The Cooking and Pneumonia Study (CAPS) in Malawi: A Cross-Sectional Assessment of Carbon Monoxide Exposure and Carboxyhemoglobin Levels in Children under 5 Years Old



Abstract
1. Introduction
2. Materials and Methods
2.1. Setting
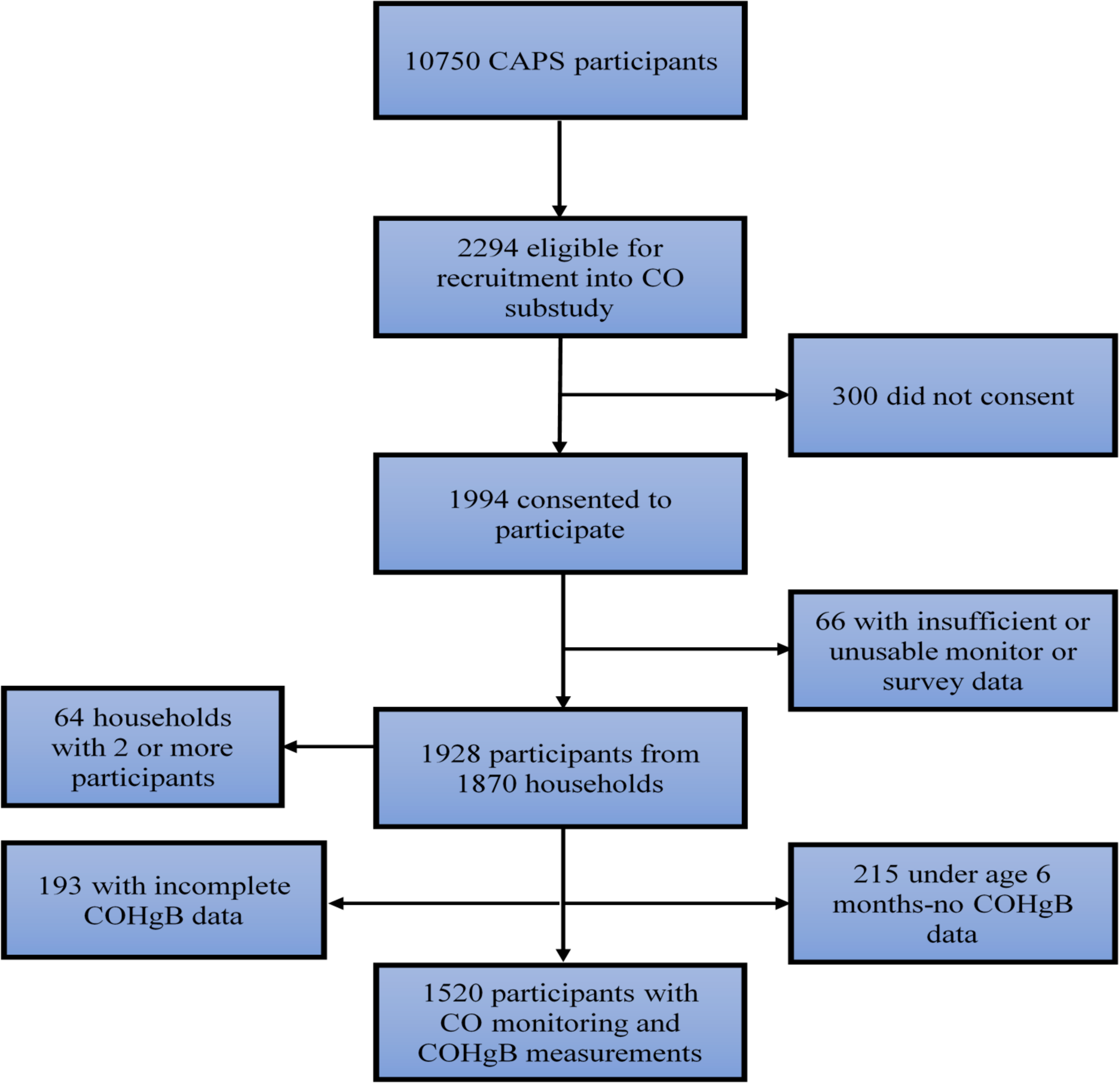
2.2. Participants
2.3. Data Collection (Questionnaires)
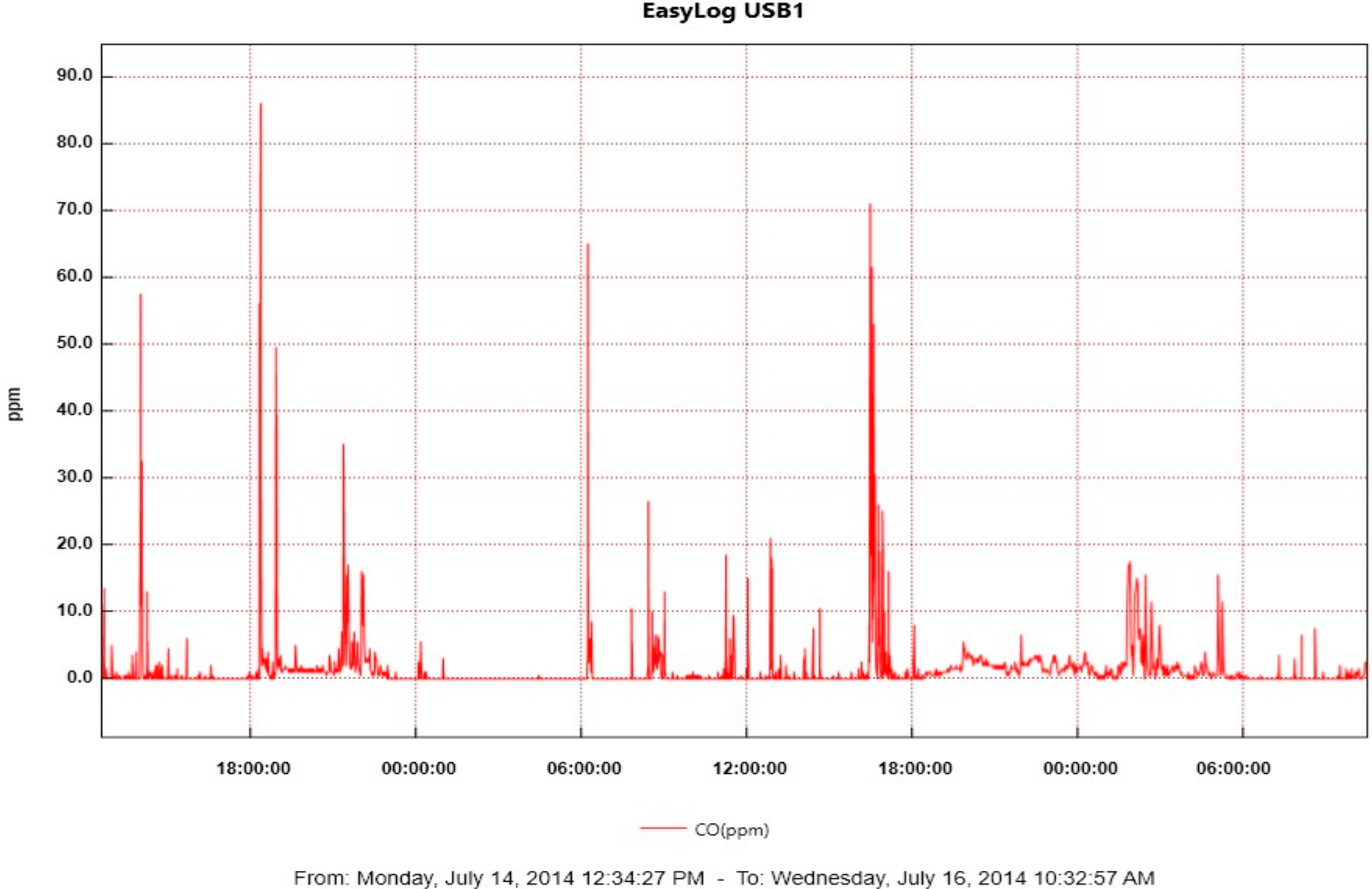
