Geographic Variations in the Risk of Emergency First Dialysis for Patients with End Stage Renal Disease in the Bretagne Region, France


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Population
2.3. Data Collection
2.4. Patient-Level Factors
2.5. Municipality-Level Factors
2.5.1. Socio-Demographic Variables
2.5.2. Degree of Urbanization
2.5.3. Potential Healthcare Offer
2.6. Analysis
2.6.1. Spatial Analysis
2.6.2. Statistical Analysis
3. Results
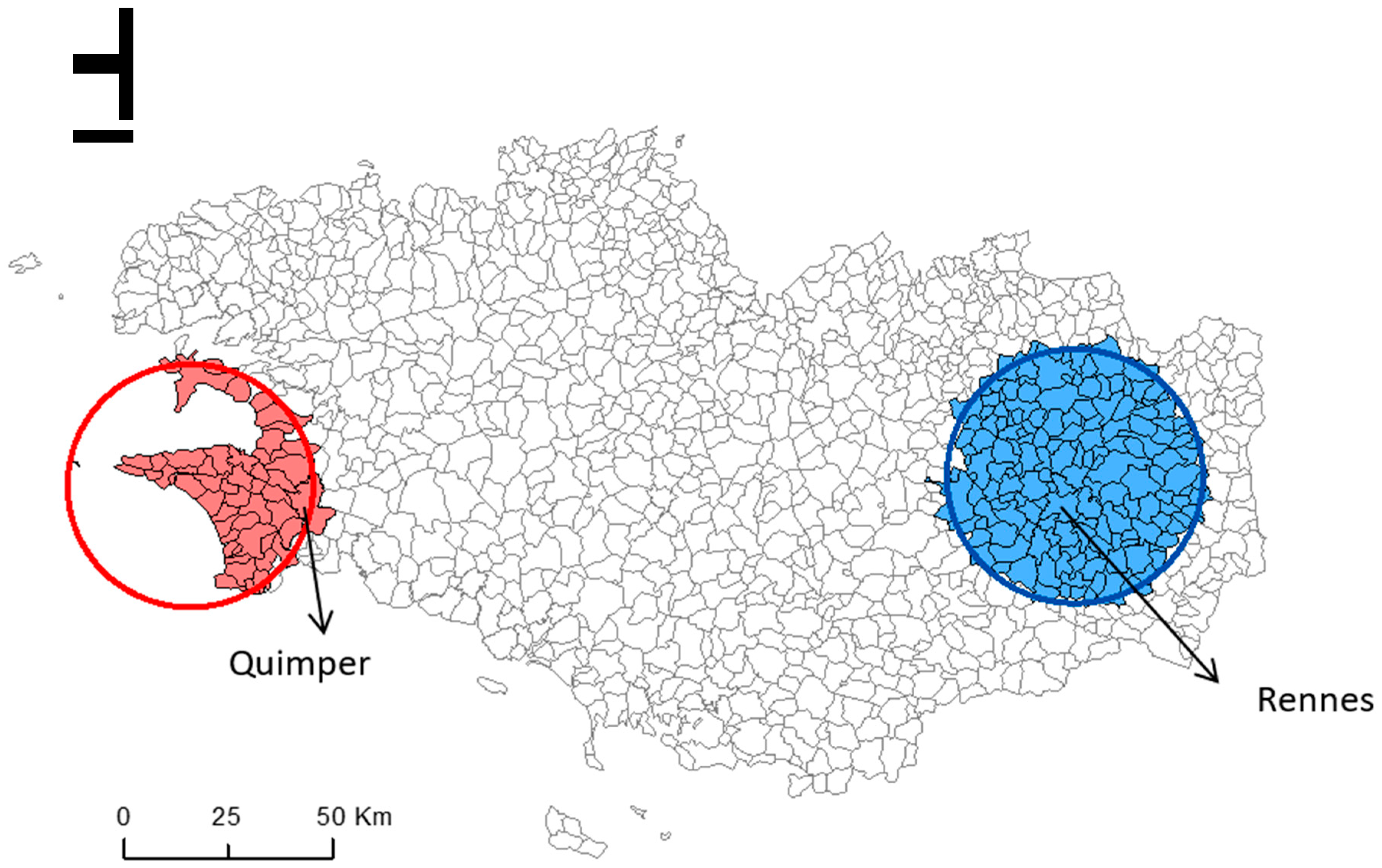
3.1. Geographic Variations
3.2. Comparison of the Higher- and Lower-Risk Clusters
3.2.1. Patient-Level Factors
3.2.2. Municipality-Level Factors
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ESRD | End Stage Renal Disease |
| CKD | Chronic Kidney Disease |
| RRT | Renal Replacement Therapy |
| RR | Relative Risk |
| BMI | Body Mass Index |
| INSEE | National Institute of Statistics and Economic Studies |
| REIN | Réseau Epidémiologie et Information en Néphrologie |
References
- Pippias, M.; Jager, K.J.; Kramer, A.; Leivestad, T.; Sánchez, M.B.; Caskey, F.J.; Collart, F.; Couchoud, C.; Dekker, F.W.; Finne, P.; et al. The changing trends and outcomes in renal replacement therapy: Data from the ERA-EDTA Registry. Nephrol. Dial. Transpl. 2016, 31, 831–841. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.M.; Akizawa, T.; Jager, K.J.; Kerr, P.G.; Saran, R.; Pisoni, R.L. Factors affecting outcomes in patients reaching end-stage kidney disease worldwide: Differences in access to renal replacement therapy, modality use, and haemodialysis practices. Lancet 2016, 388, 294–306. [Google Scholar] [CrossRef]
- Collins, A.J.; Foley, R.N.; Gilbertson, D.T.; Chen, S.-C. United States Renal Data System public health surveillance of chronic kidney disease and end-stage renal disease. Kidney Int. Suppl. 2015, 5, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Vigneau, C.; Kolko, A.; Stengel, B.; Jacquelinet, C.; Landais, P.; Rieu, P.; Bayat, S.; Couchoud, C. Ten-years trends in renal replacement therapy for end-stage renal disease in mainland France: Lessons from the French Renal Epidemiology and Information Network (REIN) registry. Nephrol. Ther. 2017, 13, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Rapport REIN 2016. Agence de la Biomédecine. Available online: http://www.agence-biomedecine.fr/IMG/pdf/rapportrein2014.pdf (accessed on 25 June 2018).
