L.E.; et al. National and regional estimates of term and preterm babies born small for gestational age in 138 low-income and middle-income countries in 2010. Lancet Glob. Health 2013, 1, e26–e36. [Google Scholar] [CrossRef] [Green Version]
- Stasinopoulos, D.M.; Rigby, R.A.; Heller, G.; Voudouris, V. Flexible Regression and Smoothing: Using GAMLSS; Chapman and Hall/CRC Press: New York, NY, USA, 2017; ISBN 9781138197909. [Google Scholar]
- Cole, T.J.; Green, P.J. Smoothing reference centile curves: The LMS method and penalized likelihood. Stat. Med. 1992, 11, 1305–1319. [Google Scholar] [CrossRef] [PubMed]
- Rigby, R.A.; Stasinopoulos, D.M. Smooth centile curves for skew and kurtotic data modeled using the Box-Cox power exponential distribution. Stat. Med. 2004, 23, 3053–3076. [Google Scholar] [CrossRef] [PubMed]
- Rigby, R.A.; Stasinopoulos, D.M. Box-Cox t Distribution for Modeling Skew and Leptokurtotic Data. Technical Report 01/04; STORM Research Centre, London Metropolitan University: London, OH, USA, 2004. [Google Scholar]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards. Growth Velocity Based on Weight, Length and Head Circumference. Methods and Development; World Health Organization: Geneva, Switzerland, 2009; Available online: https://apps.who.int/iris/handle/10665/44026 (accessed on 3 March 2019).
- World Health Organization. Preventive Chemotherapy in Human Helminthiasis: Coordinated Use of Anthelminthic Drugs in Control Interventions: A Manual for Health Professionals and Programme Managers; World Health Organization: Geneva, Switzerland, 2006; Available online: http://apps.who.int/iris/bitstream/10665/43545/1/9241547103_eng.pdf (accessed on 3 March 2019).
- American Academy of Pediatrics. Giardia intestinalis (formerly Giardia lamblia and Giardia duodenalis) infections. In Red Book: Northwest Point Blvd; Kimberlin, D.W., Brady, M.T., Jackson, M.A., Long, S.S., Eds.; American Academy of Pediatrics: Itasca, IL, USA, 2015; 334p, ISBN 978-1-58110-926-9. [Google Scholar]
- McCambridge, J.; Witton, J.; Elbourne, D.R. Systematic review of the Hawthorne effect: New concepts are needed to study research participation effects. J. Clin. Epidemiol. 2014, 67, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Short-Term Effects of Breastfeeding; World Health Organization: Geneva, Switzerland, 2013; Available online: https://apps.who.int/iris/handle/10665/95585 (accessed on 3 March 2019).
- Osmani, S.; Sen, A. The hidden penalties of gender inequality: Fetal origins of ill-health. Econ. Hum. Biol. 2003, 1, 105–121. [Google Scholar] [CrossRef]
- Schwinger, C.; Fadnes, L.T.; Shrestha, S.K.; Shrestha, P.S.; Chandyo, R.K.; Shrestha, B.; Ulak, M.; Bodhidatta, L.; Mason, C.; Strand, T.A. Predicting Undernutrition at Age 2 Years with Early Attained Weight and Length Compared with Weight and Length Velocity. J. Pediatr. 2017, 182, 127–132.e1. [Google Scholar] [CrossRef] [PubMed]
- Martorell, R.; Zongrone, A. Intergenerational influences on child growth and undernutrition. Paediatr. Perinat. Epidemiol. 2012, 26, 302–314. [Google Scholar] [CrossRef] [PubMed]