2.4. Data Collection (Carbon Monoxide Exposure Assessments)
2.5. Data Management
2.6. Statistical Methods
2.7. Ethical Considerations
2.8. Role of the Funding Source
3. Results
3.1. Study Sites
3.2. Pneumonia and Other Reported Symptoms
3.3. Cooking Location
3.4. Cooking Events
3.5. Fuels and Stoves Used
3.6. Other Sources of Smoke Exposure
3.7. CO Exposure Monitoring
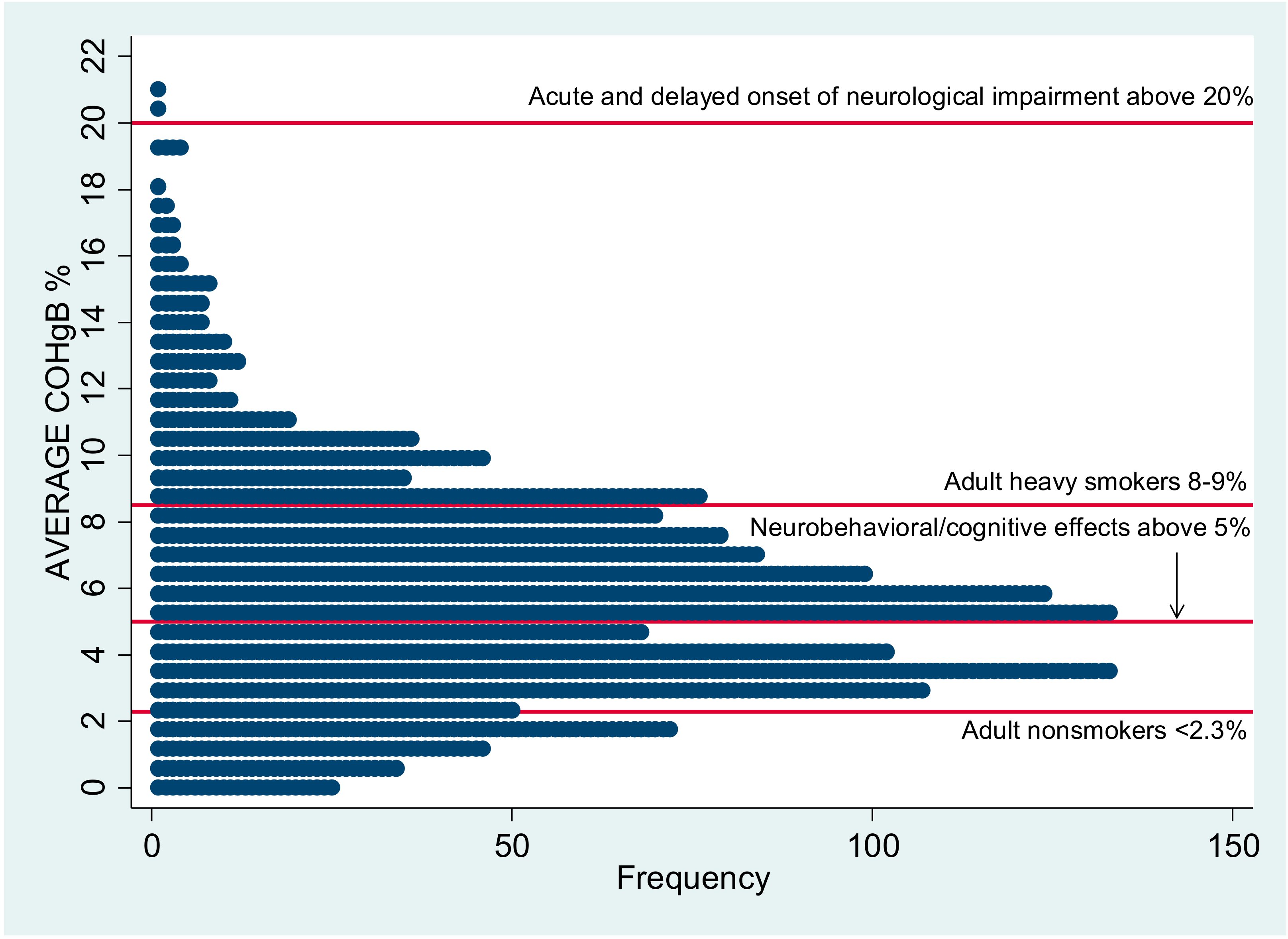
3.8. COHgB
3.9. Relationship between CO and COHgB Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- International Energy Agency. Africa Energy Outlook. 2014. Available online: http://www.iea.org/publications/freepublications/publication/WEO2014_AfricaEnergyOutlook.pdf (accessed on 10 October 2017).