- Couchoud, C.; Stengel, B.; Landais, P.; Aldigier, J.C.; De Cornelissen, F.; Dabot, C.; Maheut, H.; Joyeux, V.; Kessler, M.; Labeeuw, M.; et al. The renal epidemiology and information network (REIN): A new registry for end-stage renal disease in France. Nephrol. Dial. Transpl. 2006, 21, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Couchoud, C.; Stengel, B.; Landais, P.; Aldigier, J.C.; De Cornelissen, F.; Dabot, C.; Maheut, H.; Joyeux, V.; Kessler, M.; Labeeuw, M.; et al. Confounding factors for early death in incident end-stage renal disease patients: Role of emergency dialysis start. Hemodial. Int. 2011, 15, 23–29. [Google Scholar]
- Molnar, A.O.; Hiremath, S.; Brown, P.A.; Akbari, A. Risk factors for unplanned and crash dialysis starts: A protocol for a systematic review and meta-analysis. Syst. Rev. 2016, 5, 117. [Google Scholar] [CrossRef]
- Chen, Y.-M.; Wang, Y.-C.; Hwang, S.-J.; Lin, S.-H.; Wu, K.-D. Patterns of Dialysis Initiation Affect Outcomes of Incident Hemodialysis Patients. Nephron 2016, 132, 33–42. [Google Scholar] [CrossRef]
- Couchoud, C.; Moranne, O.; Frimat, L.; Labeeuw, M.; Allot, V.; Stengel, B. Associations between comorbidities, treatment choice and outcome in the elderly with end-stage renal disease. Nephrol. Dial. Transpl. 2007, 22, 3246–3254. [Google Scholar] [CrossRef]
- Panocchia, N.; Tazza, L.; Di Stasio, E.; Liberatori, M.; Vulpio, C.; Giungi, S.; Lucani, G.; Antocicco, M.; Bossola, M. Mortality in hospitalized chronic kidney disease patients starting unplanned urgent haemodialysis. Nephrol Carlton Vic. 2016, 21, 62–67. [Google Scholar] [CrossRef]
- Park, J.I.; Kim, M.; Kim, H.; An, J.N.; Lee, J.; Yang, S.H.; Cho, J.H.; Kim, Y.L.; Park, K.S.; Oh, Y.K.; et al. Not Early Referral but Planned Dialysis Improves Quality of Life and Depression in Newly Diagnosed End Stage Renal Disease Patients: A Prospective Cohort Study in Korea. PLoS ONE 2015, 10, e0117582. [Google Scholar] [CrossRef] [PubMed]
- Mendelssohn, D.C.; Malmberg, C.; Hamandi, B. An integrated review of “unplanned” dialysis initiation: Reframing the terminology to “suboptimal” initiation. BMC Nephrol. 2009, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Chantrel, F.; Lassalle, M.; Couchoud, C.; Frimat, L. Démarrage d’un traitement par dialyse chronique en urgence. Quels patients? Quelles conséquences? Numéro Thématique-Insuffis Rénale Chron Termin En Fr. 2010, 9, 81–86. [Google Scholar]