- Özaltin, E.; Hill, K.; Subramanian, S.V. Association of maternal stature with offspring mortality, underweight, and stunting in low- to middle-income countries. JAMA 2010, 303, 1507–1516. [Google Scholar] [CrossRef] [PubMed]
- Deaton, A. Height, health, and development. Proc. Natl. Acad. Sci. USA 2007, 104, 13232–13237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Addo, O.Y.; Stein, A.D.; Fall, C.H.; Gigante, D.P.; Guntupalli, A.M.; Horta, B.L.; Kuzawa, C.W.; Lee, N.; Norris, S.A.; Prabhakaran, P.; et al. Maternal Height and Child Growth Patterns. J. Pediatr. 2013, 163, 549–554.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | 3rd | 25th | 50th | 75th | 97th | |
|---|---|---|---|---|---|---|
| Weight-for-age (kg) | Boys | 0.1 | 0.5 | 0.7 | 0.8 | 1.2 |
| Girls | 0.3 | 0.3 | 0.5 | 0.8 | 1.4 | |
| Length-for-age (cm) | Boys | 1.8 | 1.8 | 1.7 | 1.7 | 1.7 |
| Girls | 1.8 | 1.8 | 1.8 | 1.8 | 1.8 | |
| Weight-for-length (kg/cm) | Boys | −0.4 | −0.1 | 0.1 | 0.2 | 0.3 |
| Girls | −0.4 | 0 | 0.2 | 0.4 | 0.8 | |
| BMI-for-age (kg/m2) | Boys | 0 | 0 | 0.2 | 0.4 | 0.6 |
| Girls | −0.2 | 0 | 0.1 | 0.3 | 0.6 | |
| HC-for-age (cm) | Boys | −0.5 | −0.3 | 0.1 | 0.3 | 0.2 |
| Girls | −0.5 | −0.3 | −0.1 | 0 | 0.2 |
| At Neonatal Period | At 6 Months | At 12 Months | At 24 Months | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Sex | Above 90th (%) | Below 10th (%) | Above 90th (%) | Below 10th (%) | Above 90th (%) | Below 10th (%) | Above 90th (%) | Below 10th (%) | |
| Weight-for-age (kg) | Boys | 14.12 | 10.73 | 9.59 | 8.90 | 4.79 | 22.60 | 3.60 | 14.39 |
| Girls | 13.89 | 7.78 | 8.22 | 16.44 | 27.59 | 17.24 | 1.41 | 13.38 | |
| Length-for-age (cm) | Boys | 17.51 | 4.52 | 2.07 | 14.48 | 4.11 | 21.23 | 3.65 | 18.98 |
| Girls | 16.67 | 5.56 | 2.05 | 13.01 | 2.78 | 20.14 | 3.52 | 22.54 | |
| BMI-for-age (kg/m2) | Boys | 9.04 | 2.82 | 13.79 | 5.52 | 6.16 | 14.38 | 5.84 | 8.03 |
| Girls | 10.0 | 7.22 | 14.38 | 9.59 | 5.56 | 11.81 | 4.93 | 7.75 | |
| HC-for-age (cm) | Boys | 40.68 | 0 | 18.49 | 2.74 | 5.48 | 7.53 | 5.04 | 4.32 |
| Girls | 38.33 | 0 | 16.44 | 2.05 | 12.41 | 3.45 | 5.63 | 4.23 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garzón, M.; Papoila, A.L.; Alves, M.; Pereira-da-Silva, L. Comparison of Growth Curve Estimates of Infants in São Tomé Island, Africa, with the WHO Growth Standards: A Birth Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 1693. https://doi.org/10.3390/ijerph16101693
Garzón M, Papoila AL, Alves M, Pereira-da-Silva L. Comparison of Growth Curve Estimates of Infants in São Tomé Island, Africa, with the WHO Growth Standards: A Birth Cohort Study. International Journal of Environmental Research and Public Health. 2019; 16(10):1693. https://doi.org/10.3390/ijerph16101693
Chicago/Turabian StyleGarzón, Marisol, Ana Luísa Papoila, Marta Alves, and Luís Pereira-da-Silva. 2019. "Comparison of Growth Curve Estimates of Infants in São Tomé Island, Africa, with the WHO Growth Standards: A Birth Cohort Study" International Journal of Environmental Research and Public Health 16, no. 10: 1693. https://doi.org/10.3390/ijerph16101693