- Gordon, S.B.; Bruce, N.G.; Grigg, J.; Hibberd, P.L.; Kurmi, O.P.; Lam, K.H.; Mortimer, K.; Asante, K.P.; Balakrishnan, K.; Balmes, J.; et al. Respiratory risks from household air pollution in low and middle income countries. Lancet 2014, 2, 823–860. [Google Scholar] [CrossRef]
- World Health Organization. Household Air Pollution and Health Fact Sheet. 2016. Available online: http://www.who.int/mediacentre/factsheets/fs292/en/ (accessed on 1 April 2017).
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Piddock, K.C.; Gordon, S.B.; Ngwira, A.; Msukwa, M.; Nadeau, G.; Davis, K.J.; Nyirenda, M.J.; Mortimer, K. A cross-sectional study of household biomass fuel use among a periurban population in Malawi. Ann. Am. Thorac. Soc. 2014, 11, 915–924. [Google Scholar] [CrossRef] [PubMed]
- Meghji, J.; Nadeau, G.; Davis, K.J.; Wang, D.; Nyirenda, M.J.; Gordon, S.B.; Mortimer, K. Noncommunicable lung disease in sub-Saharan Africa. A community-based cross-sectional study of adults in urban Malawi. Am. J. Respir. Crit. Care Med. 2016, 194, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Fullerton, D.G.; Semple, S.; Kalambo, F.; Suseno, A.; Malamba, R.; Henderson, G.; Ayres, J.G.; Gordon, S.B. Biomass fuel use and indoor air pollution in homes in Malawi. Occup. Environ. Med. 2009, 66, 777–783. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Pneumonia Fact Sheet. 2016. Available online: http://www.who.int/mediacentre/factsheets/fs331/en/ (accessed on 1 April 2017).
- Jetter, J.; Zhao, Y.; Smith, K.R.; Khan, B.; Yelverton, T.; DeCarlo, P.; Hays, M.D. Pollutant emissions and energy efficiency under controlled conditions for household biomass cookstoves and implications for metrics useful in setting international test standards. Environ. Sci. Technol. 2012, 46, 10827–10834. [Google Scholar] [CrossRef] [PubMed]
- Wathore, R.; Mortimer, K.; Grieshop, A.P. In-use emissions and estimated impacts of traditional, natural- and forced-draft cookstoves in rural Malawi. Environ. Sci. Technol. 2017, 51, 1929–1938. [Google Scholar] [CrossRef] [PubMed]
- Kar, A.; Rehman, I.H.; Burney, J.; Puppala, S.P.; Suresh, R.; Singh, L.; Singh, V.K.; Ahmed, T.; Ramanathan, N.; Ramanathan, V. Real-time assessment of black carbon pollution in Indian households due to traditional and improved biomass cookstoves. Environ. Sci. Technol. 2012, 46, 2993–3000. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.; McCraken, J.; Thompson, L.; Edwards, R.; Shields, K.; Caruz, E.; Bruce, N. Personal child and mother carbon monoxide exposures and kitchen levels: Methods and results from a randomized trial of woodfired chimney cookstoves in Guatemala (RESPIRE). J. Expo. Sci. Environ. Epidemiol. 2010, 20, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Carter, E.; Norris, C.; Dionisio, K.; Balakrishnan, K.; Checkley, W.; Clark, M.; Ghosh, S.; Jack, D.W.; Kinney, P.L.; Marshall, J.D.; et al. Assessing exposure to household air pollution: A systematic review and pooled analysis of carbon monoxide as a surrogate measure of particulate matter. Environ. Health Perspect. 2017, 125, 076002. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Air Quality Guidelines for Europe, 2nd ed.; World Health Organization: Geneva, Switzerland, 2000; Available online: http://www.euro.who.int/__data/assets/pdf_file/0005/74732/E71922.pdf (accessed on 6 August 2018).
- Mortimer, K.; Ndamala, C.; Naunje, A.; Malava, J.; Katundu, C.; Weston, W.; Havens, D.; Pope, D.; Bruce, N.G.; Nyirenda, M.; et al. A cleaner burning biomass-fuelled cookstove intervention to prevent pneumonia in children under 5 years old in rural Malawi (the Cooking and Pneumonia Study): A cluster randomized controlled trial. Lancet 2017, 389, 167–175. [Google Scholar] [CrossRef]
- Mortimer, K.; Gordon, S.B. Protocol 13PRT/4689: An Advanced Cookstove Intervention to Prevent Pneumonia in Children Younger Than 5 Years in Malawi: A Cluster Randomised Controlled Trial (ISRCTN59448623). Available online: http://www.thelancet.com/protocol-reviews/13PRT-4689 (accessed on 1 April 2017).