- Brown, P.A.; Akbari, A.; Molnar, A.O.; Taran, S.; Bissonnette, J.; Sood, M.; Hiremath, S. Factors Associated with Unplanned Dialysis Starts in Patients followed by Nephrologists: A Retropective Cohort Study. PLoS ONE 2015, 10, e0130080. [Google Scholar] [CrossRef] [PubMed]
- Buck, J.; Baker, R.; Cannaby, A.-M.; Nicholson, S.; Peters, J.; Warwick, G. Why do patients known to renal services still undergo urgent dialysis initiation? A cross-sectional survey. Nephrol. Dial. Transpl. 2007, 22, 3240–3245. [Google Scholar] [CrossRef] [PubMed]
- Marron, B.; Ortiz, A.; de Sequera, P.; Martín-Reyes, G.; de Arriba, G.; Lamas, J.M.; Martínez Ocaña, J.C.; Arrieta, J.; Martínez, F. Impact of end-stage renal disease care in planned dialysis start and type of renal replacement therapy—A Spanish multicentre experience. Nephrol. Dial. Transpl. 2006, 21, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Navaneethan, S.D.; Aloudat, S.; Singh, S. A systematic review of patient and health system characteristics associated with late referral in chronic kidney disease. BMC Nephrol. 2008, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, V.; Jaar, B.G.; Frisby, X.Y.; Chen, S.C.; Qiu, Y.; Li, S.; Whaley-Connell, A.T.; McCullough, P.A.; Bomback, A.S. Access to Health Care Among Adults Evaluated for CKD: Findings from the Kidney Early Evaluation Program (KEEP). Am. J. Kidney Dis. 2012, 59, S5–S15. [Google Scholar] [CrossRef]
- Caskey, F.J.; Kramer, A.; Elliott, R.F.; Stel, V.S.; Covic, A.; Cusumano, A.; Geue, C.; MacLeod, A.M.; Zwinderman, A.H.; Stengel, B.; et al. Global variation in renal replacement therapy for end-stage renal disease. Nephrol. Dial. Transpl. 2011, 26, 2604–2610. [Google Scholar] [CrossRef]
- Millman, M.; Institute of Medicine (US). Committee on Monitoring Access to Personal Health Care Services. Access to Health Care in America; National Academies Press (US): Washington, DC, USA, 1993. [Google Scholar]
- Ward, M.M. Socioeconomic status and the incidence of ESRD. Am. J. Kidney Dis. 2008, 51, 563–572. [Google Scholar] [CrossRef]
- Insee Analyses Bretagne. Bretagne: Une Région Attractive Pour les Actifs et les Retraités. Available online: https://www.insee.fr/fr/statistiques/2880138 (accessed on 27 September 2018).
- van Eupen, M.; Metzger, M.J.; Pérez-Soba, M.; Verburg, P.H.; van Doorn, A.; Bunce, R.G.H. A rural typology for strategic European policies. Land Use Policy 2012, 29, 473–482. [Google Scholar] [CrossRef]
- Organisation for Economic Co-Operation and Development. Creating Rural Indicators for Shaping Territorial Policy; OECD Publications and Information: Washington, DC, USA, 1994. [Google Scholar]
- Vard, T. Trends of Some Agri-Environmental Indicators in the European Union; EU Science Hub: Ispra (VA), Italy, 2005. [Google Scholar]
- INSEE. Measuring, Understanding. National Institute of Statistics and Economic Studies. 2013. Available online: http://www.insee.fr/fr/methodes/default.asp?page=zonages/iris.htm (accessed on 27 September 2018).
- Kulldorff, M. A spatial scan statistic. Commun. Stat. Theory Meth. 1997, 6, 1481–1496. [Google Scholar] [CrossRef]
- SaTScan Software for the Spatial, Temporal, and Space-Time Scan Statistics. Available online: https://www.satscan.org (accessed on 27 September 2018).
- Fan, Z.J.; Lackland, D.T.; Lipsitz, S.R.; Nicholas, J.S.; Egan, B.M.; Garvey, W.T.; Hutchison, F.N. Geographical patterns of end-stage renal disease incidence and risk factors in rural and urban areas of South Carolina. Health Place 2007, 13, 179–187. [Google Scholar] [PubMed]
- Cass, A.; Cunningham, J.; Wang, Z.; Hoy, W. Regional variation in the incidence of end-stage renal disease in Indigenous Australians. Med. J. Aust. 2001, 175, 24–27. [Google Scholar] [PubMed]
- Usami, T.; Sato, R.; Yoshida, A.; Kimura, G. Regional variation in end-stage renal disease. Curr. Opin. Nephrol. Hypertens. 2002, 11, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Kihal-Talantikite, W.; Deguen, S.; Padilla, C.; Siebert, M.; Couchoud, C.; Vigneau, C.; Bayat, S. Spatial distribution of end-stage renal disease (ESRD) and social inequalities in mixed urban and rural areas: A study in the Bretagne administrative region of France. Clin. Kidney J. 2015, 8, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Perchoux, C.; Kestens, Y.; Thomas, F.; Hulst, A.V.; Thierry, B.; Chaix, B. Assessing patterns of spatial behavior in health studies: Their socio-demographic determinants and associations with transportation modes (the RECORD Cohort Study). Soc. Sci. Med. 2014, 119, 64–73. [Google Scholar] [CrossRef]
- Hommel, K.; Rasmussen, S.; Kamper, A.-L.; Madsen, M. Regional and social inequalities in chronic renal replacement therapy in Denmark. Nephrol. Dial. Transpl. 2010, 25, 2624–2632. [Google Scholar] [CrossRef]
- Grace, B.S.; Clayton, P.; Cass, A.; McDonald, S.P. Socio-economic status and incidence of renal replacement therapy: A registry study of Australian patients. Nephrol. Dial. Transpl. 2012, 27, 4173–4180. [Google Scholar] [CrossRef]
- Vart, P.; Gansevoort, R.T.; Coresh, J.; Reijneveld, S.A.; Bültmann, U. Socioeconomic measures and CKD in the United States and The Netherlands. Clin. J. Am. Soc. Nephrol. CJASN 2013, 8, 1685–1693. [Google Scholar] [CrossRef]