- World Health Organization. WHO Guidelines for Indoor Air Quality: Selected Pollutants; World Health Organization: Geneva, Switzerland, 2010. Available online: https://www.ncbi.nlm.nih.gov/books/NBK138705/pdf/Bookshelf_NBK138705.pdf (accessed on 1 April 2017).
- Northcross, A.; Chowdhury, Z.; McCracken, J.; Canuz, E.; Smith, K.R. Estimating personal PM2.5 exposures using CO measurements in Guatemalan households cooking with wood fuel. J. Environ. Monit. 2010, 12, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Dionisio, K.L.; Howie, S.R.; Dominici, F.; Fornace, K.M.; Spengler, J.D.; Donkor, S.; Chimah, O.; Oluwalana, C.; Ideh, R.C.; Ebruke, B.; et al. The exposure of infants and children to carbon monoxide from biomass fuels in The Gambia: A measurement and modeling study. J. Expo. Sci. Environ. Epidemiol. 2012, 22, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.S.; Louis, V.R.; Sie, A.; Sauerborn, R. Biomass smoke in Burkina Faso: What is the relationship between particulate matter, carbon monoxide, and kitchen characteristics? Environ. Sci. Pollut. Res. Int. 2014, 21, 2581–2591. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, R.; Sambandam, S.; Pillarisetti, A.; Jack, D.; Mukhopadhyay, K.; Balakrishnan, K.; Vaswani, M.; Bates, M.N.; Kinney, P.L.; Arora, N.; et al. Cooking practices, air quality, and the acceptability of advanced cookstoves in Haryana, India: An exploratory study to inform large-scale interventions. Glob. Health Action 2012, 5, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Cynthia, A.A.; Edwards, R.D.; Johnson, M.; Zuk, M.; Rojas, L.; Jiminez, R.D.; Riojas-Rodriguez, H.; Masera, O. Reduction in personal exposures to particulate matter and carbon monoxide as a result of the installation of a Patsari improved cook stove in Michoacan Mexico. Indoor Air 2008, 18, 93–105. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Carbon Monoxide. 1999. Available online: http://www.inchem.org/documents/ehc/ehc/ehc213.htm#5.3.2 (accessed on 1 April 2017).
- Agency for Toxic Substances and Disease Registry. Toxicologic Profile for Carbon Monoxide. 2012. Available online: https://www.atsdr.cdc.gov/toxprofiles/tp201.pdf (accessed on 1 April 2017).
- Behera, D.; Dash, S.; Yadav, S.P. Carboxyhaemoglobin in women exposed to different cooking fuels. Thorax 1991, 46, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Lam, N.; Nicas, M.; Ruiz-Mercado, I.; Thompson, L.M.; Romero, C.; Smith, K.R. Non-invasive measurement of carbon monoxide burden in Guatemalan children and adults following wood-fired temazcal (sauna-bath) use. J. Environ. Monit. 2011, 13, 2171–2181. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.; Park, S.E.; Lee, K.; Yanagisawa, Y.; Spengler, J.D. Determinations of personal carbon monoxide exposure and blood carboxyhemoglobin levels in Korea. Yonsei Med. J. 1994, 35, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, S.R.; Richards, J.B. Noninvasive carbon monoxide detection: Insufficient evidence for broad clinical use. Respir. Care 2013, 58, 376–379. [Google Scholar] [CrossRef] [PubMed]
- Maisel, W.H.; Lewis, R.J. Noninvasive measurement of carboxyhemoglobin: How accurate is accurate enough? Ann. Emerg. Med. 2010, 56, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Cunnington, A.J.; Kendrick, S.F.; Wamola, B.; Lowe, B.; Newton, C.R. Carboxyhemoglobin levels in Kenyan children with Plasmodium falciparum malaria. Am. J. Trop. Med. Hyg. 2004, 71, 43–47. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CAPS (Overall) | CO Sub-Study | |