- Vart, P.; Gansevoort, R.T.; Joosten, M.M.; Bültmann, U.; Reijneveld, S.A. Socioeconomic disparities in chronic kidney disease: A systematic review and meta-analysis. Am. J. Prev. Med. 2015, 48, 580–592. [Google Scholar] [CrossRef] [PubMed]
- Vart, P.; van Zon, S.K.R.; Gansevoort, R.T.; Bültmann, U.; Reijneveld, S.A. SES, Chronic Kidney Disease, and Race in the U.S.: A Systematic Review and Meta-analysis. Am. J. Prev. Med. 2017, 53, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Liu, J.; Tao, S.; Hong, H.G.; Li, Y.; Fu, P. Associations between socioeconomic status and chronic kidney disease: A meta-analysis. J. Epidemiol. Commun. Health 2018, 72, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Couchoud, C.; Guihenneuc, C.; Bayer, F.; Lemaitre, V.; Brunet, P.; Stengel, B. Medical practice patterns and socio-economic factors may explain geographical variation of end-stage renal disease incidence. Nephrol. Dial. Transpl. 2012, 27, 2312–2322. [Google Scholar] [CrossRef] [PubMed]
- Fored, C.M.; Ejerblad, E.; Fryzek, J.P.; Lambe, M.; Lindblad, P.; Nyrén, O.; Elinder, C.G. Socio-economic status and chronic renal failure: A population-based case-control study in Sweden. Nephrol. Dial. Transpl. 2003, 18, 82–88. [Google Scholar] [CrossRef]
- Volkova, N.; McClellan, W.; Klein, M.; Flanders, D.; Kleinbaum, D.; Soucie, J.M.; Presley, R. Neighborhood poverty and racial differences in ESRD incidence. J. Am. Soc. Nephrol. JASN 2008, 19, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Crews, D.C.; Gutiérrez, O.M.; Fedewa, S.A.; Luthi, J.C.; Shoham, D.; Judd, S.E.; Powe, N.R.; McClellan, W.M. Low income, community poverty and risk of end stage renal disease. BMC Nephrol. 2014, 15, 192. [Google Scholar] [CrossRef]
- Leclerc, A.; Fassin, D.; Grandjean, H.; Kaminski, M.; Lang, T. Les Inégalités Sociales de Santé; INSERM-la Découverte: Paris, France, 2000; p. 448. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Entire Bretagne (n = 665) | Higher-Risk Cluster ** (n = 70) | Lower-Risk Cluster ** (n = 78) | p-Value * |
|---|---|---|---|---|
| Incidence of emergency first dialysis per 100,000 inhabitants (mean ± SD) ** | 270.3 ± 744.6 | 434.1 ± 573.2 | 133.1 ± 396.6 | <0.0001 |
| PRIMARY RENAL disease (%) | ||||
| Polycystic disease | 3.8 | 0 | 1.3 | 0.980 |
| Hypertensive and vascular nephropathy | 26.4 | 12.9 | 25.6 | 0.051 |
| Glomerulonephritis | 12.3 | 7.1 | 19.2 | 0.052 |
| Pyelonephritis | 5.9 | 5.7 | 5.1 | 0.973 |
| Diabetic nephropathy | 9.6 | 8.6 | 14.1 | 0.316 |
| Others (Unknown and unclassifiable nephropathy) | 42 | 65.7 | 34.6 | <0.0001 |
| COMORBIDITIES (%) | ||||
| Respiratory disease | 20.9 | 18.8 | 23.4 | 0.482 |
| Active malignancy | 22.2 | 33.3 | 20 | 0.09 |
| Hepatic disease | 4.6 | 5.9 | 5.2 | 0.940 |
| Diabetes | 31.5 | 28.6 | 32 | 0.722 |
| CARDIOVASCULAR disease (%) | 0.921 | |||
| No | 35.4 | 34.3 | 32 | |
| One | 21.2 | 22.9 | 21.8 | |
| Two or more | 43.4 | 42.9 | 46.2 | |
| PHYSICAL DISABILITIES (%) | 0.019 | |||
| No | 93.2 | 97.1 | 85.9 | |
| One or more | 6.8 | 2.9 | 14.1 | |
| PSYCHIATRIC DISORDER (yes) (%) | 26.8 | 33.3 | 26.3 | 0.901 |
| BMI (%) | 0.658 | |||
| Underweight and normal (BMI < 25) | 52.7 | 64.6 | 57.1 | |
| Overweight (BMI ≥ 25) | 29.8 | 23.1 | 28.6 | |
| Obese (BMI > 30) | 16.7 | 11.4 | 14.1 | |
| SMOKING status (%) | 0.849 | |||
| Ex-smoker | 46 | 44.7 | 50 | |
| Smoker | 17.6 | 14.9 | 13.9 | |
| Never Smoked | 36.4 | 40.4 | 36.1 | |
| ALBUMIN (%) | 0.444 | |||
| <30 g/dL | 41.1 | 35.7 | 26.5 | |
| ≥30 g/dL | 58.9 | 64.3 | 73.5 | |
| HEMOGLOBIN (%) | 0.773 | |||
| <10 g/dL | 58.1 | 48.8 | 47.9 | |
| 10–12 g/dL | 37.4 | 44.2 | 47.9 | |
| >12 g/dL | 4.4 | 7 | 4.1 |
| Variables | Entire Bretagne (n = 665) | Higher-Risk Cluster ** (n = 70) | Lower-Risk Cluster ** (n = 78) | p-Value * |
|---|---|---|---|---|
| Incidence of emergency first dialysis per 100,000 inhabitants (mean ± SD) ** | 270.3 ± 744.6 | 434.1 ± 573.2 | 133.1 ± 396.6 | <0.0001 |
| SOCIO-DEMOGRAPHIC | ||||
| PROPORTION of MEN (%) | 68.3 | 65.7 | 69.2 | 0.648 |
| AGE by group (%) | 0.579 | |||
| <45 years | 15.5 | 41.4 | 48.7 | |
| 45–75 years | 49.6 | 40.0 | 32.1 | |
| >75 years | 34.9 | 18.6 | 19.2 | |
| PATIENT’S ACTIVITY (%) | 0.304 | |||
| Inactive | 85 | 85.5 | 78.9 | |
| Active | 15 | 14.5 | 21 | |
| ESRD MANAGEMENT | ||||
| TIME in TRANSPORT (mean ± SD in minutes) | 24.4 ± 0.7 | 21.5 ± 18.8 | 15 ± 11.1 | 0.0132 |
| TYPE of TRANSPORT (%) | <0.0001 | |||
| Ambulance | 7.6 | 6.7 | 10.5 | |
| Light sanitary vehicle | 64.4 | 71.7 | 37.3 | |
| Taxi | 20.1 | 11.7 | 32.8 | |
| Car | 3.6 | 0 | 10.4 | |
| Others | 4.4 | 10 | 9 | |
| VASCULAR ACCESS procedure (%) | 0.939 | |||
| Temporary vascular access | 98 | 98.6 | 98.7 | |
| Permanent vascular access | 1.9 | 1.4 | 1.3 | |
| N° of nephrologist consultations (%) | 0.371 | |||
| No consultations | 46.4 | 58.3 | 46.4 | |
| <3 consultations | 17.6 | 11.7 | 13.0 | |
| ≥3 consultations | 36.0 | 30.0 | 40.6 | |
| Variables | Entire Bretagne (n = 1270) | Higher-Risk Cluster ** (n = 53) | Lower-Risk Cluster ** (n = 169) | p-Value * | |
|---|---|---|---|---|---|
| SOCIO-DEMOGRAPHIC | |||||
| Occupation | Proportion of blue-collar workers in the labor force (%) | 34.1 ± 12.8 | 28.8 ± 8.9 | 28.9 ± 10.3 | 0.65 |
| Proportion of managers in the labor force (%) | 8.6 ± 5.8 | 9.1 ± 5.5 | 13.4 ± 6.6 | <0.001 | |
| Proportion of intermediary workers in the labor force (%) | 48.4 ± 11 | 50.7 ± 7.7 | 50.6 ± 7.8 | 0.11 | |
| Education | People aged 15 years or older with a higher education degree (%) | 22.5 ± 6.8 | 23.3 ± 5.4 | 28.6 ± 8.0 | <0.0001 |
| People aged 15 years or older with at least a lower tertiary education (%) | 47.5 ± 4.8 | 48.3 ± 4.1 | 45.9 ± 4.9 | 0.002 | |