|---|---|---|
| Community Characteristics | 10,750 | 1928 |
| Chilumba | 6508 (60.5%) | 1105 (57.3%) |
| Chikhwawa | 4242 (39.5%) | 823 (42.7%) |
| Participant Characteristics | ||
| Age (mean) | 24 mo | 25 mo |
| Sex | ||
| Female | 5445 (50.7%) | 966 (50.1%) |
| Male | 5305 (49.3%) | 962 (49.9%) |
| Cough in past 3 months | 6259 (58.2%) | 1170 (60.7%) |
| Wheezing in past 3 months | 1770 (16.5%) | 334 (17.3%) |
| Cooking related burn in past 3 months | 516 (4.8%) | 118 (6.1%) |
| Diagnosis of pneumonia in past 12 months | 1636 (15.2%) | 317 (16.4%) |
| Household Characteristics | ||
| Number of households | 8550 | 1870 |
| Cooking Fuel | ||
| Wood | 4946 (57.8%) | 1089 (58.2%) |
| Crop Residue | 2686 (31.4%) | 657 (35.1%) |
| Charcoal | 1310 (15.3%) | 317 (17.0%) |
| Dung | 45 (0.5%) | 11 (0.6%) |
| Electricity | 19 (0.2%) | 2 (0.1%) |
| LPG | 2 (0.0%) | 0 |
| Kerosene | 8 (0.1%) | 2 (0.1%) |
| Other | 2 (0.0%) | 3 (0.2%) |
| Smoker in the household | 1443 (16.9%) | 313 (16.7%) |
| Experienced a time in the past year when there was not enough money for food | 4347 (50.8%) | 1038 (55.5%) |
| Experienced a time in the past year when there was not enough money to buy soap | 5317 (62.2%) | 1280 (68.4%) |
| Daily or almost daily exposure to smoke from: | ||
| Burning rubbish | 3471 (40.6%) | 791 (42.3%) |
| Cooking for others as a business | 1083 (12.7%) | 268 (14.3%) |
| Making beer | 100 (1.2%) | 21 (1.1%) |
| Making bricks | 395 (4.6%) | 97 (5.2%) |
| Kerosene lamps | 195 (2.3%) | 47 (2.5%) |
| Mosquito coils | 128 (1.5%) | 29 (1.6%) |
| Other sources | 111 (1.3%) | 26 (1.4%) |
| Primary cooking location—Dry season | ||
| Outside with a separate structure with a roof only | 1160 (13.6%) | 258 (13.8%) |
| Outside in a separate structure with a roof and walls | 3331 (39.0%) | 756 (40.4%) |
| Outside in the open air | 1827 (21.4%) | 422 (22.6%) |
| Outside on the veranda (khonde) | 1673 (19.6%) | 366 (19.6%) |
| Inside in a separate room (kitchen) | 355 (4.2%) | 63 (3.4%) |
| Inside in a living room | 286 (3.3%) | 63 (3.4%) |
| Primary cooking location—Rainy season | ||
| Outside with a separate structure with a roof only | 1076 (12.6%) | 229 (12.2%) |
| Outside in a separate structure with a roof and walls | 3613 (42.3%) | 816 (43.6%) |
| Outside in the open air | 87 (1.0%) | 19 (1.0%) |
| Outside on the veranda | 1981 (23.2%) | 434 (23.2%) |
| Inside in a separate room (kitchen) | 701 (8.2%) | 160 (8.6%) |
| Inside in a living room | 1174 (13.7%) | 270 (14.4%) |
| Univariable | Multivariable | |
|---|---|---|
| OR (95% CI) 2 | OR (95% CI) | |
| Presence of cough in 3 months prior | 0.78 (0.63–0.97) | 0.77 (0.62–0.96) |
| Diagnosis of pneumonia in 12 months prior | 0.83 (0.63–1.10) | |
| Presence of wheeze in 3 months prior | 1.17 (0.89–1.53) | |
| Occurrence of burn in 3 months prior | 1.63 (1.02–2.60) | 1.58 (1.00–2.50) |
| Wood | 0.17 (0.14–0.21) | 0.67 (0.36–1.24) |
| Charcoal | 0.73 (0.53–1.02) | |
| Crop | 0.55 (0.42–0.73) | 0.98 (0.75–1.27) |
| Dung | 0.25 (0.05–1.30) | |
| Other | 2.51 (0.20–31.14) | |
| Smoker in the home | 1.15 (0.86–1.55) | |
| Male gender | 1.01 (0.82–1.24) | |
| Making bricks | 0.70 (0.42–1.17) | |
| Making beer | 1.20 (0.46–3.11) | |
| Rubbish burning | 0.45 (0.31–0.67) | 0.93 (0.70–1.23) |
| Use of kerosene lamp | 0.73 (0.36–1.47) | |
| Use of mosquito coil | 0.87 (0.38–2.02) | |
| Cooking as a business | 0.76 (0.55–1.05) | |
| Period without food in the prior year | 1.91 (1.44–2.54) | 1.50 (1.14–1.95) |
| Period without money to buy soap in the prior year | 1.57 (1.20–2.06) | 1.02 (0.79–1.32) |
| Chikhwawa vs. Chilumba | 7.11 (4.11–12.28) | 3.55 (1.73–7.26) |
| Cooking inside in the dry season | 2.13 (1.36–3.36) | 1.56 (0.93–2.62) |
| Cooking inside in the rainy season | 1.38 (1.07–1.78) | 1.04 (0.78–1.38) |
| Univariable | Multivariable | |
|---|---|---|
| OR (95% CI) 2 | OR (95% CI) | |
| Presence of cough in 3 months prior | 0.97 (0.75–1.27) | |
| Diagnosis of pneumonia in 12 months prior | 1.03 (0.76–1.40) | |
| Presence of wheeze in 3 months prior | 1.34 (0.95–1.90) | |
| Occurrence of burn in 3 months prior | 1.06 (0.65–1.73) | |
| Wood | 0.34 (0.21–0.55) | 0.82 (0.36–1.89) |
| Charcoal | 0.59 (0.38–0.93) | 0.88 (0.59–1.31) |
| Crop | 0.58 (0.40–0.85) | 1.07 (0.74–1.55) |
| Dung | 0.63 (0.10–3.77) | |
| Smoker in the home | 1.27 (0.89–1.81) | |
| Male gender | 1.35 (1.02–1.79) | 1.30 (0.99–1.72) |
| Making bricks | 0.71 (0.39–1.29) | |
| Making beer | 0.61 (0.18–2.13) | |
| Rubbish burning | 0.56 (0.39–0.81) | 1.09 (0.75–1.59) |
| Use of kerosene lamp | 1.53 (0.65–3.56) | |
| Use of a mosquito coil | 0.68 (0.24–1.99) | |
| Cooking as a business | 1.05 (0.71–1.57) | |
| Period without food in the prior year | 1.47 (1.09–1.99) | 1.05 (0.79–1.40) |
| Period without money to buy soap in the prior year | 1.21 (0.90–1.62) | |
| Chikhwawa vs. Chilumba | 3.12 (1.89–5.14) | 2.77 (1.08–7.08) |
| Cooking inside in the dry season) | 1.09 (0.67–1.79) | |
| Cooking inside in the rainy season | 0.69–1.30) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Havens, D.; Wang, D.; Grigg, J.; Gordon, S.B.; Balmes, J.; Mortimer, K. The Cooking and Pneumonia Study (CAPS) in Malawi: A Cross-Sectional Assessment of Carbon Monoxide Exposure and Carboxyhemoglobin Levels in Children under 5 Years Old. Int. J. Environ. Res. Public Health 2018, 15, 1936. https://doi.org/10.3390/ijerph15091936
Havens D, Wang D, Grigg J, Gordon SB, Balmes J, Mortimer K. The Cooking and Pneumonia Study (CAPS) in Malawi: A Cross-Sectional Assessment of Carbon Monoxide Exposure and Carboxyhemoglobin Levels in Children under 5 Years Old. International Journal of Environmental Research and Public Health. 2018; 15(9):1936. https://doi.org/10.3390/ijerph15091936
Chicago/Turabian StyleHavens, Deborah, Duolao Wang, Jonathan Grigg, Stephen B. Gordon, John Balmes, and Kevin Mortimer. 2018. "The Cooking and Pneumonia Study (CAPS) in Malawi: A Cross-Sectional Assessment of Carbon Monoxide Exposure and Carboxyhemoglobin Levels in Children under 5 Years Old" International Journal of Environmental Research and Public Health 15, no. 9: 1936. https://doi.org/10.3390/ijerph15091936
APA StyleHavens, D., Wang, D., Grigg, J., Gordon, S. B., Balmes, J., & Mortimer, K. (2018). The Cooking and Pneumonia Study (CAPS) in Malawi: A Cross-Sectional Assessment of Carbon Monoxide Exposure and Carboxyhemoglobin Levels in Children under 5 Years Old. International Journal of Environmental Research and Public Health, 15(9), 1936. https://doi.org/10.3390/ijerph15091936