| People aged 15 years or older who did not go beyond elementary education (%) | 29.9 ± 7.2 | 28.3 ± 6.3 | 25.5 ± 6 | 0.006 | |
| Unemployment | Proportion of unemployed people (%) | 10.2 ± 3.4 | 10.9 ± 2.8 | 7.8 ± 2.1 | <0.001 |
| Immigration status | Proportion of foreigners in the total population (%) | 1.9 ± 2.5 | 1.2 ± 0.7 | 1.3 ± 1.1 | 0.49 |
| Housing | Subsidized housing among all primary residences (%) | 4.9 ± 4 | 6.8 ± 3.3 | 6.6 ± 4.7 | 0.37 |
| Household with at least one car (%) | 91.9 ± 5.7 | 91.2 ± 7.4 | 93.7 ± 3.1 | 0.01 | |
| Resources | Median income per consumption unit (mean ±SD) | 19,437 ± 2029 | 19,863 ± 1046 | 20,831 ± 2129 | 0.002 |
| Residential mobility | Proportion of principal residence for less than 2 years (%) | 10 ± 3.1 | 8.6 ± 2.8 | 11.3 ± 3.4 | <0.001 |
| Proportion of principal residence for more than 10 years (%) | 56. ± 6.7 | 60.7 ± 6.7 | 51.2 ± 7.1 | <0.001 | |
| Variables | Entire Bretagne (n = 1270) | Higher-Risk Cluster ** (n = 53) | Lower-Risk Cluster ** (n = 169) | p-Value * |
|---|---|---|---|---|
| Degree of URBANIZATION | ||||
| Urban (%) | 17.2 | 24.5 | 23.1 | <0.0001 |
| Peri-urban (%) | 5.3 | 0 | 10.6 | |
| Rural (%) | 77.6 | 75.5 | 66.3 | |
| POTENTIAL HEALTHCARE OFFER | ||||
| Proportion of municipalities with at least one dialysis facility, number (%) | 36 (2.8%) | 3 (5.6%) | 2 (1.2%) | 0.09 |
| General practitioners’ density per 10,000 inhabitants | 5.5 ± 7.5 | 7.6 ± 9.3 | 5.5 ± 8.2 | 0.09 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padilla, C.M.; Raffray, M.; Pladys, A.; Vigneau, C.; Bayat, S. Geographic Variations in the Risk of Emergency First Dialysis for Patients with End Stage Renal Disease in the Bretagne Region, France. Int. J. Environ. Res. Public Health 2019, 16, 18. https://doi.org/10.3390/ijerph16010018
Padilla CM, Raffray M, Pladys A, Vigneau C, Bayat S. Geographic Variations in the Risk of Emergency First Dialysis for Patients with End Stage Renal Disease in the Bretagne Region, France. International Journal of Environmental Research and Public Health. 2019; 16(1):18. https://doi.org/10.3390/ijerph16010018
Chicago/Turabian StylePadilla, Cindy M., Maxime Raffray, Adélaïde Pladys, Cécile Vigneau, and Sahar Bayat. 2019. "Geographic Variations in the Risk of Emergency First Dialysis for Patients with End Stage Renal Disease in the Bretagne Region, France" International Journal of Environmental Research and Public Health 16, no. 1: 18. https://doi.org/10.3390/ijerph16010018
APA StylePadilla, C. M., Raffray, M., Pladys, A., Vigneau, C., & Bayat, S. (2019). Geographic Variations in the Risk of Emergency First Dialysis for Patients with End Stage Renal Disease in the Bretagne Region, France. International Journal of Environmental Research and Public Health, 16(1), 18. https://doi.org/10.3390/ijerph16010018